
Potentially Inappropriate Use of Opioids in the Management of Migraine in Colombia

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
- Sociodemographic: age (years), sex (female, male), geographic region of residence according to the National Administrative Department of Statistics (DANE) of Colombia, insurer;
- Diagnosis: migraine (ICD-10 code identified; G43.0 migraine without aura [common migraine]; G43.1 migraine with aura [classic migraine]; G43.2 migraine state; G43;
- Complicated migraine; G43.8 other migraines; G43.9 migraine, unspecified), date of first migraine diagnosis (index date);
- Pharmacological: The medications used for the management of migraine were identified by classifying them into the following groups: acute episode, antimigraine (triptans, ergot derivatives), analgesics (acetaminophen, NSAIDs), and other pain relievers (opioids, metoclopramide);
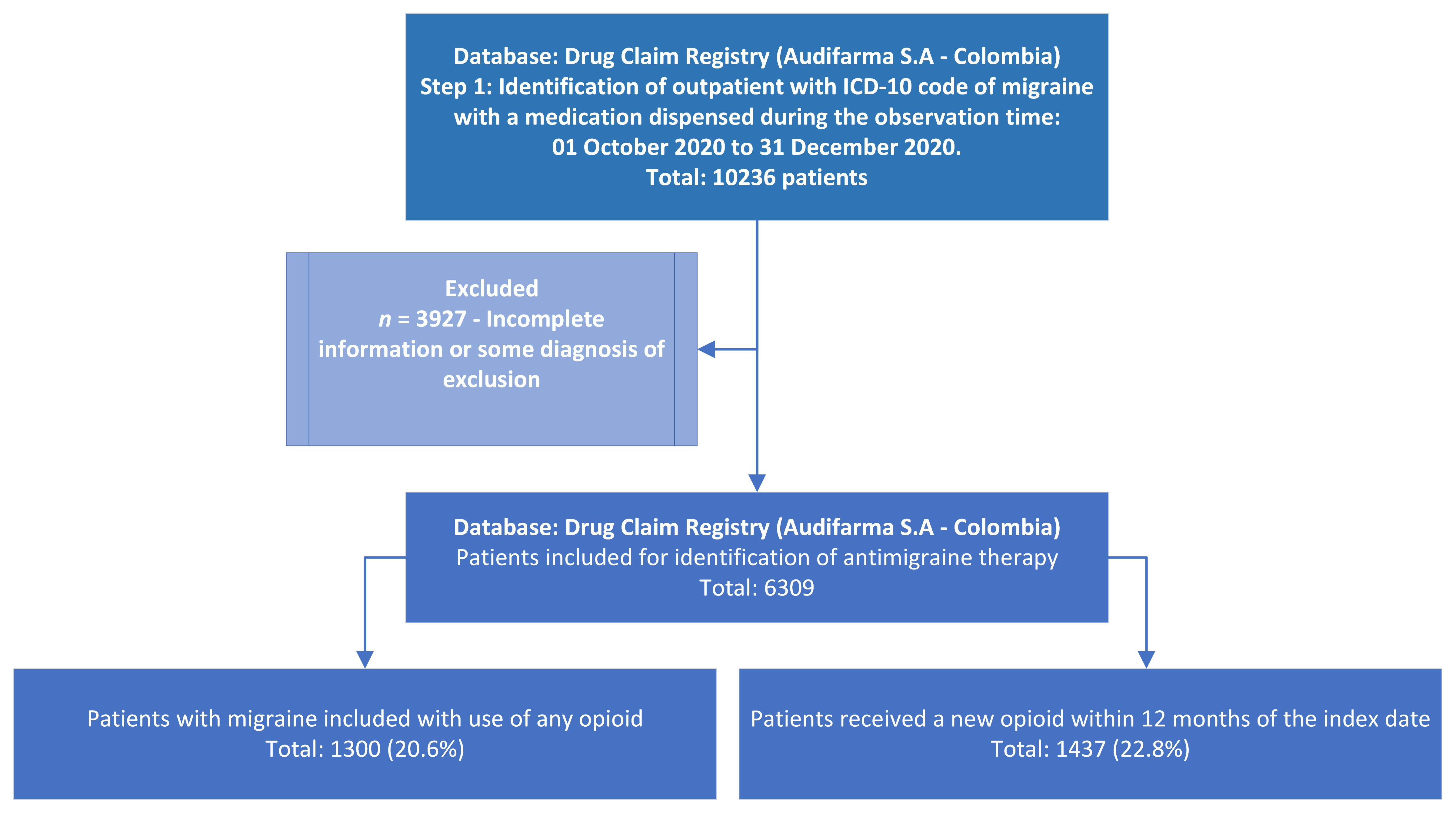
- Use of opioids: In those patients who identified the use of opioids in the management of migraine, a comparison was made with those who did not receive opioids on the index date. During the subsequent 12 months, patients were monitored to determine the frequency of new opioid prescriptions, and the specialty of the prescribing physician was identified. The time of the first prescription of opioids or other medications for the management of migraine during the observation period was determined as the index date. Follow-up was performed for 12 months from this date and continued until a patient had a new prescription for an opioid or until 31 December 2021.
2.2. Bioethical Considerations
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pascual, J. Treatment of migraine in the year 2020. Med. Clin. 2019, 152, 226–228. [Google Scholar] [CrossRef]
- American Headache Society. The American Headache Society Position Statement on Integrating New Migraine Treatments into Clinical Practice. Headache 2019, 59, 1–18. [Google Scholar]
- Lim, J.H.; Karimi, L.; Wijeratne, T. An Evaluation of Medication Prescribing Patterns for Acute Migraine in the Emergency Department: A Scoping Review. J. Clin. Med. 2021, 10, 1191. [Google Scholar] [CrossRef]
- Machado-Alba, J.E.; Gaviria-Mendoza, A.; Machado-Duque, M.E. Patterns of pharmacological treatment of patients with migraine, tension-type headache, and cluster headache in a large group of patients in Colombia, 2019. Int. Clin. Psychopharmacol. 2020, 35, 279–284. [Google Scholar] [CrossRef]
- Casucci, G.; Cevoli, S. Controversies in migraine treatment: Opioids should be avoided. Neurol. Sci. 2013, 34 (Suppl. S1), S125–S128. [Google Scholar] [CrossRef]
- Cevoli, S.; Cortelli, P. Italian Law “measures to guarantee the access to palliative and pain treatments”: Rebound on headaches’ management. Neurol. Sci. 2011, 32 (Suppl. S1), S77–S79. [Google Scholar] [CrossRef]
- Schuchat, A.; Houry, D.; Guy, G.P., Jr. New Data on Opioid Use and Prescribing in the United States. JAMA 2017, 318, 425–426. [Google Scholar] [CrossRef]
- Harder, V.S.; Plante, T.B.; Koh, I.; Rogers, E.B.; Varni, S.E.; Villanti, A.C.; Brooklyn, J.R.; Fairfield, K.M. Influence of Opioid Prescription Policy on Overdoses and Related Adverse Effects in a Primary Care Population. J. Gen. Int. Med. 2021, 36, 2013–2020. [Google Scholar] [CrossRef]
- Shao, Q.; Rascati, K.L.; Lawson, K.A.; Wilson, J.P.; Shah, S.; Garrett, J.S. Impact of emergency department opioid use on future health resource utilization among patients with migraine. Headache 2021, 61, 287–299. [Google Scholar] [CrossRef]
- Thiels, C.A.; Habermann, E.B.; Hooten, W.M.; Jeffery, M.M. Chronic use of tramadol after acute pain episode: Cohort study. BMJ 2019, 365, l1849. [Google Scholar] [CrossRef]
- Machado-Alba, J.E.; Serna-Echeverri, L.S.; Valladales-Restrepo, L.F.; Machado-Duque, M.E.; Gaviria-Mendoza, A. Use of Tramadol or Other Analgesics in Patients Treated in the Emergency Department as a Risk Factor for Opioid Use. Pain Res. Manag. 2020, 2020, 8847777. [Google Scholar] [CrossRef]
- Cohen, B.; Ruth, L.J.; Preuss, C.V. Opioid Analgesics; StatPearls Publishing LLC.: St. Petersburg, FL, USA, 2021. [Google Scholar]
- Muñoz, J.; Volcy, M.; Sobrino, F.; Ramírez, S.; Uribe, B.; Pradilla, G.; Castro, C. Consenso de expertos de la Asociación Colombiana de Neurología para el tratamiento preventivo y agudo de la migraña. Acta Neurol. Colomb. 2014, 30, 175–185. [Google Scholar]
- Thorlund, K.; Toor, K.; Wu, P.; Chan, K.; Druyts, E.; Ramos, E.; Bhambri, R.; Donnet, A.; Stark, R.; Goadsby, P.J. Comparative tolerability of treatments for acute migraine: A network meta-analysis. Cephalalgia 2017, 37, 965–978. [Google Scholar] [CrossRef]
- Bednarczuk, N.F.; Lim, M.; Siddiqui, A.; Lascelles, K. Ischemic Stroke Following Ergotamine Overdose. Pediatr. Neurol. 2019, 101, 81–82. [Google Scholar] [CrossRef]
- Machado-Alba, J.E.; Morales-Plaza, C.D. Use of ergotamine: Do physicians in Colombia know how to prescribe it? Neurologia 2014, 29, 280–285. [Google Scholar] [CrossRef]
- Diener, H.C.; Dodick, D.; Evers, S.; Holle, D.; Jensen, R.H.; Lipton, R.B.; Porreca, F.; Silberstein, S.; Schwedt, T. Pathophysiology, prevention, and treatment of medication overuse headache. Lancet Neurol. 2019, 18, 891–902. [Google Scholar] [CrossRef]
- Lee, J.H.; Shewale, A.R.; Barthold, D.; Devine, B. Geographic variation in the use of triptans and opioids for the acute treatment of migraine attacks. Headache 2021, 61, 1499–1510. [Google Scholar] [CrossRef]
- POS Pópuli-Tecnologías, Servicios y Medicamentos de Salud Financiados Con Recursos de la Unidad de Pago por Capitación del SGSSS. Ministerio de Salud de Colombia: Bogotá, Colombia, 2021. Available online: https://pospopuli.minsalud.gov.co/PospopuliWeb/paginas/home.aspx (accessed on 1 March 2023).
- Machado-Duque, M.E.; Ramírez-Valencia, D.M.; Murillo-Muñoz, M.M.; Machado-Alba, J.E. Trends in Opioid Use in a Cohort of Patients with Rheumatoid Arthritis. Pain Res. Manag. 2020, 2020, 3891436. [Google Scholar] [CrossRef]
- Valladales-Restrepo, L.F.; Rubio-Londoño, S.; Poveda-Martinez, L.F.; Machado-Alba, J.E. Prescribing Pattern of Analgesics in Colombia. Are there Differences between Capital Cities and Municipalities? A Cross-Sectional Study. Drugs Real World Outcomes 2022, 9, 487–501. [Google Scholar] [CrossRef]
- Gunasekera, L.; Akhlaghi, H.; Sun-Edelstein, C.; Heywood, J.; Sanders, L. Overuse of opioids for acute migraine in an Australian emergency department. Emerg. Med. Australas. 2020, 32, 763–768. [Google Scholar] [CrossRef]
- Lipton, R.B.; Buse, D.C.; Friedman, B.W.; Feder, L.; Adams, A.M.; Fanning, K.M.; Reed, M.L.; Schwedt, T.J. Characterizing opioid use in a US population with migraine: Results from the CaMEO study. Neurology 2020, 95, e457–e468. [Google Scholar] [CrossRef]
- Kangethe, A.; Polson, M.; Evangelatos, T.M.; Speicher, L.C.; Tenaglia, A.T.; Staats, P.S.; Liebler, E.J.; Mwamburi, M. Real-world assessment of concomitant opioid utilization and associated trends in patients with migraine. Am. J. Manag. Care 2020, 26 (Suppl. S1), S8–S14. [Google Scholar]
- Wang, P.R.; Lopez, R.; Seballos, S.S.; Campbell, M.J.; Udeh, B.L.; Phelan, M.P. Management of migraine in the emergency department: Findings from the 2010–2017 National Hospital Ambulatory Medical Care Surveys. Am. J. Emerg. Med. 2021, 41, 40–45. [Google Scholar] [CrossRef]
- Charles, A. Migraine. N. Engl. J. Med. 2017, 377, 553–561. [Google Scholar] [CrossRef]
- Swenson, C.W.; Kamdar, N.S.; Seiler, K.; Morgan, D.M.; Lin, P.; As-Sanie, S. Definition development and prevalence of new persistent opioid use following hysterectomy. Am. J. Obstet. Gynecol. 2018, 219, 486-e1. [Google Scholar] [CrossRef]
- Friedman, B.W.; West, J.; Vinson, D.R.; Minen, M.T.; Restivo, A.; Gallagher, E.J. Current management of migraine in US emergency departments: An analysis of the National Hospital Ambulatory Medical Care Survey. Cephalalgia 2015, 35, 301–309+27. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Frequency | % |
|---|---|---|
| Sociodemographic | ||
| Female—No. (%) | 5131 | 81.3 |
| Age in years (Mean, SD) | 35.5 ± 12.3 | |
| Male–Female age (mean, SD) | 35.2 (12.7)–35.5 (12.1) | |
| Age Group—No. | ||
| Age 14–30 years | 2425 | 38.4 |
| Age 30–45 years | 2540 | 40.3 |
| Age 45–60 years | 1095 | 17.4 |
| Age > 60 years | 249 | 3.9 |
| Admission diagnoses | ||
| Migraine, unspecified | 3633 | 57.6 |
| Migraine without aura | 807 | 12.8 |
| Migraine with aura [classical migraine] | 606 | 9.6 |
| Status migrainosus | 481 | 7.6 |
| Complicated migraine | 401 | 6.4 |
| Other migraine | 381 | 6.0 |
| Medication Used | Frequency | % | Most Used Presentation | Dose (Median) | DDD * |
|---|---|---|---|---|---|
| Non-specific analgesics | |||||
| Naproxen | 1823 | 28.9 | 250 mg tablet | 750 mg | 1.5 |
| Acetaminophen | 946 | 15.0 | 500 mg tablet | 1500 mg | 0.5 |
| Diclofenac (ampule) | 806 | 12.8 | 75 mg amp | 75 mg | 0.75 |
| Dipyrone | 401 | 6.4 | 1 gr amp | 1 g | 0.33 |
| Ibuprofen | 355 | 5.6 | 400 mg tablet | 1200 mg | 1.0 |
| Diclofenac (tablet) | 168 | 2.7 | 50 mg tablet | 125 mg | 1.25 |
| Celecoxib | 1 | 0.02 | 200 mg tablet | 200 mg | 1.0 |
| Opioids | |||||
| Tramadol | 433 | 6.9 | 50 mg amp | 40 mg | 0.13 |
| Meperidine | 6 | 0.1 | 100 mg amp | 100 mg | 0.25 |
| Morphine | 2 | 0.03 | 10 mg tablet | 10 mg | 0.33 |
| Oxycodone | 1 | 0.02 | 10 mg tablet | 20 mg | 0.26 |
| Acetaminophen/Codeine | 908 | 14.4 | Tablet 325 + 8 mg | 650 + 16 mg | 0.2 + 1 |
| Specific antimigraine drugs | |||||
| Ergotamine + caffeine | 1972 | 31.3 | Tablet 1 + 100 mg | 1 mg | 0.25 |
| Naratriptan | 125 | 2.0 | 2.5 mg tablet | 2.5 mg | 1.0 |
| Sumatriptan | 103 | 1.6 | 50 mg tablet | 50 mg | 1.0 |
| Zolmitriptan | 14 | 0.2 | Nasal Sol. 5 mg/dose | 7 mg | 2.8 |
| Eletriptan | 2 | 0.03 | 40 mg tablet | 40 mg | 1.0 |
| Antiemetics | |||||
| Metoclopramide | 731 | 11.6 | 10 mg tablet | 10 mg | 0.33 |
| Ondansetron | 42 | 0.7 | Amp 4 mg | 4 mg | 0.25 |
| Variable | p Value | OR Adjusted | 95% Confidence Interval | |
|---|---|---|---|---|
| Lower | Upper | |||
| Opioid prescription (index) | <0.001 | 1.65 | 1.41 | 1.93 |
| Acetaminophen (index) | 0.932 | 0.99 | 0.83 | 1.19 |
| NSAIDs (index) | 0.850 | 1.01 | 0.88 | 1.16 |
| Dipyrone (index) | 0.168 | 1.19 | 0.93 | 1.53 |
| Ergotamine + caffeine (index) | 0.953 | 1.00 | 0.86 | 1.17 |
| Triptans (index) | 0.714 | 1.04 | 0.84 | 1.29 |
| Antiemetics (index) | <0.001 | 1.40 | 1.16 | 1.68 |
| Female gender | 0.164 | 1.12 | 0.96 | 1.31 |
| Age 14–30 years | Reference | |||
| Age 30–45 years | <0.001 | 1.56 | 1.36 | 1.79 |
| Age 45–60 years | <0.001 | 1.70 | 1.43 | 2.02 |
| Age > 60 years | <0.001 | 1.97 | 1.46 | 2.66 |
| Bogota-Cundinamarca Region | Reference | |||
| The Caribbean Region | <0.001 | 1.33 | 1.14 | 1.55 |
| Central Region | 0.621 | 1.04 | 0.88 | 1.23 |
| Eastern Region | 0.003 | 0.46 | 0.28 | 0.77 |
| Pacific region | 0.933 | 0.99 | 0.72 | 1.34 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machado-Duque, M.E.; Echeverry-Gutiérrez, M.F.; Gaviria-Mendoza, A.; Valladales-Restrepo, L.F.; Machado-Alba, J.E. Potentially Inappropriate Use of Opioids in the Management of Migraine in Colombia. Biomedicines 2023, 11, 2385. https://doi.org/10.3390/biomedicines11092385
Machado-Duque ME, Echeverry-Gutiérrez MF, Gaviria-Mendoza A, Valladales-Restrepo LF, Machado-Alba JE. Potentially Inappropriate Use of Opioids in the Management of Migraine in Colombia. Biomedicines. 2023; 11(9):2385. https://doi.org/10.3390/biomedicines11092385
Chicago/Turabian StyleMachado-Duque, Manuel E., Maria Fernanda Echeverry-Gutiérrez, Andrés Gaviria-Mendoza, Luis F. Valladales-Restrepo, and Jorge E. Machado-Alba. 2023. "Potentially Inappropriate Use of Opioids in the Management of Migraine in Colombia" Biomedicines 11, no. 9: 2385. https://doi.org/10.3390/biomedicines11092385
APA StyleMachado-Duque, M. E., Echeverry-Gutiérrez, M. F., Gaviria-Mendoza, A., Valladales-Restrepo, L. F., & Machado-Alba, J. E. (2023). Potentially Inappropriate Use of Opioids in the Management of Migraine in Colombia. Biomedicines, 11(9), 2385. https://doi.org/10.3390/biomedicines11092385