
Potential Role of Selected miRNAs in the Pathogenesis of Autoimmune Thyroid Diseases in Children and Adolescents

 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Assessment of the Thyroid Hormone Concentration and Anti-Thyroid Antibody Titers
2.2. Assessment of miR-15a-5p, miR-126-3p, miR-142-5p, miR-21-5p and miR-150-5p Levels
2.3. Statistical Analysis
3. Results
3.1. Results for miR-15a-5p
3.2. Results for miR-126-3p
3.3. Results for miR-142-5p
3.4. Results for miR-150-5p
3.5. Results for miR-21-5p
4. Discussion
5. Conclusions
- The overexpression of the miR-142-5p molecule occurs in children and adolescents with thyroid diseases.
- Decreased blood levels of miR-15a-5p predispose patients to the formation of focal lesions in the thyroid gland.
- Identifying a lower expression of the miR-126-3p molecule in the blood of children with GD requires careful follow-up for the development of focal lesions in the thyroid gland and evaluation for their potential malignancy.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weetman, A.P. An update on the pathogenesis of Hashimoto’s thyroiditis. Endocrinol. Investig. 2021, 44, 883–890. [Google Scholar] [CrossRef]
- Keefe, G.; Culbreath, K.; Cherella, C.; Smith, J.R.; Zendejas, B.; Shamberger, R.C.; Richman, D.M.; Hollowell, M.L.; Modi, B.P.; Wassner, A.J. Autoimmune Thyroiditis and Risk of Malignacy in Children with Thyroid Nodules. Thyroid 2022, 32, 1109–1117. [Google Scholar] [CrossRef]
- Borysewicz-Sańczyk, H.; Pasławska, M.; Zdrodowska, M.; Sawicka, B.; Pomaski, J.; Handkiewicz-Junak, D.; Krajewska, J.; Czarniecka, A.; Jarząb, B.; Dzięcioł, J.; et al. Childhood thyroid carcinoma- single- centre experience. Endokrynol. Pol. 2021, 72, 676–677. [Google Scholar] [CrossRef]
- Borysewicz-Sańczyk, H.; Sawicka, B.; Bossowski, F.; Dzięcioł, J.; Bossowski, A. Elastographic Evaluation of Thyrodi Nodules in Children and Adolescents with Hashimoto’s Thyroiditis and Nodular Goiter with Reference to Cytological and/or Histopathological Diagnosis. J. Clin. Med. 2022, 11, 6339. [Google Scholar] [CrossRef]
- Borysewicz-Sańczyk, H.; Sawicka, B.; Karny, A.; Bossowski, F.; Marcinkiewicz, K.; Rusak, A.; Dzięcioł, J.; Bossowski, A. Suspected Malignant Thyroid Nodules in Children and Adolescents According to Ultrasound Elastography and Ultrasound-Based Risk Stratification Systems-Experience from One Center. J. Clin. Med. 2022, 11, 1768. [Google Scholar] [CrossRef]
- De Martino, M.; Esposito, F.; Capone, M.; Pallante, P.; Fusco, A. Noncoding RNAs in Thyroid- Follicular-Cell-Derived Carcinomas. Cancers 2022, 14, 3079. [Google Scholar] [CrossRef]
- Jin, Z.Q. MicroRNA targets and biomarker validation for diabetes-associated cardiac fibrosis. Pharmacol. Res. 2021, 174, 105941. [Google Scholar] [CrossRef]
- Liu, L.; Yao, H.; Zhou, X.; Chen, J.; Chen, G.; Shi, X.; Wu, G.; Zhou, G.; He, S. MiR-15a-3p regulates ferroptosis via targeting glutathione peroxidase GPX4 in colorectal cancer. Mol. Carcinog. 2022, 61, 301–310. [Google Scholar] [CrossRef]
- Li, Y.; Li, D.; Yang, Y.; Wang, J. MiR-15a-5p regulates Liver Cancer Cell Migration, Apoptosis and Cell Cycle Progression by Targeting Transcription Factor E2F3. Crit. Rev. Eukaryot. Gene Expr. 2022, 32, 1–10. [Google Scholar] [CrossRef]
- Xu, P.; Wang, Y.; Deng, Z.; Tan, Z.; Pei, X. MicroRNA-15a promotes prostate cancer cell ferroptosis by inhibiting GPX4 expression. Oncol. Lett. 2022, 23, 67. [Google Scholar] [CrossRef]
- Hutter, K.; Rulicke, T.; Szabo, T.G.; Andersen, L.; Villunger, A.; Herzog, S. The miR-15a/16-1 and miR-15b/16-2 clusters regulate early B cell development by limiting Il-7 receptor expression. Front. Immunol. 2022, 13, 967914. [Google Scholar] [CrossRef]
- Liu, Z.; Cheng, C.; Luo, X.; Xia, Q.; Zhang, Y.; Long, X.; Jiang, Q.; Fang, W. Retraction Note: CDK4 and miR-15a comprise an abnormal automodulatory feedback loop stimulating the pathogenesis and inducing chemotherapy resistance in nasopharyngeal carcinoma. BMC Cancer 2021, 21, 273. [Google Scholar] [CrossRef]
- Latchana, N.; DiVincenzo, M.J.; Regan, K.; Abrams, Z.; Zhang, X.; Jacob, N.K.; Gru, A.A.; Fadda, P.; Markowitz, J.; Howard, J.H.; et al. Alterations in patient plasma microRNA expression profiles following resection of metastatic melanoma. Surg. Oncol. 2018, 118, 501–509. [Google Scholar] [CrossRef]
- Yao, J.; Wang, Z.; Cheng, Y.; Ma, C.; Zhong, Y.; Xiao, Y.; Gao, X.; Li, Z. M2 macrophage-derived exosomal microRNAs inhibit cell migration and invasion in gliomas through PI3K/AKT/mTOR signaling pathway. Transl. Med. 2021, 19, 99. [Google Scholar] [CrossRef]
- Borsos, B.N.; Pahi, Z.G.; Ujfalundi, Z.; Sukosd, F.; Nikoleny, A.; Banko, S.; Pankotai-Bodo, G.; Olah-Nemeth, O.; Pankotai, T. BC-miR: Monitoring Breast Cancer-related miRNA Profile in Blood Sera-A Prosperous Approach for Tumor Detection. Cells 2022, 11, 2721. [Google Scholar] [CrossRef]
- Abu-Halima, M.; Oberhoffer, F.S.; Wagner, V.; Abd El Rahman, M.; Jung, A.M.; Zemlin, M.; Rohrer, T.R.; Meese, E.; Abdul-Khaliq, H. MicroRNA-126-3p/5p and Aortic Stiffness in Patients with Turner Syndrome. Children 2022, 9, 1109. [Google Scholar] [CrossRef]
- Xiong, Y.; Kotian, S.; Zeiger, M.A.; Zhang, L.; Kebebew, E. MiR-126-3p Inhibits Thyroid Cancer Cell Growth and Metastasis, and Is Associated with Aggressive Thyroid Cancer. PLoS ONE 2015, 10, e0130496. [Google Scholar] [CrossRef]
- Liu, H.; Ma, G.; Xing, E.; Xu, M.; Song, X.; Zhang, Y. Expression and diagnostic value of miR-142-5p and miR-155-5p in the serum of children with allergic rhinitis. Int. J. Pediatr. Otorhinolaryngol. 2023, 165, 111425. [Google Scholar] [CrossRef]
- Bayomy, N.R.; Alfottoh, W.M.A.; Eldeep, S.A.A.; Mersal, A.M.S.I.M.; El-Bary, H.M.A.A.; El Gayed, E.M.A. Mir-142-5p as an indicator of autoimmune processes in childhood idiopathic nephrotic syndrome and as a part of MicroRNAs expression panels for its diagnosis and prediction of response to steroid treatment. Mol. Immunol. 2022, 141, 21–32. [Google Scholar] [CrossRef]
- Zhang, Y.; Zheng, A. MiR-142-5p promotes retinoblastoma cell proliferation, migration and invasion by targeting PTEN. J. Biochem. 2021, 170, 195–202. [Google Scholar] [CrossRef]
- Carvalho, T.M.; Brasil, G.O.; Jucoski, T.S.; Adamoski, D.; Silveira de Lima, R.; Spautz, C.C.; Anselmi, K.F.; Ozawa, P.M.; Cavalli, I.J.; De Oliveira, J.C.; et al. MicroRNAs miR-142-5p, miR-150-5p, miR-320a-3p, and miR-4433b-5p in Serum and Tissue: Potential Biomarkers in Sporadic Breast Cancer. Front. Genet. 2022, 13, 865472. [Google Scholar] [CrossRef]
- Jahanbani, I.; Al-Abdallah, A.; Ali, R.H.; Al-Brahim, N.; Mojiminiyi, O. Discriminatory miRNAs for the Management of Papillary Thyroid Carcinoma and Noninvasive Follicular Thyroid Neoplasms with Papillary-Like Nuclear Features. Thyroid 2018, 28, 319–327. [Google Scholar] [CrossRef]
- Eldosoky, M.A.; Hammad, R.; Elmadbouly, A.A.; Aglan, R.B.; AbdelHamid, S.G.; Alboraie, M.; Hassan, D.A.; Shaheen, M.A.; Rushdi, A.; Ahmed, R.M.; et al. Diagnostic Significance of hsa-miR-21-5p, hsa-miR-192-5p, hsa-miR-155-5p, hsa-miR-199a-5p Panel and Ratios in Hepatocellular Carcinoma on Top of Liver Cirrhosis in HCV-Infected Patients. Int. J. Mol. Sci. 2023, 24, 3157. [Google Scholar] [CrossRef]
- Wang, J.; Jin, J.; Liang, Y.; Zhang, Y.; Wu, N.; Fan, M.; Zeng, F.; Deng, F. MiR-21-5p/PRKCE axis implicated in immune infiltration and poor prognosis of kidney renal clear cell carcinoma. Front. Genet. 2022, 13, 978840. [Google Scholar] [CrossRef]
- Sultana, A.; Alam, S.; Liu, X.; Sharma, R.; Singla, R.K.; Gundamaraju, R.; Shen, B. Single-cell RNA-seq analysis to identify potential biomarkers for diagnosis, and prognosis of non-small cell lung cancer by using comprehensive bioinformatics approaches. Transl. Oncol. 2023, 27, 101571. [Google Scholar] [CrossRef]
- Constantin, A.; Comarița, I.K.; Alexandru, N.; Filippi, A.; Bojin, F.; Gherghiceanu, M.; Vîlcu, A.; Nemecz, M.; Niculescu, L.S.; Păunescu, V.; et al. Stem cell-derived extracellular vesicles reduce the expression of molecules involved in cardiac hypertrophy-In a model of human-induced pluripotent stem cell-derived cardiomyocytes. Front. Pharmacol. 2022, 13, 1003684. [Google Scholar] [CrossRef]
- Trummer, O.; Foessl, I.; Schweighofer, N.; Arifi, E.; Haudum, C.W.; Reintar, S.; Pilz, S.; Theiler-Schwetz, V.; Trummer, C.; Zirlik, A.; et al. Expression Profiles of miR-22-5p and miR-142-3p Indicate Hashimoto’s Disease and Are related to Thyroid Antibodies. Genes 2022, 13, 171. [Google Scholar] [CrossRef]
- Saberinia, A.; Alinezhad, A.; Jafari, F.; Soltany, S.; Sigari, R.A. Oncogenic miRNAs and target therapies in colorectal cancer. Clin. Chim. Acta 2020, 508, 77–91. [Google Scholar] [CrossRef]
- Lee, K.-S.; Park, H. Machine learning on thyroid disease: A review. Front. Biosci. 2022, 27, 101. [Google Scholar] [CrossRef]
- Hamidi, A.A.; Taghehchian, N.; Basirat, Z.; Zangouei, A.S.; Moghbeli, M. MicroRNAs as the critical regulators of cell migration and invasion in thyroid cancer. Biomark. Res. 2022, 10, 40. [Google Scholar] [CrossRef]
- Aversa, T.; Corrias, A.; Salerno, M.; Tessaris, D.; Di Mase, R.; Valenzise, M.; Corica, D.; De Luca, F.; Wasniewska, M. Five-Year Prospective Evaluation of Thyroid Function Test Evolution in Children with Hashimoto’s Thyroiditis Presenting with Either Euthyroidism or Subclinical Hypothyroidism. Thyroid 2016, 26, 1450–1456. [Google Scholar] [CrossRef]
- Wasniewska, M.; Aversa, T.; Salerno, M.; Corrias, A.; Messina, M.F.; Mussa, A.; Capalbo, D.; De Luca, F.; Valenzise, M. Five-year prospective evaluation of thyroid function in girls with subclinical mild hypothyroidism of different etiology. Eur. J. Endocrinol. 2015, 173, 801–808. [Google Scholar] [CrossRef]
- Lydersen, S.; Fagerland, M.W.; Laake, P. Recommended tests for association in 2 × 2 tables. Statist. Med. 2009, 28, 1159–1175. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. Roy. Stat. Soc. B. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Lewontin, R.C. The interaction of selection and linkage. I. General considerations; heterotic models. Genetics 1964, 49, 49–67. [Google Scholar] [CrossRef]
- R Core Team. A Language and Environment for Statistical Computing, R version 4.2.3; R Foundation for Statistical Computing: Vienna, Austria, 2012; ISBN 3-900051-07-0. Available online: http://www.R.-project.org/(accessed on 15 March 2023).
- Zhu, J.; Zhang, Y.; Zhang, W.; Zhang, W.; Fan, L.; Wang, L.; Liu, Y.; Liu, S.; Guo, Y.; Wang, Y.; et al. MicroRNA-142-5p contributes to Hashimoto’s thyroiditis by targeting CLDN1. J. Transl. Med. 2016, 14, 166. [Google Scholar] [CrossRef]
- Yao, X.; Wang, Y.; Wang, L.; Cao, M.; Chen, A.; Zhang, X. Expression patterns of serum MicroRNAs related to endothelial dysfunction in patietns with subclinical hypothyroidism. Front. Endocrinol. 2022, 13, 981622. [Google Scholar] [CrossRef]
- Jin, J.; Zhang, J.; Xue, Y.; Luo, L.; Wang, S.; Tian, H. MiRNA-15a regulates the proliferation and apoptosis of papillary thyroid carcinoma via regulating AKT pathway. OncoTargets Ther. 2019, 12, 6217–6226. [Google Scholar] [CrossRef]
- Hu, J.; Li, C.; Liu, C.; Zhao, S.; Wang, Y.; Fu, Z. Expressions of miRNAs in papillary thyroid carcinoma and their associations with the clinical characteristics of PTC. Cancer Biomark. 2017, 18, 87–94. [Google Scholar] [CrossRef]
- Jiang, L.; Wu, Z.; Meng, X.; Chu, X.; Huang, H.; Xu, C. LncRNA HOXA-AS2 facilitates tumorigenesis and progression of papillary thyroid cancer by modulating the miR-15a-5p/HOXA3 axis. Hum. Gene Ther. 2019, 30, 618–631. [Google Scholar] [CrossRef]
- Zhang, H.; Cai, Y.; Zheng, L.; Zhang, Z.; Lin, X.; Jiang, N. LncRNA BISPR promotes the progression of thyroid papillary carcinoma by regulating miR-21-5p. Int. J. Immunopathol. Pharmacol. 2018, 32, 2058738418772652. [Google Scholar] [CrossRef]
- Wang, J.; Wu, L.; Jin, Y.; Li, S.; Liu, X. Identification of key miRNAs in papillary thyroid carcinoma based on data mining and bioinformatics methods. Biomed. Rep. 2020, 12, 11–16. [Google Scholar] [CrossRef]
- Wu, F.; Li, F.; Lin, X.; Xu, F.; Cui, R.R.; Zhong, J.Y.; Zhu, T.; Shan, S.K.; Liao, X.B.; Yuan, L.Q.; et al. Exsomes increased angiogensesis in papillary thyroid cancer microenvironment. Endocr. Relat. Cancer 2019, 26, 525–538. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| GD (Mean ± SD) | p^ | HT (Mean ± SD) | p^^ | Nodular Goiter (Mean ± SD) | p^^^ | Control Group | |
|---|---|---|---|---|---|---|---|
| children (female/male) | 25 (15/10) | 26 (20/6) | 20 (15/5) | 17 (8/9) | |||
| age (years) | 14.36 ± 3.6 | NS | 14.18 ± 3.9 | NS | 13.7 ± 2.9 | NS | 12.58 ± 2.6 |
| fT4 (ng/dL) | 12.68 ± 33.5 | p < 0.001 | 1.18 ± 0.24 | p < 0.01 | 2.31 ± 4.2 | NS | 1.55 ± 0.62 |
| fT3 (pg/mL) | 17.99 ± 34.39 | p < 0.001 | 2.54 ± 1.1 | NS | 4.93 ± 0.1 | NS | 3.61 ± 2.12 |
| TSH (mIU/L) | 0.96 ± 0.22 | p < 0.001 | 8.58 ± 20.45 | NS | 2.27 ± 1.54 | NS | 2.16 ± 0.95 |
| anti-TSH (U/L) | 17.84 ± 31.86 | ||||||
| aTG (IU/mL) | 248.3 ± 348.71 | p < 0.02 | 441.96 ± 442.89 | p < 0.001 | 201.78 ± 433.6 | NS | 25.25 ± 22.95 |
| aTPO (IU/mL) | 238.94 ± 182.76 | p < 0.001 | 172.31 ± 121.99 | p < 0.001 | 43.34 ± 33.9 | NS | 23.92 ± 33.9 |
| treatment | methamizole/ b-blocker | l-thyroxine | none |
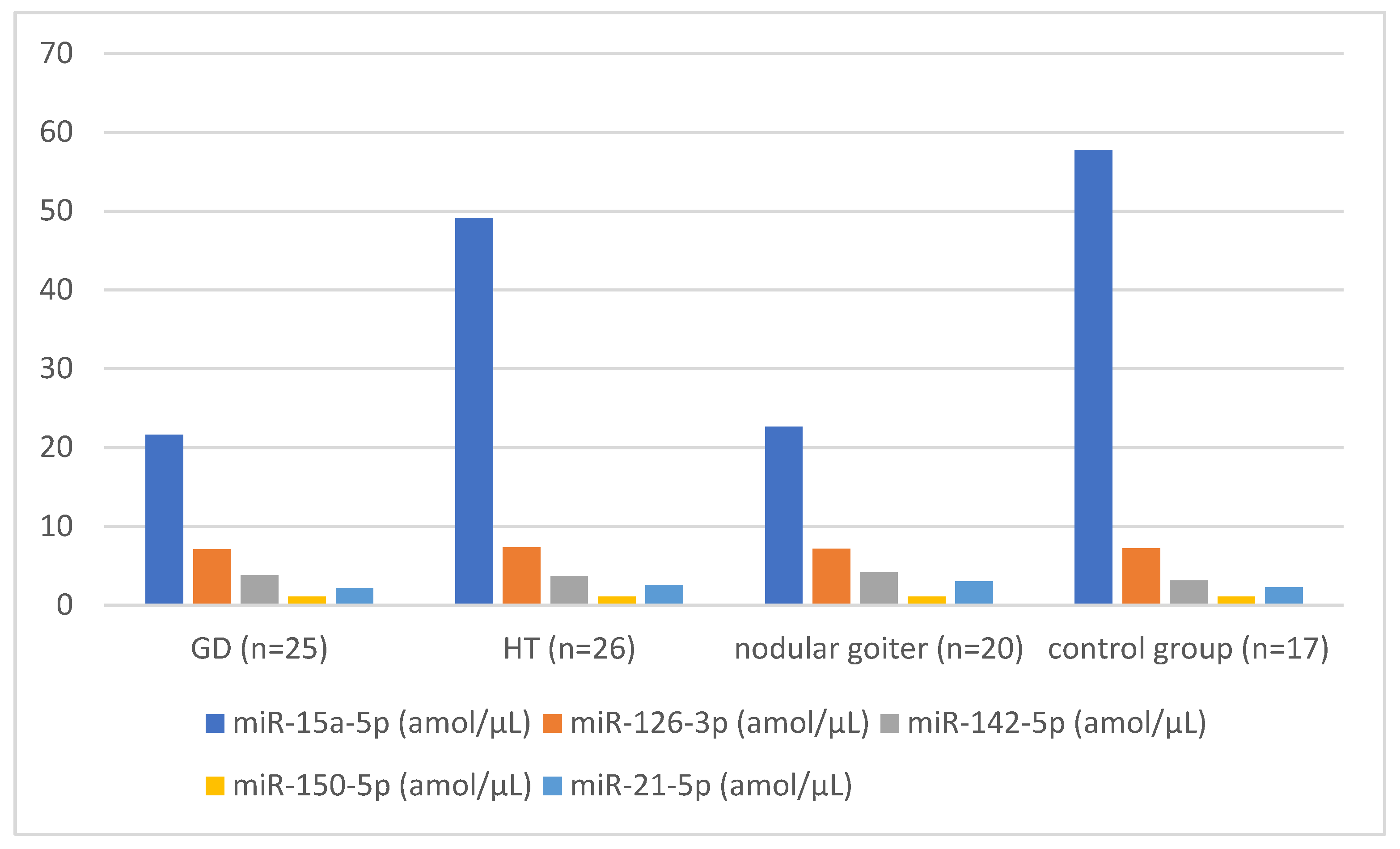
| Patients with GD (n = 25) | Patients with HT (n = 26) | Patients with Nodular Goiter (n = 20) | Control Group (n = 17) | |
|---|---|---|---|---|
| miR-15a-5p amol/µL | 21.61 (p = 0.03) p^ | 49.15 (p = NS) p^^ | 22.63 (p = 0.04) p^^^ | 57.74 |
| miR-126-3p amol/µL | 7.09 (p = 0.02) p^ | 7.31 (p = NS) p^^ | 7.14 (p = NS) p^^^ | 7.24 |
| miR-142-5p amol/µL | 3.80 (p = 0.01) p^ | 3.70 (p = NS) p^^ | 4.16 (p = 0.04) p^^^ | 3.14 |
| miR-150-5p amol/µL | 1.07 (p = NS) p^ | 1.08 (p = NS) p^^ | 1.07 (p = NS) p^^^ | 1.06 |
| miR-21-5p amol/µL | 2.16 (p = NS) p^ | 2.58 (p = NS) p^^ | 3.04 (p = NS) p^^^ | 2.28 |
| Patients with GD (n = 25) | Patients with HT (n = 26) | |
|---|---|---|
| miR-15a-5p | 21.61 amol/µL | 49.15 amol/µL (p = NS) |
| miR-126-3p | 7.09 amol/µL | 7.31 amol/µL (p = NS) |
| miR-142-5p | 3.8 amol/µL | 3.7 amol/µL (p = NS) |
| miR-150-5p | 1.07 amol/µL | 1.08 amol/µL (p = NS) |
| miR-21-5p | 2.16 amol/µL | 2.58 amol/µL (p = NS) |
| miR-150-5p | miR-21-5p | miR-15a-5p | miR-126-3p | miR-142-5p | |
|---|---|---|---|---|---|
| TSH | r = −0.099 p = NS | r = −0.304 p = NS | r = −0.011 p = NS | r = 0.132 p = NS | r = −0.447 p = NS |
| fT4 | r = 0.143 p = NS | r = 0.357 p = NS | r = 0.078 p = NS | r = 0.135 p = NS | r = 0.416 p = NS |
| fT3 | r = 0.188 p = NS | r = 0.1343 p = NS | r = 0.109 p = NS | r = 0.119 p = NS | r = 0.293 p = NS |
| aTG | r = −0.342 p = NS | r = −0.555 p = NS | r = −0.445 p = NS | r = −0.422 p = NS | r = 0.7118 p = NS |
| aTPO | r = 0.429 p = NS | r = 0.081 p = NS | r = −0.892 p = 0.007 | r = −0.648 p = NS | r = −0.188 p = NS |
| TRAb | r = −0.37 p = NS | r = 0.015 p = NS | r = 0.765 p = 0.045 | r = 0.729 p = NS | r = 0.148 p = NS |
| miR-150-5p | miR-21-5p | miR-15a-5p | miR-126-3p | miR-142-5p | |
|---|---|---|---|---|---|
| TSH | r = −0.067 p = NS | r = −0.76 p = NS | r = −0.065 p = NS | r = 0.132 p = NS | r = −0.065 p = NS |
| fT4 | r = 0.037 p = NS | r = 0.029 p = NS | r = 0.212 p = NS | r = 0.035 p = NS | r = 0.011 p = NS |
| aTG | r = 0.098 p = NS | r = 0.087 p = NS | r = 0.261 p = NS | r = 0.100 p = NS | r = 0.077 p = NS |
| aTPO | r = 0.485 p = 0.019 | r = 0.489 p = 0.018 | r = 0.152 p = NS | r = 0.478 p = 0.021 | r = 0.491 p = 0.017 |
| miR-150-5p | miR-21-5p | miR-15a-5p | miR-126-3p | miR-142-5p | |
|---|---|---|---|---|---|
| TSH | r = 0.443 p = NS | r = 0.091 p = NS | r = −0.963 p = NS | r = 0.509 p = NS | r = 0.712 p = NS |
| fT4 | r = 0.859 p = NS | r = −0.086 p = NS | r = −0.662 p = NS | r = 0.895 p = NS | r = 0.976 p = NS |
| fT3 | r = −0.992 p = NS | r = −0.073 p = NS | r = 0.302 p = NS | r = −0.999 p = 0.029 | r = −0.977 p = NS |
| aTG | r = −0.568 p = NS | r = −0.212 p = NS | r = 0.914 p = NS | r = −0.628 p = NS | r = −0.806 p = NS |
| aTPO | r = 0.681 p = NS | r = −0.061 p = NS | r = 0.592 p = 0.007 | r = 0.624 p = NS | r = 0.403 p = NS |
| miR-15a-5p | miR-150-5p | miR-21-5p | miR-126-3p | miR-142-5p | |
|---|---|---|---|---|---|
| miR-15a-5p | r = 1 | r = 0.175 | r = −0.133 | r = 0.018 | r = −0.024 |
| miR-150-5p | r = 0.175 | r = 1 | r = 0.495 | r = −0.133 | r = 0.486 |
| miR-21-5p | r = −0.133 | r = 0.495 | r = 1 | r = 0.28 | r = 0.533 |
| miR-126-3p | r = 0.018 | r = −0.133 | r = 20.8 | r = 1 | r = 0.3 |
| miR-142-5p | r = −0.24 | r = 0.486 | r = 0.533 | r = 0.03 | r = 1 |
| miR-15a-5p | miR-150-5p | miR-21-5p | miR-126-3p | miR-142-5p | |
|---|---|---|---|---|---|
| miR-15a-5p | r = 1 | r = 0.247 | r = −0.023 | r = −0.269 | r = 0.171 |
| miR-150-5p | r = 0.247 | r = 1 | r = 0.555 | r = −0.020 | r = 0.528 |
| miR-21-5p | r = −0.023 | r = 0.555 | r = 1 | r = 0.043 | r = 0.487 |
| miR-126-3p | r = −0.269 | r = −0.02 | r = 0.043 | r = 1 | r = −0.075 |
| miR-142-5p | r = 0.171 | r = 0.528 | r = 0.487 | r = −0.075 | r = 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sawicka, B.; Sulewska, A.; Kulczyńska-Przybik, A.; Bossowski, F.; Dulewicz, M.; Borysewicz-Sańczyk, H.; Mroczko, B.; Nikliński, J.; Bossowski, A. Potential Role of Selected miRNAs in the Pathogenesis of Autoimmune Thyroid Diseases in Children and Adolescents. Biomedicines 2024, 12, 731. https://doi.org/10.3390/biomedicines12040731
Sawicka B, Sulewska A, Kulczyńska-Przybik A, Bossowski F, Dulewicz M, Borysewicz-Sańczyk H, Mroczko B, Nikliński J, Bossowski A. Potential Role of Selected miRNAs in the Pathogenesis of Autoimmune Thyroid Diseases in Children and Adolescents. Biomedicines. 2024; 12(4):731. https://doi.org/10.3390/biomedicines12040731
Chicago/Turabian StyleSawicka, Beata, Anetta Sulewska, Agnieszka Kulczyńska-Przybik, Filip Bossowski, Maciej Dulewicz, Hanna Borysewicz-Sańczyk, Barbara Mroczko, Jacek Nikliński, and Artur Bossowski. 2024. "Potential Role of Selected miRNAs in the Pathogenesis of Autoimmune Thyroid Diseases in Children and Adolescents" Biomedicines 12, no. 4: 731. https://doi.org/10.3390/biomedicines12040731
APA StyleSawicka, B., Sulewska, A., Kulczyńska-Przybik, A., Bossowski, F., Dulewicz, M., Borysewicz-Sańczyk, H., Mroczko, B., Nikliński, J., & Bossowski, A. (2024). Potential Role of Selected miRNAs in the Pathogenesis of Autoimmune Thyroid Diseases in Children and Adolescents. Biomedicines, 12(4), 731. https://doi.org/10.3390/biomedicines12040731