
Pre-Treat Xenogenic Collagenous Blocks of Bone Substitutes with Saline Facilitate Their Manipulation and Guarantee High Bone Regeneration Rates, Qualitatively and Quantitatively


 , and
, and 
Abstract
:1. Introduction
- 1-
- improve the handling and reproducibility of the manual application of the block material due to better malleability and thus compaction range,
- 2-
- increase the quantity of new bone formed,
- 3-
- increase the predictability of the clinical outcome due to homogeneous scaffold conditioning thanks to volumes of NaCl 0.9% easily controlled (when blood availability may be weak and critical on the surgical site.)
- -
- the compression forces as indicators for malleability of the blocks in an in vitro series,
- -
- the amount and kinetics of bone tissue formation from 2 to 12 weeks after implantation by using a rabbit calvarial model.
2. Materials and Methods
2.1. In Vivo Experimental Design
- -
- Each condition was positioned at least once in cylinders OL, OR, FL, FR at each time point.
- -
- Each rabbit had to receive the three conditions at each time point.
- -
- Each control was to be placed on different animals in one of the four cylinders OL, OR, Fl and FR at each time point.
2.2. Bone Substitutes
2.3. Cylinders and Screws
2.4. Animals
2.5. Surgical Procedure
- Pre-anesthesia, im injection: ketamine (25 mg/kg, 50 mg/mL, 0.5 mL/kg, Pfizer, NY, USA) plus xylazin (3 mg/kg, 20 mg/mL, 0.15 mL/kg, Bayer).
- Anesthesia: propofol 2% iv (Braun, Sempach, Switzerland). Animals were then intubated and ventilated with sevoflurane 3% (Abbvie, Chicago, IL, USA) in pure oxygen. Analgesic solution of remifentanil (Bichsel, Unterseen, Switzerland) was continuously perfused iv (ear vein, 0.008–0.5 μm/kg/min, 5 g/mL).
- Surgery: skull was shaved, disinfected with povidone iodine solution 10% (Mundipharma, Frankfurt am Main, Germany) and locally anesthetized (lidocaine 2% sc, Sintetica, Mendrisio, Switzerland). A midsagittal incision was made through the skin and the periosteum which was gently elevated (Figure 1B). Four PEEK cylinders were screwed, five intramedullary holes were drilled under saline irrigation (0.8 mm in diameter, ca. 1 mm in depth) on the calvarium, within the perimeter of each cylinder, according to a precise template (Figure 1E). Cylinders were filled with bone substitutes materials and capped (Figure 1C). The surgical site was closed by using intermittent non-resorbable sutures (Prolene 4.0, Ethicon, Somerville, NJ, USA) (Figure 1D).
- Post-surgical treatment: Analgesia was dispensed by sc injections of Buprenorphine hydrochloride (Reckitt Benckiser, Slough, UK) every 6 h for 3 days (0.02 mg/kg, 0.03 mg/mL, 0.67 mL/kg). Sutures were removed after ca. 10 days of healing.
2.6. Histological Preparation and Histomorphometric Analysis
- -
- sagittal block section into two equal parts,
- -
- three sections with a range of 150 µm and a thickness of 5 µm.
2.7. Mechanical Testing
2.7.1. Venous Blood Collection
2.7.2. Passive Hydration, Semi-Quantitative Colorimetric Evaluation
2.7.3. Malleability: Compression Test
2.8. Statistical Analysis
3. Results
3.1. Mechanical Testing: DBBM-C Malleability
3.2. Clinical Course and Macroscopical Evaluation at Time of Sacrifice
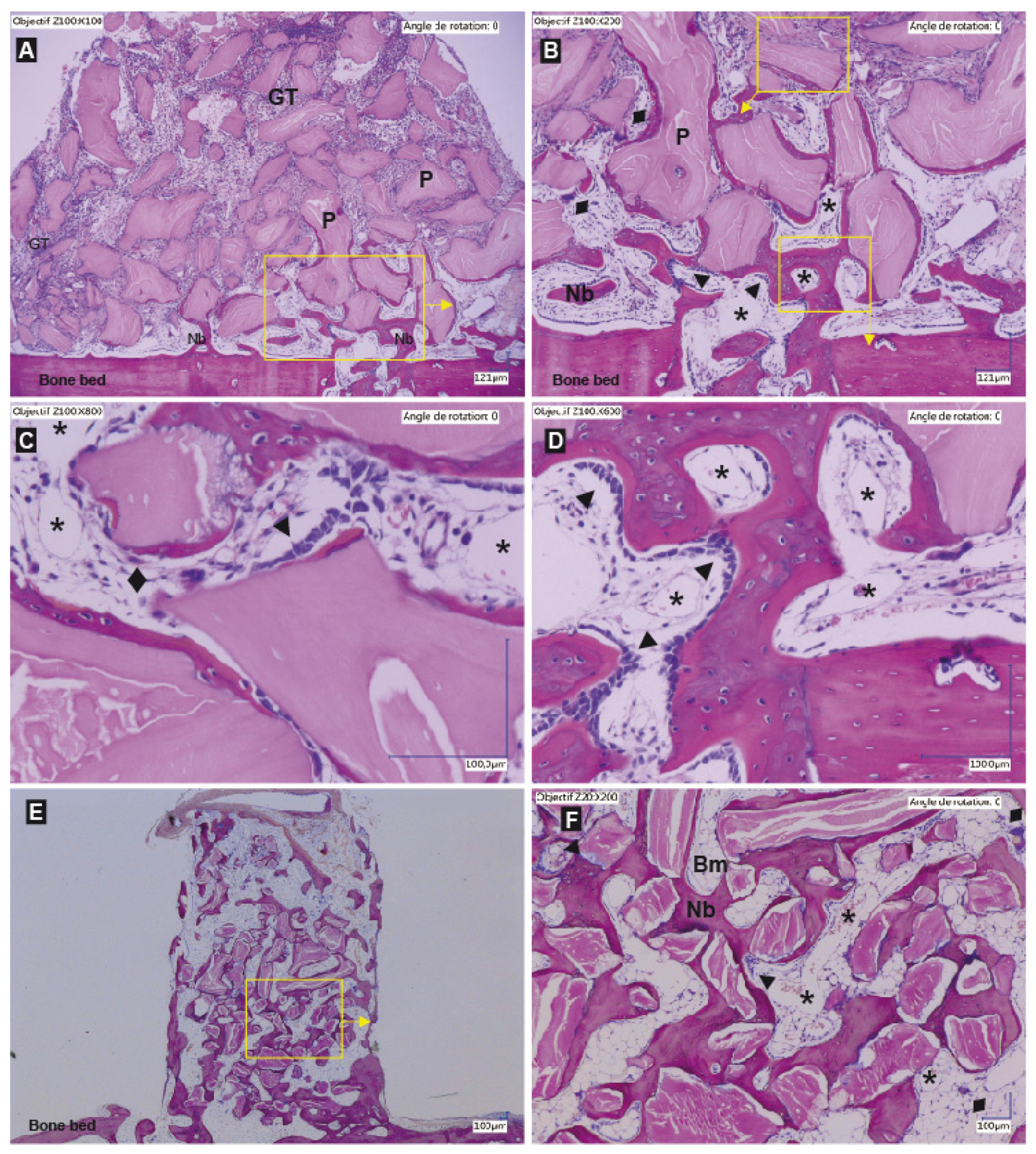
3.3. Histologic Evaluation
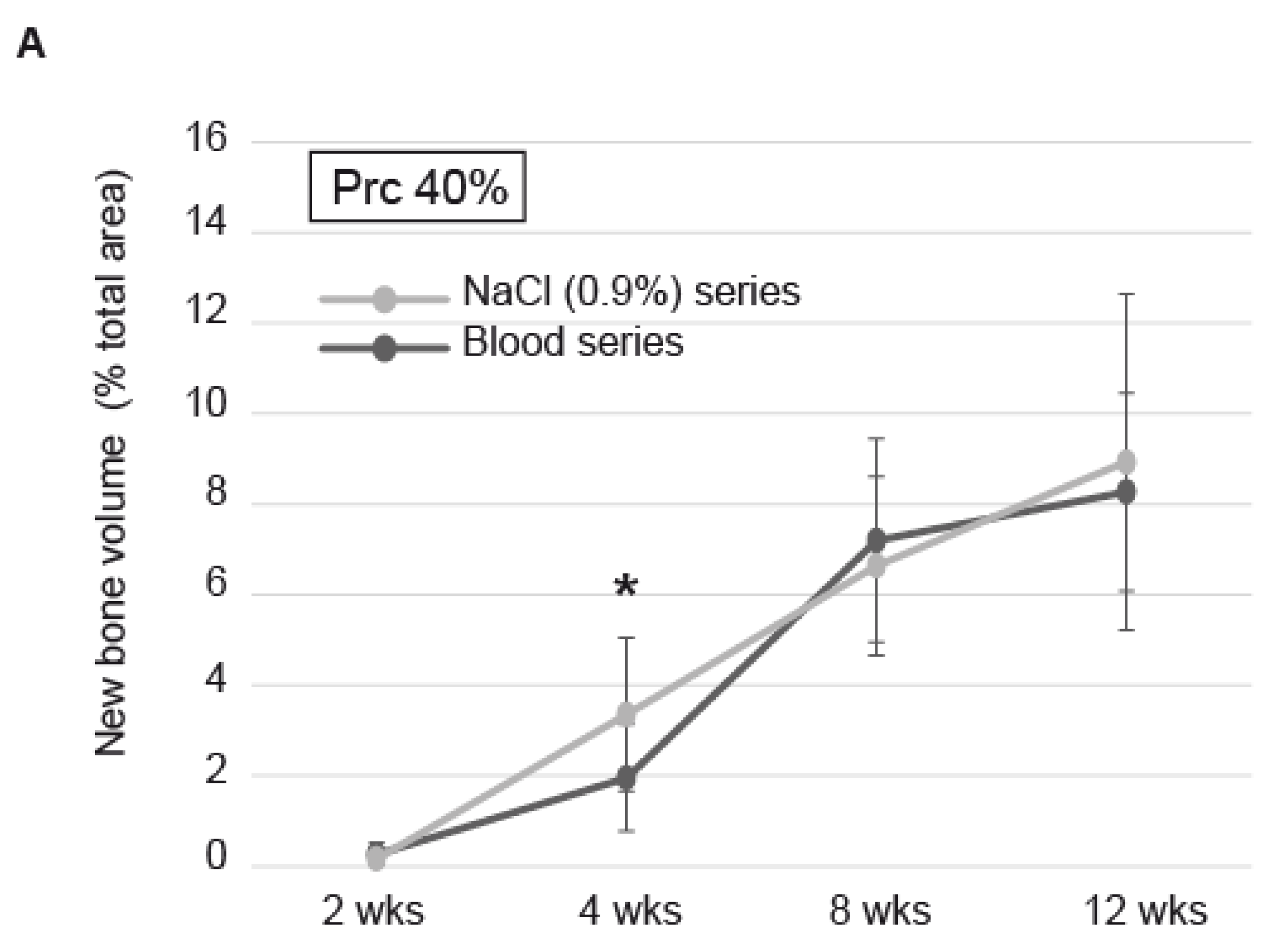
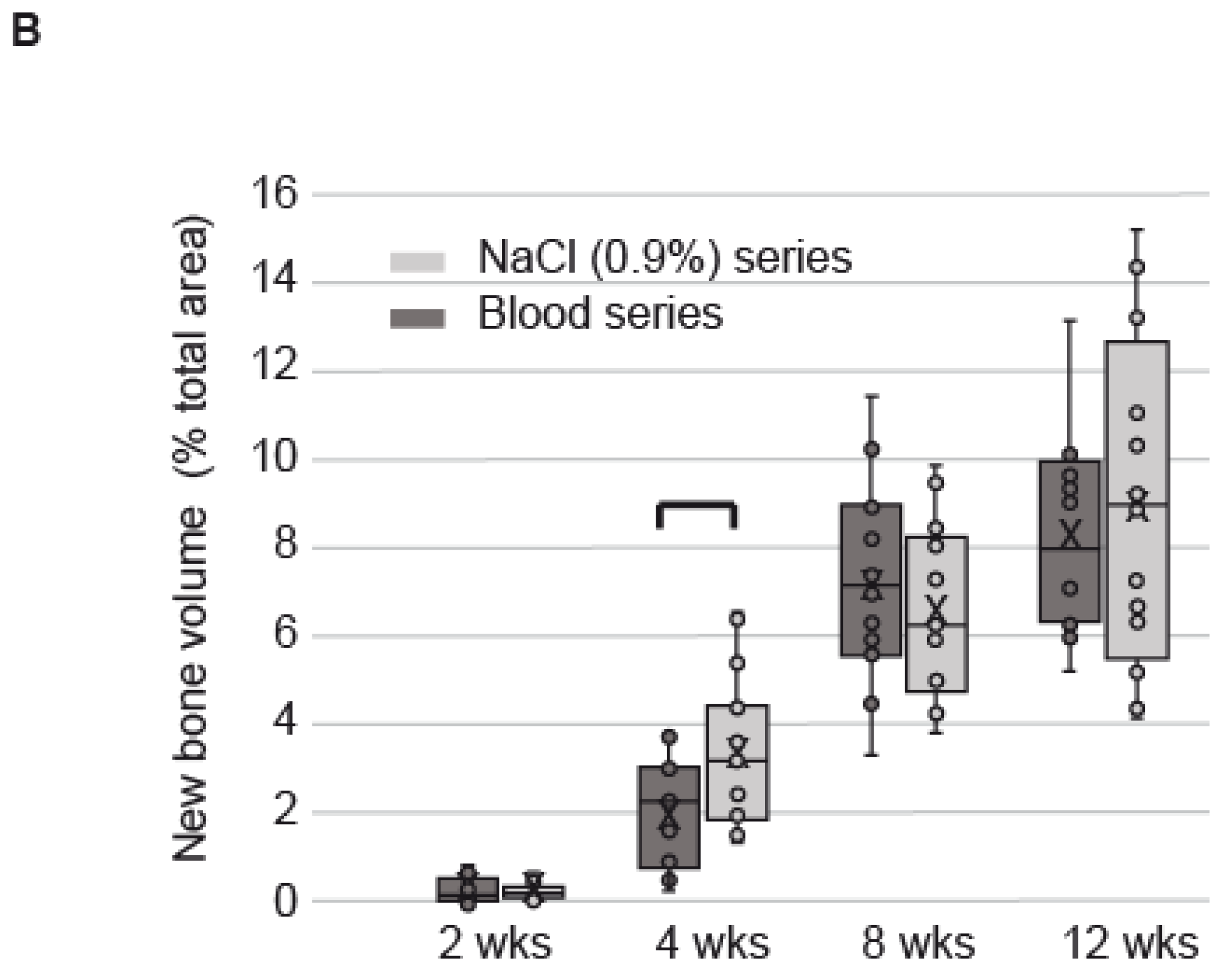
3.4. Histomorphometric Evaluation
4. Discussion
- i.
- Pretreatment with saline leads to better handling of DBBM-C i.e., increased compaction efficiency. The better the compaction the higher the contact area of the DBBM-C material to the surface of the bone and the better the conditions for osseoconduction. The easier the application the better the predictability of the clinical outcome.
- ii.
- Saline respectively serum pre-treatment data clearly indicate a high level of wettability of the DBBM-C blocks. Therefore, serum components as well as bioactive factors from the local environment in vivo must be absorbed to the DBBM-C being pre-treated with blood or saline. Differences in quantity and composition of absorbed serum or local factors may be responsible for the observed acceleration and should be thoroughly investigated.
- iii.
- The finding that erythrocytes interfuse the DBBM-C block completely only after saline treatment in vitro argues for a “blockage” of the erythrocyte in case of using whole blood. The fact that the serum alone penetrates the block completely also argues in that way. However, we have seen that blocks were mixed thoroughly with blood before placement in vivo so that they were fully hydrated and colonized homogeneously by red blood cells. Yet, we observed a delay in the vertical migration of the granulation tissue in blood-soaked blocks as compared to saline, correlated to a delay in bone formation. The same observation i.e., more bone formation in the same time-period in case of saline pre-treatment of biphasic bone substitute granules was reported by Santos et al. [24]. Thus, the observed phenomenon seems to be a general one and cannot be attributed to the composition and structure of DBBM-C alone. We believe that the reason for ours and Santos’ et al. findings may be the influence of saline on blood clotting i.e., fibrinogenesis. In the presence of saline, the activation of fibrinogen should be postponed and the evolving fibrin network less dense simply because of a reduced concentration of fibrinogen and its activators in situ. A postponed fibrinogenesis may increase the distance that erythrocytes may infuse before being trapped in the blood clot. A looser fibrin network will lead to a less rigid final product and thus better malleability and compaction. Moreover, such a loose fibrin network will allow for more rapid cell invasion in particular of polymorphonuclear cells [34] being the forefront of the healing cascade and thus accelerate the healing kinetics. Because collagen is a known activator of fibrinogenesis we predict that the effect of saline pre-treatment on bone formation kinetics will be more pronounced in case of bone substitute materials comprising particles only.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garcia-Gareta, E.; Coathup, M.J.; Blunn, G.W. Osteoinduction of bone grafting materials for bone repair and regeneration. Bone 2015, 81, 112–121. [Google Scholar] [CrossRef]
- Fini, M.; Giardino, R.; Borsari, V.; Torricelli, P.; Rimondini, L.; Giavaresi, G.; Nicoli Aldini, N. In vitro behaviour of osteoblasts cultured on orthopaedic biomaterials with different surface roughness, uncoated and fluorohydroxyapatite-coated, relative to the in vivo osteointegration rate. Int. J. Artif. Organs 2003, 26, 520–528. [Google Scholar] [CrossRef]
- Hollister, S.J.; Lin, C.Y.; Saito, E.; Schek, R.D.; Taboas, J.M.; Williams, J.M.; Partee, B.; Flanagan, C.L.; Diggs, A.; Wilke, E.N.; et al. Engineering craniofacial scaffolds. Orthod. Craniofac. Res. 2005, 8, 162–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, M.; Webster, T.J. Designing orthopedic implant surfaces: Harmonization of nanotopographical and chemical aspects. Nanomedicine 2006, 1, 351–354. [Google Scholar] [CrossRef]
- Seitz, H.; Rieder, W.; Irsen, S.; Leukers, B.; Tille, C. Three-dimensional printing of porous ceramic scaffolds for bone tissue engineering. J. Biomed. Mater. Res. B Appl. Biomater. 2005, 74, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Campana, V.; Milano, G.; Pagano, E.; Barba, M.; Cicione, C.; Salonna, G.; Lattanzi, W.; Logroscino, G. Bone substitutes in orthopaedic surgery: From basic science to clinical practice. J. Mater. Sci. Mater. Med. 2014, 25, 2445–2461. [Google Scholar] [CrossRef] [PubMed]
- Szpalski, C.; Wetterau, M.; Barr, J.; Warren, S.M. Bone tissue engineering: Current strategies and techniques—Part I: Scaffolds. Tissue Eng. Part B Rev. 2012, 18, 246–257. [Google Scholar] [CrossRef]
- Wang, W.; Yeung, K.W.K. Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioact. Mater. 2017, 2, 224–247. [Google Scholar] [CrossRef]
- Ortiz-Puigpelat, O.; Simoes, A.; Caballe-Serrano, J.; Hernandez-Alfaro, F. Blood absorption capacity of different xenograft bone substitutes. An in-vitro study. J. Clin. Exp. Dent. 2019, 11, e1018–e1024. [Google Scholar] [CrossRef]
- Rohner, D.; Hailemariam, S.; Hammer, B. Le Fort I osteotomies using Bio-Oss(R) collagen to promote bony union: A prospective clinical split-mouth study. Int. J. Oral Maxillofac. Surg. 2013, 42, 585–591. [Google Scholar] [CrossRef]
- Trevisiol, L.; Nocini, P.F.; Albanese, M.; Sbarbati, A.; D’Agostino, A. Grafting of large mandibular advancement with a collagen-coated bovine bone (Bio-Oss Collagen) in orthognathic surgery. J. Craniofac. Surg. 2012, 23, 1343–1348. [Google Scholar] [CrossRef] [PubMed]
- Cardaropoli, D.; Tamagnone, L.; Roffredo, A.; Gaveglio, L.; Cardaropoli, G. Socket preservation using bovine bone mineral and collagen membrane: A randomized controlled clinical trial with histologic analysis. Int. J. Periodontics Restor. Dent. 2012, 32, 421–430. [Google Scholar]
- Jung, R.E.; Philipp, A.; Annen, B.M.; Signorelli, L.; Thoma, D.S.; Hammerle, C.H.; Attin, T.; Schmidlin, P. Radiographic evaluation of different techniques for ridge preservation after tooth extraction: A randomized controlled clinical trial. J. Clin. Periodontol. 2012, 40, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Iaquinta, M.R.; Mazzoni, E.; Bononi, I.; Rotondo, J.C.; Mazziotta, C.; Montesi, M.; Sprio, S.; Tampieri, A.; Tognon, M.; Martini, F. Adult Stem Cells for Bone Regeneration and Repair. Front. Cell Dev. Biol. 2019, 7, 268. [Google Scholar] [CrossRef] [Green Version]
- Trajkovski, B.; Jaunich, M.; Muller, W.D.; Beuer, F.; Zafiropoulos, G.G.; Houshmand, A. Hydrophilicity, Viscoelastic, and Physicochemical Properties Variations in Dental Bone Grafting Substitutes. Materials 2018, 11, 215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alayan, J.; Vaquette, C.; Farah, C.; Ivanovski, S. A histomorphometric assessment of collagen-stabilized anorganic bovine bone mineral in maxillary sinus augmentation—A prospective clinical trial. Clin. Oral Implant. Res. 2015, 27, 850–858. [Google Scholar] [CrossRef]
- Alkan, E.A.; Parlar, A.; Yildirim, B.; Senguven, B. Histological comparison of healing following tooth extraction with ridge preservation using enamel matrix derivatives versus Bio-Oss Collagen: A pilot study. Int. J. Oral Maxillofac. Surg. 2013, 42, 1522–1528. [Google Scholar] [CrossRef]
- Araujo, M.G.; da Silva, J.C.; de Mendonca, A.F.; Lindhe, J. Ridge alterations following grafting of fresh extraction sockets in man. A randomized clinical trial. Clin. Oral Implant. Res. 2014, 26, 407–412. [Google Scholar] [CrossRef]
- Jung, R.E.; Hammerle, C.H.; Kokovic, V.; Weber, F.E. Bone regeneration using a synthetic matrix containing a parathyroid hormone peptide combined with a grafting material. Int. J. Oral. Maxillofac. Implant. 2007, 22, 258–266. [Google Scholar]
- Schneider, D.; Schmidlin, P.R.; Philipp, A.; Annen, B.M.; Ronay, V.; Hammerle, C.H.; Attin, T.; Jung, R.E. Labial soft tissue volume evaluation of different techniques for ridge preservation after tooth extraction: A randomized controlled clinical trial. J. Clin. Periodontol. 2014, 41, 612–617. [Google Scholar] [CrossRef] [Green Version]
- Heberer, S.; Al-Chawaf, B.; Hildebrand, D.; Nelson, J.J.; Nelson, K. Histomorphometric analysis of extraction sockets augmented with Bio-Oss Collagen after a 6-week healing period: A prospective study. Clin. Oral Implant. Res. 2008, 19, 1219–1225. [Google Scholar] [CrossRef] [PubMed]
- Heberer, S.; Al-Chawaf, B.; Jablonski, C.; Nelson, J.J.; Lage, H.; Nelson, K. Healing of ungrafted and grafted extraction sockets after 12 weeks: A prospective clinical study. Int. J. Oral Maxillofac. Implant. 2012, 26, 385–392. [Google Scholar]
- Heinemann, F.; Hasan, I.; Schwahn, C.; Bourauel, C.; Mundt, T. Bone level change of extraction sockets with Bio-Oss collagen and implant placement: A clinical study. Ann. Anat. 2012, 194, 508–512. [Google Scholar] [CrossRef]
- Santos, I.; de Santana, C.M.M.; Alves, A.; de Uzeda, M.; Calasans-Maia, M.D.; de Santana, R.B. Effects of methods of hydration of a biphasic ceramic graft on bone regeneration of extraction socket defects. J. Periodontol. 2019, 90, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Marger, L.; Barone, A.; Martinelli-Klay, C.P.; Schaub, L.; Strasding, M.; Mekki, M.; Sailer, I.; Scherrer, S.S.; Durual, S. Calvarial Model of Bone Augmentation in Rabbit for Assessment of Bone Growth and Neovascularization in Bone Substitution Materials. J. Vis. Exp. 2019, 13, e59976. [Google Scholar] [CrossRef]
- Sugiyama, T.; Lama, S.; Gan, L.S. Forces of Tool-Tissue Interaction to Assess Surgical Skill Level. JAMA Surg. 2018, 153, 234–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordaro, L.; Terheyden, H. Ridge Augmentation Procedures in Implant Patients: A Staged Approach. In ITI Treatment Guide; Wismeijer, D., Chen, S., Buser, D., Eds.; Quintessence: Berlin, Germany, 2014; Volume 7. [Google Scholar]
- Pearce, A.I.; Richards, R.G.; Milz, S.; Schneider, E.; Pearce, S.G. Animal models for implant biomaterial research in bone: A review. Eur. Cell Mater. 2007, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Polo, C.I.; Lima, J.L.; De Lucca, L.; Piacezzi, C.B.; Naclerio-Homem Mda, G.; Arana-Chavez, V.E.; Sendyk, W.R. Effect of recombinant human bone morphogenetic protein 2 associated with a variety of bone substitutes on vertical guided bone regeneration in rabbit calvarium. J. Periodontol. 2013, 84, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Carrel, J.P.; Wiskott, A.; Moussa, M.; Rieder, P.; Scherrer, S.; Durual, S. A 3D printed TCP/HA structure as a new osteoconductive scaffold for vertical bone augmentation. Clin. Oral Implant. Res. 2016, 27, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Moussa, M.; Carrel, J.P.; Scherrer, S.; Cattani-Lorente, M.; Wiskott, A.; Durual, S. Medium-Term Function of a 3D Printed TCP/HA Structure as a New Osteoconductive Scaffold for Vertical Bone Augmentation: A Simulation by BMP-2 Activation. Materials 2015, 8, 2174–2190. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.J.; Shin, H.S.; Shin, S.W. Effect of bone block graft with rhBMP-2 on vertical bone augmentation. Int. J. Oral Maxillofac. Surg. 2010, 39, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Tamimi, F.M.; Torres, J.; Tresguerres, I.; Clemente, C.; Lopez-Cabarcos, E.; Blanco, L.J. Bone augmentation in rabbit calvariae: Comparative study between Bio-Oss and a novel beta-TCP/DCPD granulate. J. Clin. Periodontol. 2006, 33, 922–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanson, A.J.; Quinn, M.T. Effect of fibrin sealant composition on human neutrophil chemotaxis. J. Biomed. Mater. Res. 2002, 61, 474–481. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bone Regeneration Period | |||||
|---|---|---|---|---|---|
| Samples | 2 wks | 4 wks | 8 wks | 12 wks | Total |
| Sham blood coagulum | 4 | 4 | 4 | 4 | Placement 64 Analyzed 64 |
| DBBM-C–NaCl 0.9% | 6 | 6 | 6 | 6 | |
| DBBM-C–Blood | 6 | 6 | 6 | 6 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durual, S.; Schaub, L.; Mekki, M.; Manoil, D.; Martinelli-Kläy, C.P.; Sailer, I.; Scherrer, S.S.; Marger, L. Pre-Treat Xenogenic Collagenous Blocks of Bone Substitutes with Saline Facilitate Their Manipulation and Guarantee High Bone Regeneration Rates, Qualitatively and Quantitatively. Biomedicines 2021, 9, 308. https://doi.org/10.3390/biomedicines9030308
Durual S, Schaub L, Mekki M, Manoil D, Martinelli-Kläy CP, Sailer I, Scherrer SS, Marger L. Pre-Treat Xenogenic Collagenous Blocks of Bone Substitutes with Saline Facilitate Their Manipulation and Guarantee High Bone Regeneration Rates, Qualitatively and Quantitatively. Biomedicines. 2021; 9(3):308. https://doi.org/10.3390/biomedicines9030308
Chicago/Turabian StyleDurual, Stephane, Leandra Schaub, Mustapha Mekki, Daniel Manoil, Carla P. Martinelli-Kläy, Irena Sailer, Susanne S. Scherrer, and Laurine Marger. 2021. "Pre-Treat Xenogenic Collagenous Blocks of Bone Substitutes with Saline Facilitate Their Manipulation and Guarantee High Bone Regeneration Rates, Qualitatively and Quantitatively" Biomedicines 9, no. 3: 308. https://doi.org/10.3390/biomedicines9030308
APA StyleDurual, S., Schaub, L., Mekki, M., Manoil, D., Martinelli-Kläy, C. P., Sailer, I., Scherrer, S. S., & Marger, L. (2021). Pre-Treat Xenogenic Collagenous Blocks of Bone Substitutes with Saline Facilitate Their Manipulation and Guarantee High Bone Regeneration Rates, Qualitatively and Quantitatively. Biomedicines, 9(3), 308. https://doi.org/10.3390/biomedicines9030308