
Current FDA-Approved Therapies for High-Grade Malignant Gliomas

Abstract
:1. Introduction
2. Standard of Care
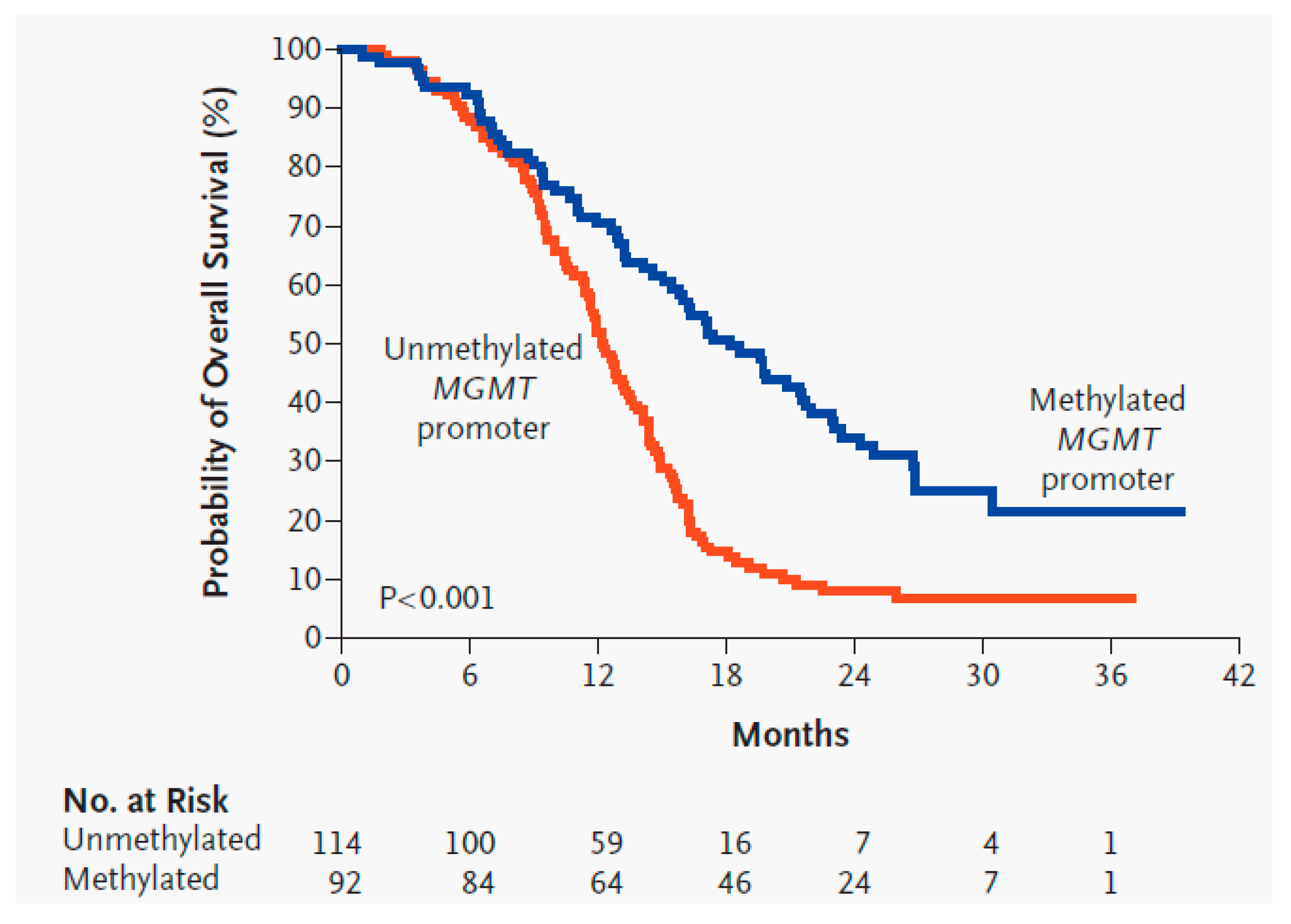
O6-Methylguanine DNA Methyltransferase Activity Predicts SOC Treatment Response
3. FDA-Approved Therapies
3.1. Lomustine
3.2. Carmustine
3.3. Carmustine Wafer Implants
3.4. Bevacizumab
3.5. Tumor Treatment Fields
3.6. 5-Aminolevulinic Acid
4. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostrom, Q.T.; Gittleman, H.; Liao, P.; Rouse, C.; Chen, Y.; Dowling, J.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2007–2011. Neuro Oncol. 2014, 16, iv1–iv63. [Google Scholar] [CrossRef] [PubMed]
- Survival Rates for Selected Adult Brain and Spinal Cord Tumors. Available online: https://www.cancer.org/cancer/brain-spinal-cord-tumors-adults/detection-diagnosis-staging/survival-rates.html (accessed on 30 September 2020).
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, C.; Costa, A.; Osório, L.; Lago, R.C.; Linhares, P.; Carvalho, B.; Caeiro, C. Current standards of care in glioblastoma therapy. In Glioblastoma; De Vleeschouwer, S., Ed.; Codon Publications: Brisbane, Australia, 2017; Chapter 11. [Google Scholar]
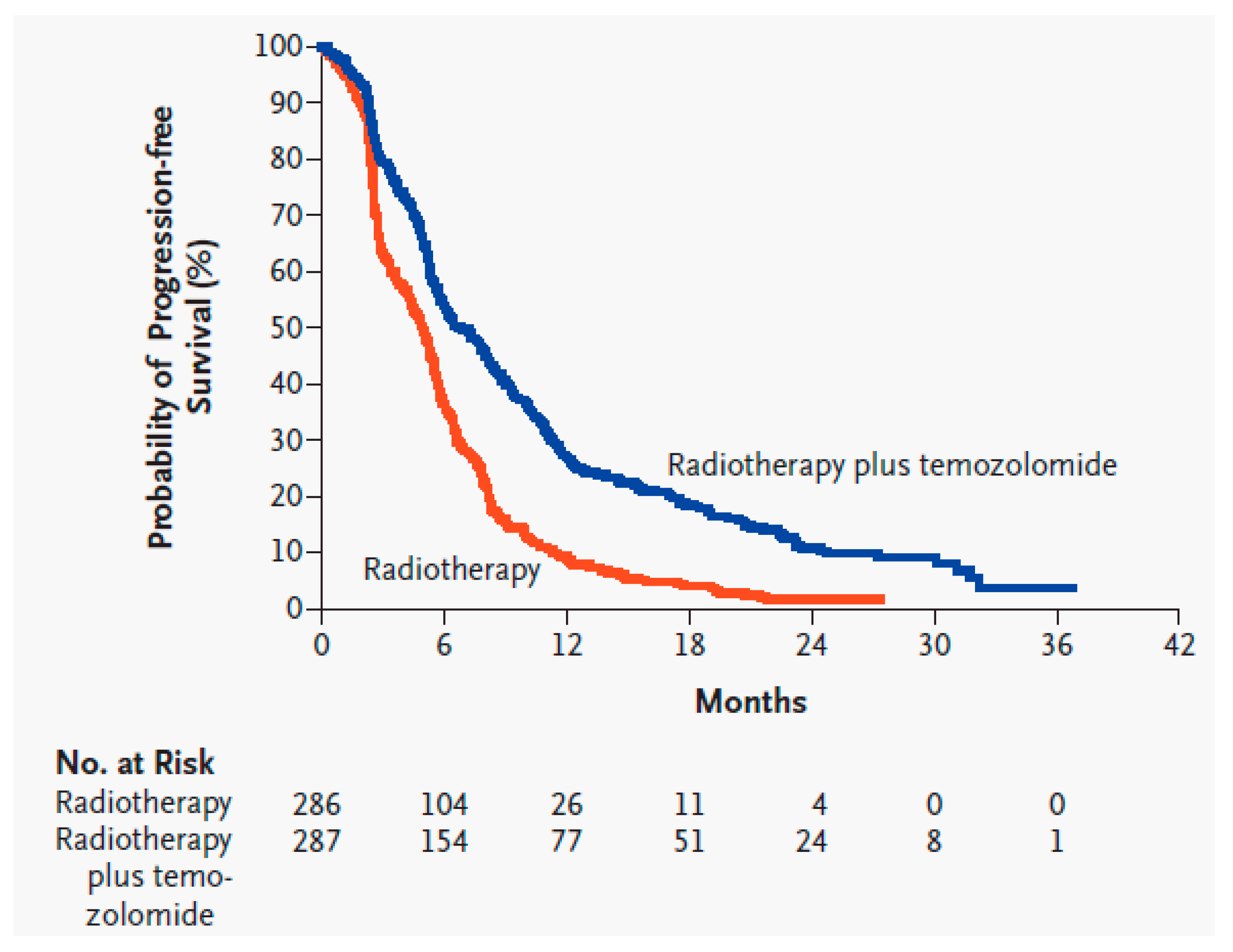
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Lara-Velazquez, M.; Al-Kharboosh, R.; Jeanneret, S.; Vazquez-Ramos, C.; Mahato, D.; Tavanaiepour, D.; Rahmathulla, G.; Quinones-Hinojosa, A. Advances in Brain Tumor Surgery for Glioblastoma in Adults. Brain Sci. 2017, 7, 166. [Google Scholar] [CrossRef] [Green Version]
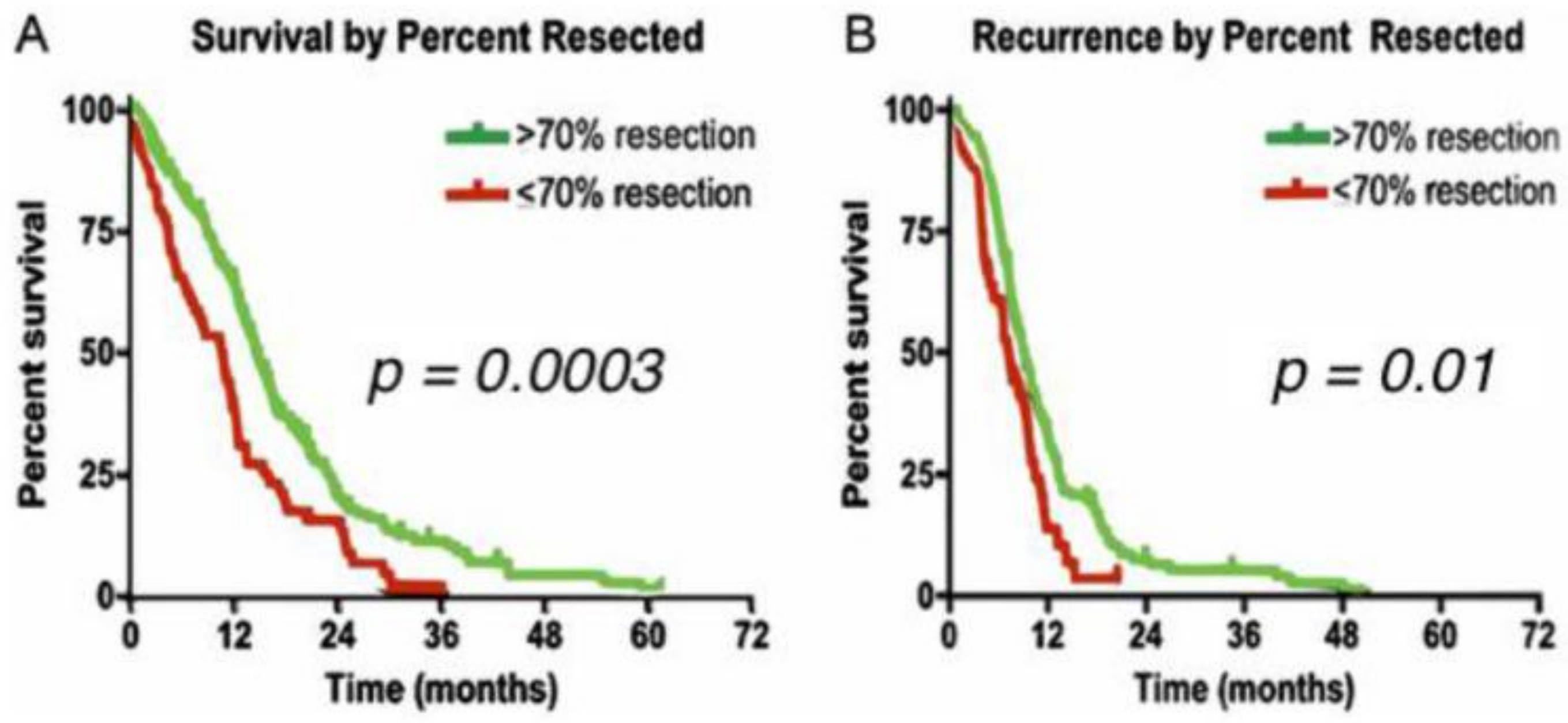
- Lacroix, M.; Abi-Said, D.; Fourney, D.R.; Gokaslan, Z.L.; Shi, W.; DeMonte, F.; Lang, F.F.; McCutcheon, I.E.; Hassenbusch, S.J.; Holland, E.; et al. A multivariate analysis of 416 patients with glioblastoma multiforme: Prognosis, extent of resection, and survival. J. Neurosurg. 2001, 95, 190–198. [Google Scholar] [CrossRef] [Green Version]
- Chaichana, K.L.; Jusue-Torres, I.; Navarro-Ramirez, R.; Raza, S.M.; Pascual-Gallego, M.; Ibrahim, A.; Hernandez-Hermann, M.; Gomez, L.; Ye, X.; Weingart, J.D.; et al. Establishing percent resection and residual volume thresholds affecting survival and recurrence for patients with newly diagnosed intracranial glioblastoma. Neuro Oncol. 2014, 16, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Bleehen, N.M.; Stenning, S.P. A Medical Research Council trial of two radiotherapy doses in the treatment of grades 3 and 4 astrocytoma. The Medical Research Council Brain Tumour Working Party. Br. J. Cancer 1991, 64, 769–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsao, M.N.; Mehta, M.P.; Whelan, T.J.; Morris, D.E.; Hayman, J.A.; Flickinger, J.C.; Mills, M.; Rogers, C.L.; Souhami, L. The American Society for Therapeutic Radiology and Oncology (ASTRO) evidence-based review of the role of radiosurgery for malignant glioma. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Hingorani, M.; Colley, W.P.; Dixit, S.; Beavis, A.M. Hypofractionated radiotherapy for glioblastoma: Strategy for poor-risk patients or hope for the future? Br. J. Radiol. 2012, 85, e770–e781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minniti, G.; Lombardi, G.; Paolini, S. Glioblastoma in Elderly Patients: Current Management and Future Perspectives. Cancers 2019, 11, 336. [Google Scholar] [CrossRef] [Green Version]
- Malmström, A.; Grønberg, B.H.; Marosi, C.; Stupp, R.; Frappaz, D.; Schultz, H.; Abacioglu, U.; Tavelin, B.; Lhermitte, B.; Hegi, M.E.; et al. Temozolomide versus standard 6-week radiotherapy versus hypofractionated radiotherapy in patients older than 60 years with glioblastoma: The Nordic randomised, phase 3 trial. Lancet Oncol. 2012, 13, 916–926. [Google Scholar] [CrossRef]
- Ohno, M.; Miyakita, Y.; Takahashi, M.; Igaki, H.; Matsushita, Y.; Ichimura, K.; Narita, Y. Survival benefits of hypofractionated radiotherapy combined with temozolomide or temozolomide plus bevacizumab in elderly patients with glioblastoma aged ≥ 75 years. Radiat. Oncol. 2019, 14, 200. [Google Scholar] [CrossRef] [Green Version]
- Perry, J.R.; Laperriere, N.; O’Callaghan, C.J.; Brandes, A.A.; Menten, J.; Phillips, C.; Fay, M.; Nishikawa, R.; Cairncross, J.G.; Roa, W.; et al. Short-Course Radiation plus Temozolomide in Elderly Patients with Glioblastoma. N. Engl. J. Med. 2017, 376, 1027–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hegi, M.E.; Diserens, A.C.; Gorlia, T.; Hamou, M.F.; de Tribolet, N.; Weller, M.; Kros, J.M.; Hainfellner, J.A.; Mason, W.; Mariani, L.; et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N. Engl. J. Med. 2005, 352, 997–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumenthal, D.T.; Gorlia, T.; Gilbert, M.R.; Kim, M.M.; Burt Nabors, L.; Mason, W.P.; Hegi, M.E.; Zhang, P.; Golfinopoulos, V.; Perry, J.R.; et al. Is more better? The impact of extended adjuvant temozolomide in newly diagnosed glioblastoma: A secondary analysis of EORTC and NRG Oncology/RTOG. Neuro Oncol. 2017, 19, 1119–1126. [Google Scholar] [CrossRef]
- Athanassiou, H.; Synodinou, M.; Maragoudakis, E.; Paraskevaidis, M.; Verigos, C.; Misailidou, D.; Antonadou, D.; Saris, G.; Beroukas, K.; Karageorgis, P. Randomized phase II study of temozolomide and radiotherapy compared with radiotherapy alone in newly diagnosed glioblastoma multiforme. J. Clin. Oncol. 2005, 23, 2372–2377. [Google Scholar] [CrossRef]
- Szczepanek, D.; Marchel, A.; Moskała, M.; Krupa, M.; Kunert, P.; Trojanowski, T. Efficacy of concomitant and adjuvant temozolomide in glioblastoma treatment: A multicentre randomized study. Neurol. Neurochir. Pol. 2013, 47, 101–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karacetin, D.; Okten, B.; Yalcin, B.; Incekara, O. Concomitant temozolomide and radiotherapy versus radiotherapy alone for treatment of newly diagnosed glioblastoma multiforme. J. BU ON Off. J. Balk. Union Oncol. 2011, 16, 133–137. [Google Scholar]
- Feng, E.; Sui, C.; Wang, T.; Sun, G. Temozolomide with or without Radiotherapy in Patients with Newly Diagnosed Glioblastoma Multiforme: A Meta-Analysis. Eur. Neurol. 2017, 77, 201–210. [Google Scholar] [CrossRef]
- Sharma, S.; Salehi, F.; Scheithauer, B.W.; Rotondo, F.; Syro, L.V.; Kovacs, K. Role of MGMT in tumor development, progression, diagnosis, treatment and prognosis. Anticancer Res. 2009, 29, 3759–3768. [Google Scholar]
- Test ID: MGMTMGMT Promoter Methylation, Tumor. Available online: https://www.mayocliniclabs.com/test-catalog/Clinical+and+Interpretive/36733 (accessed on 30 September 2020).
- Yin, A.A.; Zhang, L.H.; Cheng, J.X.; Dong, Y.; Liu, B.L.; Han, N.; Zhang, X. The predictive but not prognostic value of MGMT promoter methylation status in elderly glioblastoma patients: A meta-analysis. PLoS ONE 2014, 9, e85102. [Google Scholar] [CrossRef] [Green Version]
- Hadjipanayis, C.G.; Stummer, W. 5-ALA and FDA approval for glioma surgery. J. Neurooncol. 2019, 141, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Current Treatments for Brain Tumors. Available online: https://braintumor.org/wp-content/assets/2017_NBTS_CurrentTreatmentOptions_083017.pdf (accessed on 30 September 2020).
- Drugs Approved for Brain Tumors. Available online: https://www.cancer.gov/about-cancer/treatment/drugs/brain (accessed on 30 September 2020).
- Davis, M.E. Glioblastoma: Overview of Disease and Treatment. Clin. J. Oncol. Nurs. 2016, 20, S2–S8. [Google Scholar] [CrossRef] [Green Version]
- Bloch, O.; Han, S.J.; Cha, S.; Sun, M.Z.; Aghi, M.K.; McDermott, M.W.; Berger, M.S.; Parsa, A.T. Impact of extent of resection for recurrent glioblastoma on overall survival: Clinical article. J. Neurosurg. 2012, 117, 1032–1038. [Google Scholar] [CrossRef] [PubMed]
- Brandes, A.A.; Bartolotti, M.; Franceschi, E. Second surgery for recurrent glioblastoma: Advantages and pitfalls. Expert Rev. Anticancer Ther. 2013, 13, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Kazmi, F.; Soon, Y.Y.; Leong, Y.H.; Koh, W.Y.; Vellayappan, B. Re-irradiation for recurrent glioblastoma (GBM): A systematic review and meta-analysis. J. Neurooncol. 2019, 142, 79–90. [Google Scholar] [CrossRef]
- Hochberg, F.H.; Linggood, R.; Wolfson, L.; Baker, W.H.; Kornblith, P. Quality and duration of survival in glioblastoma multiforme. Combined surgical, radiation, and lomustine therapy. JAMA 1979, 241, 1016–1018. [Google Scholar] [CrossRef]
- Walker, M.D.; Alexander, E., Jr.; Hunt, W.E.; MacCarty, C.S.; Mahaley, M.S., Jr.; Mealey, J., Jr.; Norrell, H.A.; Owens, G.; Ransohoff, J.; Wilson, C.B.; et al. Evaluation of BCNU and/or radiotherapy in the treatment of anaplastic gliomas. A cooperative clinical trial. J. Neurosurg. 1978, 49, 333–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westphal, M.; Hilt, D.C.; Bortey, E.; Delavault, P.; Olivares, R.; Warnke, P.C.; Whittle, I.R.; Jääskeläinen, J.; Ram, Z. A phase 3 trial of local chemotherapy with biodegradable carmustine (BCNU) wafers (Gliadel wafers) in patients with primary malignant glioma. Neuro Oncol. 2003, 5, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.H.; Shen, Y.L.; Keegan, P.; Pazdur, R. FDA drug approval summary: Bevacizumab (Avastin) as treatment of recurrent glioblastoma multiforme. Oncologist 2009, 14, 1131–1138. [Google Scholar] [CrossRef]
- Stupp, R.; Taillibert, S.; Kanner, A.A.; Kesari, S.; Steinberg, D.M.; Toms, S.A.; Taylor, L.P.; Lieberman, F.; Silvani, A.; Fink, K.L.; et al. Maintenance Therapy with Tumor-Treating Fields Plus Temozolomide vs. Temozolomide Alone for Glioblastoma: A Randomized Clinical Trial. JAMA 2015, 314, 2535–2543. [Google Scholar] [CrossRef] [PubMed]
- Lomustine. Available online: https://go.drugbank.com/drugs/DB01206 (accessed on 30 September 2020).
- Wirsching, H.G.; Tritschler, I.; Palla, A.; Renner, C.; Weller, M.; Tabatabai, G. The management of lomustine overdose in malignant glioma patients. Neurooncol. Pract. 2014, 1, 178–183. [Google Scholar] [CrossRef]
- Weller, M.; Le Rhun, E. How did lomustine become standard of care in recurrent glioblastoma? Cancer Treat. Rev. 2020, 87, 102029. [Google Scholar] [CrossRef]
- Wick, W.; Gorlia, T.; Bendszus, M.; Taphoorn, M.; Sahm, F.; Harting, I.; Brandes, A.A.; Taal, W.; Domont, J.; Idbaih, A.; et al. Lomustine and Bevacizumab in Progressive Glioblastoma. N. Engl. J. Med. 2017, 377, 1954–1963. [Google Scholar] [CrossRef]
- Lassen, U.; Mau-Sørensen, M.; Poulsen, H.S. Orphan drugs in glioblastoma multiforme: A review. Orphan Drugs Res. Rev. 2014, 4, 83–91. [Google Scholar] [CrossRef] [Green Version]
- Brada, M.; Stenning, S.; Gabe, R.; Thompson, L.C.; Levy, D.; Rampling, R.; Erridge, S.; Saran, F.; Gattamaneni, R.; Hopkins, K.; et al. Temozolomide versus procarbazine, lomustine, and vincristine in recurrent high-grade glioma. J. Clin. Oncol. 2010, 28, 4601–4608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kappelle, A.C.; Postma, T.J.; Taphoorn, M.J.B.; Groeneveld, G.J.; van den Bent, M.J.; van Groeningen, C.J.; Zonnenberg, B.A.; Sneeuw, K.C.A.; Heimans, J.J. PCV chemotherapy for recurrent glioblastoma multiforme. Neurology 2001, 56, 118–120. [Google Scholar] [CrossRef]
- Carmustine. Available online: https://go.drugbank.com/drugs/DB00262 (accessed on 30 September 2020).
- Carmustine (Rx)Brand and Other Names: BiCNU, Gliadel. Available online: https://reference.medscape.com/drug/bicnu-gliadel-carmustine-342194 (accessed on 30 September 2020).
- DRUG NAME: Carmustine. Available online: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/Carmustine%20monograph.pdf (accessed on 30 September 2020).
- Gliadel. Available online: https://www.rxlist.com/gliadel-drug.htm#description (accessed on 30 September 2020).
- Highlights of Prescribing Information. Available online: https://gliadel.com/hcp/media/_pdfs/prescribing-information-gliadel.pdf (accessed on 30 September 2020).
- Bota, D.A.; Desjardins, A.; Quinn, J.A.; Affronti, M.L.; Friedman, H.S. Interstitial chemotherapy with biodegradable BCNU (Gliadel) wafers in the treatment of malignant gliomas. Ther. Clin. Risk Manag. 2007, 3, 707–715. [Google Scholar]
- Attenello, F.J.; Mukherjee, D.; Datoo, G.; McGirt, M.J.; Bohan, E.; Weingart, J.D.; Olivi, A.; Quinones-Hinojosa, A.; Brem, H. Use of Gliadel (BCNU) wafer in the surgical treatment of malignant glioma: A 10-year institutional experience. Ann. Surg. Oncol. 2008, 15, 2887–2893. [Google Scholar] [CrossRef] [PubMed]
- Grossman, R.; Burger, P.; Soudry, E.; Tyler, B.; Chaichana, K.L.; Weingart, J.; Olivi, A.; Gallia, G.L.; Sidransky, D.; Quiñones-Hinojosa, A.; et al. MGMT inactivation and clinical response in newly diagnosed GBM patients treated with Gliadel. J. Clin. Neurosci. 2015, 22, 1938–1942. [Google Scholar] [CrossRef] [PubMed]
- McGirt, M.J.; Than, K.D.; Weingart, J.D.; Chaichana, K.L.; Attenello, F.J.; Olivi, A.; Laterra, J.; Kleinberg, L.R.; Grossman, S.A.; Brem, H.; et al. Gliadel (BCNU) wafer plus concomitant temozolomide therapy after primary resection of glioblastoma multiforme. J. Neurosurg. 2009, 110, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Bregy, A.; Shah, A.H.; Diaz, M.V.; Pierce, H.E.; Ames, P.L.; Diaz, D.; Komotar, R.J. The role of Gliadel wafers in the treatment of high-grade gliomas. Expert Rev. Anticancer Ther. 2013, 13, 1453–1461. [Google Scholar] [CrossRef] [PubMed]
- Bevacizumab. Available online: https://go.drugbank.com/drugs/DB00112 (accessed on 30 September 2020).
- Blumenthal, D.T.; Mendel, L.; Bokstein, F. The optimal regimen of bevacizumab for recurrent glioblastoma: Does dose matter? J. Neurooncol. 2016, 127, 493–502. [Google Scholar] [CrossRef]
- Poulsen, H.S.; Urup, T.; Michaelsen, S.R.; Staberg, M.; Villingshøj, M.; Lassen, U. The impact of bevacizumab treatment on survival and quality of life in newly diagnosed glioblastoma patients. Cancer Manag. Res. 2014, 6, 373–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vredenburgh, J.J.; Desjardins, A.; Herndon, J.E., 2nd; Dowell, J.M.; Reardon, D.A.; Quinn, J.A.; Rich, J.N.; Sathornsumetee, S.; Gururangan, S.; Wagner, M.; et al. Phase II trial of bevacizumab and irinotecan in recurrent malignant glioma. Clin. Cancer Res. 2007, 13, 1253–1259. [Google Scholar] [CrossRef] [Green Version]
- Carrillo, J.A.; Hsu, F.P.; Delashaw, J.; Bota, D. Efficacy and safety of bevacizumab and etoposide combination in patients with recurrent malignant gliomas who have failed bevacizumab. Rev. Health Care 2014, 5, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Mrugala, M.M.; Crew, L.K.; Fink, J.R.; Spence, A.M. Carboplatin and bevacizumab for recurrent malignant glioma. Oncol. Lett. 2012, 4, 1082–1086. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, M.R.; Dignam, J.J.; Armstrong, T.S.; Wefel, J.S.; Blumenthal, D.T.; Vogelbaum, M.A.; Colman, H.; Chakravarti, A.; Pugh, S.; Won, M.; et al. A randomized trial of bevacizumab for newly diagnosed glioblastoma. N. Engl. J. Med. 2014, 370, 699–708. [Google Scholar] [CrossRef] [Green Version]
- Ameratunga, M.; Pavlakis, N.; Wheeler, H.; Grant, R.; Simes, J.; Khasraw, M. Anti-angiogenic therapy for high-grade glioma. Cochrane Database Syst. Rev. 2018, 11, CD008218. [Google Scholar] [CrossRef]
- Lemercier, P.; Paz Maya, S.; Patrie, J.T.; Flors, L.; Leiva-Salinas, C. Gradient of apparent diffusion coefficient values in peritumoral edema helps in differentiation of glioblastoma from solitary metastatic lesions. AJR Am. J. Roentgenol. 2014, 203, 163–169. [Google Scholar] [CrossRef]
- Meng, X.; Zhao, R.; Shen, G.; Dong, D.; Ding, L.; Wu, S. Efficacy and safety of bevacizumab treatment for refractory brain edema: Case report. Medicine 2017, 96, e8280. [Google Scholar] [CrossRef] [PubMed]
- Buboltz, J.B.; Tadi, P. Hyperbaric Treatment of Brain Radiation Necrosis; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Chao, S.T.; Ahluwalia, M.S.; Barnett, G.H.; Stevens, G.H.; Murphy, E.S.; Stockham, A.L.; Shiue, K.; Suh, J.H. Challenges with the diagnosis and treatment of cerebral radiation necrosis. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 449–457. [Google Scholar] [CrossRef]
- Gonzalez, J.; Kumar, A.J.; Conrad, C.A.; Levin, V.A. Effect of bevacizumab on radiation necrosis of the brain. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, H.; Shi, S.; Yuan, Z.; Chang, J.Y. Bevacizumab treatment for radiation brain necrosis: Mechanism, efficacy and issues. Mol. Cancer 2019, 18, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stupp, R.; Taillibert, S.; Kanner, A.; Read, W.; Steinberg, D.; Lhermitte, B.; Toms, S.; Idbaih, A.; Ahluwalia, M.S.; Fink, K.; et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs. Maintenance Temozolomide Alone on Survival in Patients with Glioblastoma: A Randomized Clinical Trial. JAMA 2017, 318, 2306–2316. [Google Scholar] [CrossRef] [Green Version]
- Taphoorn, M.J.B.; Dirven, L.; Kanner, A.A.; Lavy-Shahaf, G.; Weinberg, U.; Taillibert, S.; Toms, S.A.; Honnorat, J.; Chen, T.C.; Sroubek, J.; et al. Influence of Treatment with Tumor-Treating Fields on Health-Related Quality of Life of Patients with Newly Diagnosed Glioblastoma: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2018, 4, 495–504. [Google Scholar] [CrossRef]
- Onken, J.; Staub-Bartelt, F.; Vajkoczy, P.; Misch, M. Acceptance and compliance of TTFields treatment among high grade glioma patients. J. Neurooncol. 2018, 139, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Mehta, M.; Wen, P.; Nishikawa, R.; Reardon, D.; Peters, K. Critical review of the addition of tumor treating fields (TTFields) to the existing standard of care for newly diagnosed glioblastoma patients. Crit. Rev. Oncol. Hematol. 2017, 111, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Hadjipanayis, C.G.; Widhalm, G.; Stummer, W. What is the Surgical Benefit of Utilizing 5-Aminolevulinic Acid for Fluorescence-Guided Surgery of Malignant Gliomas? Neurosurgery 2015, 77, 663–673. [Google Scholar] [CrossRef] [Green Version]
- Stummer, W.; Pichlmeier, U.; Meinel, T.; Wiestler, O.D.; Zanella, F.; Reulen, H.J.; ALA-Glioma Study Group. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: A randomised controlled multicentre phase III trial. Lancet Oncol. 2006, 7, 392–401. [Google Scholar] [CrossRef]
- Glenn, C.A.; Baker, C.M.; Conner, A.K.; Burks, J.D.; Bonney, P.A.; Briggs, R.G.; Smitherman, A.D.; Battiste, J.D.; Sughrue, M.E. An Examination of the Role of Supramaximal Resection of Temporal Lobe Glioblastoma Multiforme. World Neurosurg. 2018, 114, e747–e755. [Google Scholar] [CrossRef]
- Vanderbeek, A.M.; Rahman, R.; Fell, G.; Ventz, S.; Chen, T.; Redd, R.; Parmigiani, G.; Cloughesy, T.F.; Wen, P.Y.; Trippa, L.; et al. The clinical trials landscape for glioblastoma: Is it adequate to develop new treatments? Neuro Oncol. 2018, 20, 1034–1043. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, A.; Gromeier, M.; Herndon, J.E., 2nd; Beaubier, N.; Bolognesi, D.P.; Friedman, A.H.; Friedman, H.S.; McSherry, F.; Muscat, A.M.; Nair, S.; et al. Recurrent Glioblastoma Treated with Recombinant Poliovirus. N. Engl. J. Med. 2018, 379, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Abedalthagafi, M.; Barakeh, D.; Foshay, K.M. Immunogenetics of glioblastoma: The future of personalized patient management. NPJ Precis. Oncol. 2018, 2, 27. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Chai, Y.; Qi, J.; Zhang, C.W.H.; Tong, Z.; Shi, Y.; Yan, J.; Tan, S.; Gao, G.F. Remarkably similar CTLA-4 binding properties of therapeutic ipilimumab and tremelimumab antibodies. Oncotarget 2017, 8, 67129–67139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, J.; Alvarez-Breckenridge, C.A.; Wang, Q.E.; Yu, J. TGF-β signaling and its targeting for glioma treatment. Am. J. Cancer Res. 2015, 5, 945–955. [Google Scholar] [PubMed]
- Kanaly, C.W.; Ding, D.; Heimberger, A.B.; Sampson, J.H. Clinical applications of a peptide-based vaccine for glioblastoma. Neurosurg. Clin. N. Am. 2010, 21, 95–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Tumor (WHO Grade) | 5-Year Relative Survival Rate | ||
|---|---|---|---|
| Age | |||
| 20–44 | 45–54 | 55–64 | |
| Anaplastic astrocytoma (III) | 58% | 29% | 15% |
| Glioblastoma (IV) | 22% | 9% | 6% |
| Anaplastic oligodendroglioma (III) | 76% | 67% | 45% |
| Variable | RT Alone (n = 286) | RT Plus TMZ (n = 287) |
|---|---|---|
| Median OS (months) | 12.1 months | 14.6 months |
| OS at 6 months (%) | 84.20% | 86.30% |
| OS at 12 months (%) | 50.60% | 61.10% |
| OS at 18 months (%) | 20.90% | 39.40% |
| OS at 24 months (%) | 10.40% | 26.50% |
| Variable | RT Alone (n = 286) | RT Plus TMZ (n = 287) |
|---|---|---|
| Median PFS (months) | 5 months | 6.9 months |
| PFS at 6 months (%) | 36.40% | 53.90% |
| PFS at 12 months (%) | 9.10% | 26.90% |
| PFS at 18 months (%) | 3.90% | 18.40% |
| PFS at 24 months (%) | 1.50% | 10.70% |
| FDA-Approved Therapy | Year Approved | Randomized Controlled Trial | Approved for | Mechanism | Application | Dosage | Common Toxicities | Overall Survival | Progression-Free Survival at 6 Months | Other Notes |
|---|---|---|---|---|---|---|---|---|---|---|
| Lomustine (CCNU) | 1976 | Hochberg et al., 1979 [32] | Recurrent HGG | Nonspecific alkylating agent that causes crosslinking of DNA and RNA in dividing cells triggering cell death | Oral | 80–110 mg/m2 every 6 weeks | Hematologic toxicity (49.7%) | 11.5 months | Unknown | No benefit compared to RT alone |
| Carmustine (BCNU) | 1977 | Walker et al., 1978 [33] | Recurrent HGG | Nonspecific alkylating agent that causes crosslinking of DNA and RNA in dividing cells; also binds to and modifies glutathione reductase | IV | 150–200 mg/m2 every 6 weeks | Pulmonary toxicity (<30%), ocular toxicity (>10%) and bone marrow suppression (>10%) | 11.75 months | Unknown | No benefit compared to RT alone |
| Carmustine wafer implants (BCNU wafers) | 1996 & 2003 | Westphal et al., 2003 [34] | Recurrent and new HGG | Nonspecific alkylating agent that causes crosslinking of DNA and RNA in dividing cells; also binds to and modifies glutathione reductase | Directly applied during surgery | 8 wafers: 61.6 mg | Wound healing complications (12%), intracranial infection (1–10%), and cerebral edema (1–10%) | 13.9 months | Unknown | High complication rate (42.7%) and expensive |
| Temozolomide (TMZ) | 2005 | Stupp et al., 2005 [5] | All HGGs (SOC) | Nonspecific alkylating agent that causes mismatch repair in DNA by methylation at the O6 position of guanine | Oral | 75 mg/m2 per day with RT, 150–200 mg/m2 per day | Hematologic toxicity (16%): thrombocytopenia (12%), leukopenia (7%), and neutropenia (7%) | 14.6–16.1 months | 53.90% | Standard of Care |
| Bevacizumab (BVZ) | 2009 | Cohen et al., 2009 [35] | Recurrent HGG | Targeted therapeutic antibody that binds and inhibits VEGF protein in tumor cells | IV | 10 mg/kg every 2 weeks | Hypertension (5.5–11.4%), thromboembolic events (3.2–11.9%), gastrointestinal perforation (1.5–5.4%), cerebral bleeding (2–5.3%), wound healing complications (0.8–3.3%), and proteinuria (2.7–11.4%) | 9.3 months (recurrent) | 36% (recurrent) | Used to treat symptomatic edema and radiation necrosis |
| Optune device (TTFields) | 2011 & 2015 | Stupp et al., 2015 [36] | Recurrent and new HGG | Low-intensity (1–3 V/cm), intermediate-frequency (200 kHz) alternating electric fields that disrupt mitosis in tumor cells | Portal device, electrodes on scalp | Greater than 18 h a day for >4 weeks | Skin toxicity (43%) and seizures (7%) | 20.5–20.9 months | 56% | Not SOC because of marginal survival benefits, expensive costs, and inconvenience for patients |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fisher, J.P.; Adamson, D.C. Current FDA-Approved Therapies for High-Grade Malignant Gliomas. Biomedicines 2021, 9, 324. https://doi.org/10.3390/biomedicines9030324
Fisher JP, Adamson DC. Current FDA-Approved Therapies for High-Grade Malignant Gliomas. Biomedicines. 2021; 9(3):324. https://doi.org/10.3390/biomedicines9030324
Chicago/Turabian StyleFisher, Jacob P., and David C. Adamson. 2021. "Current FDA-Approved Therapies for High-Grade Malignant Gliomas" Biomedicines 9, no. 3: 324. https://doi.org/10.3390/biomedicines9030324
APA StyleFisher, J. P., & Adamson, D. C. (2021). Current FDA-Approved Therapies for High-Grade Malignant Gliomas. Biomedicines, 9(3), 324. https://doi.org/10.3390/biomedicines9030324