
miR-30b-5p Downregulation as a Predictive Biomarker of Coronary In-Stent Restenosis

 , , and
, , and
Abstract
:1. Introduction
2. Experimental Section
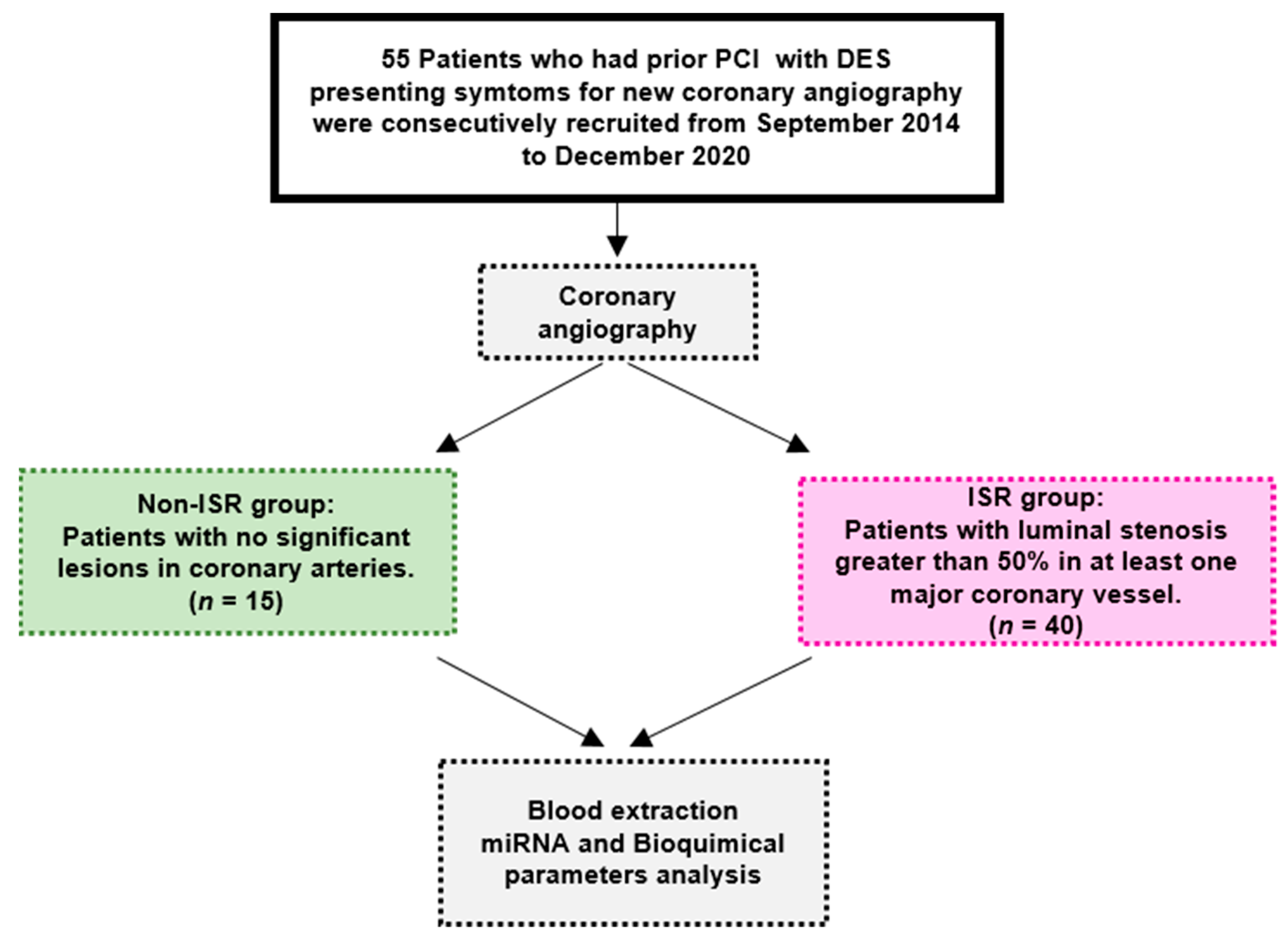
2.1. Study Subjects and Data Collection
2.2. Blood Extraction, miRNA Isolation, and Quantification
2.3. GeneChip miRNA Arrays
2.4. miRNA Quantification by qRT-PCR
2.5. Statistical Analysis
3. Results
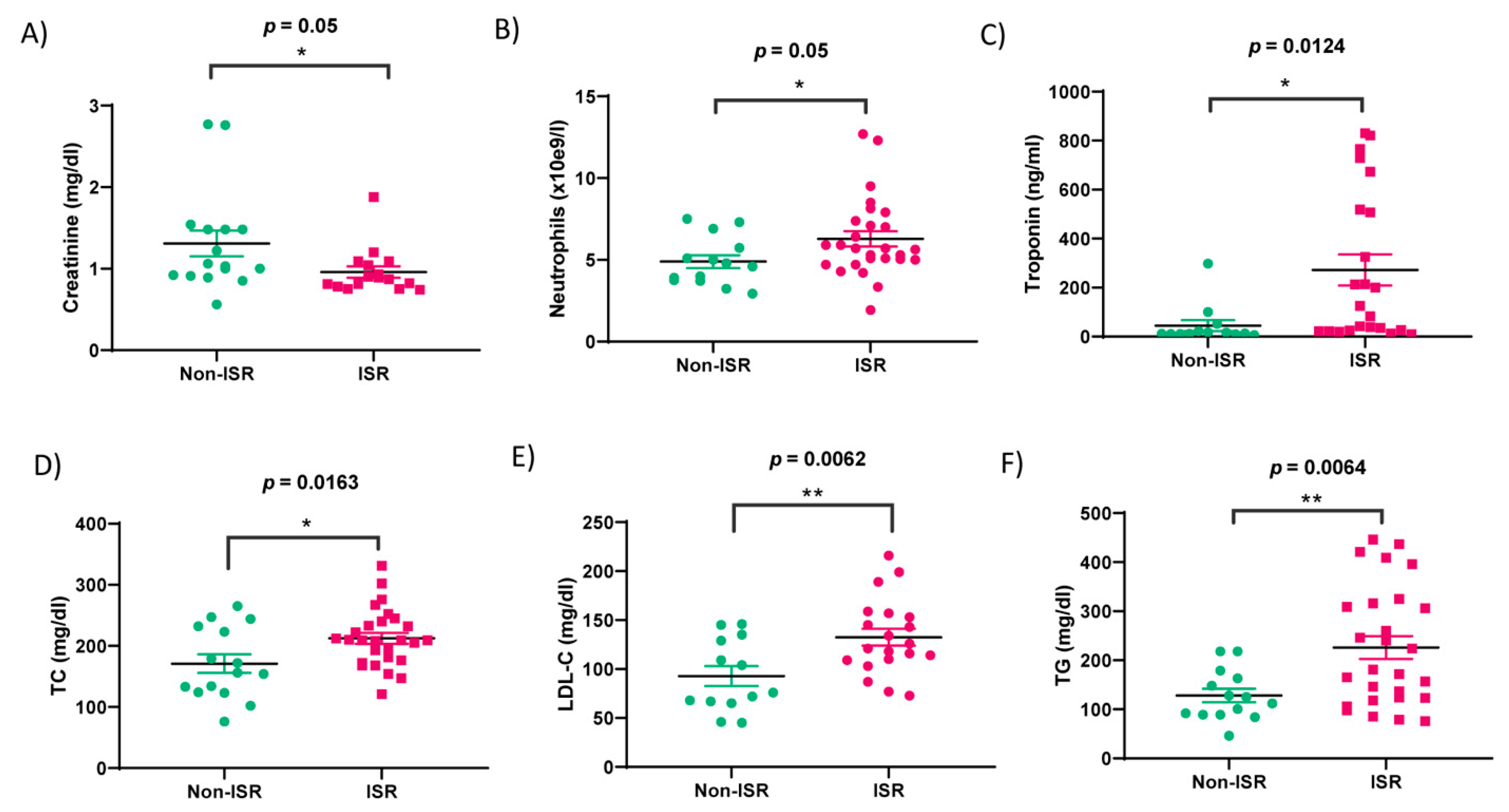
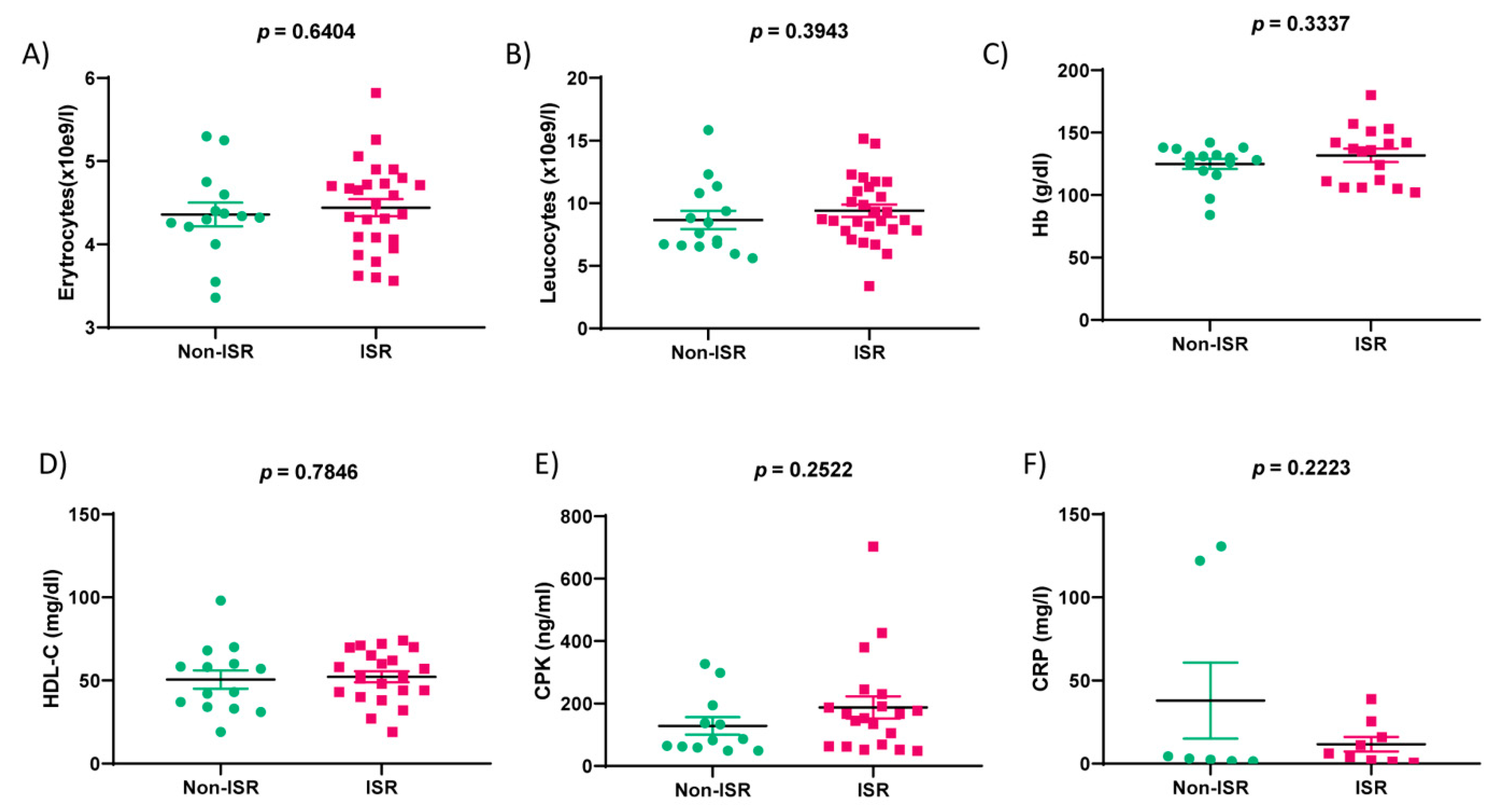
3.1. Clinical Characteristics of the Patients
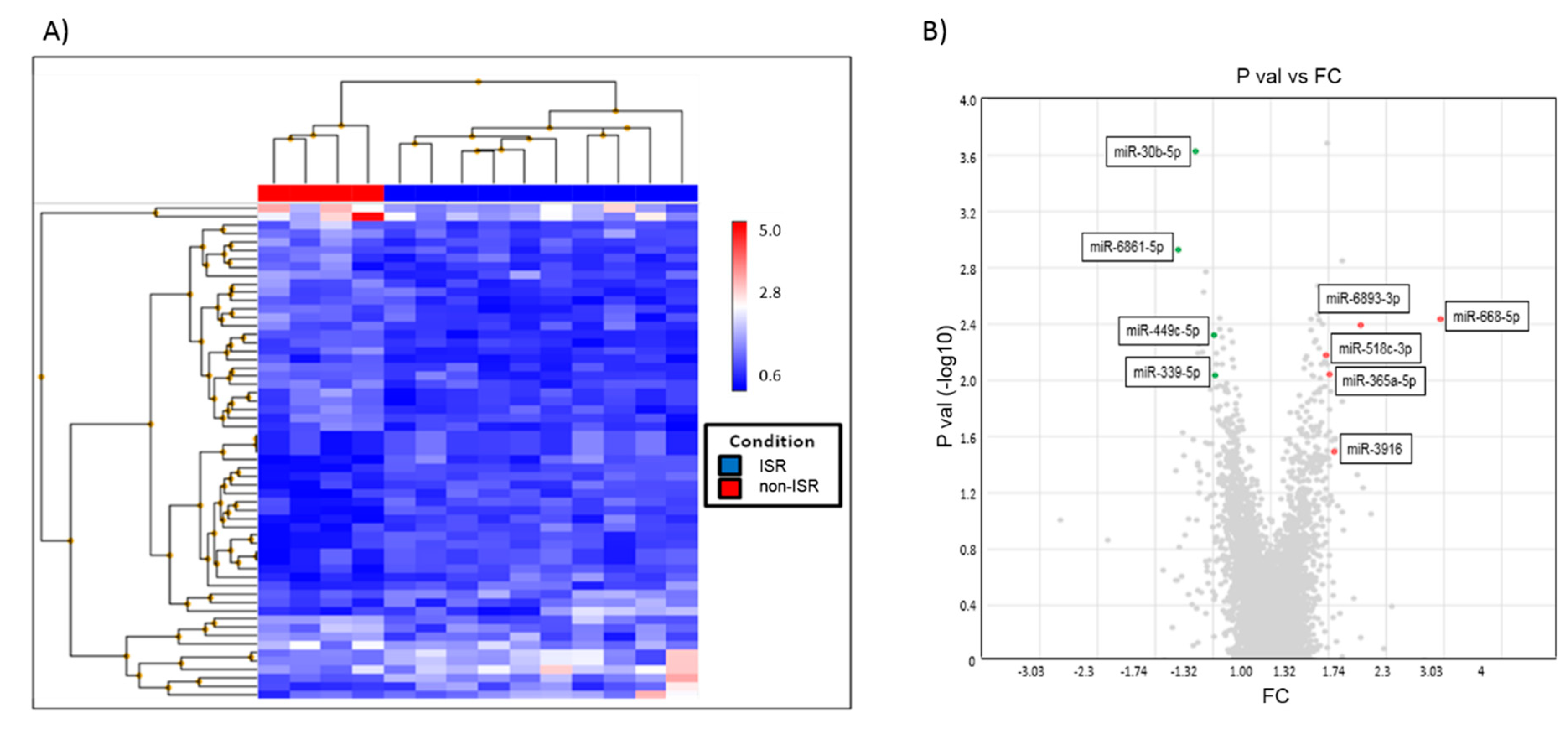
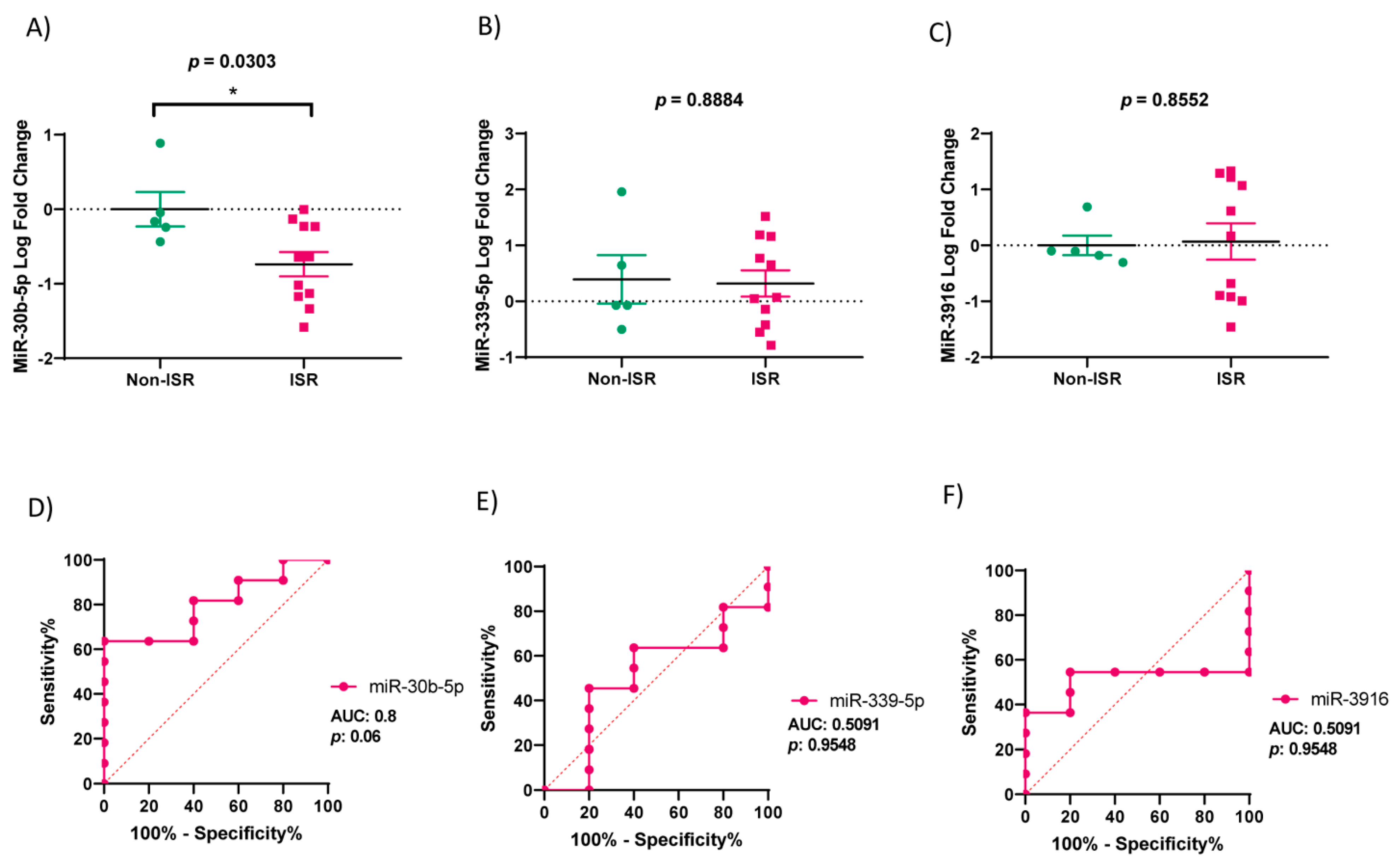
3.2. miRNA Expression Profiles in ISR Patients
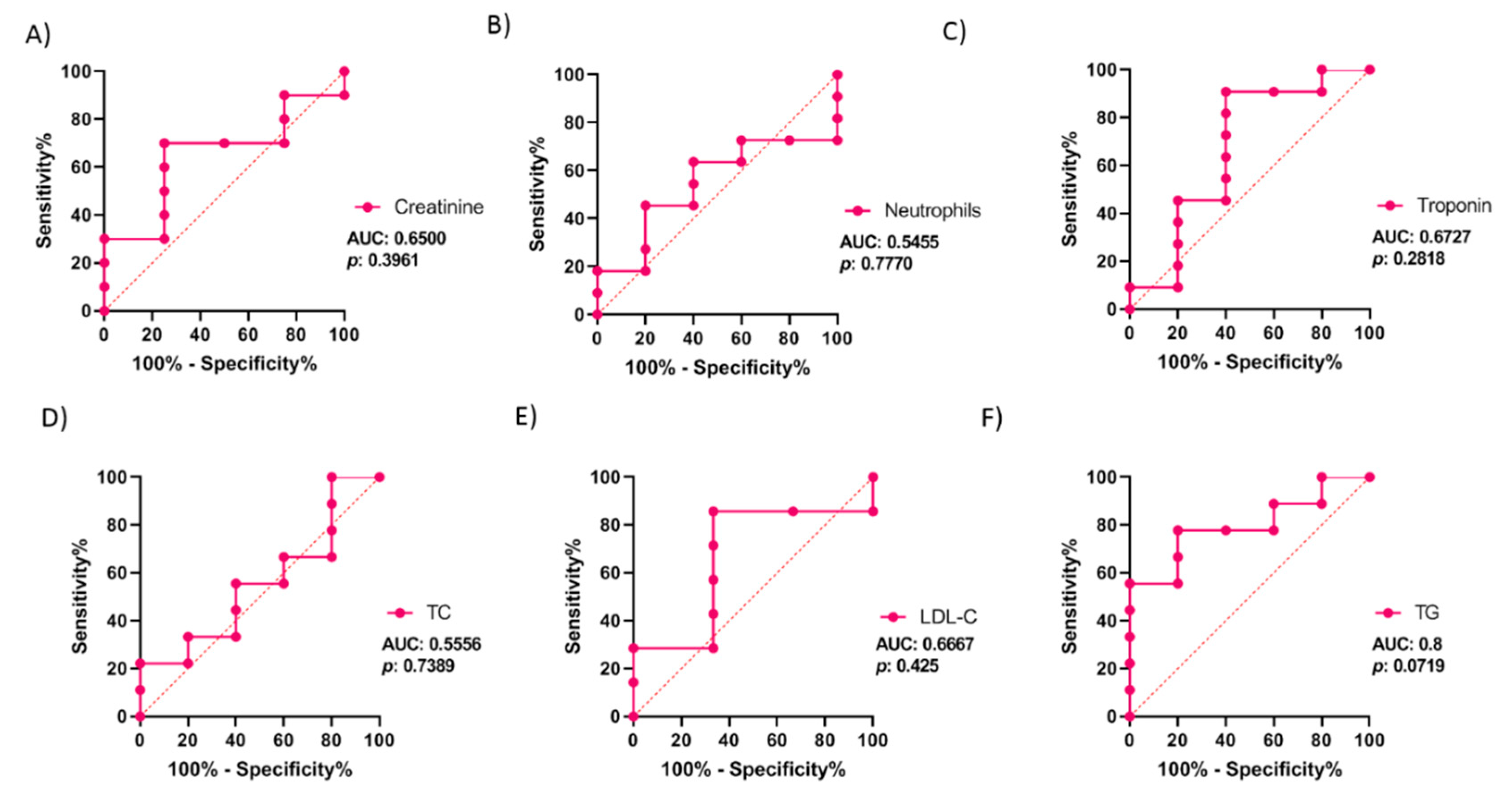
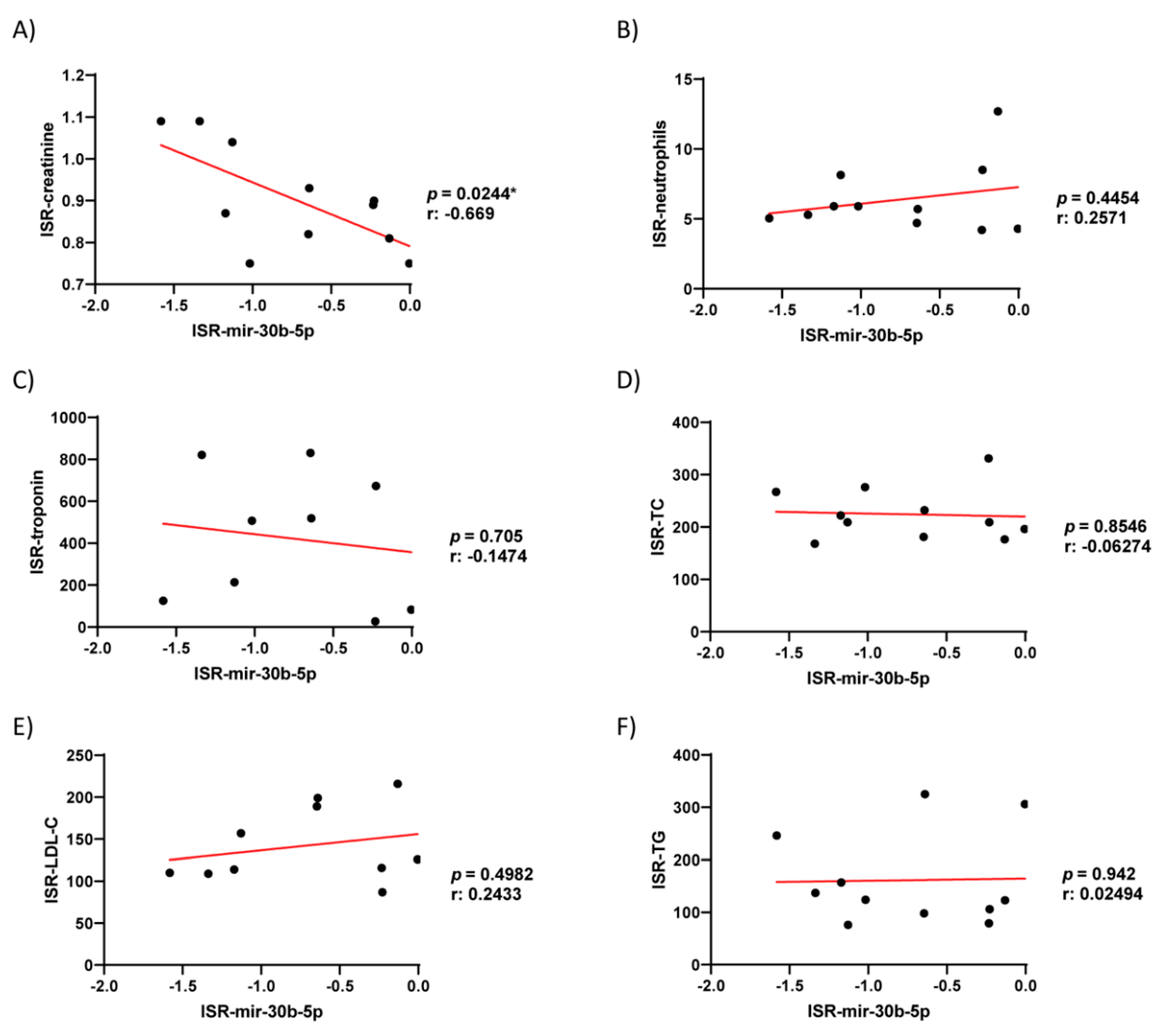
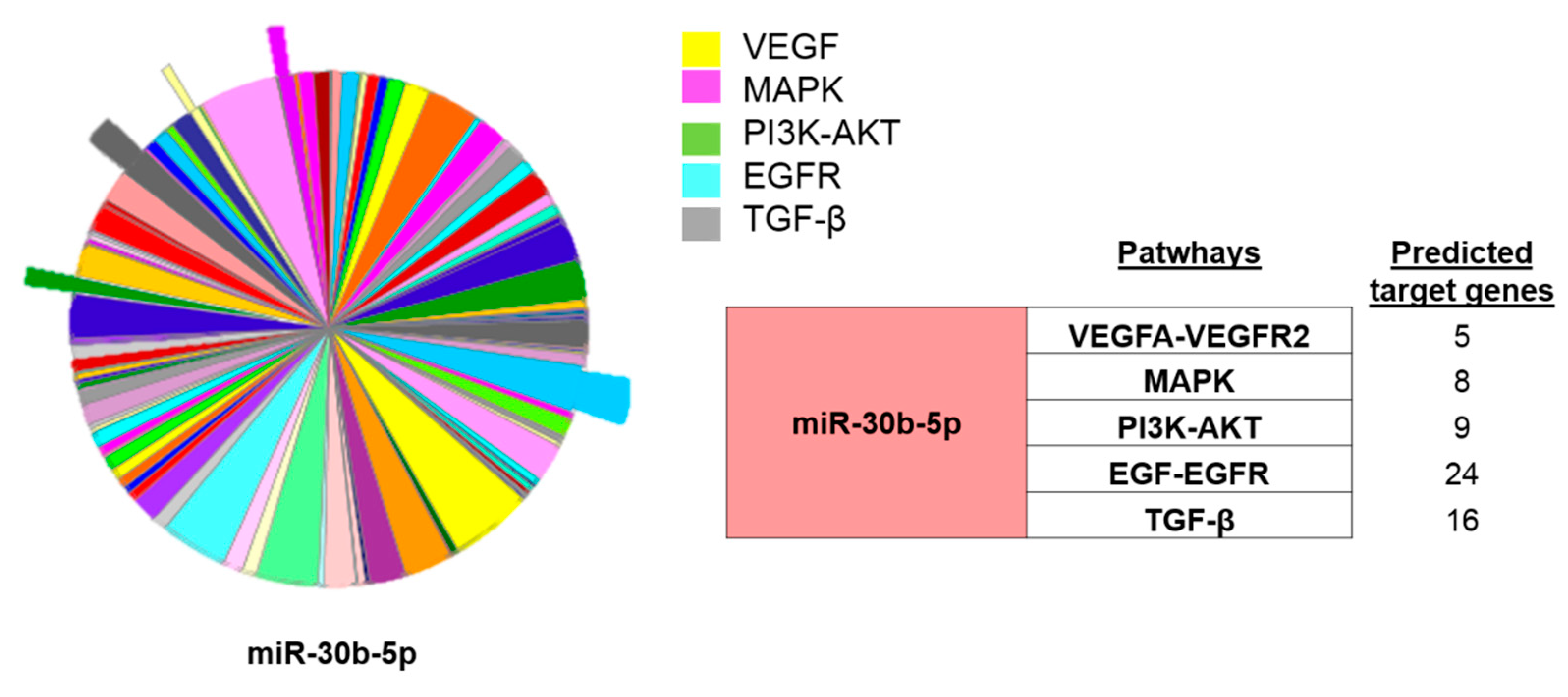
3.3. Validation of the Expression of miRNA and In Silico Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACS | Acute Coronary Symptoms |
| CVD | Cardiovascular Diseases |
| CRP | C Reactive Protein |
| CAD | Coronary Artery Disease |
| CPK | Creatine phosphokinase |
| DES | Drug-Eluting Stents |
| EGR-EGFR | Endothelial Grow Factor and its receptor |
| HF | Heart Failure |
| HDL-C | High-Density Lipoprotein Cholesterol |
| LDL-C | Low-Density Lipoprotein Cholesterol |
| NT-proBNP | N-terminal natriuretic peptide |
| MAPK | Mitogen-Activated Protein Kinases |
| PCI | Percutaneous Coronary Intervention |
| PI3K-AKT | Phosphatidylinositol 3-Kinase |
| TG | Triglycerides |
| TC | Total Cholesterol |
| TGF | Transforming Growth Factor |
| VEGF-VEGFR2 | Vascular Endothelial Growth Factor and its Receptor2 |
| VSMC | Vascular Smooth Muscle Cells |
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Varela, N.; Lanas, F.; Salazar, L.A.; Zambrano, T. The Current State of MicroRNAs as Restenosis Biomarkers. Front. Genet. 2020, 10, 1247. [Google Scholar] [CrossRef]
- Wong, N.D. Epidemiological studies of CHD and the evolution of preventive cardiology. Nat. Rev. Cardiol. 2014, 11, 276–289. [Google Scholar] [CrossRef] [PubMed]
- Wassif, H.; Welt, F.G.P. Restenosis. In SCAI Interventional Cardiology Board Review, 2nd ed.; Wolters Kluwer Health Adis (ESP): London, UK, 2013; pp. 10–15. ISBN 9781469832777. [Google Scholar]
- Cassese, S.; Xu, B.; Habara, S.; Rittger, H.; Byrne, R.A.; Waliszewski, M.; Pérez-Vizcayno, M.J.; Gao, R.; Kastrati, A.; Alfonso, F. Incidence and predictors of reCurrent restenosis after drug-coated balloon Angioplasty for Restenosis of a drUg-eluting Stent: The ICARUS Cooperation. Rev. Esp. Cardiol. 2018, 71, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Dai, R.; Liu, Y.; Zhou, Y.; Xiong, X.; Zhou, W.; Li, W.; Zhou, W.; Chen, M. Potential of circulating pro-angiogenic microRNA expressions as biomarkers for rapid angiographic stenotic progression and restenosis risks in coronary artery disease patients underwent percutaneous coronary intervention. J. Clin. Lab. Anal. 2020, 34. [Google Scholar] [CrossRef]
- Kamal, N.N.S.B.N.M.; Shahidan, W.N.S. Non-exosomal and exosomal circulatory MicroRNAs: Which are more valid as biomarkers? Front. Pharmacol. 2020, 10, 1500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiano, C.; Benincasa, G.; Franzese, M.; Mura, N.D.; Pane, K.; Salvatore, M.; Napoli, C. Epigenetic-sensitive pathways in personalized therapy of major cardiovascular diseases. Pharmacol. Ther. 2020, 210, 107514. [Google Scholar] [CrossRef]
- Smani, T.; Mayoral-Gonzalez, I.; Galeano-Otero, I.; Gallardo-Castillo, I.; Rosado, J.A.; Ordoñez, A.; Hmadcha, A. Non-coding RNAs and Ischemic Cardiovascular Diseases. In Advances in Experimental Medicine and Biology; Springer Nature: Basingstoke, UK, 2020; ISBN 22148019. [Google Scholar]
- Valadi, H.; Ekström, K.; Bossios, A.; Sjöstrand, M.; Lee, J.J.; Lötvall, J.O. Exosome-mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat. Cell Biol. 2007, 9, 654–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, G.W.; Ellis, S.G.; Colombo, A.; Grube, E.; Popma, J.J.; Uchida, T.; Bleuit, J.S.; Dawkins, K.D.; Russell, M.E. Long-term safety and efficacy of paclitaxel-eluting stents: Final 5-year analysis from the TAXUS clinical trial program. JACC Cardiovasc. Interv. 2011, 4, 530–542. [Google Scholar] [CrossRef]
- Giacoppo, D.; Gargiulo, G.; Aruta, P.; Capranzano, P.; Tamburino, C.; Capodanno, D. Treatment strategies for coronary in-stent restenosis: Systematic review and hierarchical Bayesian network meta-analysis of 24 randomised trials and 4880 patients. BMJ 2015, 351, h5392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pleva, L.; Kukla, P.; Hlinomaz, O. Treatment of coronary in-stent restenosis: A systematic review. J. Geriatr. Cardiol. 2018, 15, 173–184. [Google Scholar]
- Zhang, D.M.; Chen, S. In-stent restenosis and a drug-coated balloon: Insights from a clinical therapeutic strategy on coronary artery diseases. Cardiol. Res. Pract. 2020, 2020, 8104939. [Google Scholar] [CrossRef]
- Çakmak, H.A.; Demir, M. Microrna and cardiovascular diseases. Balkan Med. J. 2020, 37, 60–71. [Google Scholar] [CrossRef]
- De Cock, D.; Bennett, J.; Ughi, G.J.; Dubois, C.; Sinnaeve, P.; Dhooge, J.; Desmet, W.; Belmans, A.; Adriaenssens, T. Healing course of acute vessel wall injury after drug-eluting stent implantation assessed by optical coherence tomography. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 800–809. [Google Scholar] [CrossRef]
- Indolfi, C.; Esposito, G.; Di Lorenzo, E.; Rapacciuolo, A.; Feliciello, A.; Porcellini, A.; Avvedimento, V.E.; Condorelli, M.; Chiariello, M. Smooth muscle cell proliferation is proportional to the degree of balloon injury in a rat model of angioplasty. Circulation 1995, 92, 1230–1235. [Google Scholar] [CrossRef]
- Bradley, S.M.; Spertus, J.A.; Kennedy, K.F.; Nallamothu, B.K.; Chan, P.S.; Patel, M.R.; Bryson, C.L.; Malenka, D.J.; Rumsfeld, J.S. Patient selection for diagnostic coronary angiography and hospital-level percutaneous coronary intervention appropriateness: Insights from the national cardiovascular data registry. JAMA Intern. Med. 2014, 174, 1630–1639. [Google Scholar] [CrossRef] [PubMed]
- Jarolim, P.; Morrow, D.A. Use of high sensitivity cardiac troponin assays as an adjunct to cardiac stress testing. Clin. Biochem. 2016, 49, 419–420. [Google Scholar] [CrossRef] [PubMed]
- Brankovic, M.; Akkerhuis, K.M.; Hoorn, E.J.; Boven, N.; Berge, J.C.; Constantinescu, A.; Brugts, J.; Ramshorst, J.; Germans, T.; Hillege, H.; et al. Renal tubular damage and worsening renal function in chronic heart failure: Clinical determinants and relation to prognosis (Bio-SHiFT study). Clin. Cardiol. 2020, 43, 630–638. [Google Scholar] [CrossRef] [Green Version]
- Merten, M.; Dong, J.F.; Lopez, J.A.; Thiagarajan, P. Cholesterol sulfate: A new adhesive molecule for platelets. Circulation 2001, 103, 2032–2034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turczyński, B.; Słowińska, L.; Szyguła, J.; Michalska-Małecka, K.; Szczurek-Katański, K.; Wilczewski, P.; Fudal, M.; Wodniecki, J. Viscosity of blood and plasma in patients with single- and multi-vascular coronary heart disease. Pol. Arch. Med. Wewn. 2000, 104, 475–481. [Google Scholar]
- Chang, Z.; Zheng, J.; Liu, Z.; Guo, Q. The Relationship Between the Neutrophil-Lymphocyte Ratio and In-Stent Restenosis in Patients With Femoropopliteal Chronic Total Occlusions. Angiology 2018, 69, 177–182. [Google Scholar] [CrossRef]
- Shiiba, M.; Zhang, B.; Miura, S.-I.; Ike, A.; Nose, D.; Kuwano, T.; Imaizumi, S.; Sugihara, M.; Iwata, A.; Nishikawa, H.; et al. Association between discordance of LDL-C and non-HDL-C and clinical outcomes in patients with stent implantation: From the FU-Registry. Heart Vessel. 2018, 33, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Galeano-Otero, I.; Del Toro, R.; Guisado, A.; Díaz, I.; Mayoral-González, I.; Guerrero-Márquez, F.; Gutiérrez-Carretero, E.; Casquero-Domínguez, S.; Díaz-de la Llera, L.; Barón-Esquivias, G.; et al. Circulating miR-320a as a Predictive Biomarker for Left Ventricular Remodelling in STEMI Patients Undergoing Primary Percutaneous Coronary Intervention. J. Clin. Med. 2020, 9, 1051. [Google Scholar] [CrossRef] [Green Version]
- Jafarzadeh-Esfehani, R.; Mostafa Parizadeh, S.; Sabeti Aghabozorgi, A.; Yavari, N.; Sadr-Nabavi, A.; Alireza Parizadeh, S.; Ghandehari, M.; Javanbakht, A.; Rezaei-Kalat, A.; Mahdi Hassanian, S.; et al. Circulating and tissue microRNAs as a potential diagnostic biomarker in patients with thrombotic events. J. Cell. Physiol. 2020, 235, 6393–6403. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Zhang, X.; Lu, Y.M.; Li, Y.G.; Zhou, X.; Wang, Y.S. Elevated level of miR-17 along with decreased levels of TIMP-1 and IL-6 in plasma associated with the risk of in-stent restenosis. Biosci. Trends 2019, 13, 423–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, M.; Baker, M.B.; Patel, R.S.; Quyyumi, A.A.; Bao, G.; Searles, C.D. MicroRNA Expression Profile in CAD Patients and the Impact of ACEI/ARB. Cardiol. Res. Pract. 2011, 2011. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Dong, S.; Jia, Q.; Zhang, A.; Li, Y.; Zhu, Y.; Lv, S.; Zhang, J. The microRNA in ventricular remodeling: The MIR-30 family. Biosci. Rep. 2019, 39. [Google Scholar] [CrossRef] [Green Version]
- Lv, Y.X.; Zhong, S.; Tang, H.; Luo, B.; Chen, S.J.; Chen, L.; Zheng, F.; Zhang, L.; Wang, L.; Li, X.Y.; et al. VEGF-A and VEGF-B Coordinate the Arteriogenesis to Repair the Infarcted Heart with Vagus Nerve Stimulation. Cell. Physiol. Biochem. 2018, 48, 433–449. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.L.; Wu, J.Y.; Tsai, C.S.; Lin, C.Y.; Tsai, Y.T.; Lin, C.S.; Wang, Y.F.; Yet, S.F.; Hsu, Y.J.; Kuo, C.C. TLR4-activated MAPK-IL-6 axis regulates vascular smooth muscle cell function. Int. J. Mol. Sci. 2016, 17, 1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; Li, F.; Wang, X.; Gong, J.; Xian, Y.; Wang, G.; Zheng, Z.; Shang, C.; Wang, B.; He, Y.; et al. MiR-145 alleviates Hcy-induced VSMC proliferation, migration, and phenotypic switch through repression of the PI3K/Akt/mTOR pathway. Histochem. Cell Biol. 2020, 153, 357–366. [Google Scholar] [CrossRef]
- Smiljanic, K.; Obradovic, M.; Jovanovic, A.; Djordjevic, J.; Dobutovic, B.; Jevremovic, D.; Marche, P.; Isenovic, E.R. Thrombin stimulates VSMC proliferation through an EGFR-dependent pathway: Involvement of MMP-2. Mol. Cell. Biochem. 2014, 396, 147–160. [Google Scholar] [CrossRef] [PubMed]
- Grootaert, M.O.J.; da Costa Martins, P.A.; Bitsch, N.; Pintelon, I.; de Meyer, G.R.Y.; Martinet, W.; Schrijvers, D.M. Defective autophagy in vascular smooth muscle cells accelerates senescence and promotes neointima formation and atherogenesis. Autophagy 2015, 11, 2014–2032. [Google Scholar] [CrossRef]
- Rodríguez-Moyano, M.; Díaz, I.; Dionisio, N.; Zhang, X.; Ávila-Medina, J.; Calderón-Sánchez, E.; Trebak, M.; Rosado, J.A.; Ordóñez, A.; Smani, T. Urotensin-II promotes vascular smooth muscle cell proliferation through store-operated calcium entry and EGFR transactivation. Cardiovasc. Res. 2013, 100, 297–306. [Google Scholar] [CrossRef]
- Duan, Q.; Chen, C.; Yang, L.; Li, N.; Gong, W.; Li, S.; Wang, D.W. MicroRNA regulation of unfolded protein response transcription factor XBP1 in the progression of cardiac hypertrophy and heart failure in vivo. J. Transl. Med. 2015, 13, 363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.; Ma, G.; Yue, Y.; Wei, Y.; Li, Q.; Tong, Z.; Zhang, L.; Miao, G.; Zhang, J. Downregulation of the miR-30 family microRNAs contributes to endoplasmic reticulum stress in cardiac muscle and vascular smooth muscle cells. Int. J. Cardiol. 2014, 173, 65–73. [Google Scholar] [CrossRef]
- Liu, Y.F.; Spinelli, A.; Sun, L.Y.; Jiang, M.; Singer, D.V.; Ginnan, R.; Saddouk, F.Z.; Van Riper, D.; Singer, H.A. MicroRNA-30 inhibits neointimal hyperplasia by targeting Ca2+/calmodulin-dependent protein kinase IIδ (CaMKIIδ). Sci. Rep. 2016, 6, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Xu, T.; Qiu, X.; Sheng, Z.; Han, Y.; Wang, J.; Tian, B.; Yao, L. Restoration of microRNA-30b expression alleviates vascular calcification through the mTOR signaling pathway and autophagy. J. Cell. Physiol. 2019, 234, 14306–14318. [Google Scholar] [CrossRef]
- Balderman, J.A.F.; Lee, H.Y.; Mahoney, C.E.; Handy, D.E.; White, K.; Annis, S.; Lebeche, D.; Hajjar, R.J.; Loscalzo, J.; Leopold, J.A. Bone morphogenetic protein-2 decreases microRNA-30b and microRNA-30c to promote vascular smooth muscle cell calcification. J. Am. Heart Assoc. 2012, 1, e003905. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Characteristics | Non-ISR Group (15) | ISR Group (40) | p-Value |
|---|---|---|---|
| Age | 62 ± 2.73 | 66.5 ± 1.8 | 0.1844 |
| Gender, N (%) | male 3 (20%) | male 8 (20%) | 1 |
| female 12 (80%) | female 32 (80%) | 0.576 | |
| Risk Factors, N (%) | |||
| Smoking | 8 (53.3%) | 28 (70%) | 0.255 |
| Hypertension | 11 (73.3%) | 30 (75%) | 0.902 |
| Diabetes Mellitus | 6 (40%) | 25 (62.5%) | 0.139 |
| Diabetes Type I | 3 (20%) | 9 (22.5%) | 0.845 |
| Dyslipidemia | 12 (80%) | 28 (70%) | 0.547 |
| Clinical Data, N (%) | |||
| Angina Pectoris | 10 (66%) | 23 (57.5%) | 0.34 |
| Acute Coronary Symptoms | 3 (20%) | 16 (40.0%) | 0.382 |
| Chronic Kidney Disease | 1 (7%) | 0 (0%) | 0.103 |
| Heart Failure | 1 (7%) | 1 (2.5%) | 0.471 |
| Stent Details of the 1st PCI | |||
| N° Stenosis | 26 | 70 | |
| Affected Vessels: | |||
| LAD | 21 (80.8%) | 45 (64.3%) | 0.47 |
| LCX | 4 (15.4%) | 16 (22.8%) | 0.09 |
| RCA * | 1 (3.8%) | 9 (12.9%) | 0.04 |
| Stent Details of the 2nd PCI | |||
| N° Stent Implanted | 58 | ||
| Affected Vessels: | |||
| LAD | 31 (53.4%) | ||
| LCX | 18 (31.1%) | ||
| RCA | 9 (15.5%) | ||
| Treatments | |||
| PCI | 36 (90%) | ||
| CABG | 3 (7.5%) | ||
| Pharmacologic Treatment | 1 (2.5%) |
| Biochemical Characteristics | Non-ISR Group (15) | ISR Group (40) | p-Value |
|---|---|---|---|
| Hemoglobin (g/dL) | 125.0 ± 4.1 (84–142) | 131.8 (102–180) | n.s |
| Creatinine (mg/dL) | 1.3 ± 0.2 (0.56–2.8) | 1.0 ± 0.1 (0.74–1.88) | = 0.05 |
| CPK (ng/mL) | 128.3 ± 27.9 (49–327) | 187.8 ± 35.6 (48–703) | n.s |
| CRP (mg/L) | 37.9 ± 22.9 (1.4–130.7) | 11.7 ± 4.3 (0.5–38.8) | n.s |
| Troponin (ng/mL) * | 44.4 ± 22.3 (5.9–298) | 272.1 ± 63.2 (9.3–830) | <0.05 |
| NT-proBNP | 5821 ± 5742 (78.2–11563) | 6845 ± 2359 (4486–11563) | n.s. |
| Total Cholesterol (mg/dL) * | 170.9 ± 15.1 (76–265.00) | 212.5 ± 9.1 (121–331) | <0.05 |
| HDL-C (mg/dL) | 50.6 ± 5.5 (19–98) | 52.2 ± 3.3 (19–74) | n.s. |
| LDL-C (mg/dL) *** | 92.9 ± 10.2 (45–146) | 132.4 ± 8.6 (72.9–216) | <0.01 |
| TG (mg/dl) *** | 128.0 ± 13.8 (46–218) | 226.0 ± 23.3 (76–446) | <0.001 |
| Erythrocytes (×10e9/L) | 4.4 ± 0.1 (3.36–5.3) | 4.4 ± 0.1 (3.56–5.82) | n.s. |
| Leucocytes (×10e9/L) | 8.7 ± 0.7 (5.6–15.84) | 9.4 ± 0.5 (3.38–15.16) | n.s. |
| Neutrophils (×10e9/L) ** | 4.9 ± 0.4 (2.93–7.5) | 6.3 ± 0.5 (1.93–12.7) | <0.01 |
| MIRNAS | VEGF-VEGFR2 | MAPK | PI3K-AKT | EGF-EGFR | TGF-β | LOG (FC) | p-Value |
|---|---|---|---|---|---|---|---|
| miR-30b-5p | • | • | • | • | • | −1.44 | 0.0002 |
| miR-3916 | • | • | • | • | • | 1.36 | 0.0323 |
| miR-6893-3p | • | • | • | • | • | 1.55 | 0.0040 |
| miR-339-5p | • | • | • | • | - | −1.31 | 0.0092 |
| miR-449c-5p | • | • | • | - | • | −1.31 | 0.0047 |
| miR-6737-5p | • | • | • | • | - | −1.35 | 0.083 |
| miR-365a-5p | • | - | • | • | - | 1.33 | 0.009 |
| miR-518c-3p | - | • | - | • | - | 1.31 | 0.0066 |
| miR-668-5p | - | - | • | - | - | 2.26 | 0.0037 |
| miR-6861-5p | • | - | • | - | - | −1.56 | 0.0012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutierrez-Carretero, E.; Mayoral-González, I.; Jesús Morón, F.; Fernández-Quero, M.; Domínguez-Rodríguez, A.; Ordóñez, A.; Smani, T. miR-30b-5p Downregulation as a Predictive Biomarker of Coronary In-Stent Restenosis. Biomedicines 2021, 9, 354. https://doi.org/10.3390/biomedicines9040354
Gutierrez-Carretero E, Mayoral-González I, Jesús Morón F, Fernández-Quero M, Domínguez-Rodríguez A, Ordóñez A, Smani T. miR-30b-5p Downregulation as a Predictive Biomarker of Coronary In-Stent Restenosis. Biomedicines. 2021; 9(4):354. https://doi.org/10.3390/biomedicines9040354
Chicago/Turabian StyleGutierrez-Carretero, Encarnación, Isabel Mayoral-González, Francisco Jesús Morón, Mónica Fernández-Quero, Alejandro Domínguez-Rodríguez, Antonio Ordóñez, and Tarik Smani. 2021. "miR-30b-5p Downregulation as a Predictive Biomarker of Coronary In-Stent Restenosis" Biomedicines 9, no. 4: 354. https://doi.org/10.3390/biomedicines9040354
APA StyleGutierrez-Carretero, E., Mayoral-González, I., Jesús Morón, F., Fernández-Quero, M., Domínguez-Rodríguez, A., Ordóñez, A., & Smani, T. (2021). miR-30b-5p Downregulation as a Predictive Biomarker of Coronary In-Stent Restenosis. Biomedicines, 9(4), 354. https://doi.org/10.3390/biomedicines9040354