
The Role of Endothelins, IL-18, and NGAL in Kidney Hypothermic Machine Perfusion

 , , ,
, , ,
Abstract
:1. Introduction
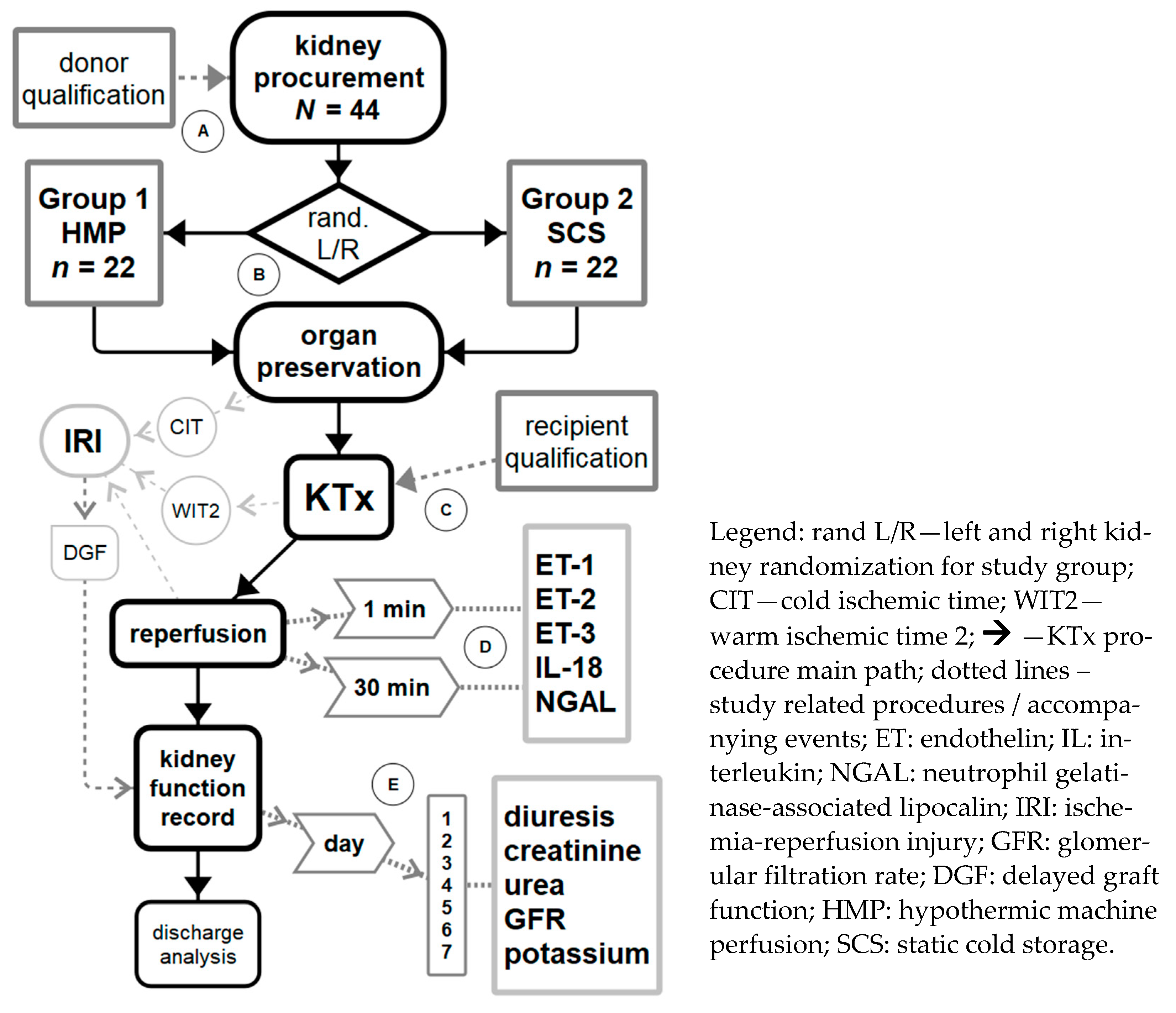
2. Materials and Methods
2.1. Study Group and Inclusion/Exclusion Criteria
2.2. Transplant Procedure
2.3. Post-Transplant Care
2.4. Laboratory Analysis
2.4.1. Sample Collection and Laboratory Kits
2.4.2. General Overview of ELISA Procedure Performed
2.4.3. Detailed ELISA Procedure and Results Reading
2.5. Ethical Approcal
2.6. Statistical Analysis
3. Results
3.1. Study Group Characteristics
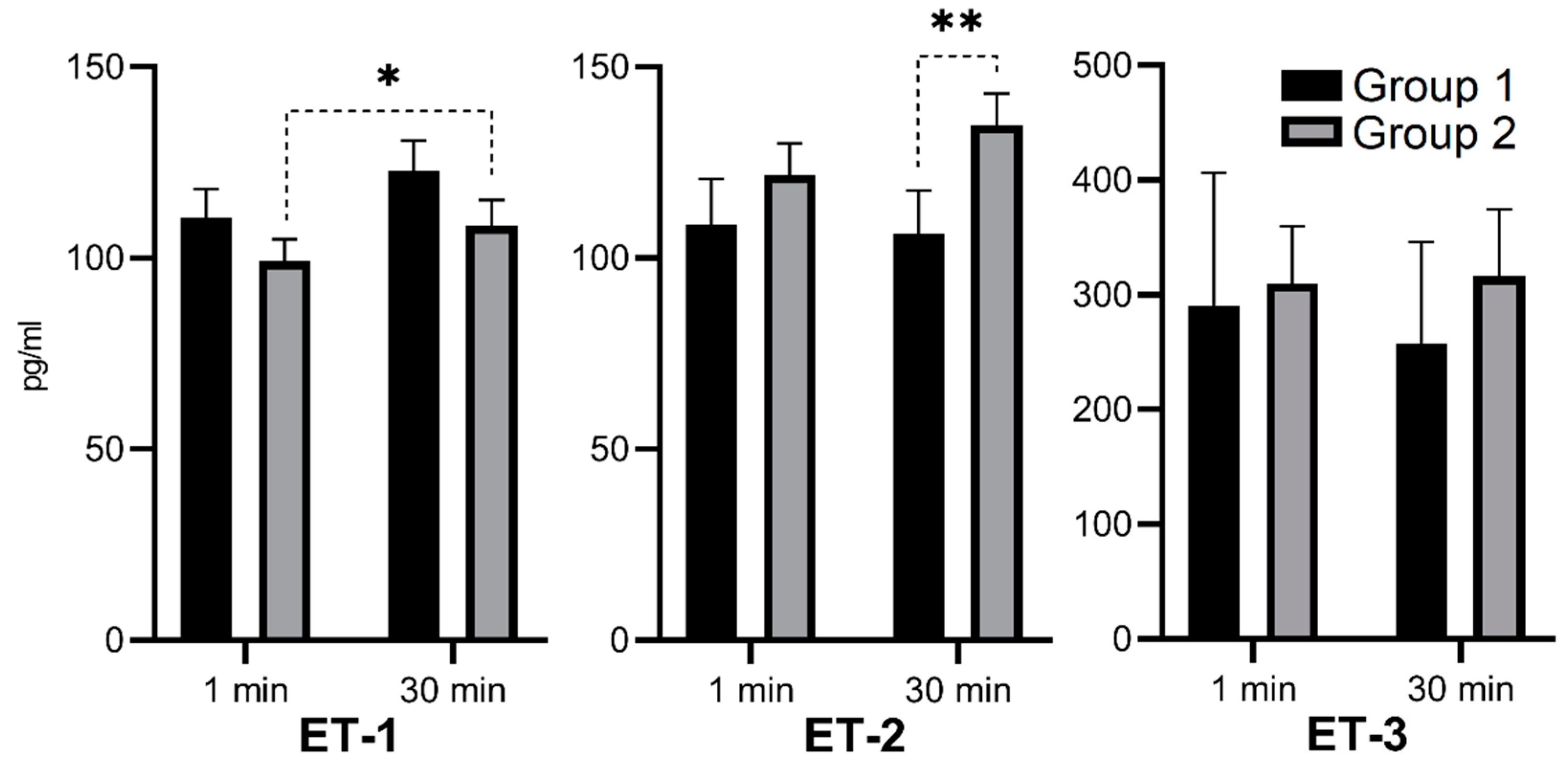
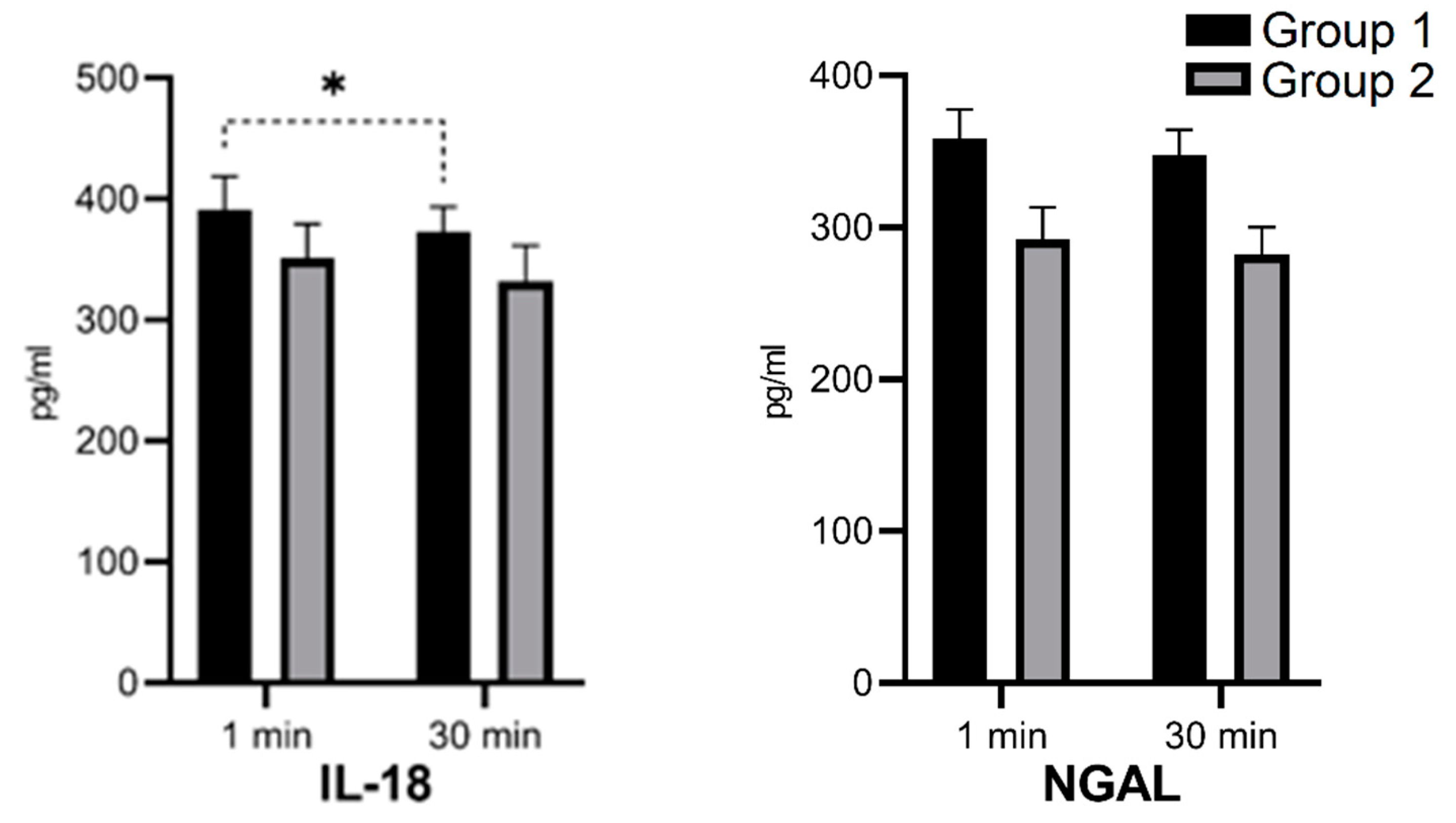
3.2. Absolute Serum Concentrations of ET-1, ET-2, ET-3, IL-18, and NGAL in the 1st and 30th Minutes of Kidney Reperfusion
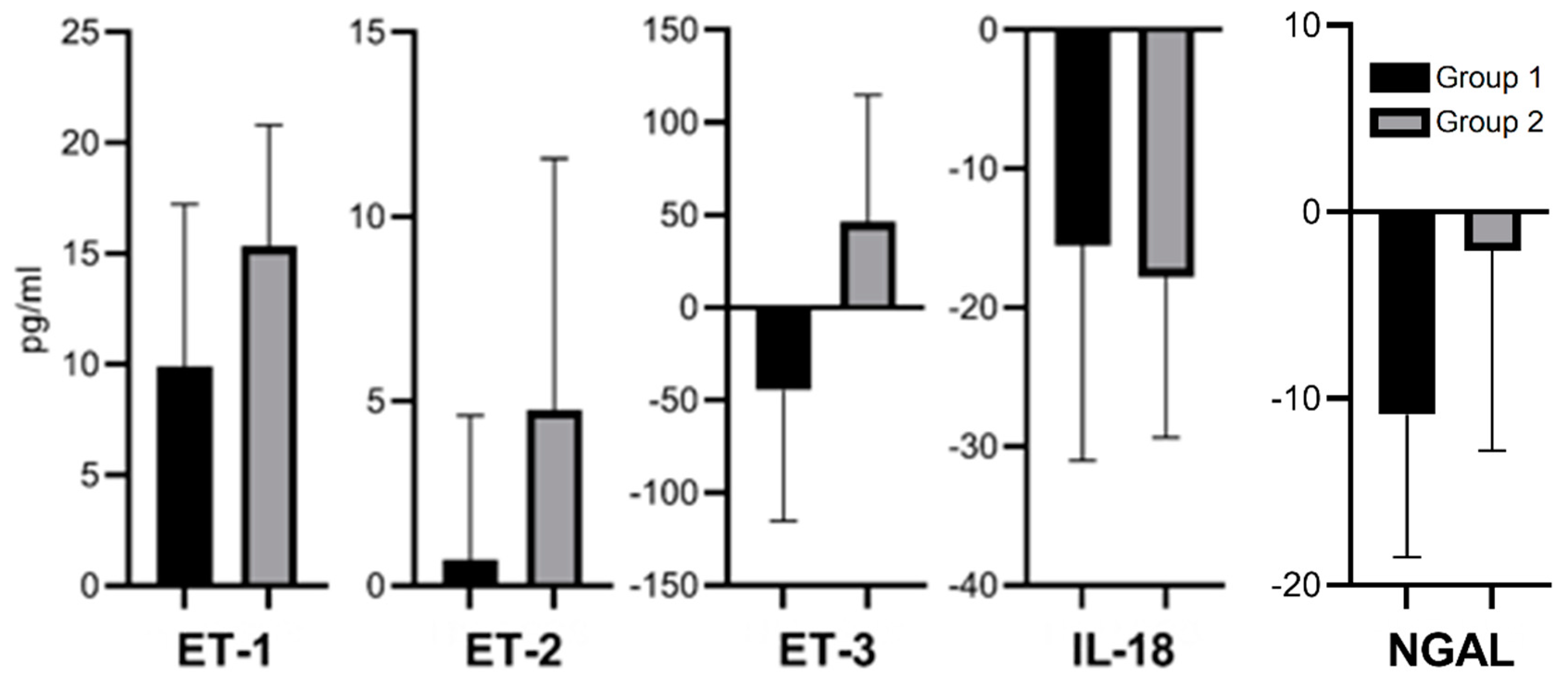
3.3. Relative Serum Concentration Changes (Δ) of ET-1, ET-2, ET-3, IL-18, and NGAL After 30 Min of a Kidney Reperfusion
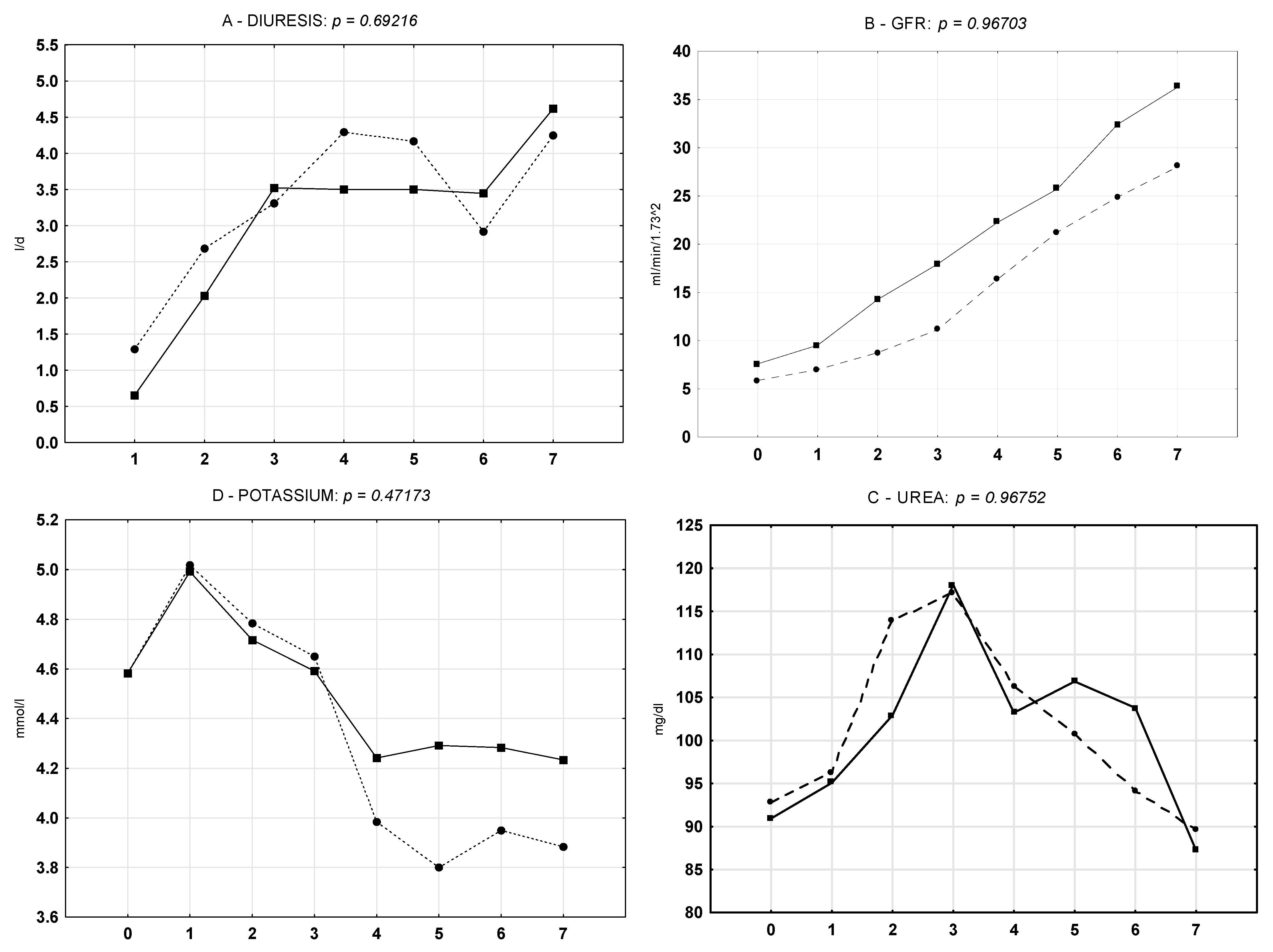
3.4. Classic Biomarkers of Kidney Function During the Seven-Day Postoperative Observation Period
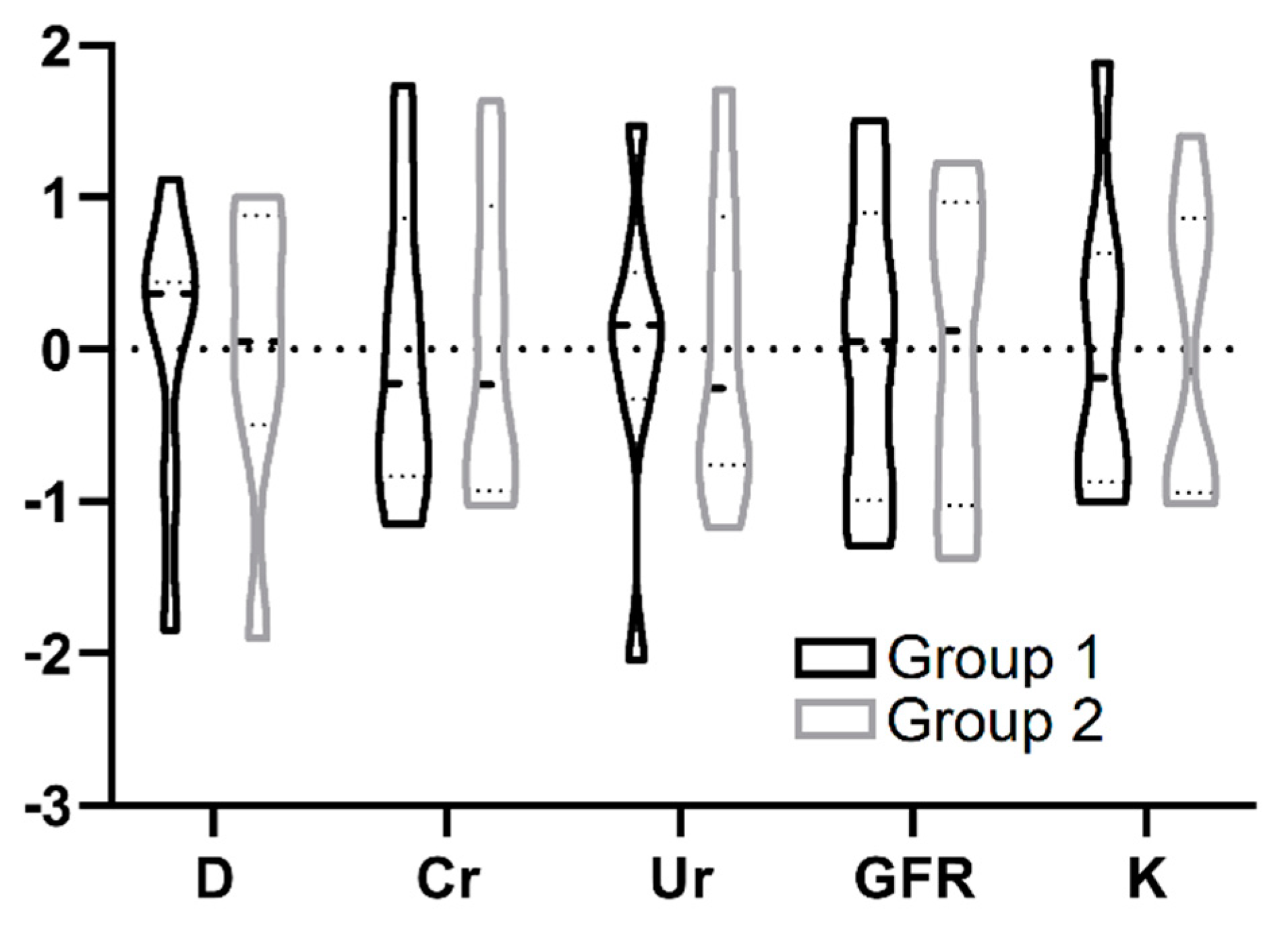
3.5. Correlations Between Absolute and Relative Concentrations of ET-1, ET-2, ET-3, IL-18, and NGAL and Kidney Function Parameters During Seven-Day Postoperative Observation
4. Discussion
4.1. Endothelins
4.2. Interleukin-18 (IL-18)
4.3. Neutrophil Gelatinase-Associated Lipocalin (NGAL)
4.4. Kidney Function and HMP
4.5. Modern vs. Classic Kidney Function Biomarkers
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zukowski, M.; Kotfis, K.; Biernawska, J.; Zegan-Barańska, M.; Kaczmarczyk, M.; Ciechanowicz, A.; Brykczynski, M.; Ostrowski, M.; Nikodemski, T.; Bohatyrewicz, R. Donor-Recipient Gender Mismatch Affects Early Graft Loss After Kidney Transplantation. Transplant. Proc. 2011, 43, 2914–2916. [Google Scholar] [CrossRef]
- Soares, R.O.S.; Losada, D.M.; Jordani, M.C.; Évora, P.; Castro-E-Silva, O. Ischemia/Reperfusion Injury Revisited: An Overview of the Latest Pharmacological Strategies. Int. J. Mol. Sci. 2019, 20, 5034. [Google Scholar] [CrossRef] [Green Version]
- Panisello-Roselló, A.; Roselló-Catafau, J. Molecular Mechanisms and Pathophysiology of Ischemia-Reperfusion Injury. Int. J. Mol. Sci. 2018, 19, 4093. [Google Scholar] [CrossRef] [Green Version]
- Fernández, A.R.; Sánchez-Tarjuelo, R.; Cravedi, P.; Ochando, J.; López-Hoyos, M. Review: Ischemia Reperfusion Injury—A Translational Perspective in Organ Transplantation. Int. J. Mol. Sci. 2020, 21, 8549. [Google Scholar] [CrossRef]
- Hentia, C.; Rizzato, A.; Camporesi, E.; Yang, Z.; Muntean, D.M.; Săndesc, D.; Bosco, G. An overview of protective strategies against ischemia/reperfusion injury: The role of hyperbaric oxygen preconditioning. Brain Behav. 2018, 8, e00959. [Google Scholar] [CrossRef] [PubMed]
- Nastos, C.; Kalimeris, K.; Papoutsidakis, N.; Tasoulis, M.-K.; Lykoudis, P.M.; Theodoraki, K.; Smyrniotis, V.; Arkadopoulos, N. Global consequences of liver ischemia/reperfusion injury. Oxid. Med. Cell Longev. 2014, 906965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pantazi, E. Role of sirtuins in ischemia-reperfusion injury. World J. Gastroenterol. 2013, 19, 7594–7602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panisello-Roselló, A.; Roselló-Catafau, J.; Adam, R. New Insights in Molecular Mechanisms and Pathophysiology of Ischemia-Reperfusion Injury 2.0: An Updated Overview. Int. J. Mol. Sci. 2020, 22, 28. [Google Scholar] [CrossRef] [PubMed]
- Eltzschig, H.K.; Eckle, T. Ischemia and reperfusion—from mechanism to translation. Nat. Med. 2011, 17, 1391–1401. [Google Scholar] [CrossRef] [Green Version]
- Czigany, Z.; Lurje, I.; Schmelzle, M.; Schöning, W.; Öllinger, R.; Raschzok, N.; Sauer, I.M.; Tacke, F.; Strnad, P.; Trautwein, C.; et al. Ischemia-Reperfusion Injury in Marginal Liver Grafts and the Role of Hypothermic Machine Perfusion: Molecular Mechanisms and Clinical Implications. J. Clin. Med. 2020, 9, 846. [Google Scholar] [CrossRef] [Green Version]
- Kvietkauskas, M.; Zitkute, V.; Leber, B.; Strupas, K.; Stiegler, P.; Schemmer, P. The Role of Metabolomics in Current Concepts of Organ Preservation. Int. J. Mol. Sci. 2020, 21, 6607. [Google Scholar] [CrossRef]
- Kvietkauskas, M.; Leber, B.; Strupas, K.; Stiegler, P.; Schemmer, P. Machine Perfusion of Extended Criteria Donor Organs: Immunological Aspects. Front. Immunol. 2020, 11. [Google Scholar] [CrossRef]
- Hofmann, J.; Otarashvili, G.; Meszaros, A.; Ebner, S.; Weissenbacher, A.; Cardini, B.; Oberhuber, R.; Resch, T.; Öfner, D.; Schneeberger, S.; et al. Restoring Mitochondrial Function While Avoiding Redox Stress: The Key to Preventing Ischemia/Reperfusion Injury in Machine Perfused Liver Grafts? Int. J. Mol. Sci. 2020, 21, 3132. [Google Scholar] [CrossRef]
- Kasil, A.; Giraud, S.; Couturier, P.; Amiri, A.; Danion, J.; Donatini, G.; Matillon, X.; Hauet, T.; Badet, L. Individual and Combined Impact of Oxygen and Oxygen Transporter Supplementation during Kidney Machine Preservation in a Porcine Preclinical Kidney Transplantation Model. Int. J. Mol. Sci. 2019, 20, 1992. [Google Scholar] [CrossRef] [Green Version]
- Davenport, A.P.; Hyndman, K.A.; Dhaun, N.; Southan, C.; Kohan, D.E.; Pollock, J.S.; Pollock, D.M.; Webb, D.J.; Maguire, J.J. Endothelin. Pharmacol. Rev. 2016, 68, 357–418. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, S.; Serizawa, A.; Sakaguchi, T.; Tsuchiya, Y.; Kojima, Y.; Okamoto, K.; Kurachi, K.; Konno, H.; Fujise, Y.; Baba, S.; et al. The roles of platelet-activating factor and endothelin-1 in renal damage after total hepatic ischemia and reperfusion1. Transplant. 2000, 69, 2267–2273. [Google Scholar] [CrossRef] [PubMed]
- Marzi, I.; Rucker, M.; Walcher, F.; Takei, Y. Endothelin-1 is involved in hepatic sinusoidal vasoconstriction after ischemia and reperfusion. Transpl. Int. 1994, 7, 503–506. [Google Scholar] [CrossRef] [PubMed]
- Schwarting, A.; Tesch, G.; Kinoshita, K.; Maron, R.; Weiner, H.L.; Kelley, V.R. IL-12 drives IFN-gamma-dependent autoimmune kidney disease in MRL-Fas(lpr) mice. J. Immunol. 1999, 163, 6884–6891. [Google Scholar] [PubMed]
- Schwarting, A.; Wada, T.; Kinoshita, K.; Tesch, G.; Kelley, V.R. IFN-gamma receptor signaling is essential for the initiation, acceleration, and destruction of autoimmune kidney disease in MRL-Fas(lpr) mice. J. Immunol. 1998, 161, 494–503. [Google Scholar] [PubMed]
- Melnikov, V.Y.; Faubel, S.; Siegmund, B.; Lucia, M.S.; Ljubanović, D.; Edelstein, C.L. Neutrophil-independent mechanisms of caspase-1– and IL-18–mediated ischemic acute tubular necrosis in mice. J. Clin. Investig. 2002, 110, 1083–1091. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Canga, J.L.; Penagos, L.M.; Diego, R.B.; Cecilio, R.V.S.; Calabia, E.R.; Vega, L.B.; Soto, M.S.; Martínez, L.R.; Cuesta, C.L.D.M.; Millán, J.R.S. Effect of Cold Ischemia Time on Kidney Graft Function and Survival: Differences Between Paired Kidney Transplants From the Same Donor. Transplant. Proc. 2019, 51, 321–323. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.; Rose, C.; Joffres, Y.; Kadatz, M.; Gill, J. Cold ischemia time up to 16 h has little impact on living donor kidney transplant outcomes in the era of kidney paired donation. Kidney Int. 2017, 92, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Kohan, N.E. Endothelins in the normal and diseased kidney. Am. J. Kidney Dis. 1997, 29, 2–26. [Google Scholar] [CrossRef]
- Clavel, A.L.; Burnett, J.C. Physiologic and pathophysiologic roles of endothelin in the kidney. Curr. Opin. Nephrol. Hypertens. 1994, 3, 66–72. [Google Scholar] [CrossRef]
- Rosen, B.; Barg, J.; Zimlichman, R. The effects of angiotensin II, endothelin-1, and protein kinase C inhibitor on DNA synthesis and intracellular calcium mobilization in vascular smooth muscle cells from young normotensive and spontaneously hypertensive rats. Am. J. Hypertens. 1999, 12, 1243–1251. [Google Scholar] [CrossRef] [Green Version]
- Klahr, S. Mechanisms of progression of chronic renal damage. J. Nephrol. 2000, 12, 2–4. [Google Scholar]
- Ehrenreich, H.; Anderson, R.W.; Fox, C.H.; Rieckmann, P.; Hoffman, G.S.; Travis, W.D.; Coligan, J.E.; Kehrl, J.H.; Fauci, A.S. Endothelins, peptides with potent vasoactive properties, are produced by human macrophages. J. Exp. Med. 1990, 172, 1741–1748. [Google Scholar] [CrossRef] [Green Version]
- KawanabeSurya, Y.; Nauli, S.M. Endothelin. Cell. Mol. Life Sci. 2010, 68, 195–203. [Google Scholar] [CrossRef]
- Miyauchi, T.; Sakai, S. Endothelin and the heart in health and diseases. Peptides 2019, 111, 77–88. [Google Scholar] [CrossRef]
- Davenport, A.P. International Union of Pharmacology. XXIX. Update on endothelin receptor nomenclature. Pharmacol. Rev. 2002, 54, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Böhm, F.; Pernow, J. The importance of endothelin-1 for vascular dysfunction in cardiovascular disease. Cardiovasc. Res. 2007, 76, 8–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, L.; Toledo, A.H.; Lopez-Neblina, F.; Anaya-Prado, R.; Toledo-Pereyra, L.H. Nitric Oxide Mechanism of Protection in Ischemia and Reperfusion Injury. J. Investig. Surg. 2009, 22, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.; Zaigham, K.; Iqbal, M.S.; Ali, Q. Detection of Endothelin 2 (Et-2) as a novel biomarker of renal dysfunction in patients of liver Cirrhosis with Ascites. PKP 2016, 3, 112–118. [Google Scholar]
- Nowanska, K.; Donizy, P.; Kościelska-Kasprzak, K.; Kaminska, D.; Krajewska, M.; Mazanowska, O.; Madziarska, K.; Zmonarski, S.; Chudoba, P.; Małkiewicz, B.; et al. Endothelin A Receptors Expressed in Renal Blood Vessels of Renal Transplant Patients Are Connected With Acute Tubular Necrosis or Antibody-Mediated Rejection. Transplant. Proc. 2018, 50, 1760–1764. [Google Scholar] [CrossRef]
- Weitzberg, E.; Hemsén, A.; Lundberg, J.M.; Ahlborg, G. ET-3 is extracted by and induces potent vasoconstriction in human splanchnic and renal vasculatures. J. Appl. Physiol. 1995, 79, 1255–1259. [Google Scholar] [CrossRef]
- Martinez, F.; Deray, G.; Dubois, M.; Jacquiaud, C.; Schmitt, F.; Jacobs, C. Chronic effects of endothelin-3 on blood pressure and renal haemodynamics in rats. Nephrol. Dial. Transplant. 1996, 11, 270–274. [Google Scholar] [CrossRef]
- Nozaki, Y.; Hino, S.; Ri, J.; Sakai, K.; Nagare, Y.; Kawanishi, M.; Niki, K.; Funauchi, M.; Matsumura, I. Lipopolysaccharide-Induced Acute Kidney Injury Is Dependent on an IL-18 Receptor Signaling Pathway. Int. J. Mol. Sci. 2017, 18, 2777. [Google Scholar] [CrossRef] [Green Version]
- Boraschi, D.; Dinarello, C.A. IL-18 in autoimmunity: Review. Eur. Cytokine Netw. 2006, 17, 224–252. [Google Scholar]
- Yasuda, K.; Nakanishi, K.; Tsutsui, H. Interleukin-18 in Health and Disease. Int. J. Mol. Sci. 2019, 20, 649. [Google Scholar] [CrossRef] [Green Version]
- Cui, L.-Y.; Zhu, X.; Yang, S.; Zhou, J.-S.; Zhang, H.-X.; Liu, L.; Zhang, J. Prognostic Value of Levels of Urine Neutrophil Gelatinase-associated Lipocalin and Interleukin-18 in Patients With Delayed Graft Function After Kidney Transplantation. Transpl. Proc. 2015, 47, 2846–2851. [Google Scholar] [CrossRef]
- Kamińska, D.; Kościelska-Kasprzak, K.; Chudoba, P.; Mazanowska, O.; Banasik, M.; Żabinska, M.; Boratyńska, M.; Lepiesza, A.; Gomółkiewicz, A.; Dzięgiel, P.; et al. Pretransplant Immune- and Apoptosis-Related Gene Expression Is Associated with Kidney Allograft Function. Mediat. Inflamm. 2016, 2016, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Parikh, C.R.; Abraham, E.; Ancukiewicz, M.; Edelstein, C.L. Urine IL-18 Is an Early Diagnostic Marker for Acute Kidney Injury and Predicts Mortality in the Intensive Care Unit. J. Am. Soc. Nephrol. 2005, 16, 3046–3052. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Craft, M.L.; Wang, P.; Wyburn, K.R.; Chen, G.; Ma, J.; Hambly, B.; Chadban, S.J. IL-18 Contributes to Renal Damage after Ischemia-Reperfusion. J. Am. Soc. Nephrol. 2008, 19, 2331–2341. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.-D.; Ryu, H.-M.; Choi, J.-Y.; Choi, H.-J.; Choi, H.-J.; Cho, J.-H.; Park, S.-H.; Won, D.-I.; Kim, Y.-L. Association of G–137C IL-18 Promoter Polymorphism with Acute Allograft Rejection in Renal Transplant Recipients. Transplantation 2008, 86, 1610–1614. [Google Scholar] [CrossRef]
- Kuncio, G.S.; Neilson, E.G.; Haverty, T. Mechanisms of tubulointerstitial fibrosis. Kidney Int. 1991, 39, 550–556. [Google Scholar] [CrossRef] [Green Version]
- Marchewka, Z.; Tacik, A.; Piwowar, A. KIM-1 and NGAL as potential biomarkers for the diagnosis and cancer progression. Postępy Hig. i Med. Doświadczalnej 2016, 70, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Lisowska-Myjak, B. Serum and Urinary Biomarkers of Acute Kidney Injury. Blood Purif. 2010, 29, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Hall, I.E.; Yarlagadda, S.G.; Coca, S.G.; Wang, Z.; Doshi, M.; Devarajan, P.; Han, W.K.; Marcus, R.J.; Parikh, C.R. IL-18 and Urinary NGAL Predict Dialysis and Graft Recovery after Kidney Transplantation. J. Am. Soc. Nephrol. 2009, 21, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.Y.; Kim, M.S.; Park, Y.; Kim, H.-S. Serum Neutrophil Gelatinase-Associated Lipocalin and Interleukin-18 as Predictive Biomarkers for Delayed Graft Function After Kidney Transplantation. J. Clin. Lab. Anal. 2012, 26, 295–301. [Google Scholar] [CrossRef]
- Rysz, J.; Gluba-Brzózka, A.; Franczyk, B.; Jabłonowski, Z.; Ciałkowska-Rysz, A. Novel Biomarkers in the Diagnosis of Chronic Kidney Disease and the Prediction of Its Outcome. Int. J. Mol. Sci. 2017, 18, 1702. [Google Scholar] [CrossRef]
- Stratta, R.J.; Moore, P.S.; Farney, A.C.; Rogers, J.; Hartmann, E.L.; Reeves-Daniel, A.; Gautreaux, M.D.; Iskandar, S.S.; Adams, P.L. Influence of Pulsatile Perfusion Preservation on Outcomes in Kidney Transplantation from Expanded Criteria Donors. J. Am. Coll. Surg. 2007, 204, 873–882. [Google Scholar] [CrossRef]
- Matsuoka, L.; Shah, T.; Aswad, S.; Bunnapradist, S.; Cho, Y.; Mendez, R.G.; Selby, R. Pulsatile Perfusion Reduces the Incidence of Delayed Graft Function in Expanded Criteria Donor Kidney Transplantation. Arab. Archaeol. Epigr. 2006, 6, 1473–1478. [Google Scholar] [CrossRef]
- Schold, J.D.; Kaplan, B.; Howard, R.J.; Reed, A.I.; Foley, D.P.; Meier-Kriesche, H.-U. Are We Frozen in Time? Analysis of the Utilization and Efficacy of Pulsatile Perfusion in Renal Transplantation. Arab. Archaeol. Epigr. 2005, 5, 1681–1688. [Google Scholar] [CrossRef]
- Wszola, M.; Kwiatkowski, A.; Domagala, P.; Wirkowska, A.; Bieniasz, M.; Diuwe, P.; Kieszek, R.; Durlik, M.; Chmura, A. Preservation of Kidneys by Machine Perfusion Influences Gene Expression and May Limit Ischemia/Reperfusion Injury. Prog. Transplant. 2014, 24, 19–26. [Google Scholar] [CrossRef]
- Gracia-Sancho, J.; Villarreal, G.; Zhang, Y.; Yu, J.X.; Liu, Y.; Tullius, S.G.; García-Cardeña, G. Flow Cessation Triggers Endothelial Dysfunction During Organ Cold Storage Conditions: Strategies for Pharmacologic Intervention. Transplantation 2010, 90, 142–149. [Google Scholar] [CrossRef] [Green Version]
- Bathini, V.; McGregor, T.; McAlister, V.C.; Luke, P.P.; Sener, A. Renal Perfusion Pump vs. Cold Storage for Donation After Cardiac Death Kidneys: A Systematic Review. J. Urol. 2013, 189, 2214–2220. [Google Scholar] [CrossRef]
- Tingle, S.J.; Figueiredo, R.S.; Moir, J.A.; Goodfellow, M.; Talbot, D.; Wilson, C.H. Machine perfusion preservation versus static cold storage for deceased donor kidney transplantation. Cochrane Database Syst. Rev. 2019, 3, CD011671. [Google Scholar] [CrossRef] [PubMed]
- Hameed, A.M.; Pleass, H.C.; Wong, G.; Hawthorne, W.J. Maximizing kidneys for transplantation using machine perfusion. Medicine 2016, 95, e5083. [Google Scholar] [CrossRef]
- Peng, P.; Ding, Z.; He, Y.; Zhang, J.; Wang, X.; Yang, Z. Hypothermic Machine Perfusion Versus Static Cold Storage in Deceased Donor Kidney Transplantation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Artif. Organs 2019, 43, 478–489. [Google Scholar] [CrossRef] [PubMed]
- Sirolli, V.; Pieroni, L.; Di Liberato, L.; Urbani, A.; Bonomini, M. Urinary Peptidomic Biomarkers in Kidney Diseases. Int. J. Mol. Sci. 2019, 21, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Waele, L.; Van Gaal, P.-J.; Abramowicz, D. Electrolytes disturbances after kidney transplantation. Acta Clin. Belg. 2019, 74, 48–52. [Google Scholar] [CrossRef]
- Filho, A.C.D.; Alves, J.R.; Da Cruz, P.R.C.; Santana, V.B.B.D.M.; Riccetto, C.L.Z.; Dias, A.C. Predicting urine output after kidney transplantation: Development and internal validation of a nomogram for clinical use. Int. Braz j Urol 2019, 45, 588–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swanson, K.J.; Aziz, F.; Garg, N.; Mohamed, M.; Mandelbrot, D.; Djamali, A.; Parajuli, S. Role of novel biomarkers in kidney transplantation. World J. Transplant. 2020, 10, 230–255. [Google Scholar] [CrossRef] [PubMed]
- Hollmen, M.E.; Kyllönen, L.E.; Inkinen, K.A.; Lalla, M.L.; Merenmies, J.; Salmela, K.T. Deceased donor neutrophil gelatinase-associated lipocalin and delayed graft function after kidney transplantation: A prospective study. Crit. Care 2011, 15, R121. [Google Scholar] [CrossRef] [Green Version]
- Hollmen, M.E.; Kyllönen, L.E.; Inkinen, K.A.; Lalla, M.L.; Salmela, K.T.; Kyll, L.E. Urine neutrophil gelatinase-associated lipocalin is a marker of graft recovery after kidney transplantation. Kidney Int. 2011, 79, 89–98. [Google Scholar] [CrossRef] [Green Version]
- A Eremenko, A.; Minbolatova, N.M.; Kaabak, M.M.; Babenko, N.N. Neutrophil gelatinase-associated lipocalin (u-NGAL) in the assessment of renal function in patients after kidney allotransplantation. Anesteziol. i Reanimatol. 2015, 59, 10–15. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Recipients Characteristics (Unit) | Value Description | Group 1 HMP Group (n = 22) | Group 2 SCS Group (n = 22) | p |
|---|---|---|---|---|
| Age (years) | Median Range | 55.0 34.0–69.0 | 54.0 33.0–70.0 | 0.36 |
| Sex (n/%) | Men—M Women—F | 15 (68.2%) 7 (31.8%) | 11 (50%) 11 (50%) | 0.22 |
| BMI (kg/m2) | Median Range | 27.3 23.2–28.1 | 27.9 24.1–30. 9 | 0.70 |
| Hemodialysis time (months) | Median Range | 37.0 18–53.5 | 48.0 24.5–60.0 | 0.43 |
| Serum urea (mg/dl) | Median Range | 101 75.0–140.0 | 85.5 55.0–111.0 | 0.19 |
| Serum creatinine (mg/dl) | Median Range | 7.4 5.6–9.4 | 7.9 6.6–8.6 | 0.99 |
| eGFR (ml/min/1.73 m2) | Median Range | 7.7 5.0–9.0 | 6.0 5.0–8.0 | 0.52 |
| Leukocytes (G/μL) | Median Range | 7.7 5.6–8.7 | 6.5 5.6–7.7 | 0.97 |
| Platelets (G/μL) | Median Range | 210.0 165.0–245.0 | 194.0 169.0–212.0 | 0.50 |
| Potassium (mmol/L) | Median Range | 4.5 4.2–4.7 | 4.6 4.6–4.7 | 0.40 |
| Hematocrit (l/l) | Median Range | 37.7 37.2–40.4 | 35.3 32.9–37 | 0.75 |
| Mismatch A | Median Range | 1 1–2 | 1 0–1 | 0.46 |
| Mismatch B | Median Range | 1 1–2 | 1 1–2 | 0.59 |
| Mismatch DR | Median Range | 1 0–1 | 1 1–1 | 0.50 |
| HLA mismatches sum | Median Range | 3 2–4 | 3 2–4 | 0.98 |
| * HLA mismatch preferential points | Median Range | 20 14–25 | 17 12–19 | 0.42 |
| DGF | Incidence | n = 2 (9.1%) | n = 3 (13.6%) | 0.60 |
| CIT (h) | Median Range | 18.4 4.5–26.9 | 11.6 4.9–22.9 | 0.07 |
| Tac/CsA (%) | IS | 95.5/4.5 | 95.5/4.5 | NA |
| MMF (%) | IS | 100 | 100 | NA |
| Steroids (%) | IS | 100 | 100 | NA |
| Group 1 (HMP) | Group 2 (SCS) | |||||||||||||||
| D | Cr | Ur | GFR | K | D | Cr | Ur | GFR | K | |||||||
| abs | abs | abs | Δ | abs | Δ | abs | Δ | abs | abs | abs | Δ | abs | Δ | abs | Δ | |
| ET-1 1 m * | ◯ | ⚫ | ⚫ | ⚫ | ◯ | ◯ | ||||||||||
| ET-1 30 m ** | ◯ | ⚫ | ⚫ | ◯ | ⚫ | |||||||||||
| ET-1 Δ ∗∗ | ◯ | ⚫ | ⚫ | ◯ | ||||||||||||
| ET-2 1 m | ◯ | ⚫ | ◯ | |||||||||||||
| ET-2 30 m # | ◯ | ◯ | ◯ | ⚫ | ⚫ | ◯ | ◯ | ⚫ | ◯ | ◯ | ⚫ | ⚫ | ||||
| ET-2 Δ | ◯ | ◯ | ◯ | |||||||||||||
| ET-3 1 m | ◯ | ⚫ | ||||||||||||||
| ET-3 30 m ## | ◯ | ⚫ | ◯ | ◯ | ⚫ | |||||||||||
| ET-3 Δ | ⚫ | ◯ | ||||||||||||||
| IL-18 1 m | ◯ | ⚫ | ◯ | |||||||||||||
| IL-18 30 m | ◯ | ◯ | ||||||||||||||
| IL-18 Δ + | ⚫ | ◯ | ◯ | ◯ | ⚫ | ⚫ | ⚫ | ◯ | ⚫ | |||||||
| NGAL 1 m ++ | ◯ | ⚫ | ||||||||||||||
| NGAL 30 m ++ | ⚫ | ◯ | ⚫ | |||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tejchman, K.; Nowacki, A.; Kotfis, K.; Skwirczynska, E.; Kotowski, M.; Zair, L.; Ostrowski, M.; Sienko, J. The Role of Endothelins, IL-18, and NGAL in Kidney Hypothermic Machine Perfusion. Biomedicines 2021, 9, 417. https://doi.org/10.3390/biomedicines9040417
Tejchman K, Nowacki A, Kotfis K, Skwirczynska E, Kotowski M, Zair L, Ostrowski M, Sienko J. The Role of Endothelins, IL-18, and NGAL in Kidney Hypothermic Machine Perfusion. Biomedicines. 2021; 9(4):417. https://doi.org/10.3390/biomedicines9040417
Chicago/Turabian StyleTejchman, Karol, Adam Nowacki, Katarzyna Kotfis, Edyta Skwirczynska, Maciej Kotowski, Labib Zair, Marek Ostrowski, and Jerzy Sienko. 2021. "The Role of Endothelins, IL-18, and NGAL in Kidney Hypothermic Machine Perfusion" Biomedicines 9, no. 4: 417. https://doi.org/10.3390/biomedicines9040417
APA StyleTejchman, K., Nowacki, A., Kotfis, K., Skwirczynska, E., Kotowski, M., Zair, L., Ostrowski, M., & Sienko, J. (2021). The Role of Endothelins, IL-18, and NGAL in Kidney Hypothermic Machine Perfusion. Biomedicines, 9(4), 417. https://doi.org/10.3390/biomedicines9040417