
Egyptian Pediatric Guidelines for the Management of Children with Isolated Thrombocytopenia Using the Adapted ADAPTE Methodology—A Limited-Resource Country Perspective

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
- Adapted from Source Guidelines:
- American Society of Hematology 2019 guidelines for immune thrombocytopenia [1].
- The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition [2].
- Management of severe perioperative bleeding: guidelines from the European Society of Anesthesiology [3].
- Fetal and neonatal alloimmune thrombocytopenia: recommendations for evidence-based practice, an international approach, 2019 [4].
- Guidelines on transfusion for fetuses, neonates and older children [5].
- Guidelines for the Laboratory Investigations of heritable disorders of platelet function [6].
- Updated international consensus report on the investigation and management of primary immune thrombocytopenia [7].
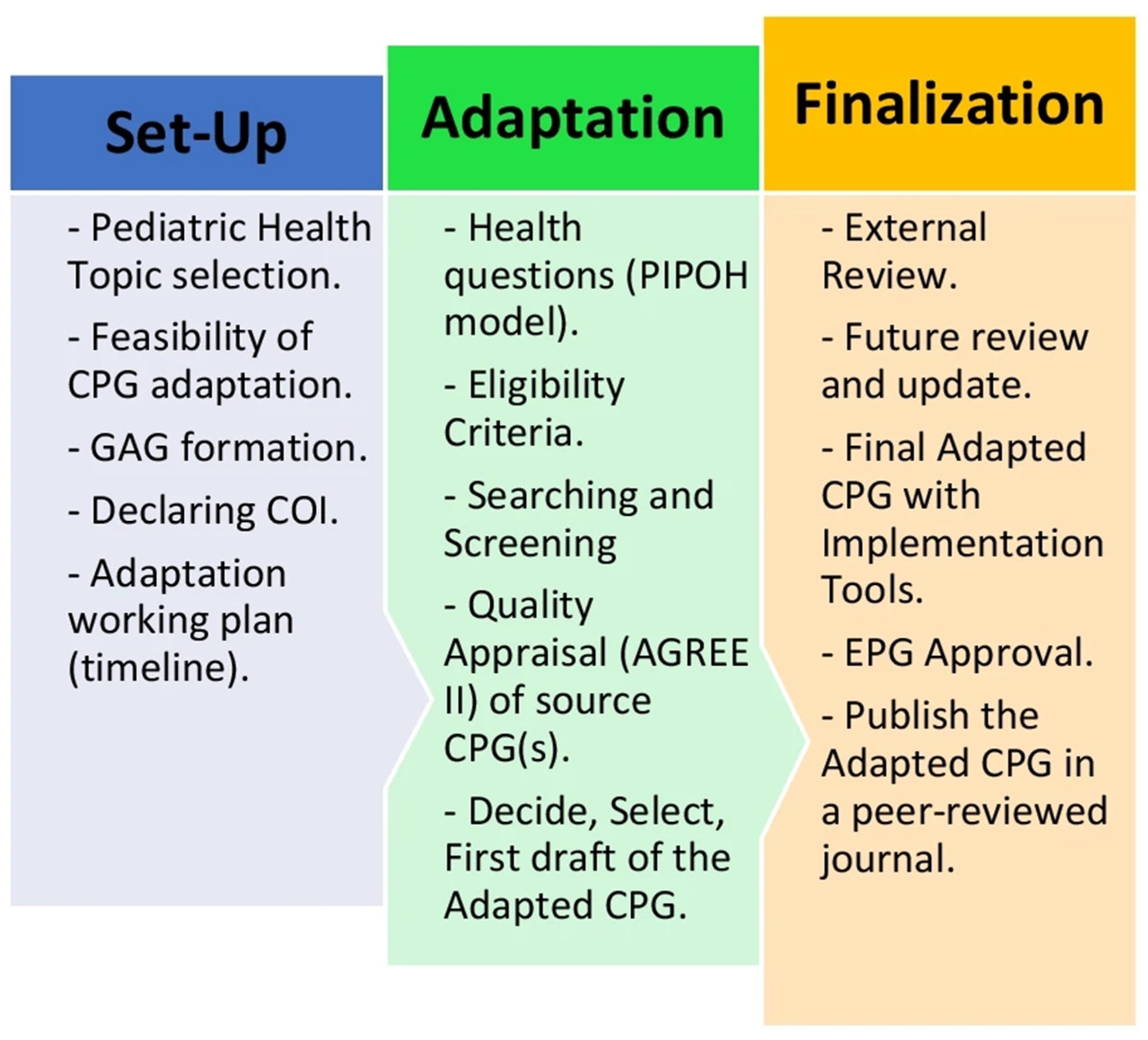
2. Materials and Methods
3. Results
- 1.
- Diagnosis of thrombocytopenia
- 1.1.
- What is a validated bleeding score used for neonates?
- 1.2.
- What is the initial evaluation for neonates presenting with bleeding and thrombocytopenia?
- 1.3.
- What is the initial evaluation for fetal/neonatal alloimmune thrombocytopenia (FNAIT)?
- 1.4.
- What are the antenatal diagnostic tests for possible FNAIT?
- 1.5.
- What are the points in history and examination suggestive of inherited thrombocytopenia in children?
- 1.6.
- What are the tests required to exclude inherited thrombocytopenia?
- 1.7.
- What is the initial evaluation for children and adolescents presenting with bleeding and thrombocytopenia?
- 1.8.
- What is a validated general bleeding score used for children?
- 1.9.
- What are the diagnostic criteria for immune thrombocytopenia?
- 1.10.
- What are the additional diagnostic tests required in children and adolescents with ITP?
- 1.11.
- What are the indications of bone marrow examination in patients with ITP?
- 1.12.
- What are the subsequent investigations in children and adolescents with persistent or chronic ITP?
- 1.13.
- When to suspect cyclic thrombocytopenia?
- 2.
- Treatment of isolated thrombocytopenia
- 2.1.
- What is the initial treatment of bleeding in a neonate with FNAIT?
- 2.2.
- What are the indications of platelet transfusion in a neonate with thrombocytopenia?
- 2.3.
- What is the management of a neonate of mother with ITP?
- (1)
- Management of delivery
- (2)
- Management after delivery
- 2.4.
- What are the indications of hospitalization in pediatric patients with ITP?
- 2.5.
- What is the initial treatment of pediatric patients with ITP?
- I.
- The watch-and-wait policy based on clinical classification
- II.
- Children with newly diagnosed ITP who have non-life-threatening mucosal bleeding and/or diminished HRQoL can start with any of the 1st line therapy:
- 2.6.
- What are the indications of platelet transfusion in pediatric patients with thrombocytopenia?
- I.
- In non-immune thrombocytopenia (2C).
- 2.7.
- What is the treatment of life-threatening bleeding in pediatric patient with thrombocytopenia?
- 2.8.
- What is the treatment of menorrhagia in adolescent girl with thrombocytopenia?
- 3.
- Prevention of bleeding in children and adolescents with isolated thrombocytopenia
- 3.1.
- How to prevent serious bleeding in a fetus/neonate with FNAIT?
At delivery:
- If the fetal platelet count is unknown, assisted delivery and invasive procedures on the fetus during delivery should be avoided, including forceps, vacuum-assisted delivery, scalp blood sampling and scalp electrodes (1D). Cesarian section is advised
- A cord blood sample should be sent for platelet count determination immediately after delivery (1C).
- Ideally, HPA-selected platelets should be available at the time of delivery (1C). Random platelets and IV Ig need to be available and are often effective.After delivery:
- In the absence of life-threatening bleeding in a neonate, such as intracranial or gastrointestinal bleeding, platelets should be transfused to maintain a platelet count above 30 × 109/L (1D).
- 3.2.
- How to prevent alloimmunization (maternal and transfusion related)?
- 3.3.
- What are the drugs to be avoided in a thrombocytopenic child with history of bleeding?
- 3.4.
- How to prevent bleeding in a thrombocytopenic child receiving antiplatelet medications?
- 3.5.
- How to prevent further bleeding in a thrombocytopenic child following trauma?
- 3.6.
- How to assess risk of bleeding in children during preoperative evaluation?
4. Discussion
5. Strength and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| aPTT | Activated partial thromboplastin time |
| AGREE II | Appraisal of Guidelines for REsearch and Evaluation (Version II) |
| CPG | Clinical practice guideline |
| CBC | Complete blood count |
| DAT | Direct antibody test |
| EPG | Egyptian Pediatric Clinical Practice Guidelines Committee |
| FNAIT | Fetal/neonatal alloimmune thrombocytopenia |
| FAST | Focused assessment with sonography in trauma |
| HRQoL | Health related quality of life |
| ITP | Immune thrombocytopenic purpura |
| Ig | Immunoglobulin |
| INR | International normalized ratio |
| IVIg | Intravenous immunoglobulins |
| ICH | Intracranial hemorrhage |
| ISTH-SCC BAT | International Society of Hemostasis and thrombosis–Bleeding assessment tool |
| NAIT | Neonatal allo-immune thrombocytopenia |
| NSAIDs | Non-steroidal anti-inflammatory drugs |
| PREPARE | Practice Guideline REgistry for transPAREncy |
| TXA | Tranexamic acid |
| TPO-Ras | Thrombopoietin receptor agonist |
| WBCT | Whole-body CT |
| WHO | World Health Organization |
References
- Neunert, C.; Terrell, D.R.; Arnold, D.M.; Buchanan, G.; Cines, D.B.; Cooper, N.; Cuker, A.; Despotovic, J.M.; George, J.N.; Grace, R.F.; et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2019, 3, 3829–3866. [Google Scholar] [CrossRef] [PubMed]
- Spahn, D.R.; Bouillon, B.; Cerny, V.; Duranteau, J.; Filipescu, D.; Hunt, B.J.; Komadina, R.; Maegele, M.; Nardi, G.; Riddez, L.; et al. The European guideline on management of major bleeding and coagulopathy following trauma: Fifth edition. Crit. Care 2019, 23, 98. [Google Scholar] [CrossRef] [PubMed]
- Kozek-Langenecker, S.A.; Ahmed, A.B.; Afshari, A.; Albaladejo, P.; Aldecoa, C.; Barauskas, G.; De Robertis, E.; Faraoni, D.; Filipescu, D.C.; Fries, D.; et al. Management of severe perioperative bleeding: Guidelines from the European Society of Anaesthesiology: First update 2016. Eur. J. Anaesthesiol. 2017, 34, 332–395. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, L.; Greinacher, A.; Murphy, M.F.; Bussel, J.; Bakchoul, T.; Corke, S.; Kjaer, M.; Kjeldsen-Kragh, J.; Bertrand, G.; Oepkes, D.; et al. Fetal and neonatal alloimmune thrombocytopenia: Recommendations for evidence-based practice, an international approach. Br. J. Haematol. 2019, 185, 549–562. [Google Scholar] [CrossRef] [PubMed]
- New, H.V.; Berryman, J.; Bolton-Maggs, P.H.; Cantwell, C.; Chalmers, E.A.; Davies, T.; Gottstein, R.; Kelleher, A.; Kumar, S.; Morley, S.L.; et al. Guidelines on transfusion for fetuses, neonates and older children. Br. J. Haematol. 2016, 175, 784–828. [Google Scholar] [CrossRef] [PubMed]
- Gomez, K.; Anderson, J.; Baker, P.; Biss, T.; Jennings, I.; Lowe, G.; Platton, S.; British Society for Haematology Guidelines. Clinical and laboratory diagnosis of heritable platelet disorders in adults and children: A British Society for Haematology Guideline. Br. J. Haematol. 2021, 195, 46–72. [Google Scholar] [CrossRef]
- Provan, D.; Arnold, D.M.; Bussel, J.B.; Chong, B.H.; Cooper, N.; Gernsheimer, T.; Ghanima, W.; Godeau, B.; González-López, T.J.; Grainger, J.; et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019, 3, 3780–3817. [Google Scholar] [CrossRef]
- Johnson, B.; Fletcher, S.J.; Morgan, N.V. Inherited thrombocytopenia: Novel insights into megakaryocyte maturation, proplatelet formation and platelet lifespan. Platelets 2016, 27, 519–525. [Google Scholar] [CrossRef]
- Stasi, R.; Amadori, S.; Osborn, J.; Newland, A.C.; Provan, D. Long-term outcome of otherwise healthy individuals with incidentally discovered borderline thrombocytopenia. PLoS Med. 2006, 3, e24. [Google Scholar] [CrossRef]
- Rodeghiero, F.; Stasi, R.; Gernsheimer, T.; Michel, M.; Provan, D.; Arnold, D.M.; Bussel, J.B.; Cines, D.B.; Chong, B.H.; Cooper, N.; et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: Report from an international working group. Blood 2009, 113, 2386–2393. [Google Scholar] [CrossRef]
- Stasi, R. How to approach thrombocytopenia. Hematol. Am. Soc. Hematol. Educ. Program 2012, 2012, 191–197. [Google Scholar] [CrossRef]
- Roberts, I.; Stanworth, S.; Murray, N.A. Thrombocytopenia in the neonate. Blood Rev. 2008, 22, 173–186. [Google Scholar] [CrossRef] [PubMed]
- Sola-Visner, M.; Saxonhouse, M.A.; Brown, R.E. Neonatal thrombocytopenia: What we do and don’t know. Early Hum. Dev. 2008, 84, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Marin, F.; Chavda, C.; Lampa, M.; Michelson, A.D.; Frelinger, A.L., III; Sola-Visner, M. Effects of in vitro adult platelet transfusions on neonatal hemostasis. J. Thromb. Haemost. 2011, 9, 1020–1028. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; Vasa, R.; Neumann, L.; Karpatkin, M. Thrombocytopenia in the high-risk infant. J. Pediatr. 1980, 97, 791–794. [Google Scholar] [CrossRef] [PubMed]
- Chakravorty, S.; Roberts, I. How I manage neonatal thrombocytopenia. Br. J. Haematol. 2012, 156, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Bussel, J.B.; Vander Haar, E.L.; Berkowitz, R.L. New developments in fetal and neonatal alloimmune thrombocytopenia. Am. J. Obstet. Gynecol. 2021, 225, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Noris, P.; Pecci, A. Hereditary thrombocytopenias: A growing list of disorders. Hematol. Am. Soc. Hematol. Educ. Program. 2017, 2017, 385–399. [Google Scholar] [CrossRef]
- Drachman, J.G. Inherited thrombocytopenia: When a low platelet count does not mean ITP. Blood 2004, 103, 390–398. [Google Scholar] [CrossRef]
- Terrell, D.R.; Beebe, L.A.; Vesely, S.K.; Neas, B.R.; Segal, J.B.; George, J.N. The incidence of immune thrombocytopenic purpura in children and adults: A critical review of published reports. Am. J. Hematol. 2010, 85, 174–180. [Google Scholar] [CrossRef]
- Khalifa, A.; Tolba, K.; El-Alfy, M.; Gadallah, M.; Ibrahim, F.H. Idiopathic thrombocytopenic purpura in Egyptian children. Acta Haematol. 1993, 90, 125–129. [Google Scholar] [CrossRef] [PubMed]
- ElAlfy, M.; Farid, S.; Abdel Maksoud, A. Predictors of chronic idiopathic thrombocytopenic purpura. Pediatr. Blood Cancer 2010, 54, 959–962. [Google Scholar] [CrossRef] [PubMed]
- Moussalem, M.; Yassine, N. Immune thrombocytopenic purpura in childhood: A Lebanese perspective. Mol. Immunol. 2003, 39, 1105–1110. [Google Scholar] [CrossRef] [PubMed]
- Heitink-Pollé, K.M.J.; Uiterwaal, C.S.P.M.; Porcelijn, L.; Tamminga, R.Y.J.; Smiers, F.J.; van Woerden, N.L.; Wesseling, J.; Vidarsson, G.; Laarhoven, A.G.; de Haas, M.; et al. Intravenous immunoglobulin vs observation in childhood immune thrombocytopenia: A randomized controlled trial. Blood 2018, 132, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Neunert, C.; Lim, W.; Cohen, A.; Solberg, L.; Crowther, M.A. The American Society of Hematology 2011 evidence-based practice guideline for immune thrombocytopenia. Blood 2011, 117, 4190–4207. [Google Scholar] [CrossRef] [PubMed]
- Dal, S.E.; Ersoy, Y.; Erkurt, M.A.; Yetkin, F.; Kuzucu, C.; Akdogan, O. An uncommon case of acute brucellosis presenting with severe thrombocytopenia. Intern. Med. 2012, 51, 3291–3293. [Google Scholar] [CrossRef]
- Kumar, S.; Nair, S.; Rajam, L. Case series of pediatric systemic lupus erythematosus from Kerala: Comparison with other Indian series. Int. J. Rheum. Dis. 2010, 13, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Hatta, K.; Kunishima, S.; Suganuma, H.; Tanaka, N.; Ohkawa, N.; Shimizu, T. A family having type 2B von Willebrand disease with a novel VWF p.R1308S mutation: Detection of characteristic platelet aggregates on peripheral blood smears as the key aspect of diagnosis. Thromb. Res. 2015, 136, 813–817. [Google Scholar] [CrossRef]
- Lee, A.C.; Li, C.H.; Wong, L.M. Childhood thrombocytopenia associated with Graves disease is distinct from idiopathic thrombocytopenic purpura. Pediatr. Hematol. Oncol. 2003, 20, 39–42. [Google Scholar] [CrossRef]
- Olaniyi, J.A. An Acute Leukaemia Masquerading as Immune Thrombocytopaenic Purpura (ITP)? A Case Report. Clin. Med. Case Rep. 2009, 2, 31–34. [Google Scholar] [CrossRef]
- Bhattacharjee, S.; Banerjee, M. Immune Thrombocytopenia Secondary to COVID-19: A Systematic Review. SN Compr. Clin. Med. 2020, 2, 2048–2058. [Google Scholar] [CrossRef]
- Tsao, H.S.; Chason, H.M.; Fearon, D.M. Immune thrombocytopenia (ITP) in a pediatric patient positive for SARS-CoV-2. Pediatrics 2020, 146, e20201419. [Google Scholar] [CrossRef]
- Patel, P.A.; Chandrakasan, S.; Mickells, G.E.; Yildirim, I.; Kao, C.M.; Bennett, C.M. Severe pediatric COVID-19 presenting with respiratory failure and severe thrombocytopenia. Pediatrics 2020, 146, e20201437. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Yang, B.; Li, Z.; Wang, P.; Chen, Y.; Zhou, H. Sudden severe thrombocytopenia in a patient in the recovery stage of COVID-19. Lancet Haematol. 2020, 7, e624. [Google Scholar] [CrossRef]
- Aster, R.H.; Bougie, D.W. Drug-induced immune thrombocytopenia. N. Engl. J. Med. 2007, 357, 580–587. [Google Scholar] [CrossRef] [PubMed]
- British Committee for Standards in Haematology General Haematology Task F. Guidelines for the investigation and management of idiopathic thrombocytopenic purpura in adults, children and in pregnancy. Br. J. Haematol. 2003, 120, 574–596. [Google Scholar] [CrossRef] [PubMed]
- Rotz, S.J.; Ware, R.E.; Kumar, A. Diagnosis and management of chronic and refractory immune cytopenias in children, adolescents, and young adults. Pediatr. Blood Cancer 2018, 65, e27260. [Google Scholar] [CrossRef]
- Monteagudo, M.; Amengual, M.J.; Munoz, L.; Soler, J.; Roig, I.; Tolosa, C. Reticulated platelets as a screening test to identify thrombocytopenia aetiology. QJM 2008, 101, 549–555. [Google Scholar] [CrossRef]
- Grimaldi-Bensouda, L.; Nordon, C.; Leblanc, T.; Abenhaim, L.; Allali, S.; Armari-Alla, C.; Berger, C.; Courcoux, M.-F.; Fouyssac, F.; Guillaumat, C.; et al. Childhood immune thrombocytopenia: A nationwide cohort study on condition management and outcomes. Pediatr. Blood Cancer 2017, 64, e26389. [Google Scholar] [CrossRef]
- Amer, Y.S.; Elzalabany, M.M.; Omar, T.I.; Ibrahim, A.G.; Dowidar, N.L. The ‘Adapted ADAPTE’: An approach to improve utilization of the ADAPTE guideline adaptation resource toolkit in the Alexandria Center for Evidence-Based Clinical Practice Guidelines. J. Eval. Clin. Pract. 2015, 21, 1095–1106. [Google Scholar] [CrossRef]
- Fervers, B.; Burgers, J.S.; Voellinger, R.; Brouwers, M.; Browman, G.P.; Graham, I.D.; Harrison, M.B.; Latreille, J.; Mlika-Cabane, N.; Paquet, L.; et al. Guideline adaptation: An approach to enhance efficiency in guideline development and improve utilisation. BMJ Qual. Saf. 2011, 20, 228–236. [Google Scholar] [CrossRef] [PubMed]
- The ADAPTE Collaboration. The ADAPTE Manual and Resource Toolkit for Guideline Adaptation. Version 2.0. 2009. Available online: https://g-i-n.net/get-involved/resources (accessed on 2 May 2023).
- Alshehri, A.F.; Almazroua, S.F.; Amer, Y.S. A review of the methodological frameworks adopted by the Eastern Mediterranean countries for adaptation of the global practice guidelines to the national context. East. Mediterr. Health J. 2023, 29, 540–553. [Google Scholar] [CrossRef] [PubMed]
- Abdel Baky, A.; Omar, T.; Amer, Y. Adapting global evidence-based practice guidelines to the Egyptian healthcare context: The Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) Initiative. Bull. Natl. Res. Cent. 2023, 47, 88. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in health care. CMAJ 2010, 182, E839–E842. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, M.C.; Florez, I.D.; McNair, S.A.; Vella, E.T.; Yao, X. Clinical Practice Guidelines: Tools to support high quality patient care. Semin. Nucl. Med. 2019, 49, 145–152. [Google Scholar] [CrossRef] [PubMed]
- AGREE II. AGREE Enterprise Website. Available online: https://www.agreetrust.org/resource-centre/agree-ii/ (accessed on 2 May 2023).
- Chen, Y.; Guyatt, G.H.; Munn, Z.; Florez, I.D.; Marušić, A.; Norris, S.L.; Kredo, T.; Qaseem, A. Clinical Practice Guidelines Registry: Toward Reducing Duplication, Improving Collaboration, and Increasing Transparency. Ann. Intern. Med. 2021, 174, 705–707. [Google Scholar] [CrossRef]
- Xun, Y.; Liu, H.; Meng, M.; Wang, Z.; Zhou, Q.; Yao, Y.; Su, R.; Luo, X.; Shi, Q.; Yang, N.; et al. Characteristics of guidelines registered on the PREPARE platform. J. Evid. Based Med. 2022, 15, 341–346. [Google Scholar] [CrossRef]
- Letsky, E.A.; Greaves, M. Maternal and Neonatal Haemostasis Working Party of the Haemostasis and Thrombosis Task Force of the British Society for Haematology. Br. J. Haematol. 1996, 95, 21–26. [Google Scholar]
- Israels, S.; Kahr, W.; Blanchette, V.; Luban, N.; Rivard, G.; Rand, M. Platelet disorders in children: A diagnostic approach. Pediatr. Blood Cancer 2011, 56, 975–983. [Google Scholar] [CrossRef]
- Bolton-Maggs, P.; Chalmers, E.; Collins, P.; Harrison, P.; Kitchen, S.; Liesner, R.; Minford, A.; Mumford, A.; Parapia, L.; Perry, D.; et al. A review of inherited platelet disorders with guidelines for their management on behalf of the UKHCDO. Br. J. Haematol. 2006, 135, 603–633. [Google Scholar] [CrossRef]
- Rodeghiero, F.; Pabinger, I.; Ragni, M.; Abdul-Kadir, R.; Berntorp, E.; Blanchette, V.; Bodó, I.; Casini, A.; Gresele, P.; Lassila, R.; et al. Fundamentals for a Systematic Approach to Mild and Moderate Inherited Bleeding Disorders: An EHA Consensus Report. Hemasphere 2019, 3, e286. [Google Scholar] [CrossRef] [PubMed]
- Ponnampalam, J. Trust Guideline for the Management of Newly Diagnosed Immune Thrombocytopenia (ITP) in Children 2021. Available online: https://www.nnuh.nhs.uk/publication/download/idiopathic-thrombocytopenic-purpura-in-children-ca1072-v5-1/ (accessed on 23 June 2023).
- Vernooij, R.W.; Alonso-Coello, P.; Brouwers, M.; Martínez García, L.; CheckUp Panel. Reporting Items for Updated Clinical Guidelines: Checklist for the Reporting of Updated Guidelines (CheckUp). PLoS Med. 2017, 14, e1002207. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Alonso-Coello, P.; Ballesteros, M.; Cluzeau, F.; Vernooij, R.W.M.; Arayssi, T.; Bhaumik, S.; Chen, Y.; Ghersi, D.; Langlois, E.V.; et al. A Reporting Tool for Adapted Guidelines in Health Care: The RIGHT-Ad@pt Checklist. Ann. Intern. Med. 2022, 175, 710–719. [Google Scholar] [CrossRef] [PubMed]
- RIGHT-Ad@pt Checklist. Reporting Items for Practice Guidelines in Healthcare (RIGHT). 2022. Available online: http://www.right-statement.org/extensions/13 (accessed on 2 May 2023).
- Venkatesh, V.; Curley, A.; Khan, R.; Clarke, P.; Watts, T.; Josephson, C.; Muthukumar, P.; New, H.; Seeney, F.; Morris, S.; et al. A novel approach to standardised recording of bleeding in a high risk neonatal population. ADC Fetal Neonatal Ed. 2013, 98, F260–F263. [Google Scholar] [CrossRef]


{kind=link}
| Domains | ||||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | Overall | Is CPG Recommended for Use? | |
| CPG1 | 95.9 | 100 | 100 | 95.9 | 89.7 | 92.6 | 95.7 | Yes |
| CPG2 | 87.9 | 82.9 | 83 | 85.7 | 75 | 64.6 | 79.9 | Yes |
| CPG3 | 77.4 | 77.4 | 73.7 | 100 | 73.7 | 73.7 | 79.3 | Yes |
| CPG4 | 87.7 | 78.7 | 89.1 | 87.7 | 81.6 | 87.7 | 85.4 | Yes |
| CPG5 | 89.7 | 84.4 | 89.1 | 89.7 | 79.6 | 89.7 | 87.0 | Yes |
| CPG6 | 74.7 | 74.7 | 94.3 | 100 | 89.3 | 92.9 | 87.7 | Yes |
| CPG7 | 95.6 | 96.9 | 97.5 | 100 | 83.2 | 89.7 | 93.8 | Yes |
| CPG8 | 33.3 | 55.6 | 25 | 83.3 | 58.3 | 66.7 | 46 | No |
| CPG9 | 33.3 | 77.8 | 22.9 | 83.3 | 66.7 | 66.7 | 50.1 | No |
| CPG10 | 11.1 | 55.6 | 25 | 83.3 | 66.7 | 66.7 | 49.2 | No |
| CPG11 | 33.3 | 77.8 | 22.9 | 55.6 | 58.3 | 66.7 | 45.7 | No |
| CPG12 | 11.1 | 11.1 | 4.2 | 38.9 | 33.3 | 66.7 | 23.6 | No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Evidence Level | Definition |
|---|---|
| Ia | Evidence obtained from meta-analysis of RCTs |
| Ib | Evidence obtained from ≥1 RCT |
| IIa | Evidence obtained from ≥1 well-designed controlled study without randomization |
| IIb | Evidence obtained from ≥1 other type of well-designed quasi-experimental study |
| III | Evidence obtained from well-designed non-experimental descriptive studies, such as comparative studies, correlated studies, and case studies |
| IV | Evidence obtained from expert committee reports or opinions and/or clinical experience of respected authorities |
| Grade of Recommendation | Definition | Level of Evidence |
|---|---|---|
| A | Requires ≥ 1 RCT as part of a body of literature of overall good quality and consistency addressing specific recommendation | Evidence levels Ia and Ib |
| B | Requires the availability of well-conducted clinical studies but no randomized clinical trials on the topic of recommendation | Evidence levels IIa, IIb and III |
| C | Requires evidence obtained from expert committee reports or opinions and/or clinical experiences of respected authorities. Indicates an absence of directly applicable clinical studies of good quality | Evidence level IV |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mokhtar, G.; Abdelbaky, A.; Adly, A.; Ezzat, D.; Abdel Hakeem, G.; Hassab, H.; Youssry, I.; Ragab, I.; Sherief, L.M.; Zakaria, M.; et al. Egyptian Pediatric Guidelines for the Management of Children with Isolated Thrombocytopenia Using the Adapted ADAPTE Methodology—A Limited-Resource Country Perspective. Children 2024, 11, 452. https://doi.org/10.3390/children11040452
Mokhtar G, Abdelbaky A, Adly A, Ezzat D, Abdel Hakeem G, Hassab H, Youssry I, Ragab I, Sherief LM, Zakaria M, et al. Egyptian Pediatric Guidelines for the Management of Children with Isolated Thrombocytopenia Using the Adapted ADAPTE Methodology—A Limited-Resource Country Perspective. Children. 2024; 11(4):452. https://doi.org/10.3390/children11040452
Chicago/Turabian StyleMokhtar, Galila, Ashraf Abdelbaky, Amira Adly, Dina Ezzat, Gehan Abdel Hakeem, Hoda Hassab, Ilham Youssry, Iman Ragab, Laila M. Sherief, Marwa Zakaria, and et al. 2024. "Egyptian Pediatric Guidelines for the Management of Children with Isolated Thrombocytopenia Using the Adapted ADAPTE Methodology—A Limited-Resource Country Perspective" Children 11, no. 4: 452. https://doi.org/10.3390/children11040452
APA StyleMokhtar, G., Abdelbaky, A., Adly, A., Ezzat, D., Abdel Hakeem, G., Hassab, H., Youssry, I., Ragab, I., Sherief, L. M., Zakaria, M., Hesham, M., Salama, N., Salah, N., Afifi, R. A. A., El-Ashry, R., Makkeyah, S., Adolf, S., Amer, Y. S., Omar, T. E. I., ... Florez, I. (2024). Egyptian Pediatric Guidelines for the Management of Children with Isolated Thrombocytopenia Using the Adapted ADAPTE Methodology—A Limited-Resource Country Perspective. Children, 11(4), 452. https://doi.org/10.3390/children11040452