
Colonic Volvulus in Children: Surgical Management of a Challenging Condition

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Clinical Features
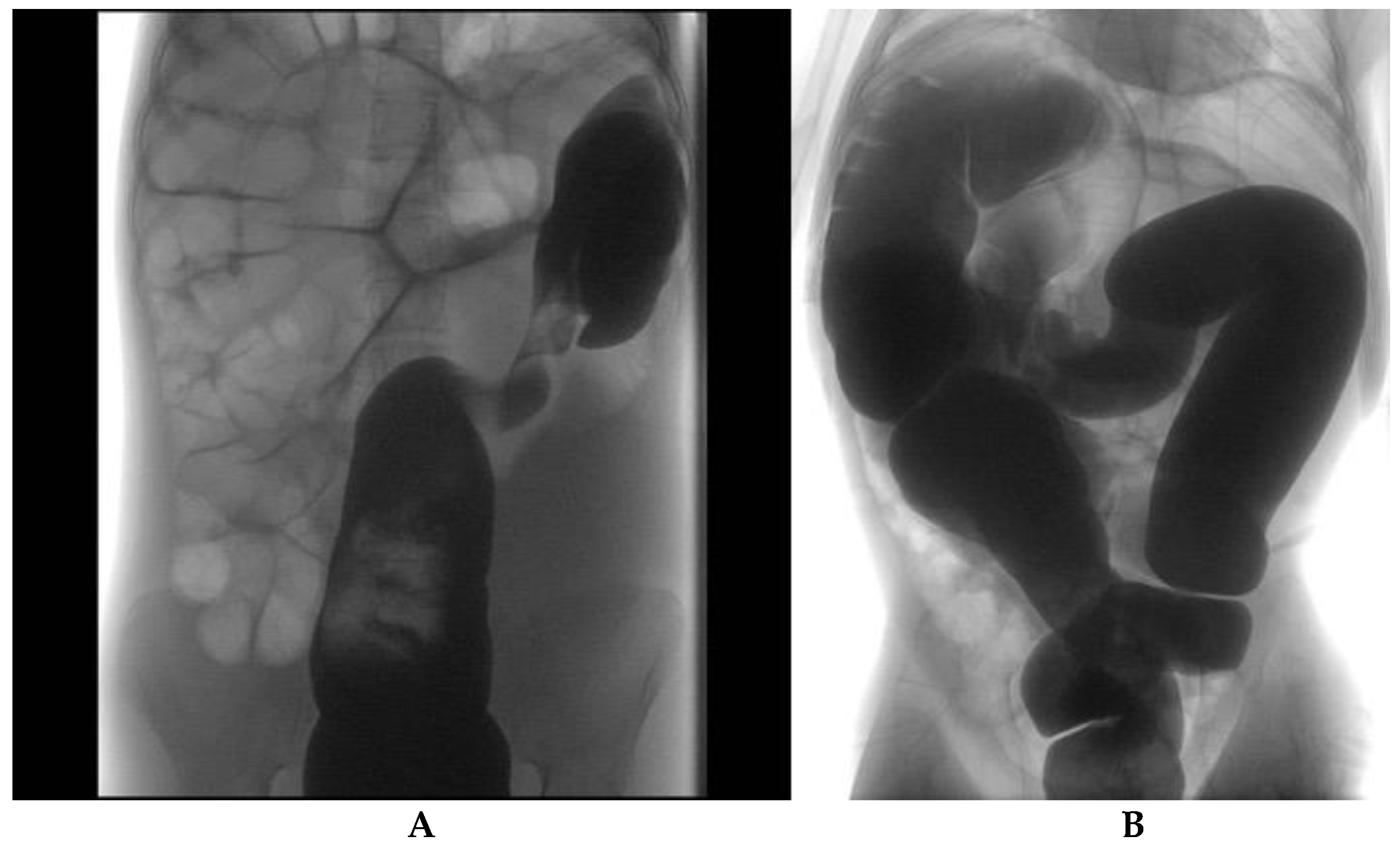
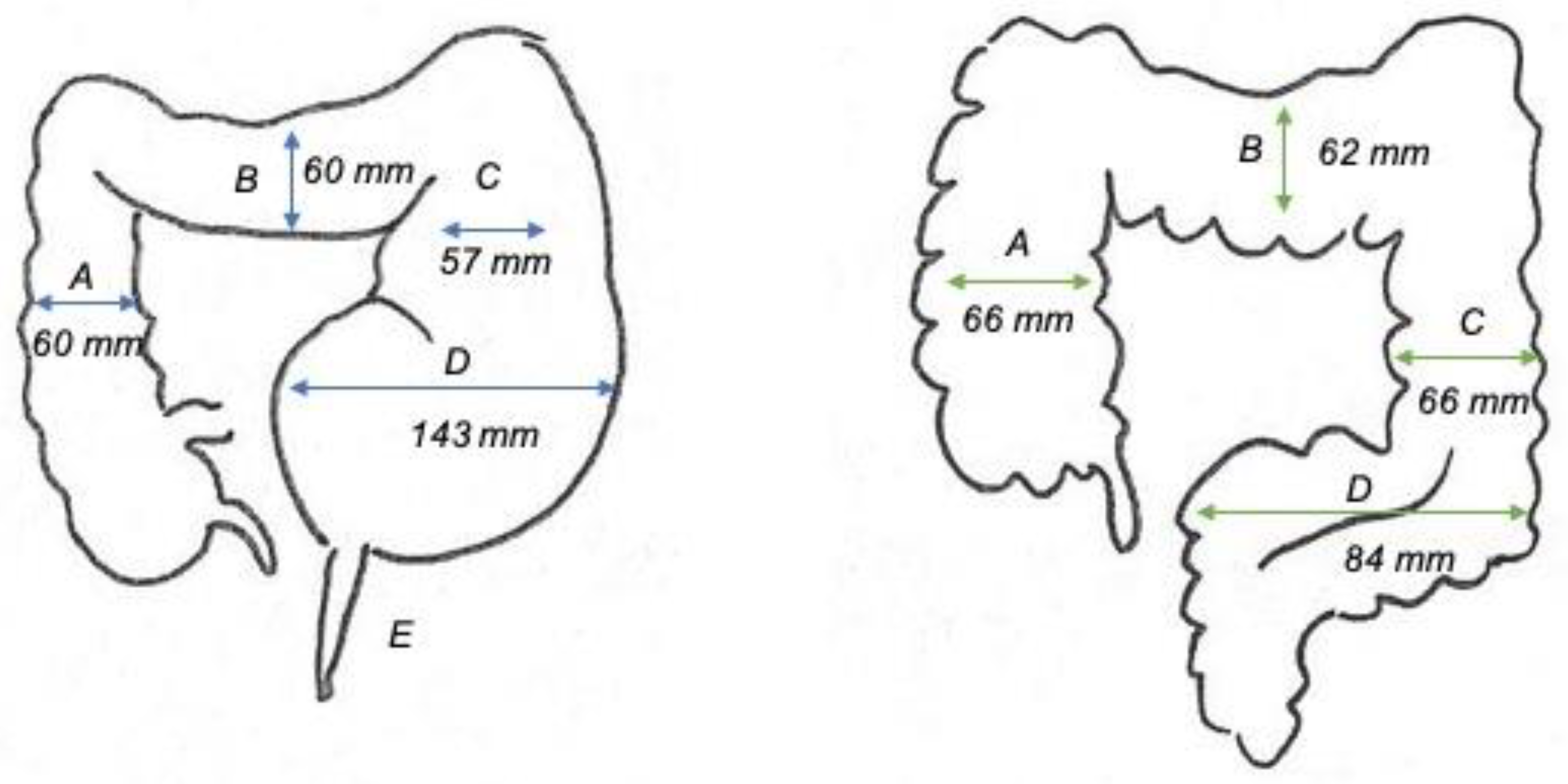
3.2. Instrumental Results
3.3. Surgical Management
3.4. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Atamanalp, S.S. Sigmoid volvulus. Eurasian J. Med. 2010, 42, 142–147. [Google Scholar] [CrossRef]
- Atamanalp, S.S. A new classification, treatment algorithm and prognosis-estimating system for sigmoid volvulus. Colorectal Dis. 2017, 19, 1033–1035. [Google Scholar] [CrossRef]
- Atamanalp, S.S. Reply to ‘Comments on a new classification, treatment algorithm and prognosis-estimating system for sigmoid volvulus: Factors affecting recurrence’. Colorectal Dis. 2018, 20, 821–822. [Google Scholar] [CrossRef]
- Catalano, O. Computed tomographic appearance of sigmoid volvulus. Abdom. Imaging 1996, 21, 314–317. [Google Scholar] [CrossRef]
- Ismail, A. Recurrent colonic volvulus in children. J. Pediatr. Surg. 1997, 32, 1739–1742. [Google Scholar] [CrossRef]
- Perrot, L.; Fohlen, A.; Alves, A.; Lubrano, J. Management of the colonic volvulus in 2016. J. Visc. Surg. 2016, 153, 183–192. [Google Scholar] [CrossRef]
- Salas, S.; Angel, C.A.; Salas, N.; Murillo, C.; Swischuk, L. Sigmoid volvulus in children and adolescents. J. Am. Coll. Surg. 2000, 190, 717–723. [Google Scholar] [CrossRef]
- Samuel, M.; Boddy, S.A.; Nicholls, E.; Capps, S. Large bowel volvulus in childhood. ANZ J. Surg. 2000, 70, 258–262. [Google Scholar] [CrossRef]
- Gingold, D.; Murrell, Z. Management of Colonic Volvulus. Clin. Colon Rectal Surg. 2012, 25, 236–244. [Google Scholar] [CrossRef] [Green Version]
- Bagarani, M.; Conde, A.S.; Longo, R.; Italiano, A.; Terenzi, A.; Venuto, G. Sigmoid volvulus in west Africa: A prospective study on surgical treatments. Dis. Colon Rectum. 1993, 36, 186–190. [Google Scholar] [CrossRef]
- Van Leeuwen, J.S. Sigmoid volvulus in a West African population. Dis. Colon Rectum. 1985, 28, 712–716. [Google Scholar] [CrossRef]
- Halabi, W.J.; Jafari, M.D.; Kang, C.Y.; Nguyen, V.Q.; Carmichael, J.C.; Mills, S.; Pigazzi, A.; Stamos, M.J. Colonic volvulus in the United States: Trends, outcomes, and predictors of mortality. Ann. Surg. 2014, 259, 293–301. [Google Scholar] [CrossRef]
- Raveenthiran, V.; Madiba, T.E.; Atamanalp, S.S.; De, U. Volvulus of the sigmoid colon. Colorectal Dis. 2010, 12, e1–e17. [Google Scholar] [CrossRef]
- Tan, F.L.S.; Tan, Y.-M.; Heah, S.M.; Seow-Choen, F. Adult Hirschsprung’s disease presenting as sigmoid volvulus: A case report and review of literature. Tech. Coloproctology 2006, 10, 245–248. [Google Scholar] [CrossRef]
- Atamanalp, S.S.; Yildirgan, M.I.; Başoğlu, M.; Kantarci, M.; Yılmaz, I. Sigmoid colon volvulus in children: Review of 19 cases. Pediatr. Surg. Int. 2004, 20, 492–495. [Google Scholar] [CrossRef]
- Atamanalp, S.S. Comments on "Hirschsprung’s Disease Complicated by Sigmoid Volvulus: A Systematic Review". Balkan Med. J. 2021, 38, 259. [Google Scholar] [CrossRef]
- Available, N.A.N.; Khanna, R.; Gangopadhyay, A.N.; Shahoo, S.P.; Khanna, A.K. Puneet Sigmoid volvulus in childhood: Report of six cases. Pediatr. Surg. Int. 2000, 16, 132–133. [Google Scholar] [CrossRef]
- Uylas, U.; Gunes, O.; Kayaalp, C. Hirschsprung’s Disease Complicated by Sigmoid Volvulus: A Systematic Review. Balkan Med. J. 2021, 38, 1–6. [Google Scholar]
- Kim, E.M.; Kang, B.M.; Kim, B.C.; Kim, J.Y.; Park, J.H.; Oh, B.Y.; Kim, J.W. Clinical outcomes of sigmoid volvulus and risk factors for its recurrence: A multicenter study in Korea. Int. J. Colorectal Dis. 2020, 35, 1841–1847. [Google Scholar] [CrossRef]
- Garel, C.; Blouet, M.; Belloy, F.; Petit, T.; Pelage, J.-P. Diagnosis of pediatric gastric, small-bowel and colonic volvulus. Pediatr. Radiol. 2015, 46, 130–138. [Google Scholar] [CrossRef]
- Dolejs, S.C.; Guzman, M.J.; Fajardo, A.D.; Holcomb, B.K.; Robb, B.W.; Waters, J.A. Contemporary Management of Sigmoid Vol-vulus. J. Gastrointest. Surg. 2018, 22, 1404–1411. [Google Scholar] [CrossRef]
- Colinet, S.; On behalf of the French-speaking Pediatric Hepatology Gastroenterology and Nutrition Group (GFHGNP); Rebeuh, J.; Gottrand, F.; Kalach, N.; Paquot, I.; Djeddi, D.; Le Henaff, G.; Rebouissoux, L.; Robert, V.; et al. Presentation and endoscopic management of sigmoid volvulus in children. Eur. J. Nucl. Med. Mol. Imaging 2015, 174, 965–969. [Google Scholar] [CrossRef]
- Parolini, F.; Orizio, P.; Bulotta, A.L.; Magne, M.G.; Boroni, G.; Cengia, G.; Torri, F.; Alberti, D. Endoscopic management of sigmoid volvulus in children. World J. Gastrointest. Endosc. 2016, 8, 439–443. [Google Scholar] [CrossRef]
- Lee, B.; Wu, A. Pediatric Sigmoid Volvulus. Pediatr. Emerg. Care 2019, 35, e232–e233. [Google Scholar] [CrossRef]
- Marine, M.B.; Cooper, M.L.; Delaney, L.R.; Jennings, S.G.; Rescorla, F.J.; Karmazyn, B. Diagnosis of pediatric colonic volvulus with abdominal radiography: How good are we? Pediatr. Radiol. 2017, 47, 404–410. [Google Scholar] [CrossRef]
- Folaranmi, S.E.; Cho, A.; Tareen, F.; Morabito, A.; Rakoczy, G.; Cserni, T. Proximal large bowel volvulus in children: 6 new cas-es and review of the literature. J. Pediatr. Surg. 2012, 47, 1572–1575. [Google Scholar] [CrossRef]
- Khalayleh, H.; Koplewitz, B.Z.; Kapuller, V.; Armon, Y.; Abu-Leil, S.; Arbell, D. Neonatal sigmoid volvulus. J. Pediatr. Surg. 2016, 51, 1782–1785. [Google Scholar] [CrossRef]
- Parolini, F.; Alberti, D. Sigmoid volvulus in children. Surgeons 2016, 161, 562–563. [Google Scholar] [CrossRef]
- Ranjan, A.; Jain, V.; Sharma, S.; Gupta, D.K. Sigmoid volvulus: An uncommon complication of Hirschsprung’s disease. BMJ Case Rep. 2016, bcr2016214693. [Google Scholar] [CrossRef]
- Daly, M.; Zarate-Lopez, N. Functional gastrointestinal disorders: History taking skills in practice. Clin. Med. 2021, 21, e480–e486. [Google Scholar] [CrossRef]
- Davies, C.; Mishra, D.; Eshraghi, R.S.; Mittal, J.; Sinha, R.; Bulut, E.; Mittal, R.; Eshraghi, A.A. Altering the gut microbiome to po-tentially modulate behavioral manifestations in autism spectrum disorders: A systematic review. Neurosci. Biobehav. Rev. 2021, 128, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.-H.; Jeng, C.-M.; Chen, D.-F.; Lin, L.-H. A case report and literature review of sigmoid volvulus in children. Medicine 2017, 96, e9434. [Google Scholar] [CrossRef]
- Osiro, S.; Cunningham, D.; Shoja, M.M.; Tubbs, R.S.; Gielecki, J.; Loukas, M. Article Commentary: The Twisted Colon: A Review of Sigmoid Volvulus. Am. Surg. 2012, 78, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.D.; Golladay, E.S.; Wagner, C.; Seibert, J.J. Sigmoid Volvulus in Childhood. South. Med. J. 1990, 83, 778–781. [Google Scholar] [CrossRef] [PubMed]
- Tannouri, S.; Hendi, A.; Gilje, E.; Grissom, L.; Katz, D. Pediatric colonic volvulus: A single-institution experience and review. J. Pediatr. Surg. 2017, 52, 1062–1066. [Google Scholar] [CrossRef] [PubMed]
- Fujiya, K.; Chong, J.-M.; Ando, M.; Akita, H.; Fukuda, A.; Nagahama, T.; Arai, K. Sigmoid volvulus is associated with a decrease in enteric plexuses and ganglion cells: A case–control study. Int. J. Colorectal Dis. 2015, 30, 673–678. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Pt | Sex | Age (Years) | Associated Anomalies | Previous Abdominal Surgery | History of Chronic Constipation | Segment Involved |
|---|---|---|---|---|---|---|
| 1 | M | 15 | None | None | No | Sigmoid |
| 2 | F | 15 | Hirschsprung’s disease | None | Yes | Sigmoid |
| 3 | M | 15 | None | None | No | Sigmoid |
| 4 | F | 10 | Hirschsprung’s disease | None | Yes | Sigmoid |
| 5 | M | 7 | None | None | Yes | Sigmoid |
| 6 | F | 14 | Cerebral palsy, autism, anterior anus; simultaneous splenic, gastric and pancreatic volvulus | None | Yes | Sigmoid |
| 7 | F | 11 | None | None | Yes | Sigmoid |
| 8 | F | 15 | Acquired cerebral palsy | None | Yes | Sigmoid |
| 9 | F | 15 | Hirschsprung’s disease; Ito syndrome, cerebral palsy | None | Yes | Transverse |
| 10 | M | 11 | Infantile cerebral palsy post meningoencephalitis | Yes (ventriculoperitoneal shunt placement) | Yes | Transverse |
| 11 | F | 14 | Dystonic spastic tetraparesis, kernicterus | Yes (videolaparoscopic surgery, Nissen, gastrostomy) | Yes | Total colon |
| Sigmoid Diameter (mm) | Left Colon Diameter (mm) | Transverse Diameter (mm) | Right Colon Diameter (mm) | |
|---|---|---|---|---|
| All cases | 102 ± 41 | 63 ± 18 | 61 ± 17 | 64 ± 17 |
| HD patients | 143 ± 49 | 57 ± 17 | 60 ± 20 | 60 ± 23 |
| Non-HD patients | 84 ± 22 | 66 ± 19 | 62 ± 18 | 66 ± 16 |
| Pt | Associated Anomalies | Treatment Upon Admittance (Effect) | Surgery | Follow-Up |
|---|---|---|---|---|
| 1 | None | Endoscopic detorsion (success) | Sigmoid resection (VLS converted to open) | Uneventful |
| 2 | Hirschsprung’s disease | Endoscopic detorsion (failure: sigmoid resection and colostomy) | Soave pull-through (open) | Uneventful |
| 3 | None | Endoscopic detorsion (recurrency) | Left hemicolectomy (VLS-SILS port) | Uneventful |
| 4 | Hirschsprung’s disease | Endoscopic detorsion (success) | Soave pull-through (VLS) | Uneventful |
| 5 | None | Radiologic detorsion (success) | Sigmoid resection (VLS) | Uneventful |
| 6 | Psychomotor retardation, autism, anterior anus; simultaneous splenic, gastric and pancreatic volvulus | Surgery: sigmoid detorsion, splenectomy, temporary ileostomy (success) | Total colectomy (VLS) | Anastomotic stenosis (redo anastomosis); periodic episodes of intestinal sub-obstruction |
| 7 | None | Radiologic detorsion (success) | Sigmoid resection (VLS) | Uneventful |
| 8 | Acquired psychomotor retardation | Radiologic detorsion (success) | Refused by parents | N/D |
| 9 | Hirschsprung’s disease; Ito syndrome, psychomotor retardation | Colostomy (persistent intestinal obstruction) | Total colectomy, pouch ileoanal anastomosis, ileostomy (open) | Uneventful |
| 10 | Infantile cerebral palsy post meningoencephalitis | Surgery: transverse detorsion and colopexy (persistent intestinal obstruction) | Total colectomy, ileostomy (open) | Two episodes of intestinal sub-obstruction |
| 11 | Dystonic spastic tetraparesis, kernicterus | Surgery: detorsion and colopexy (open) | No | Uneventful |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Destro, F.; Maestri, L.; Meroni, M.; Campari, A.; Pederiva, F.; Costanzo, S.; Del Re, G.; Roveri, M.; Zuccotti, G.; Calcaterra, V.; et al. Colonic Volvulus in Children: Surgical Management of a Challenging Condition. Children 2021, 8, 982. https://doi.org/10.3390/children8110982
Destro F, Maestri L, Meroni M, Campari A, Pederiva F, Costanzo S, Del Re G, Roveri M, Zuccotti G, Calcaterra V, et al. Colonic Volvulus in Children: Surgical Management of a Challenging Condition. Children. 2021; 8(11):982. https://doi.org/10.3390/children8110982
Chicago/Turabian StyleDestro, Francesca, Luciano Maestri, Milena Meroni, Alessandro Campari, Federica Pederiva, Sara Costanzo, Giulia Del Re, Margherita Roveri, Gianvincenzo Zuccotti, Valeria Calcaterra, and et al. 2021. "Colonic Volvulus in Children: Surgical Management of a Challenging Condition" Children 8, no. 11: 982. https://doi.org/10.3390/children8110982
APA StyleDestro, F., Maestri, L., Meroni, M., Campari, A., Pederiva, F., Costanzo, S., Del Re, G., Roveri, M., Zuccotti, G., Calcaterra, V., & Pelizzo, G. (2021). Colonic Volvulus in Children: Surgical Management of a Challenging Condition. Children, 8(11), 982. https://doi.org/10.3390/children8110982