
Effectiveness and Acceptability of Telerehabilitation in Physical Therapy during COVID-19 in Children: Findings of a Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Information Sources and Search Strategy
2.3. Data Abstraction and Quality Assessment
3. Results
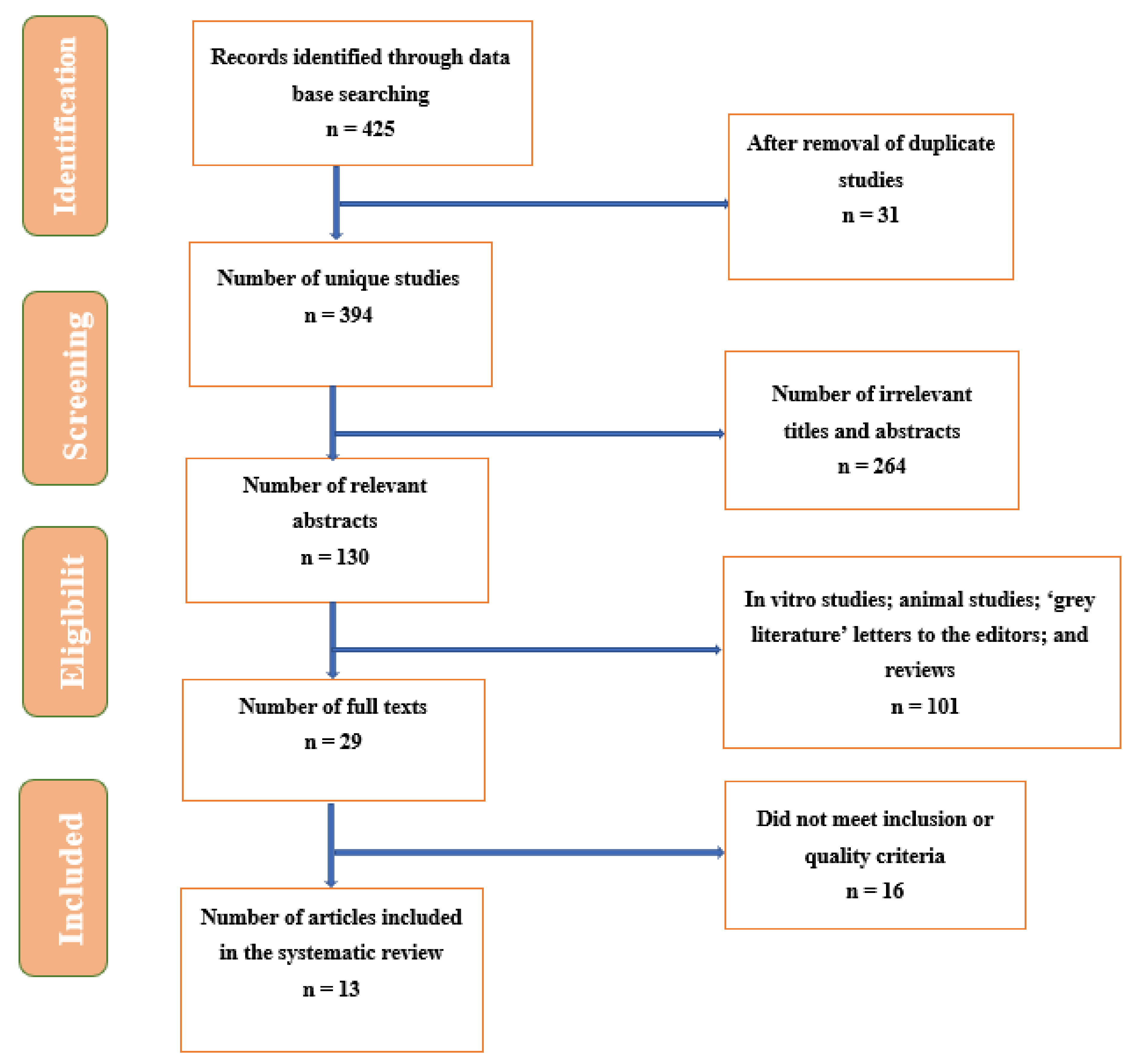
3.1. Findings of the Search Strategy
3.2. Characteristics of the Eligible Studies
3.3. Synthesis and Review of Findings Summarizing the Effectiveness and Acceptability of Telerehabilitation in PT during COVID-19 in Children
4. Discussion
4.1. Strengths and Limitations
4.2. Future Implications for Clinical Practice and Research
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Seron, P.; Oliveros, M.-J.; Gutierrez-Arias, R.; Fuentes-Aspe, R.; Torres-Castro, R.C.; Merino-Osorio, C.; Nahuelhual, P.; Inostroza, J.; Jalil, Y.; Solano, R.; et al. Effectiveness of Telerehabilitation in Physical Therapy: A Rapid Overview. Phys. Ther. 2021, 101, pzab053. [Google Scholar] [CrossRef] [PubMed]
- Rabatin, A.E.; Lynch, M.E.; Severson, M.C.; Brandenburg, J.E.; Driscoll, S.W. Pediatric telerehabilitation medicine: Making your virtual visits efficient, effective and fun. J. Pediatr. Rehabil. Med. 2020, 13, 355–370. [Google Scholar] [CrossRef] [PubMed]
- Damiano, D.L. Activity, Activity, Activity: Rethinking Our Physical Therapy Approach to Cerebral Palsy. Phys. Ther. 2006, 86, 1534–1540. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.; Gorter, J.W. The ‘F-words’ in childhood disability: I swear this is how we should think! Child. Care Health Dev. 2012, 38, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; McIntyre, S.; Morgan, C.; Campbell, L.; Dark, L.; Morton, N.; Stumbles, E.; Wilson, S.-A.; Goldsmith, S. A systematic review of interventions for children with cerebral palsy: State of the evidence. Dev. Med. Child. Neurol. 2013, 55, 885–910. [Google Scholar] [CrossRef] [PubMed]
- Camden, C.; Wilson, B.; Kirby, A.; Sugden, D.; Missiuna, C. Best practice principles for management of children with developmental coordination disorder (DCD): Results of a scoping review. Child. Care Health Dev. 2014, 41, 147–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zampolini, M.; Todeschini, E.; Guitart, M.B.; Hermens, H.; Ilsbroukx, S.; Macellari, V.; Magni, R.; Rogante, M.; Marchese, S.S.; Vollenbroek, M.; et al. Tele-rehabilitation: Present and future. Ann. Dell’istituto Super. Di Sanità 2008, 44, 125–134. [Google Scholar]
- Cruz, V.T.; Pais, J.; Bento, V.; Mateus, C.; Colunas, M.; Alves, I.; Coutinho, P.; Rocha, N. A Rehabilitation Tool Designed for Intensive Web-Based Cognitive Training: Description and Usability Study. JMIR Res. Protoc. 2013, 2, e59. [Google Scholar] [CrossRef]
- Kayyali, R.; Hesso, I.; Mahdi, A.; Hamzat, O.; Adu, A.; Gebara, S.N. Telehealth: Misconceptions and experiences of healthcare professionals in England. Int. J. Pharm. Pr. 2017, 25, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Edirippulige, S.; Reyno, J.; Armfield, N.; Bambling, M.; Lloyd, O.; McNevin, E. Availability, spatial accessibility, utilisation and the role of telehealth for multi-disciplinary paediatric cerebral palsy services in Queensland. J. Telemed. Telecare 2016, 22, 391–396. [Google Scholar] [CrossRef]
- Demers, M.; Martinie, O.; Winstein, C.; Robert, M.T. Active Video Games and Low-Cost Virtual Reality: An Ideal Therapeutic Modality for Children with Physical Disabilities During a Global Pandemic. Front. Neurol. 2020, 11, 601898. [Google Scholar] [CrossRef]
- Iacono, T.; Stagg, K.; Pearce, N.; Chambers, A.H. A scoping review of Australian allied health research in ehealth. BMC Heal. Serv. Res. 2016, 16, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Ekeland, A.G.; Bowes, A.; Flottorp, S. Effectiveness of telemedicine: A systematic review of reviews. Int. J. Med. Informatics 2010, 79, 736–771. [Google Scholar] [CrossRef] [Green Version]
- Seidman, Z.; McNamara, R.; Wootton, S.; Leung, R.; Spencer, L.; Dale, M.; Dennis, S.; McKeough, Z. People attending pulmonary rehabilitation demonstrate a substantial engagement with technology and willingness to use telerehabilitation: A survey. J. Physiother. 2017, 63, 175–181. [Google Scholar] [CrossRef]
- Russell, T.G. Physical rehabilitation using telemedicine. J. Telemed. Telecare 2007, 13, 217–220. [Google Scholar] [CrossRef]
- Dantas, L.O.; Barreto, R.P.G.; Ferreira, C.H.J. Digital physical therapy in the COVID-19 pandemic. Braz. J. Phys. Ther. 2020, 24, 381–383. [Google Scholar] [CrossRef]
- International Network of Physiotherapy Regulatory Authorities. Report of the Wcpt/INPTRA digital physical therapy practice task force. World Confed. Phys. Ther. 2020, 2020, 1–24. [Google Scholar]
- Camden, C.; Pratte, G.; Fallon, F.; Couture, M.; Berbari, J.; Tousignant, M. Diversity of practices in telerehabilitation for children with disabilities and effective intervention characteristics: Results from a systematic review. Disabil. Rehabil. 2019, 42, 3424–3436. [Google Scholar] [CrossRef]
- Bettger, J.P.; Resnik, L.J. Telerehabilitation in the Age of COVID-19: An Opportunity for Learning Health System Research. Phys. Ther. 2020, 100, 1913–1916. [Google Scholar] [CrossRef]
- Kairy, D.; Lehoux, P.; Vincent, C.; Visintin, M. A systematic review of clinical outcomes, clinical process, healthcare utilization and costs associated with telerehabilitation. Disabil. Rehabil. 2009, 31, 427–447. [Google Scholar] [CrossRef]
- Suso-Martí, L.; La Touche, R.; Herranz-Gómez, A.; Angulo-Díaz-Parreño, S.; Paris-Alemany, A.; Cuenca-Martínez, F. Effectiveness of Telerehabilitation in Physical Therapist Practice: An Umbrella and Mapping Review with Meta–Meta-Analysis. Phys. Ther. 2021, 101, pzab075. [Google Scholar] [CrossRef]
- Dias, J.F.; Oliveira, V.C.; Borges, P.R.T.; Dutra, F.C.M.S.; Mancini, M.C.; Kirkwood, R.N.; Resende, R.A.; Sampaio, R.F. Effectiveness of exercises by telerehabilitation on pain, physical function and quality of life in people with physical disabilities: A systematic review of randomised controlled trials with GRADE recommendations. Br. J. Sports Med. 2020, 55, 155–162. [Google Scholar] [CrossRef]
- Amatya, B.; Galea, M.; Kesselring, J.; Khan, F. Effectiveness of telerehabilitation interventions in persons with multiple sclerosis: A systematic review. Mult. Scler. Relat. Disord. 2015, 4, 358–369. [Google Scholar] [CrossRef]
- Johansson, T.; Wild, C. Telerehabilitation in stroke care—a systematic review. J. Telemed. Telecare 2011, 17, 1–6. [Google Scholar] [CrossRef]
- Prabawa, I.M.Y.; Silakarma, D.; Widnyana, M. Telerehabilitation as a physical therapy solution for post-stroke patient in COVID-19 pandemic situations: A review. Multidiscip. J. Sci. Med. Res. 2021, 12, 1–5. [Google Scholar]
- Mark, M.; Finley, J.R.; Brazelton, A.; Kozel, C.E.; Waterman, J.; Binkley, J. Implementation and outcomes of telerehabilitation to deliver evidence based physical therapy to breast cancer patients. Rehabil. Oncology. 2021, 39, E31. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Brindle, M.E.; Gawande, A. Managing COVID-19 in Surgical Systems. Ann. Surg. 2020, 272, e1–e2. [Google Scholar] [CrossRef]
- Potdar, R.D.; Sahariah, S.A.; Gandhi, M.; Kehoe, S.H.; Brown, N.; Sane, H.; Dayama, M.; Jha, S.; Lawande, A.; Coakley, P.J.; et al. Improving women’s diet quality preconceptionally and during gestation: Effects on birth weight and prevalence of low birth weight—a randomized controlled efficacy trial in India (Mumbai Maternal Nutrition Project). Am. J. Clin. Nutr. 2014, 100, 1257–1268. [Google Scholar] [CrossRef] [Green Version]
- Sobierajska-Rek, A.; Mański, Ł.; Jabłońska-Brudło, J.; Śledzińska, K.; Wasilewska, E.; Szalewska, D. Respiratory Telerehabilitation of Boys and Young Men with Duchenne Muscular Dystrophy in the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 6179. [Google Scholar] [CrossRef]
- Pamela Frigerio, L.D.M.; Sotgiu, A.; de Giacomo, C.; Vignoli, A. Parents’ Satisfaction of Tele-Rehabilitation for Children with Neurodevelopmental Disabilities During the Covid-19 Pandemic. BMC Fam. Pract. 2021. (in preprint). [Google Scholar] [CrossRef]
- Sobierajska-Rek, A.; Mański, Ł.; Jabłońska-Brudło, J.; JŚledzińska, K.; Ucińska, A.; Wierzba, J. Establishing a telerehabilitation program for patients with Duchenne muscular dystrophy in the COVID-19 pandemic. Wien. Klin. Wochenschr. 2021, 133, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Tanner, L.R.; Grinde, K.; McCormick, C. The Canadian Occupational Performance Measure: A Feasible Multidisciplinary Outcome Measure for Pediatric Telerehabilitation. Int. J. Telerehabil. 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Bican, R.; Christensen, C.; Fallieras, K.; Sagester, G.; O’Rourke, S.; Byars, M.; Tanner, K. Rapid Implementation of Telerehabilitation for Pediatric Patients During COVID-19. Int. J. Telerehabil. 2021, 13. [Google Scholar] [CrossRef]
- Romano, A.; Di Rosa, G.; Tisano, A.; Fabio, R.A.; Lotan, M. Effects of a remotely supervised motor rehabilitation program for individuals with Rett syndrome at home. Disabil. Rehabil. 2021, 2021, 1–11. [Google Scholar] [CrossRef]
- Krasovsky, T.; Silberg, T.; Barak, S.; Eisenstein, E.; Erez, N.; Feldman, I.; Guttman, D.; Liber, P.; Patael, S.; Sarna, H.; et al. Transition to Multidisciplinary Pediatric Telerehabilitation during the COVID-19 Pandemic: Strategy Development and Implementation. Int. J. Environ. Res. Public Health 2021, 18, 1484. [Google Scholar] [CrossRef]
- Provenzi, L.; Grumi, S.; Gardani, A.; Aramini, V.; Dargenio, E.; Naboni, C.; Vacchini, V.; Borgatti, R. Engaging with Families through On-line Rehabilitation for Children during the Emergency (EnFORCE) Group Italian parents welcomed a telehealth family-centred rehabilitation programme for children with disability during COVID-19 lockdown. Acta Paediatr. 2021, 110, 194–196. [Google Scholar] [CrossRef]
- Hall, J.B.; Woods, M.L.; Luechtefeld, J.T. Pediatric Physical Therapy Telehealth and COVID-19: Factors, Facilitators, and Barriers Influencing Effectiveness—a Survey Study. Pediatr. Phys. Ther. 2021, 33, 112–118. [Google Scholar] [CrossRef]
- Gagnon, M.; Merlo, G.M.; Yap, R.; Collins, J.; Elfassy, C.; Sawatzky, B.; Marsh, J.; Hamdy, R.; Veilleux, L.-N.; Dahan-Oliel, N. Using Telerehabilitation to Deliver a Home Exercise Program to Youth with Arthrogryposis: Single Cohort Pilot Study. J. Med. Internet Res. 2021, 23, e27064. [Google Scholar] [CrossRef]
- Assenza, C.; Catania, H.; Antenore, C.; Gobbetti, T.; Gentili, P.; Paolucci, S.; Morelli, D. Continuity of Care During COVID-19 Lockdown: A Survey on Stakeholders’ Experience with Telerehabilitation. Front. Neurol. 2021, 11, 617276. [Google Scholar] [CrossRef]
- Tanner, K.; Bican, R.; Boster, J.; Christensen, C.; Coffman, C.; Fallieras, K.; Long, R.; Mansfield, C.; O’Rourke, S.; Pauline, L.; et al. Feasibility and Acceptability of Clinical Pediatric Telerehabilitation Services. Int. J. Telerehabil. 2020, 12, 43–52. [Google Scholar] [CrossRef]
- Iannizzotto, G.; Nucita, A.; Fabio, R.A.; Caprì, T.; Bello, L.L. Remote Eye-Tracking for Cognitive Telerehabilitation and Interactive School Tasks in Times of COVID-19. Information 2020, 11, 296. [Google Scholar] [CrossRef]
- Mani, S.; Sharma, S.; Omar, B.; Paungmali, A.; Joseph, L. Validity and reliability of Internet-based physiotherapy assessment for musculoskeletal disorders: A systematic review. J. Telemed. Telecare 2017, 23, 379–391. [Google Scholar] [CrossRef]
- Piga, M.; Cangemi, I.; Mathieu, A.; Cauli, A. Telemedicine for patients with rheumatic diseases: Systematic review and proposal for research agenda. Semin. Arthritis Rheum. 2017, 47, 121–128. [Google Scholar] [CrossRef]
- Grona, S.L.; Bath, B.; Busch, A.; Rotter, T.; Trask, C.; Harrison, E. Use of videoconferencing for physical therapy in people with musculoskeletal conditions: A systematic review. J. Telemed. Telecare 2018, 24, 341–355. [Google Scholar] [CrossRef]
- DeFre Galea, M. Telemedicine in Rehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2019, 30, 473–483. [Google Scholar] [CrossRef]
- Howard, I.M.; Kaufman, M.S. Telehealth applications for outpatients with neuromuscular or musculoskeletal disorders. Muscle Nerve 2018, 58, 475–485. [Google Scholar] [CrossRef]
- Brennan, D.; Tindall, L.; Theodoros, D.; Brown, J.; Campbell, M.; Christiana, D.; Smith, D.; Cason, J.; Lee, A. A Blueprint for Telerehabilitation Guidelines. Int. J. Telerehabil. 2010, 2, 31–34. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Section and Topic | Item | Checklist Item | Location Where Item Is Reported |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | Page 1 |
| ABSTRACT | |||
| Abstract | 2 | See PRISMA 2020 for abstracts checklist. | Page 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | Page 2 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | Page 2 and 3 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | Page 3 |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | Page 3 and 4 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | Page 3 and 4 |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and details of automation tools used in the process if applicable. | Page 4 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and details of automation tools used in the process if applicable. | Page 4 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points and analyses), and if not the methods used to decide which results to collect should be specified. | Page 4 and 5 |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics and funding sources). Describe any assumptions made about any missing or unclear information. | Page 4 and 5 | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable details of automation tools used in the process. | Page 4 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio and mean difference) used in the synthesis or presentation of results. | NA |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | NA |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics or data conversions. | NA | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | NA | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s) and method(s) that identify the presence and extent of statistical heterogeneity and software package(s) used. | NA | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis and meta-regression). | NA | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | NA | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | NA |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | NA |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | Page 4 and Figure 1 |
| 16b | Cite studies that might appear to meet the inclusion criteria but that were excluded and explain why they were excluded. | Page 5 and Figure 1 | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | Page 5 and 8 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | Page 8 |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) effect estimates and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | Page 8 to 13 |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | Page 8 to 13 |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was conducted, present the summary estimate for each and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | NA | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | NA | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | NA | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | NA |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | NA |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | Page 13 to 15 |
| 23b | Discuss any limitations of the evidence included in the review. | Page 15 | |
| 23c | Discuss any limitations of the review processes used. | Page 15 | |
| 23d | Discuss implications of the results for practice, policy and future research. | Page 16 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number or state that the review was not registered. | NA |
| 24b | Indicate where the review protocol can be accessed or state that a protocol was not prepared. | Na | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | NA | |
| Support | 25 | Describe sources of financial or non-financial support for the review and the role of the funders or sponsors in the review. | Page 16 |
| Competing interests | 26 | Declare any competing interests of review authors. | Page 16 |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; and any other materials used in the review. | NA |
| Study | Year | Country | Study Design | Health Condition | Sample Size | Age (Years) | Gender |
|---|---|---|---|---|---|---|---|
| (Sobierajska-Rek et al., 2021) [30] | 2021 | Poland | Survey | Duchenne muscular dystrophy | 152 | Mean age: 11.00 (SD 7.88) | Boys |
| (Pamela Frigerio, 2021) [31] | 2021 | Italy | Survey | Neurodevelopmental Disabilities | 128 families | 0 to 14 | NR |
| (A. Sobierajska-Rek et al., 2021) [32] | 2021 | Poland | Online survey | Duchenne muscular dystrophy | 69 | 7.38 years; SD 3.06 | boys |
| (Tanner, Grinde and McCormick, 2021) [33] | 2021 | Canada | Cross-sectional study | Different conditions | 86 | 8.13 in group 1, 7.21 in group 2 and 6.24 in group 3 | Girls: 52 Boys: 34 |
| (Bican et al., 2021) [34] | 2021 | USA | Retrospective, observational study | Different conditions such as Musculoskeletal impairment, cerebral palsy, movement disorder, delayed milestones, feeding difficulties and prematurity or low birth weight | 514 | 4.3 ± 3.5 years | NR |
| (Romano, Di Rosa, Tisano, Fabio and Lotan, 2021) [35] | 2021 | Italy | Case series with multiple evaluation meetings | Rett syndrome | 47 goals | 17 ± 7.11 | Girls |
| Krasovsky et al., 2021 [36] | 2021 | Israel | Qualitative survey with Focus groups of experts | All conditions need physical therapy | 15 | 11.31 ± 4.8 years | Both boys and girls |
| (Provenzi et al., 2021) [37] | 2021 | Italy | Cross-sectional survey | Autism spectrum disorders, cerebral palsy, neuromuscular diseases, three with rare genetic or malformative syndromes and extremely premature and psychomotor or cognitive delay conditions. | 36 | 5.8 years (range 1–15) | 25 boys and 11 girls |
| Hall et al. [38] | 2021 | USA | Cross-sectional survey | All conditions need physical therapy in children | 259 | NA since the respondents were physical therapists | Both |
| Gagnon et al. [39] | 2021 | Canada | Single-cohort pilot study | Arthrogryposis multiplex congenital | 114 were approached and 10 consented | 8 to 21 with a mean age of 16.9 years | Both with equal ratio |
| (Assenza et al., 2021) [40] | 2020 | Italy | An observational transversal study | Children with different musculoskeletal and neurodevelopment problems | 138 | 0 to 6 years old for children | NR |
| (K. Tanner et al., 2020) [41] | 2020 | USA | Retrospective chart review and survey | Different conditions required physical, occupational and speech therapy | 767 | NR | NR |
| (Iannizzotto, Nucita, Fabio, Caprì and Lo Bello, 2020) [42] | 2021 | Italy | Experiment | Rett genetic syndrome | 300 | 11.31 ± 4.8 years | girls |
| Study | Year | Country | Type of Intervention | Key Findings |
|---|---|---|---|---|
| (Sobierajska-Rek et al., 2021) [30] | 2021 | Poland | Respiratory physical therapy telerehabilitationVideo with the instructions of respiratory exercises | The average rating for the satisfaction with the therapy was 4.7 out of 5, and it was 4.78 out of 5 for intelligibility. Around 83% of the study participants reported performing the exercises and their caregivers mentioned that it was feasible for their children to perform the recommended exercises a few times a week or daily. |
| (Pamela Frigerio, 2021) [31] | 2021 | Italy | Remote therapy | Almost 80.5% of the caregivers showed their satisfaction with telerehabilitation. More than 50% of the families mentioned a higher degree of satisfaction with telerehabilitation. |
| (A. Sobierajska-Rek et al., 2021) [32] | 2021 | Poland | The rehabilitation programs | Using physiotherapy can continue home-based rehabilitation. Parents or caregivers accepted instructions or videos given remotely to a greater extent. |
| (Tanner, Grinde and McCormick, 2021) [33] | 2021 | Canada | The Canadian Occupational Performance Measure | Canadian Occupational Performance Measure (COPM) is considered a feasible measure as perceived positively by professional pediatric therapists. Around 83% of the therapists agreed or strongly agreed that COPM is easy to use and is reasonable in a given period of time and can be used with children of different conditions. |
| (Bican et al., 2021) [34] | 2021 | USA | Physical or occupational therapy with 938 video visits and 150 telephone encounters. | Telerehabilitation services were received by 83.4% of the children, and most occupational and physical therapists (69.1%) agreed that telerehabilitation is as effective as in-person care. Around 93% of the therapists reported that caregivers were available during the sessions and were actively participating. |
| (Romano, Di Rosa, Tisano, Fabio and Lotan, 2021) [35] | 2021 | Italy | Rehabilitation program with 47 goals with a customized program for each participant | Out of the total 47 rehabilitative goals set, 78.7% were achieved with around 76.9% of the children’s gross motor function improving with a modest effect (0.604). Parents and caregivers rated the telerehabilitation program satisfactorily with a score of 4.4/5 and general satisfaction was 4.5/5 with adherence to the program being 4.4/5. |
| Krasovsky et al., 2021 [36] | 2021 | Israel | Telerehabilitation sessions | Three components including child, parent and sessions were found to explain 71.3% of the variance in the Clinician Evaluation of Telerehabilitation Service. Therapists mentioned that their capability to maintain therapeutic alliance was superior in that they were able to achieve other goals. According to the families, the therapist was highly involved in providing therapy to children regardless of the type of treatment. These results are in the favor of transitioning to telerehabilitation for the pediatric population. |
| (Provenzi et al., 2021) [37] | 2021 | Italy | Online Rehabilitation of Children during the Epidemic (EnFORCE) telehealth program that included case-specific tailored telehealth sessions that include parental support and child rehabilitation sessions. | The findings showed that > 80% of the parents mentioned that their children benefited from the program during the lockdown. Parents from 86 to 95% reported increased feelings of engagement, perceived support and self-relevance. |
| Hall et al. [38] | 2021 | USA | Telehealth | The study found that a higher degree of engagement and access to telehealth with stable technology is considered a crucial factor for the effectiveness of telehealth. This model of telehealth is supported and correlates to factors such as internet availability and good connection, and the interaction between child and caregiver and resilience of family may play a vital role in moving towards telerehabilitation during the COVID-19 crisis. |
| Gagnon et al. [39] | 2021 | Canada | Physiotec (Physiotec Québec Inc.), a software program that can create a home exercise program | The study found that participants performed home exercise program almost twice a week (Mean: 2.04 with 95% CI of 1.25 to 4.08), and they were satisfied with the approach. Out of 15 goals that were set at the beginning of the program, 12 goals were achieved. The study found a statistically significant improvements in pain and comfort for pediatric outcomes (p-value: 0.048) on the physical activity questionnaire. |
| (Assenza et al., 2021) [40] | 2020 | Italy | Physical, speech, occupational and cognitive-behavioral therapy using telerehabilitation | The findings revealed a correlation among caretakers of children aged 0–3 with feeling overwhelmed with distance care (OR = 3.27), low perception of telerehabilitation for improving objectives (OR = 6.51) and a great perception of feeling supported in establishing regular activity (OR = 2.96). It was concluded that telerehabilitation can be a helpful strategy during a global pandemic. |
| (K. Tanner et al., 2020) [41] | 2020 | USA | Telerehabilitation services (speech-language pathology, developmental occupational and physical therapies and sports and orthopedic therapies) | There was a high satisfaction found with 98.97% of the positive responses. Seventy-three point five percent of pre-pandemic patients were returned after implementing telerehabilitation services. |
| (Iannizzotto, Nucita, Fabio, Caprì and Lo Bello, 2020) [42] | 2021 | Italy | Eye gaze technology with a videoconferencing software | The preliminary results of the study revealed that videoconferencing software is promising and can be used at a larger base cost effectively without relying on expensive and complicated devices in which children can remotely communicate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonazi, A. Effectiveness and Acceptability of Telerehabilitation in Physical Therapy during COVID-19 in Children: Findings of a Systematic Review. Children 2021, 8, 1101. https://doi.org/10.3390/children8121101
Alonazi A. Effectiveness and Acceptability of Telerehabilitation in Physical Therapy during COVID-19 in Children: Findings of a Systematic Review. Children. 2021; 8(12):1101. https://doi.org/10.3390/children8121101
Chicago/Turabian StyleAlonazi, Asma. 2021. "Effectiveness and Acceptability of Telerehabilitation in Physical Therapy during COVID-19 in Children: Findings of a Systematic Review" Children 8, no. 12: 1101. https://doi.org/10.3390/children8121101
APA StyleAlonazi, A. (2021). Effectiveness and Acceptability of Telerehabilitation in Physical Therapy during COVID-19 in Children: Findings of a Systematic Review. Children, 8(12), 1101. https://doi.org/10.3390/children8121101