
Paediatric Multiple Sclerosis: A Scoping Review of Patients’ and Parents’ Perspectives


Abstract
:1. Introduction
1.1. Paediatric-Onset MS
1.2. Diagnosis of MS
1.3. Burden of Paediatric MS
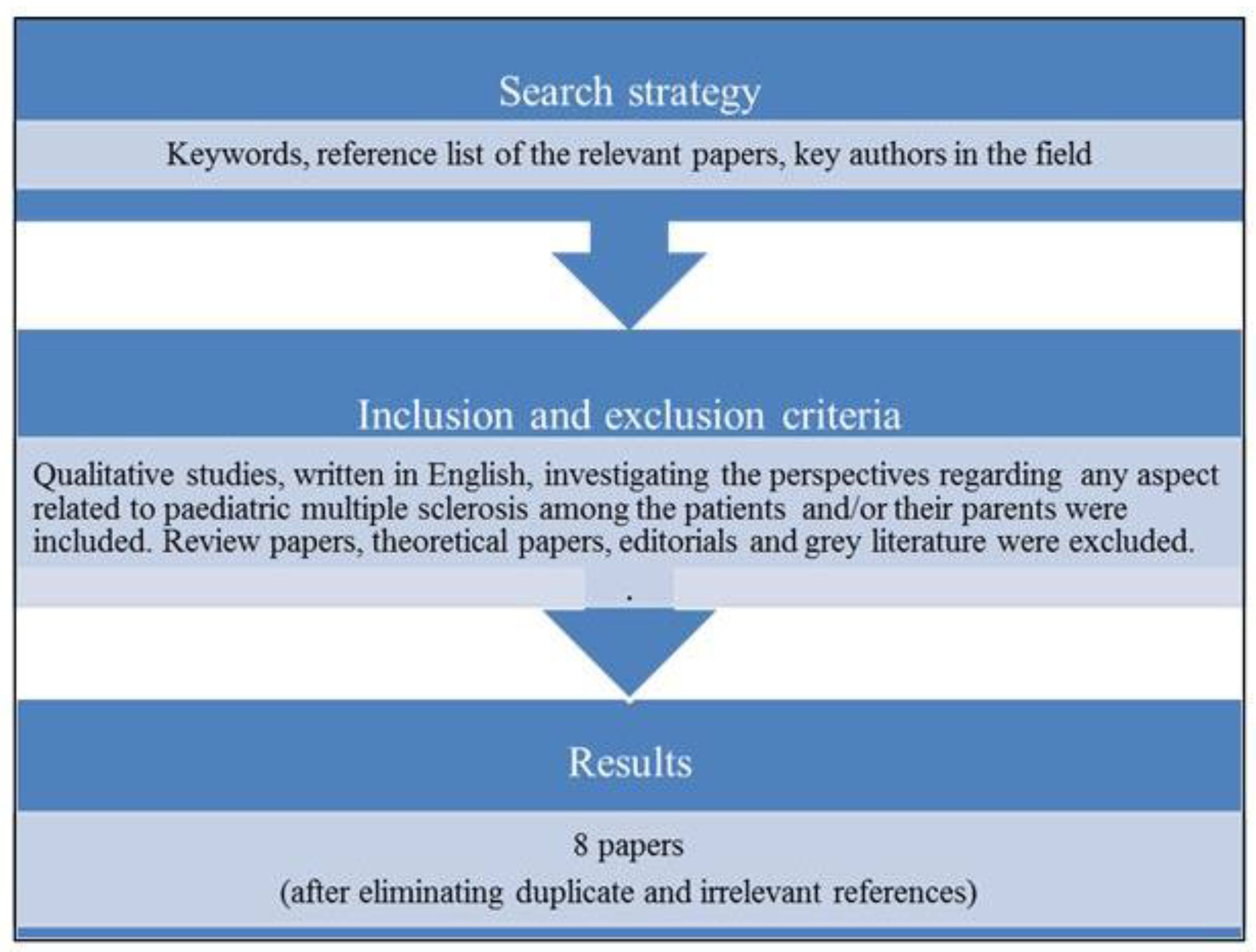
2. Materials and Methods
| “paediatric” OR “pediatric” OR “child” OR “children” OR “childhood” OR “juvenile” OR “youth” OR “youngster*” |
| “multiple sclerosis” OR “MS” OR “demyelinating disorder” OR “relapsing-remitting” |
| “perspective*” OR “perception*” OR “opinion*” OR “experience*” OR “attitude*” OR “impression*” OR “lived experience” |
| “caregiver*” OR “parent*” OR “mother*” OR “father*” OR “family” |
2.1. Selection of the Papers
2.2. Relevance
2.3. Data Extraction
3. Results
3.1. Onset of Symptoms
3.2. Diagnostic Process
3.3. Reaction to the Diagnosis
3.4. Management and Acceptance of MS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- McFarland, H.F.; Martin, R. Multiple sclerosis: A complicated picture of autoimmunity. Nat. Immunol. 2007, 8, 913–919. [Google Scholar] [CrossRef]
- Wootla, B.; Eriguchi, M.; Rodriguez, M. Is multiple sclerosis an autoimmune disease? Autoimmune Dis. 2012, 2012, 969657. [Google Scholar] [CrossRef]
- Feinstein, A. The neuropsychiatry of multiple sclerosis. Can J. Psychiatry 2004, 49, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Induruwa, I.; Constantinescu, C.S.; Gran, B. Fatigue in multiple sclerosis—A brief review. J. Neurol. Sci. 2012, 323, 9–15. [Google Scholar] [CrossRef]
- Vasconcelos, C.C.F.; Thuler, L.C.S.; Rodrigues, B.C.; Calmon, A.B.; Alvarenga, R.M.P. Multiple sclerosis in Brazil: A systematic review. Clin. Neurol. Neurosurg. 2016, 151, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Giordano, A.; Granella, F.; Lugaresi, A.; Martinelli, V.; Trojano, M.; Confalonieri, P.; Radice, D.; Solari, A.; SIMS-Trial Group. Anxiety and depression in multiple sclerosis patients around diagnosis. J. Neurol. Sci. 2011, 307, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Kroencke, D.C.; Denney, D.R.; Lynch, S.G. Depression during exacerbations in multiple sclerosis: The importance of uncertainty. Mult Scler J. 2001, 7, 237–242. [Google Scholar] [CrossRef] [Green Version]
- Krysko, K.M.; Graves, J.S.; Rensel, M.; Weinstock-Guttman, B.; Rutatangwa, A.; GAaen, R.; Belman, A.; Benson, L.; Chitnis, T.; Gorman, M.; et al. Real-world effectiveness of initial disease-modifying therapies in pediatric multiple sclerosis. Ann. Neurol. 2020, 88, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Langer-Gould, A.; Moses, H.H.; Murray, T.J. Strategies for managing the side effects of treatments for multiple sclerosis. Neurology 2004, 63, S35–S41. [Google Scholar] [CrossRef]
- Klauer, T.; Zettl, U.K. Compliance, adherence, and the treatment of multiple sclerosis. J. Neurol. 2008, 255, 87–92. [Google Scholar] [CrossRef]
- Halper, J. The psychosocial effect of multiple sclerosis: The impact of relapses. J. Neurol. Sci. 2007, 256, S34–S38. [Google Scholar] [CrossRef] [PubMed]
- Kouzoupis, A.B.; Paparrigopoulos, T.; Soldatos, M.; Papadimitriou, G.N. The family of the multiple sclerosis patient: A psychosocial perspective. Int. Rev. Psychiatry 2010, 22, 83–89. [Google Scholar] [CrossRef]
- MacAllister, W.S.; Boyd, J.R.; Holland, N.J.; Milazzo, M.C.; Krupp, L.B. The psychosocial consequences of pediatric multiple sclerosis. Neurology 2007, 68, S66–S69. [Google Scholar] [CrossRef]
- Luca, M.; Chisari, C.G.; D’Amico, E.; Patti, F. Hopelessness in multiple sclerosis: Psychological and organic correlates. J. Psychiatry Psychiatr. Disord. 2019, 3, 241–244. [Google Scholar] [CrossRef]
- Walton, C.; King, R.; Rechtman, L.; Marrie, R.A.; Robertson, N.; la Rocca, N.; Uitdehaag, B.; van der Mei, I.; Wallin, M.; Helme, A.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS. Mult. Scler. J. 2020, 26, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- Chou, I.J.; Wang, H.S.; Whitehouse, W.P.; Constantinescu, C.S. Paediatric multiple sclerosis: Update on diagnostic criteria, imaging, histopathology and treatment choices. Curr. Neurol. Neurosci. Rep. 2016, 16, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alroughani, R.; Boyko, A. Pediatric multiple sclerosis: A review. BMC Neurol. 2018, 18, 1–8. [Google Scholar] [CrossRef]
- Ghezzi, A.; Baroncini, D.; Zaffaroni, M.; Comi, G. Pediatric versus adult MS: Similar or different? Mult. Scler. Demyelinating Disord. 2017, 2, 5. [Google Scholar] [CrossRef] [Green Version]
- Hinton, D.; Kirk, S. Paediatric multiple sclerosis: A qualitative study of families’ diagnosis experiences. Arch. Dis. Child 2015, 100, 623–629. [Google Scholar] [CrossRef]
- Cross, T.P.; Shanks, A.K.; Duffy, L.V.; Rintell, D.J. Families’ experience of pediatric onset multiple sclerosis. J. Child Adolesc. Trauma 2019, 12, 425–435. [Google Scholar] [CrossRef]
- Hinton, D.; Kirk, S. Living with uncertainty and hope: A qualitative study exploring parents’ experiences of living with childhood multiple sclerosis. Chronic Illn. 2017, 13, 88–99. [Google Scholar] [CrossRef] [PubMed]
- Gorman, M.P.; Healy, B.C.; Polgar-Turcsanyi, M.; Chitnis, T. Increased relapse rate in pediatric-onset compared with adult-onset multiple sclerosis. Arch. Neurol. 2009, 66, 54–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chisari, C.G.; Toro, M.D.; Cimino, V.; Rejdak, R.; Luca, M.; Rapisarda, L.; Avitabile, T.; Posarelli, C.; Rejdak, K.; Reibaldi, M.; et al. Retinal nerve fiber layer thickness and higher relapse frequency may predict poor recovery after optic neuritis in MS patients. J. Clin. Med. 2019, 8, 2022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasemi, M.; Gorji, Y.; Ashtar, F.; Ghasemi, M. A study of psychological well-being in people with multiple sclerosis and their primary caregivers. Adv. Biomed. Res. 2015, 4, 49. [Google Scholar] [CrossRef] [PubMed]
- Mickens, M.; Perrin, P.B.; Aguayo, A.; Macias, M.A.; Arango-Lasprilla, J.C. Comparing health-related quality of life and psychological well-being between Mexican MS caregivers and controls. J. Lat. Psychol. 2013, 1, 195. [Google Scholar] [CrossRef]
- Patti, F.; Amato, M.P.; Battaglia, M.A.; Pitaro, M.; Russo, P.; Solaro, C.; Trojano, M. Caregiver quality of life in multiple sclerosis: A multicentre Italian study. Mult. Scler. J. 2007, 13, 412–419. [Google Scholar] [CrossRef]
- Bassi, M.; Cilia, S.; Falautano, M.; Grobberio, M.; Negri, L.; Niccolai, C.; Pattini, M.; Pietrolongo, E.; Quartuccio, M.E.; Viterbo, R.G.; et al. The caring experience in multiple sclerosis: Caregiving tasks, coping strategies and psychological well-being. Health Soc. Care Community 2020, 28, 236–246. [Google Scholar] [CrossRef]
- Delle Fave, A.; Bassi, M.; Allegri, B.; Sabina, C.; Monica, F.; Benedetta, G.; Monica, G.; Eleonora, M.; Marianna, P.; Erika, P.; et al. Beyond disease: Happiness, goals, and meanings among persons with multiple sclerosis and their caregivers. Front. Psychol. 2017, 8, 2216. [Google Scholar] [CrossRef] [Green Version]
- Maguire, R.; Maguire, P. Caregiver burden in multiple sclerosis: Recent trends and future directions. Curr. Neurol. Neurosci. Rep. 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Thannhauser, J.E. Grief—Peer dynamics: Understanding experiences with pediatric multiple sclerosis. Qual. Health Res. 2009, 19, 766–777. [Google Scholar] [CrossRef]
- McCubbin, H.I.; Patterson, J.M. The family stress process: The double ABCX model of adjustment and adaptation. Marriage Fam. Rev. 1983, 6, 7–37. [Google Scholar] [CrossRef]
- The Joanna Briggs Institute Manual for Evidence Synthesis. Available online: https://synthesismanual.jbi.global (accessed on 15 May 2021).
- Hebert, D.; Geisthardt, C.; Hoffman, H. Insights and recommendations from parents receiving a diagnosis of pediatric multiple sclerosis for their child. J. Child Neurol. 2019, 34, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Thannhauser, J.E. Navigating life and loss in pediatric multiple sclerosis. Qual. Health Res. 2014, 24, 1198–1211. [Google Scholar] [CrossRef] [PubMed]
- Carroll, S.; Chalder, T.; Hemingway, C.; Heyman, I.; Moss-Morris, R. “It feels like wearing a giant sandbag.” Adolescent and parent perceptions of fatigue in paediatric multiple sclerosis. Eur. J. Paediatr. Neurol. 2016, 20, 938–945. [Google Scholar] [CrossRef] [Green Version]
- Boyd, J.R.; MacMillan, L.J. Experiences of children and adolescents living with multiple sclerosis. J. Neurosci. Nurs. 2005, 37, 334–342. [Google Scholar] [CrossRef]
- Bryman, A. Social Research Methods, 5th ed.; Oxford University Press: Oxford, UK, 2016; pp. 400–402. [Google Scholar]
- Eyckmans, L.; Hilderson, D.; Westhovens, R.; Wouters, C.; Moons, P. What does it mean to grow up with juvenile idiopathic arthritis? A qualitative study on the perspectives of patients. Clin. Rheumatol. 2011, 30, 459–465. [Google Scholar] [CrossRef]
- Gómez-Ramírez, O.; Gibbon, M.; Berard, R.; Jurencak, R.; Green, J.; Tucker, L.; Shiff, N.; Guzman, J. A recurring rollercoaster ride: A qualitative study of the emotional experiences of parents of children with juvenile idiopathic arthritis. Pediatr. Rheumatol. 2016, 14, 13. [Google Scholar] [CrossRef] [Green Version]
- Aldridge, M.D. How do families adjust to having a child with chronic kidney failure? A systematic review. Nephrol. Nurs. J. 2008, 35, 157–162. [Google Scholar] [PubMed]
- Rasmussen, G.S.; Kragballe, K.; Maindal, H.T.; Lomborg, K. Experience of being young with psoriasis: Self-management support needs. Qual. Health Res. 2018, 28, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Anderson, A.K.; Wais, P.E.; Gabrieli, J.D. Emotion enhances remembrance of neutral events past. Proc. Natl. Acad. Sci. USA 2006, 103, 1599–1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etemadifar, M.; Sedaghat, N.; Aghababaee, A.; Kargaran, P.K.; Maracy, M.R.; Ganjalikhani-Hakemi, M.; Rayani, M.; Abhari, A.P.; Khorvash, R.; Salari, M.; et al. COVID-19 and the Risk of Relapse in Multiple Sclerosis Patients: A Fight with No Bystander Effect? Mult. Scler. Relat. Disord. 2021, 51, 102915. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Papers (Titles Abbreviated) | Methodology | Methods | Phenomenon of Interest | Recruitment | Participants | Country | Data Analysis |
|---|---|---|---|---|---|---|---|
| Families’ experience of pediatric onset multiple sclerosis. Cross et al., 2019 | Thematic analysis | In person interview | (1) Stresses of parenting a child with MS (2) Stress management | 2 MS centres for children | 19 parents 2 couples | USA | Identification of themes |
| Insights and recommendations from parents receiving a diagnosis. Hebert et al., 2019 | Thematic analysis | Phone interview | Receiving the diagnosis | National MS Society | 42 parents | USA | Identification of themes |
| Living with uncertainty and hope: a qualitative study exploring parents’ experiences. Hinton et al., 2017 | Grounded theory | In person interview | Experiences of parents dealing with paediatric MS | 16 MS centres 4 voluntary organisations | 31 parents | UK | Coding and generation of categories using NVivo software |
| “It feels like wearing a giant sandbag”. Adolescent and parent perceptions of fatigue. Carroll et al., 2016 | Elements of grounded theory | In person /Phone interview | (1) Experiences of fatigue in patients and parents (2) Management of fatigue | NHS paediatric neurology clinics MS charities Support fora | 15 patients 13 parents Age: 6–18, reporting fatigue | UK | Coding Development of themes and sub-themes |
| Paediatric multiple sclerosis: a qualitative study of families’ diagnosis experiences. Hinton et al., 2015 | Elements of grounded theory | In person interview | (1) Diagnostic process (2) Families’ support needs (3) Barriers/facilitators to early diagnosis | 16 NHS Trusts 4 voluntary organisations | 31 parents 21 patients Age: 8–17 | UK | Identification and comparison of codes using NVivo software |
| Navigating life and loss in pediatric multiple sclerosis. Thannhauser, 2014 | Charmaz’s constructivist grounded theory | (1) In person interview (2) Blog | Adjustment to paediatric MS | 3 MS centres | 7 patients 6 parents Age: 16–21 | Canada | Coding and generation of categories consider that reality is socially constructed |
| Grief-peer dynamics: understanding experiences with pediatric multiple sclerosis. Thannhauser, 2009 | Grounded Theory | (1) In person interview (2) Focus group | (1) Experience of adolescents with MS (2) Peer relationships within this experience | 1 MS centre | 6 patients 6 parents Age: 14–21 | Canada | Coding Generating of categories Finding relationships within the data Theorizing |
| Experiences of children and adolescents living with multiple sclerosis. Boyd et al., 2005 | Phenomenology | In person interview | Experiences of children and adolescents living with MS | 1 MS centre | 12 patients Age: 8–18 | Canada | Narrative analysis. Themes were compared and integrated using NVivo software |
| Papers (Titles Abbreviated) | Focus | Identified Areas of Interest |
|---|---|---|
| Families’ experience of pediatric onset multiple sclerosis. Cross et al., 2019 | (1) Stresses of parenting a child with MS (2) Stress management | Experience prior to the diagnosis: shock and fear for the sudden symptoms; shame and guilt for dismissing the early signs Receiving the diagnosis: praise for physicians clarifying that prognosis is not necessarily dreadful and there are new therapies for paediatric MS Reaction to the diagnosis (parents): shock and fear Children’s reaction (parents’ account): from severe distress to apparent carelessness
Treatment:
Impact at school:
|
| Insights and recommendations from parents receiving a diagnosis. Hebert et al., 2019 | Receiving the diagnosis | Initial symptoms and diagnostic process:
Recommendations from parents to medical professionals:
|
| Papers (Titles Abbreviated) | Focus | Identified Areas of Interest |
|---|---|---|
| Living with uncertainty and hope: a qualitative study exploring parents’ experiences. Hinton et al., 2017 | Experiences of parents dealing with paediatric MS | Diagnostic uncertainty:
|
| “It feels like wearing a giant sandbag”. Adolescent and parent perceptions of fatigue. Carroll et al., 2016 | (1) Experiences of fatigue in patients and parents (2) Management of fatigue | (1) Lived experience and impact of fatigue
|
| Papers | Focus | Identified Areas of Interest |
|---|---|---|
| Paediatric multiple sclerosis: a qualitative study of families’ diagnosis experiences. Hinton et al., 2015 | (1) Diagnostic process (2) Families’ support needs (3) Barriers/facilitators to early diagnosis | Symptoms: gradual onset of a-specific symptoms, that come and go Recognising a problem: “wait and see approach” Seeking medical advice: general practitioner first Communicating concerns to medical professionals: from being heard to being blamed of imagining symptoms, overreacting to/causing them Medical interpretation of the symptoms: In primary care, symptoms frequently dismissed as signs of viruses or psychological problems. In secondary care, paediatricians seemed to be unprepared to interpret MRI findings. Questioning medical opinion:
|
| Navigating life and loss in pediatric multiple sclerosis. Thannhauser, 2014 | Adjustment to paediatric MS | Recurring loss in the patients (1) suffering: shock, confusion, sadness (2) fearing the unknown (loss of future) (3) losing trust (professionals’ uncertainty, being blamed of faking the symptoms) (4) sense making (reconstruction of the believes about themselves and reality) Denial as a defence mechanism. Carrying on in the patients (1) becoming me: knowing more about yourself (2) putting MS in its place: MS dose not define the self (3) pushing boundaries: risk-taking behaviours aimed at reducing the limitations imposed by MS (4) finding normal: maintaining normalcy and reinventing normal (re-conceptualization of independence) (5) becoming an expert: controlling symptoms through lifestyle; making medical decisions by themselves; information seeking (severe cases increase suffering); advocating for self (setting boundaries with others); planning for the future (e.g., intellectual career) Selectively disclosing:
integrating MS in one’s own life through perspective taking, reprioritizing, finding purpose, remaining hopeful TURNING POINTS The following aspects strongly influence the experiences of loss and the ability to carry on: (1) labelling the disease; (2) develop emotional awareness; (3) managing medication; (4) dynamic relationships (support from others help to carry on; losing experiences and friends, being teased and rejected contribute to grief) |
| Papers | Focus | Identified Areas of Interest |
|---|---|---|
| Grief-peer dynamics: understanding experiences with pediatric multiple sclerosis. Thannhauser, 2009 | (1)Experience of adolescents with MS (2)Peer relationships within this experience | Grief experience Mood swings; shifts between grief and acceptance Major loss: physical health Secondary losses: identity shift; loss of control due to unpredictable symptoms; loss of friends; loss of hope for the future; loss of normality (medication, diet…); loss of assumptions about the world (the world does not make sense after all) Manifestations of grief: denial, anger, anxiety, sadness… Manifestations of acceptance: face the challenge, learn to prioritize, maintain a positive perspective, be more compassionate Relationship dynamics Peer relationships influenced psychological well-being Medication–peer-tug-of-war: negative reactions to the injections favoured the loss experience, positive reaction prompted acceptance Shifting friendships: losing friends, deepening old relationships, make new friends Finding supportive relationships: rely to a small group of positive and supportive friends Dealing with others’ worry: overprotection favours grief Talking about MS: despite cautiousness, disclosing the disease favours acceptance Acting normal: hide the diagnosis to maintain normalcy and avoid rejection |
| Experiences of children and adolescents living with multiple sclerosis. Boyd et al., 2005 | Experiences of children and adolescents living with MS | Learning the diagnosis: fear, sadness, relief. Concerns about possible death Noticing the differences: symptoms and medication limiting everyday life Staying the same: the interviewed patients described a rather normal life, despite the difficulties, and did not feel changed by MS Coping with MS: stressors: intermittent symptoms, medication, being treated differently, missing school, parental worry, potential disability strategies: stay positive, identify role models with MS or other conditions, remain busy Unhealthy strategies can include denial, manipulation, unhealthy habits, etc. Gaining support: all patients refer to someone as really supportive Dealing with treatment: injection discomfort, bruises, side effects Changing relationships: feeling closer to the family; hide symptoms to prevent patients’ worry; received favouritism; manipulate; test friendships through diagnosis disclosure Peer response: usually positive, some experiences of exclusion from activities Disclosing the diagnosis: be selective Effect learning: learning problems, absenteeism Looking toward the future: move forward and be hopeful Advice to peers with MS: remain positive. Take care of yourself; medication is needed; seek support from others |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luca, M.; Ortega-Castro, N.; Patti, F. Paediatric Multiple Sclerosis: A Scoping Review of Patients’ and Parents’ Perspectives. Children 2022, 9, 11. https://doi.org/10.3390/children9010011
Luca M, Ortega-Castro N, Patti F. Paediatric Multiple Sclerosis: A Scoping Review of Patients’ and Parents’ Perspectives. Children. 2022; 9(1):11. https://doi.org/10.3390/children9010011
Chicago/Turabian StyleLuca, Maria, Nerea Ortega-Castro, and Francesco Patti. 2022. "Paediatric Multiple Sclerosis: A Scoping Review of Patients’ and Parents’ Perspectives" Children 9, no. 1: 11. https://doi.org/10.3390/children9010011
APA StyleLuca, M., Ortega-Castro, N., & Patti, F. (2022). Paediatric Multiple Sclerosis: A Scoping Review of Patients’ and Parents’ Perspectives. Children, 9(1), 11. https://doi.org/10.3390/children9010011