
Vaccination Coverage during Childhood and Adolescence among Undergraduate Health Science Students in Greece

 ,
, 

Abstract
:1. Introduction
2. Methods
3. Statistical Analysis
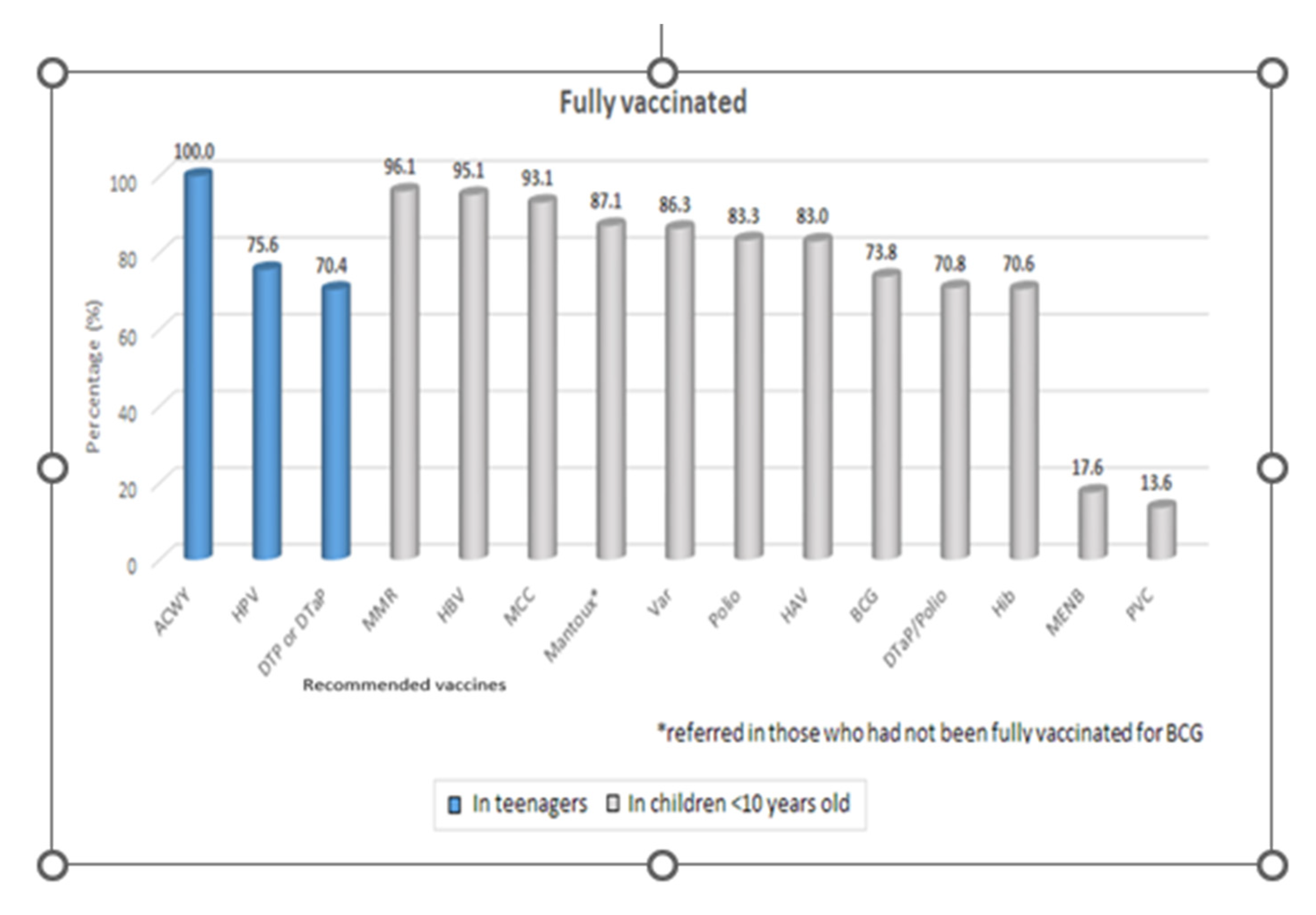
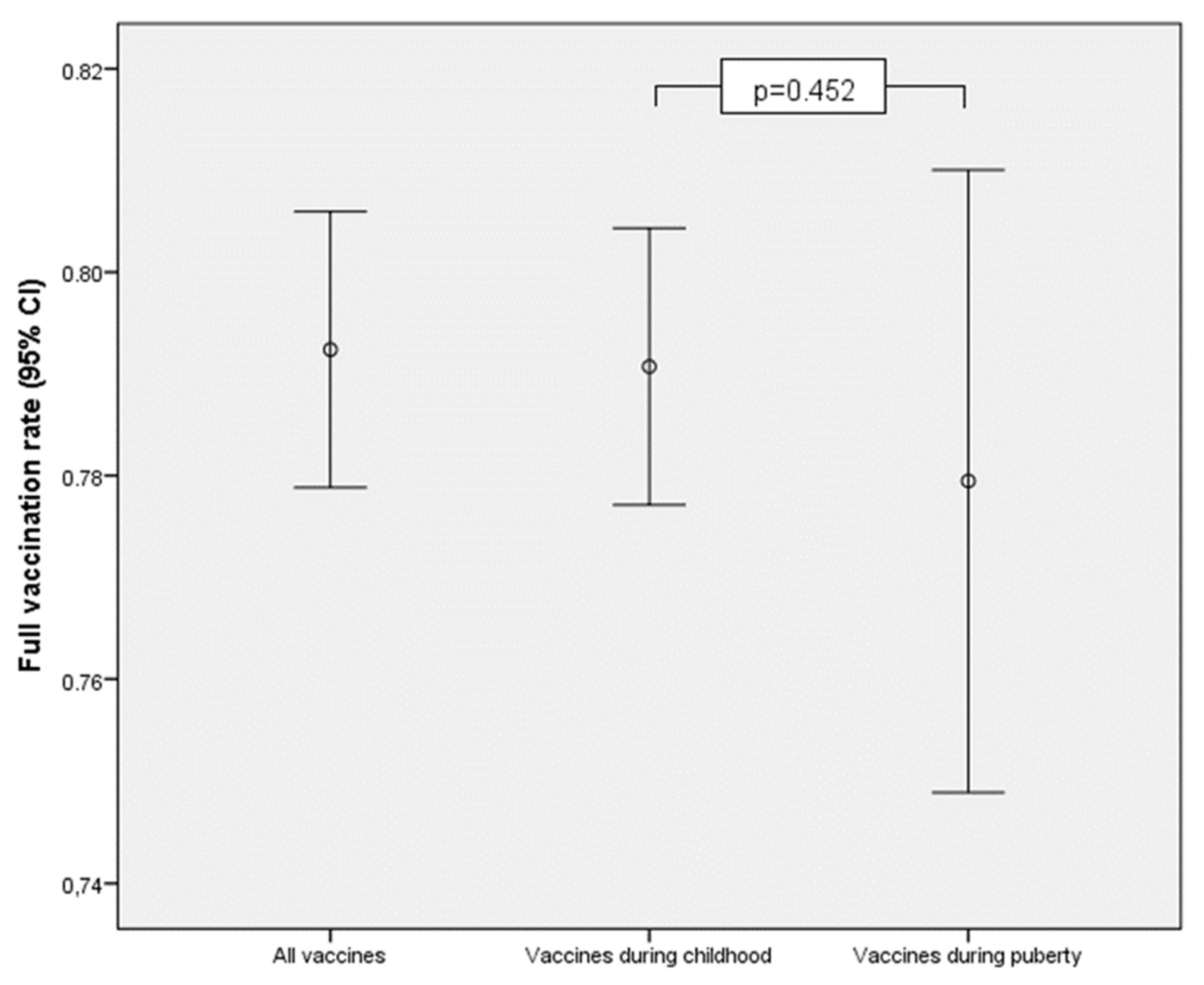
4. Results
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNICEF. Levels & Trends in Child Mortality: Report 2019-Estimates Developed by the UN Inter-Agency Group for Child Mortality Estimation; UNICEF: New York, NY, USA, 2019. [Google Scholar]
- WHO. Immunization Coverage; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Vaccine preventable deaths and the Global Immunization Vision and Strategy, 2006–2015 Centers for Disease Control and Prevention (CDC). MMWR Morb. Mortal Wkly. Rep. 2006, 55, 511–515.
- Brown, N.J.; Platt, M.P.; Beattie, R.M. Women, children, and global public health: Beyond the millennium development goals. BMJ 2015, 350, h1755. [Google Scholar] [CrossRef]
- World Health Organization. Global Vaccine Action Plan 2011–2020; WHO Press: Geneva, Switzerland, 2013; pp. 1–7. Available online: https://www.who.int/immunization/global_vaccine_action_plan/GVAP_doc_2011_2020/en/ (accessed on 17 April 2022).
- Peck, M.; Gacic-Dobo, M.; Diallo, M.S.; Nedelec, Y.; Sodha, S.S.; Wallace, A.S. Global Routine Vaccination Coverage, 2018. MMWR. Morb. Mortal. Wkly. Rep. 2019, 68, 937–942. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. WHO and UNICEF: Updates on immunization coverage and how can we improve upon? J Res Medi Sci. 2015, 20, 1216–1217. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Immunization Coverage; WHO Press: Geneva, Switzerland, 2015; Available online: http://who.int/immunization/monitoring_surveillance/routine/coverage/en/ (accessed on 17 April 2022).
- ECDC. Vaccine-Preventable Diseases Programme. Available online: https://www.ecdc.europa.eu/en/about-uswho-we-aredisease-programmes/vaccine-preventable-diseases-programme (accessed on 17 April 2022).
- Vanderslott, S.; Marks, T. Charting mandatory childhood vaccination policies worldwide. Vaccine 2021, 39, 4054–4062. [Google Scholar] [CrossRef]
- Larson, H.J. The state of vaccine confidence. Lancet 2018, 392, 2244–2246. [Google Scholar] [CrossRef]
- Holzmann, H.; Wiedermann, U. Mandatory vaccination: Suited to enhance vaccination coverage in Europe? Eurosurveillance 2019, 24, 1900376. [Google Scholar] [CrossRef] [Green Version]
- Søegaard, S.H.; Rostgaard, K.; Schmiegelow, K.; Kamper-Jørgensen, M.; Hargreave, M.; Hjalgrim, H.; Hviid, A. Childhood vaccinations and risk of acute lymphoblastic leukaemia in children. Int. J. Epidemiology 2017, 46, 905–913. [Google Scholar] [CrossRef] [Green Version]
- Agopian, A.; Young, H.; Quinlan, S.; Rice, M.M. Timeliness of childhood vaccinations in Armenia, 2015–2016. Vaccine 2020, 19, 4671–4678. [Google Scholar] [CrossRef] [PubMed]
- Nicola Princip, N.; Susanna Esposito, N. Adolescents and vaccines in the western world. Vaccine 2013, 31, 5366–5374. [Google Scholar] [CrossRef]
- CDC. Vaccination Requirements. 2011. Available online: http://www2a.cdc.gov/nip/schoolsurv/schImmRqmt.asp (accessed on 17 April 2022).
- May, T.; Silverman, R.D. Clustering of exemptions as a collective action threat to herd immunity. Vaccine 2003, 21, 1048–1051. [Google Scholar] [CrossRef]
- Noula, M.; Raftopoulos, V.; Gesouli, E.; Tsaprounis, T.; Deltsidou, A. Greek nursing students’ immunization coverage: Data from central continental Greece. Nurs. Health Sci. 2008, 10, 169–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunze, U.; Schweinzer, H. Self-reported vaccination status and attitudes towards mandatory vaccinations for health care workers among medical students. Vaccine 2020, 38, 5695–5699. [Google Scholar] [CrossRef] [PubMed]
- Petersen, S.; Roggendorf, H.; Wicker, S. Vaccine Preventable Diseases: Knowledge, Attitudes and Vaccination Status of Medical Students. Gesundheitswesen 2017, 79, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Baer, G.; Bonhoeffer, J.; Schaad, U.B.; Heininger, U. Seroprevalence and immunization history of selected vaccine preventable diseases in medical students. Vaccine 2005, 23, 2016–2020. [Google Scholar] [CrossRef] [PubMed]
- Loulergue, P.; Fonteneau, L.; Armengaud, J.B.; Momcilovic, S.; Levy-Brühl, D.; Launay, O.; Guthmann, J.P. Studyvax survey group. Vaccine coverage of healthcare students in hospitals of the Paris region in 2009: The Studyvax survey. Vaccine 2013, 31, 2835–2838. [Google Scholar] [CrossRef]
- Wicker, S.; Rabenau, H.F.; von Gierke, L.; François, G.; Hambach, R.; De Schryver, A. Hepatitis B and influenza vaccines: Important occupational vaccines differently perceived among medical students. Vaccine 2013, 31, 5111–5117. [Google Scholar] [CrossRef]
- Faure, E.; Cortot, C.; Gosset, D.; Cordonnier, A.; Deruelle, P.; Guery, B. Vaccinal status of healthcare students in Lille. Med. Mal. Infect. 2013, 43, 114–117. [Google Scholar] [CrossRef]
- Karageorgou, K.; Katerelos, P.; Efstathiou, A.; Theodoridou, M.; Maltezou, H.C. Vaccination coverage and susceptibility against vaccine-preventable diseases of healthcare students in Athens, Greece. Vaccine 2014, 32, 5083–5086. [Google Scholar] [CrossRef]
- Papagiannis, D.; Tsimtsiou, Z.; Chatzichristodoulou, I.; Adamopoulou, M.; Kallistratos, I.; Pournaras, S.; Arvanitidou, M.; Rachiotis, G. Hepatitis B Virus Vaccination Coverage in Medical, Nursing, and Paramedical Students: A Cross-Sectional, Multi-Centered Study in Greece. Int. J. Environ. Res. Public Health 2016, 13, 323. [Google Scholar] [CrossRef] [Green Version]
- Maltezou, H.C.; Rahiotis, C.; Tseroni, M.; Madianos, P.; Tzoutzas, I. Attitudes toward Vaccinations and Vaccination Coverage Rates among Dental Students in Greece. Int. J. Environ. Res. Public Health 2022, 19, 2879. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Karantoni, H.; Petrikkos, P.; Georgota, P.; Katerelos, P.; Liona, A.; Tsagarakis, S.; Theodoridou, M.; Hatzigeorgiou, D. Vaccination coverage and immunity levels against vaccine-preventable diseases in male Air Force recruits in Greece. Vaccine 2019, 38, 1181–1185. [Google Scholar] [CrossRef] [PubMed]
- Therre, H.; Baron, S. Contributors Pertussis immunisation in Europe—The situation in late 1999. Eurosurveillance 2000, 5, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.; Trindade, E.; Skowronski, D. Epidemiology of pertussis. Pediatr. Infect. Dis. J. 2005, 24, S10–S18. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Lionis, C. The financial crisis and the expected effects on vaccinations in Europe: A literature review. Infect. Dis. 2015, 47, 437–446. [Google Scholar] [CrossRef]
- Donadiki, E.M.; Jiménez-García, R.; Hernández-Barrera, V.; Carrasco-Garrido, P.; López de Andrés, A.; Velonakis, E.G. Hu-man papillomavirus vaccination coverage among Greek higher education female students and predictors of vaccine uptake. Vaccine 2012, 30, 6967–6970. [Google Scholar] [CrossRef]
- Michail, G.; Smaili, M.; Vozikis, A.; Jelastopulu, E.; Adonakis, G.; Poulas, K. Female students receiving post-secondary education in Greece: The results of a collaborative human papillomavirus knowledge survey. Public Health 2014, 128, 1099–1105. [Google Scholar] [CrossRef]
- Jelastopulu, E.; Fafliora, E.; Plota, A.; Babalis, V.; Bartsokas, C.; Poulas, K.; Plotas, P. Knowledge, behaviours and attitudes regarding HPV infection and its prevention in female students in West Greece. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 2622–2629. [Google Scholar]
- Rachiotis, G.; Papagiannis, D.; Symvoulakis, E.; Daponte, A.; Grivea, I.; Syrogiannopoulos, G.A.; Hadjichristodoulou, C. Vaccination against human papillomavirus among 865 female students from the health professions in central Greece: A questionnaire- based cross-sectional study. J. Multidiscip. Health 2013, 6, 435–439. [Google Scholar] [CrossRef] [Green Version]
- Bakogianni, G.D.; Nikolakopoulos, K.M.; Nikolakopoulou, N.M. HPV vaccine acceptance among female Greek students. Int. J. Adolesc. Med. Health 2010, 22, 271–274. [Google Scholar] [CrossRef]
- Allen, J.D.; Mohllajee, A.P.; Shelton, R.C.; Othus, M.K.; Fontenot, H.; Hanna, R. Stage of adoption of the human papillomavirus vaccine among college women. Prev. Med. 2009, 48, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Blödt, S.; Holmberg, C.; Müller-Nordhorn, J.; Rieckmann, N. Human Papillomavirus awareness, knowledge and vaccine acceptance: A survey among 18–25 year old male and female vocational school students in Berlin, Germany. Eur. J. Public Health 2011, 22, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Iliadou, M.; Sahini, K.; Sakellari, E.; Daglas, M.; Orovou, E.; Iatrakis, G.; Antoniou, E. What do Young People Think About HPV and HPV Vaccination? The Role of Health Education Interventions and Health Professionals. Mater. Socio Medica 2021, 33, 219. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Wu, J.; Zheng, M. Barriers to and Facilitators of Human Papillomavirus Vaccination Among People Aged 9 to 26 Years: A Systematic Review. Sex Transm. Dis. 2021, 48, e255–e262. [Google Scholar] [CrossRef]
- Kyrka, A.; Tragiannidis, A.; Cassimos, D.; Pantelaki, K.; Tzoufi, M.; Mavrokosta, M.; Pedeli, X.; Athanassiadou, F.; Hatzimichael, A.; Konstantopoulos, A.; et al. Seroepidemiology of hepatitis A among Greek children indicates that the virus is still prevalent: Implication for universal vaccination. J. Med. Virol. 2009, 81, 582–587. [Google Scholar] [CrossRef]
- Katsafadou, A.; Ferentinos, G.; Constantopoulos, A.; Papaevangelou, V. The epidemiology of varicella in school-aged Greek children before the implementation of universal vaccination. Eur. J. Clin. Microbiol. 2007, 27, 223–226. [Google Scholar] [CrossRef]
- Kuter, B.; Matthews, H.; Shinefield, H.; Black, S.; Dennehy, P.; Watson, B.; Reisinger, K.; Kim, L.L.; Lupinacci, L.; Hartzel, J.; et al. Ten year follow-up of healthy children who received one or two injections of varicella vaccine. Pediatr. Infect. Dis. J. 2004, 23, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, N.; Booy, R.; Schmitt, H.J.; Peltola, H.; Van-Damme, P.; Schumacher, R.F.; Campins, M.; Rodrigo, C.; Heikkinen, T.; Seward, J.; et al. Varicella vaccination in Europe: Are we ready for a universal childhood programme? Eur. J. Pediatr. 2008, 167, 47–55. [Google Scholar] [CrossRef]
- Kafetzis, D.; Stamboulidis, K.; Tzanakaki, G.; Kourea Kremastinou, J.; Skevaki, C.; Konstantopoulos, A.; Tsolia, M. Menin-gococcal group C disease in Greece during 1993–2006: The impact of an unofficial single-dose vaccination scheme adopted by most paediatricians. Clinic. Microbiol. Infect. 2007, 13, 550–552. [Google Scholar] [CrossRef] [Green Version]
- Navarro-Torné, A.; Montuori, E.A.; Kossyvaki, V.; Méndez, C. Burden of pneumococcal disease among adults in Southern Europe (Spain, Portugal, Italy, and Greece): A systematic review and meta-analysis. Hum. Vaccin. Immunother. 2021, 17, 3670–3686. [Google Scholar] [CrossRef]
- Wicker, S.; Rabenau, H.F.; Betz, W.; Lauer, H.C. Attitudes of dental healthcare workers towards the influenza vaccination. Int. J. Hyg. Environ. Health 2012, 215, 482–486. [Google Scholar] [CrossRef]
- Hernández-García, I.; Domínguez, B.; González, R. Influenza vaccination rates and determinants among Spanish medical students. Vaccine 2012, 31, 1–2. [Google Scholar] [CrossRef]
- Betsch, C.; Wicker, S. E-health use, vaccination knowledge and perception of own risk: Drivers of vaccination uptake in medical students. Vaccine 2012, 30, 1143–1148. [Google Scholar] [CrossRef] [PubMed]
- Pavlopoulou, I.D.; Daikos, G.L.; Tzivaras, A.; Bozas, E.; Kosmidis, C.; Tsournakas, C.; Theodoridou, M. Medical and nursing students with suboptimal protective immunity against vaccine-preventable diseases. Infect. Control Hosp. Epidemiol. 2009, 30, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Trevisan, A.; Bruno, A.; Mongillo, M.; Morandin, M.; Pantaleoni, A.; Borella-Venturini, M.; Giraldo, M. Prevalence of Markers for Hepatitis B Virus and Vaccination Compliance Among Medical School Students in Italy. Infect. Control Hosp. Epidemiol. 2008, 29, 1189–1191. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| N (%) | |
|---|---|
| Gender | |
| Females | 417 (85.8) |
| Males | 69 (14.2) |
| Age, mean (SD) | 22.2 (1.4) |
| Age | |
| 18–22 | 244 (50.2) |
| 23–30 | 242 (49.8) |
| Full Vaccination Percentage | P Student’s t-Test | ||
|---|---|---|---|
| Mean % | 95% CI | ||
| Total sample | 79 | 78–81 | - |
| Gender | |||
| Females | 80 | 78–81 | 0.10 |
| Males | 76 | 72–81 | |
| Age | |||
| 18–22 | 79 | 77–81 | 0.89 |
| 23–30 | 79 | 77–81 | |
| Full Vaccination Percentage for Vaccines during Childhood | P Student’s t-Test | Full Vaccination Percentage for Vaccines during Adolescence | P Student’s t-Test | |||
|---|---|---|---|---|---|---|
| Mean % | 95% CI | Mean % | 95% CI | |||
| Total sample | 79 | 78–80 | - | 78 | 75–81 | - |
| Gender | ||||||
| Females | 80 | 78–81 | 0.045 | 78 | 74–81 | 0.48 |
| Males | 76 | 71–80 | 81 | 72–89 | ||
| Age | ||||||
| 18–22 | 79 | 77–81 | 0.76 | 78 | 73–82 | 0.83 |
| 23–30 | 79 | 77–81 | 78 | 74–83 | ||
| Total Sample | Gender | |||
|---|---|---|---|---|
| Females | Males | |||
| N (%) | N (%) | N (%) | P | |
| In adolescents | ||||
| Td or Tdap | 238 (70.4) | 201 (69.6) | 37 (75.5) | 0.40 + |
| Men ACWY | 288 (100) | 251 (100) | 37 (100) | - |
| HPV 1 | 285 (75.6) | 282 (76.6) | 3 (33.3) | 0.008 ++ |
| In children < 10 years old | ||||
| DTaP/TdaP | 243 (70.8) | 205 (70) | 38 (76) | 0.39 + |
| Polio (IPV) | 390 (83.3) | 339 (84.1) | 51 (78.5) | 0.26 + |
| Hib | 314 (70.6) | 271 (70.6) | 43 (70.5) | 0.99 + |
| HBV | 448 (95.1) | 390 (96.3) | 58 (87.9) | 0.008 ++ |
| PVC | 45 (13.6) | 39 (13.9) | 6 (11.5) | 0.64 + |
| MMR | 463 (96.1) | 400 (96.9) | 63 (91.3) | 0.04 ++ |
| Var | 404 (86.3) | 354 (87.8) | 50 (76.9) | 0.017 + |
| HAV | 372 (83) | 321 (82.7) | 51 (85) | 0.66 + |
| MCC | 406 (93.1) | 350 (92.8) | 56 (94.9) | 0.78 ++ |
| BCG | 335 (73.8) | 286 (73.3) | 49 (76.6) | 0.59 + |
| Mantoux * | 121 (87.1) | 108 (87.1) | 13 (86.7) | >0.99 ++ |
| Additional vaccines | ||||
| INFL | 293 (64.1) | 251 (63.9) | 42 (65.6) | 0.79 + |
| INFL ** | 91 (34) | 78 (43.1) | 8 (34.8) | 0.45 + |
| MENB 2 | 43 (17.6) | 37 (17.3) | 6 (19.4) | 0.78 + |
| Full Vaccination Percentage for Health Professionals (%) | |||
|---|---|---|---|
| Mean | 95% CI | P | |
| Total sample | 84% | 82–85% | |
| Gender | |||
| Females | 83.90 | 82.4–85.5 | 0.31 |
| Males | 81.70 | 76.6–86.7 | |
| Age | |||
| 18–22 | 84.10 | 81.8–86.3 | 0.54 |
| 23–30 | 83.10 | 81.1–85.2 | |
| Year | Modification |
|---|---|
| 1991 | Inclusion of the second dose of MMR for adolescents 11–12 years |
| 1999 | Shift of the second dose of MMR to children aged of 4–6 years |
| 1998 | Introduction of HBV vaccine |
| 2006 | Inclusion of MenC vaccine |
| 2006 | Introduction of the VAR vaccine (2 doses for children > 12 years old and 1 dose for younger children) |
| 2008 | Modification of the VAR vaccine to two doses for all children >15 months. Inclusion of the HAV vaccine (available since 1995). The Td booster was replaced by the Tdap. Recommendation of catch-up vaccinations for adolescents. |
| 2011 | Introduction of the MenACYW vaccine for adolescents aged of 11–16 years. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrie, E.K.; Sakellari, E.; Barbouni, A.; Tsitsika, A.K.; Lagiou, A. Vaccination Coverage during Childhood and Adolescence among Undergraduate Health Science Students in Greece. Children 2022, 9, 1553. https://doi.org/10.3390/children9101553
Andrie EK, Sakellari E, Barbouni A, Tsitsika AK, Lagiou A. Vaccination Coverage during Childhood and Adolescence among Undergraduate Health Science Students in Greece. Children. 2022; 9(10):1553. https://doi.org/10.3390/children9101553
Chicago/Turabian StyleAndrie, Elisabeth K., Evanthia Sakellari, Anastasia Barbouni, Artemis K. Tsitsika, and Areti Lagiou. 2022. "Vaccination Coverage during Childhood and Adolescence among Undergraduate Health Science Students in Greece" Children 9, no. 10: 1553. https://doi.org/10.3390/children9101553
APA StyleAndrie, E. K., Sakellari, E., Barbouni, A., Tsitsika, A. K., & Lagiou, A. (2022). Vaccination Coverage during Childhood and Adolescence among Undergraduate Health Science Students in Greece. Children, 9(10), 1553. https://doi.org/10.3390/children9101553