
Transitional Care in Pediatric Brain Tumor Patients: A Systematic Literature Review



Abstract
:1. Introduction
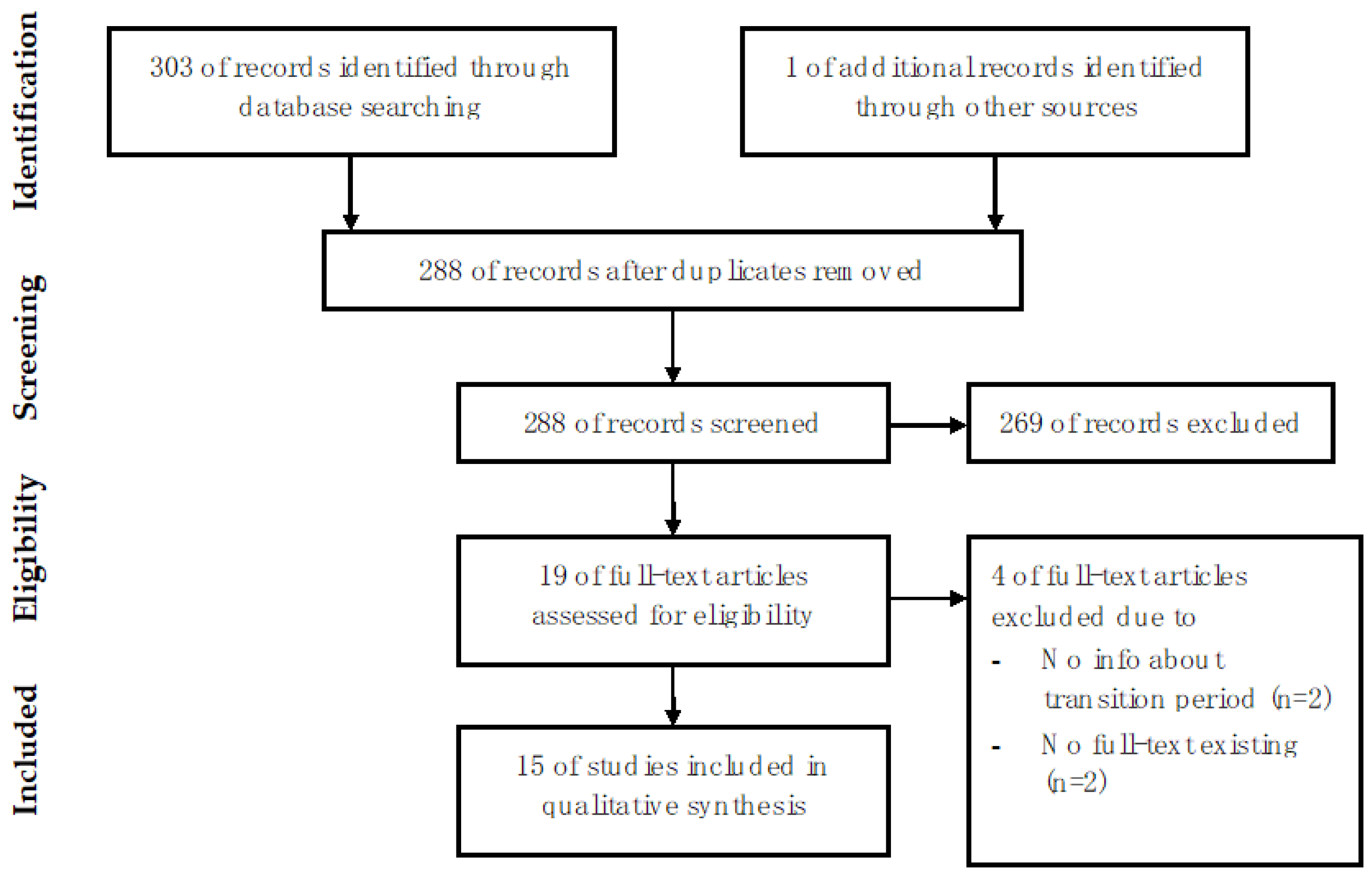
2. Materials and Methods
3. Results
3.1. Transition Models
- The “adult caregiver model”.
- The “shared caregiver model”.
- The “joint caregiver model”.
- The “continued caregiver model”.
- The “specialized clinic model”.
3.2. Difficulties and Challenges from the Patient’s Perspective during the Transition Period, Transition Age, Follow-Up Duration
3.3. Pediatric Brain Tumor Patients
3.4. Neurofibromatosis Type 1 Patients
3.5. Tuberous Sclerosis Complex Patients
4. Discussion
4.1. Transition Models
4.2. Our Institution’s Transition Model
4.3. Difficulties and Challenges during Transition
4.4. Transition Age
4.5. Follow-Up Duration
4.6. Follow-Up Diagnostics
4.7. Future Directions of Transitional Care in Patients with PBT
4.8. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tallen, G.; Resch, A.; Calaminus, G.; Wiener, A.; Leiss, U.; Pletschko, T.; Friedrich, C.; Langer, T.; Grabow, D.; Driever, P.H.; et al. Strategies to improve the quality of survival for childhood brain tumour survivors. Eur. J. Paediatr. Neurol. 2015, 19, 619–639. [Google Scholar] [CrossRef]
- Gajjar, A.; Bowers, D.; Karajannis, M.; Leary, S.; Witt, H.; Gottardo, N. Pediatric Brain Tumors: Innovative Genomic Information Is Transforming the Diagnostic and Clinical Landscape. J. Clin. Oncol. 2015, 33, 2986–2998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sands, S.A.; Zhou, T.; O’Neil, S.H.; Patel, S.K.; Allen, J.; Cullen, P.M.; Kaleita, T.A.; Noll, R.; Sklar, C.; Finlay, J.L. Long-Term Follow-Up of Children Treated for High-Grade Gliomas: Children’s Oncology Group L991 Final Study Report. J. Clin. Oncol. 2012, 30, 943–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, G.T.; Stovall, M.; Robison, L.L. Long-Term Effects of Radiation Exposure among Adult Survivors of Childhood Cancer: Results from the Childhood Cancer Survivor Study. Radiat. Res. 2010, 174, 840–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellenberg, L.; Liu, Q.; Gioia, G.; Yasui, Y.; Packer, R.J.; Mertens, A.; Donaldson, S.S.; Stovall, M.; Kadan-Lottick, N.; Armstrong, G.; et al. Neurocognitive status in long-term survivors of childhood CNS malignancies: A report from the Childhood Cancer Survivor Study. Neuropsychology 2009, 23, 705–717. [Google Scholar] [CrossRef] [Green Version]
- Hudson, M.M.; Mertens, A.C.; Yasui, Y.; Hobbie, W.; Chen, H.; Gurney, J.G.; Yeazel, M.; Recklitis, C.J.; Marina, N.; Robison, L.R.; et al. Health Status of Adult Long-term Survivors of Childhood Cancer: A Report From the Childhood Cancer Survivor Study. JAMA: J. Am. Med. Assoc. 2003, 290, 1583–1592. [Google Scholar] [CrossRef] [Green Version]
- Campbell, F.; Biggs, K.; Aldiss, S.K.; O’Neill, P.M.; Clowes, M.; McDonagh, J.; While, A.; Gibson, F. Transition of care for adolescents from paediatric services to adult health services. Cochrane Database Syst. Rev. 2016, 4, CD009794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bar, C.; Ghobeira, R.; Azzi, R.; Ville, D.; Riquet, A.; Touraine, R.; Chemaly, N.; Nabbout, R. Experience of follow-up, quality of life, and transition from pediatric to adult healthcare of patients with tuberous sclerosis complex. Epilepsy Behav. 2019, 96, 23–27. [Google Scholar] [CrossRef]
- Both, P.; Holt, L.T.; Mous, S.; Patist, J.; Rietman, A.; Dieleman, G.; Hoopen, L.T.; Vergeer, M.; de Wit, M.-C.; Heus, K.B.-D.; et al. Tuberous sclerosis complex: Concerns and needs of patients and parents from the transitional period to adulthood. Epilepsy Behav. 2018, 83, 13–21. [Google Scholar] [CrossRef]
- Roux, A.; Beccaria, K.; Blauwblomme, T.; Mahlaoui, N.; Chretien, F.; Varlet, P.; Puget, S.; Pallud, J. Toward a transitional care from childhood and adolescence to adulthood in surgical neurooncology? A lesson from the Necker-Enfants Malades and the Sainte-Anne Hospitals collaboration. J. Neurosurgery Pediatr. 2021, 28, 380–386. [Google Scholar] [CrossRef]
- Thiele, E.A.; Granata, T.; Matricardi, S.; Chugani, H.T. Transition into adulthood: Tuberous sclerosis complex, Sturge-Weber syndrome, and Rasmussen encephalitis. Epilepsia 2014, 55, 29–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Lierde, A.; Menni, F.; Bedeschi, M.F.; Natacci, F.; Guez, S.; Vizziello, P.; Costantino, M.A.; Lalatta, F.; Esposito, S. Healthcare transition in patients with rare genetic disorders with and without developmental disability: Neurofibromatosis 1 and williams-beuren syndrome. Am. J. Med. Genet. Part A 2013, 161, 1666–1674. [Google Scholar] [CrossRef] [PubMed]
- Vinchon, M.; Dhellemmes, P. The transition from child to adult in neurosurgery. Adv. Tech. Stand. Neurosurg. 2007, 32, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Vinchon, M.; Baroncini, M.; Leblond, P.; Delestret, I. Morbidity and tumor-related mortality among adult survivors of pediatric brain tumors: A review. Child’s Nerv. Syst. 2011, 27, 697–704. [Google Scholar] [CrossRef]
- Ellenbogen, Y.; Yang, K.; Ajani, O. Transition of Care for Children with High-Grade Central Nervous System Tumors. J. Pediatr. Neurol. 2020, 18, 301–306. [Google Scholar] [CrossRef]
- Eshelman-Kent, D.; Gilger, E.; Gallagher, M. Transitioning Survivors of Central Nervous System Tumors: Challenges for Patients, Families, and Health Care Providers. J. Pediatr. Oncol. Nurs. 2009, 26, 280–294. [Google Scholar] [CrossRef]
- Evans, D.G.R.; Salvador, H.; Chang, V.Y.; Erez, A.; Voss, S.D.; Schneider, K.W.; Scott, H.S.; Plon, S.E.; Tabori, U. Cancer and Central Nervous System Tumor Surveillance in Pediatric Neurofibromatosis 1. Clin. Cancer Res. 2017, 23, e46–e53. [Google Scholar] [CrossRef] [Green Version]
- Heitzer, A.M.; Ris, D.; Raghubar, K.; Kahalley, L.S.; Hilliard, M.E.; Gragert, M. Facilitating Transitions to Adulthood in Pediatric Brain Tumor Patients: The Role of Neuropsychology. Curr. Oncol. Rep. 2020, 22, 102. [Google Scholar] [CrossRef]
- Janss, A.J.; Mazewski, C.; Patterson, B. Guidelines for Treatment and Monitoring of Adult Survivors of Pediatric Brain Tumors. Curr. Treat. Options Oncol. 2019, 20, 10. [Google Scholar] [CrossRef]
- Nicklin, E.; Pointon, L.; Glaser, A.; Sarwar, N.; Kwok-Williams, M.; Debono, M.; Velikova, G.; Boele, F.W. Unmet support needs in teenage and young adult childhood brain tumour survivors and their caregivers: “it’s all the aftermath, and then you’re forgotten about”. Support. Care Cancer 2021, 29, 6315–6324. [Google Scholar] [CrossRef]
- Peron, A.; Canevini, M.P.; Ghelma, F.; di Marco, F.; Vignoli, A. Healthcare transition from childhood to adulthood in Tuberous Sclerosis Complex. Am. J. Med. Genet. Part C Semin. Med. Genet. 2018, 178, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Rietman, A.B.; Van Helden, H.; Both, P.H.; Taal, W.; Legerstee, J.S.; van Staa, A.; Moll, H.A.; Oostenbrink, R.; Van Eeghen, A.M. Worries and needs of adults and parents of adults with neurofibromatosis type 1. Am. J. Med. Genet. Part A 2018, 176, 1150–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greuter, L.; Guzman, R.; Soleman, J. Typical Pediatric Brain Tumors Occurring in Adults—Differences in Management and Outcome. Biomedicines 2021, 9, 356. [Google Scholar] [CrossRef] [PubMed]
- Greuter, L.; Guzman, R.; Soleman, J. Pediatric and Adult Low-Grade Gliomas: Where Do the Differences Lie? Children 2021, 8, 1075. [Google Scholar] [CrossRef]
- Turner, C.D.; Rey-Casserly, C.; Liptak, C.C.; Chordas, C. Late Effects of Therapy for Pediatric Brain Tumor Survivors. J. Child Neurol. 2009, 24, 1455–1463. [Google Scholar] [CrossRef]
- Steinbok, P.; Hentschel, S.; Cochrane, D.; Kestle, J.R.W. Value of postoperative surveillance imaging in the management of children with some common brain tumors. J. Neurosurg. 1996, 84, 726–732. [Google Scholar] [CrossRef]
- Zaazoue, M.A.; Manley, P.E.; Al Mehdar, M.; Ullrich, N.J.; Dasenbrock, H.H.; Chordas, C.A.; Goumnerova, L.C. Optimizing Postoperative Surveillance of Pediatric Low-Grade Glioma Using Tumor Behavior Patterns. Clin. Neurosurg. 2020, 86, 288–297. [Google Scholar] [CrossRef]
- Children’s Oncology Group. Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers. 2018. Available online: www.survivorshipguidelines.org (accessed on 20 February 2022).
- Bergqvist, C.; Network, N.F.; Servy, A.; Valeyrie-Allanore, L.; Ferkal, S.; Combemale, P.; Wolkenstein, P. Neurofibromatosis 1 French national guidelines based on an extensive literature review since 1966. Orphanet J. Rare Dis. 2020, 15, 37. [Google Scholar] [CrossRef] [Green Version]
- Krueger, D.A.; Northrup, H.; Krueger, D.A.; Roberds, S.; Smith, K.; Sampson, J.; Korf, B.; Kwiatkowski, D.J.; Mowat, D.; Nellist, M.; et al. Frost, Tuberous Sclerosis Complex Surveillance and Management: Recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr. Neurol. 2013, 49, 255–265. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Models | Description | Advantages | Disadvantages | Mentioned in (%) | Subcategory (n) |
|---|---|---|---|---|---|
| Adult caregiver model | Transition from multidisciplinary pediatric care to an adult primary care provider |
|
| 5/11 studies (45.5%) [8,9,15,16,21] | PBT (2) TSC (3) |
| Shared caregiver model | Shared care by two or more providers of different specialties (e.g., GP and cancer center) |
| 2/11 studies (18.2%) [15,16] | PBT (2) | |
| Joint caregiver model | Joint consultations with the previous and future physician for a certain period during the transition period | 5/11 studies (45.5%) [9,10,12,16,21] | PBT (2) NF1 (1) TSC (2) | ||
| Continued caregiver model | Continued follow-up by the pediatric specialist team (e.g., pediatric neurology or neurooncology team) |
|
| 3/11 studies (27.3%) [13,15,20] | PBT (3) |
| Specialized clinic model | Patients are followed up and treated lifelong in a specialized clinic (e.g., neurocutaneous disease clinic) treating pediatric and adult patients |
| 3/11 studies (27.3%) [17,21,22] | TSC (1) NF1 (2) |
| PBT Patients | NF1 Patients | TSC Patients | |
|---|---|---|---|
| Problems during transition |
| ||
| Suggested age of transition |
| ||
| Follow-up duration |
| N/A | |
| Follow-up diagnostics * |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ebel, F.; Greuter, L.; Guzman, R.; Soleman, J. Transitional Care in Pediatric Brain Tumor Patients: A Systematic Literature Review. Children 2022, 9, 501. https://doi.org/10.3390/children9040501
Ebel F, Greuter L, Guzman R, Soleman J. Transitional Care in Pediatric Brain Tumor Patients: A Systematic Literature Review. Children. 2022; 9(4):501. https://doi.org/10.3390/children9040501
Chicago/Turabian StyleEbel, Florian, Ladina Greuter, Raphael Guzman, and Jehuda Soleman. 2022. "Transitional Care in Pediatric Brain Tumor Patients: A Systematic Literature Review" Children 9, no. 4: 501. https://doi.org/10.3390/children9040501
APA StyleEbel, F., Greuter, L., Guzman, R., & Soleman, J. (2022). Transitional Care in Pediatric Brain Tumor Patients: A Systematic Literature Review. Children, 9(4), 501. https://doi.org/10.3390/children9040501