
Photoplethysmography Analysis with Duffing–Holmes Self-Synchronization Dynamic Errors and 1D CNN-Based Classifier for Upper Extremity Vascular Disease Screening





 and
and 
Abstract
:1. Introduction
2. Materials and Methods
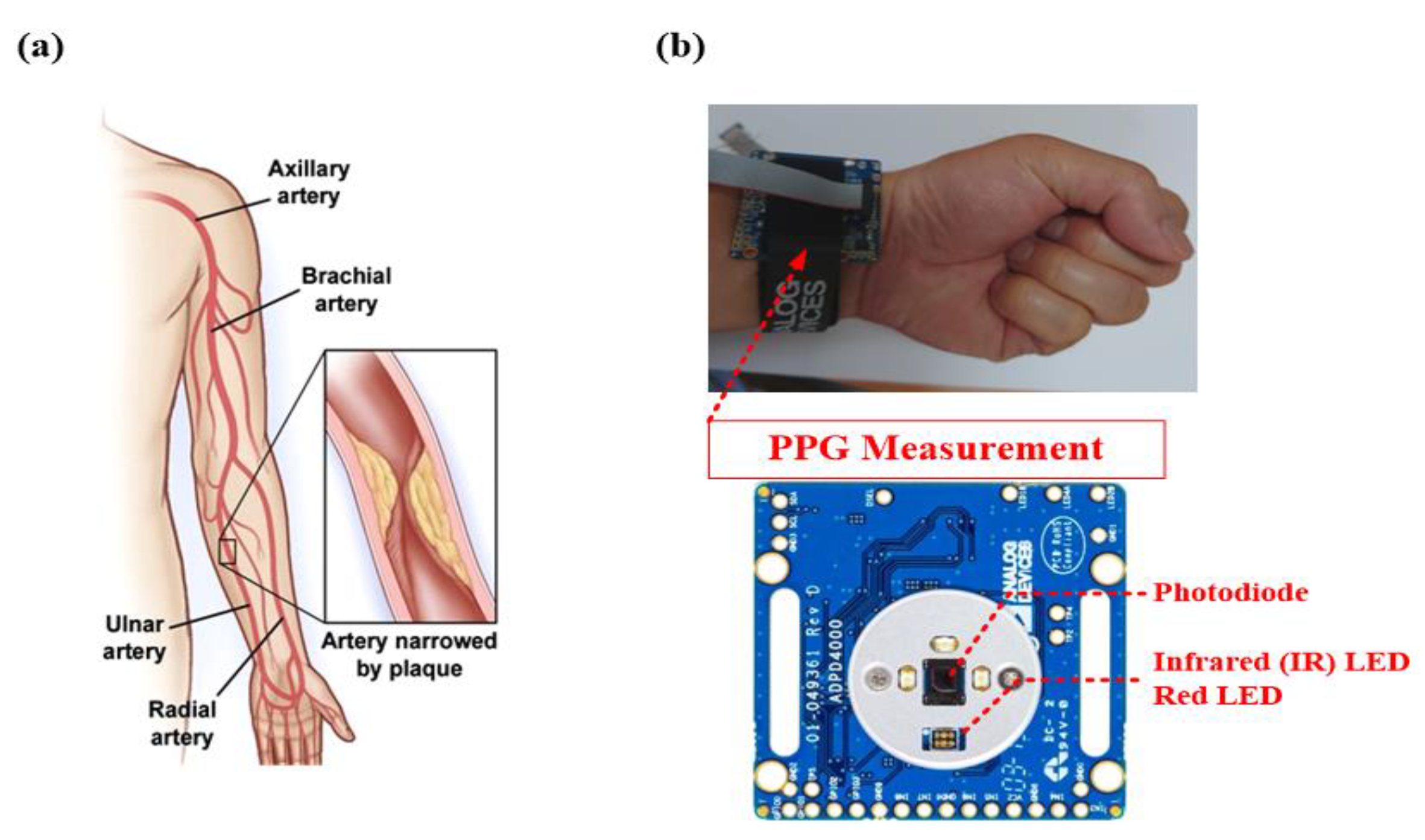
2.1. PPG Measurement
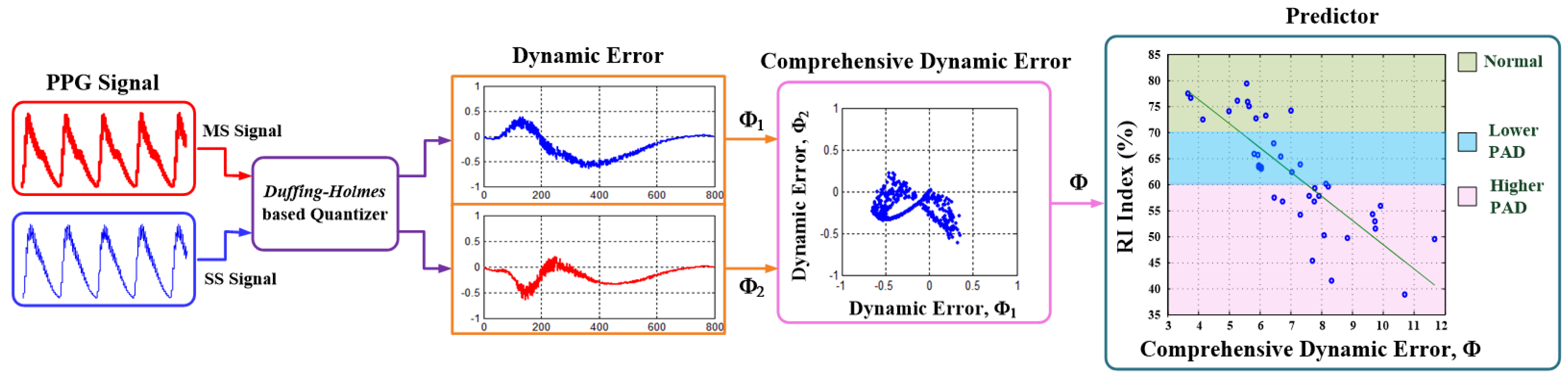
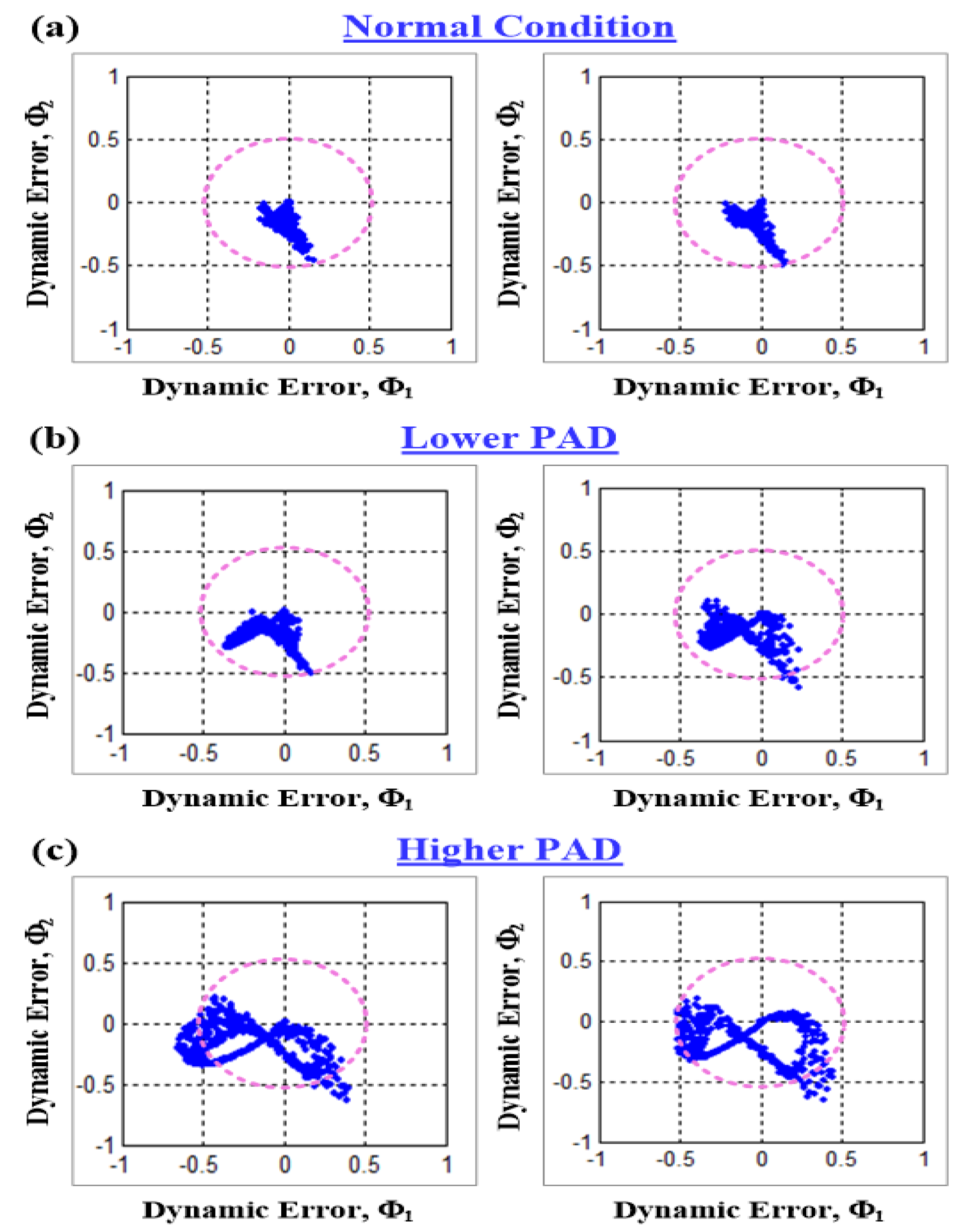
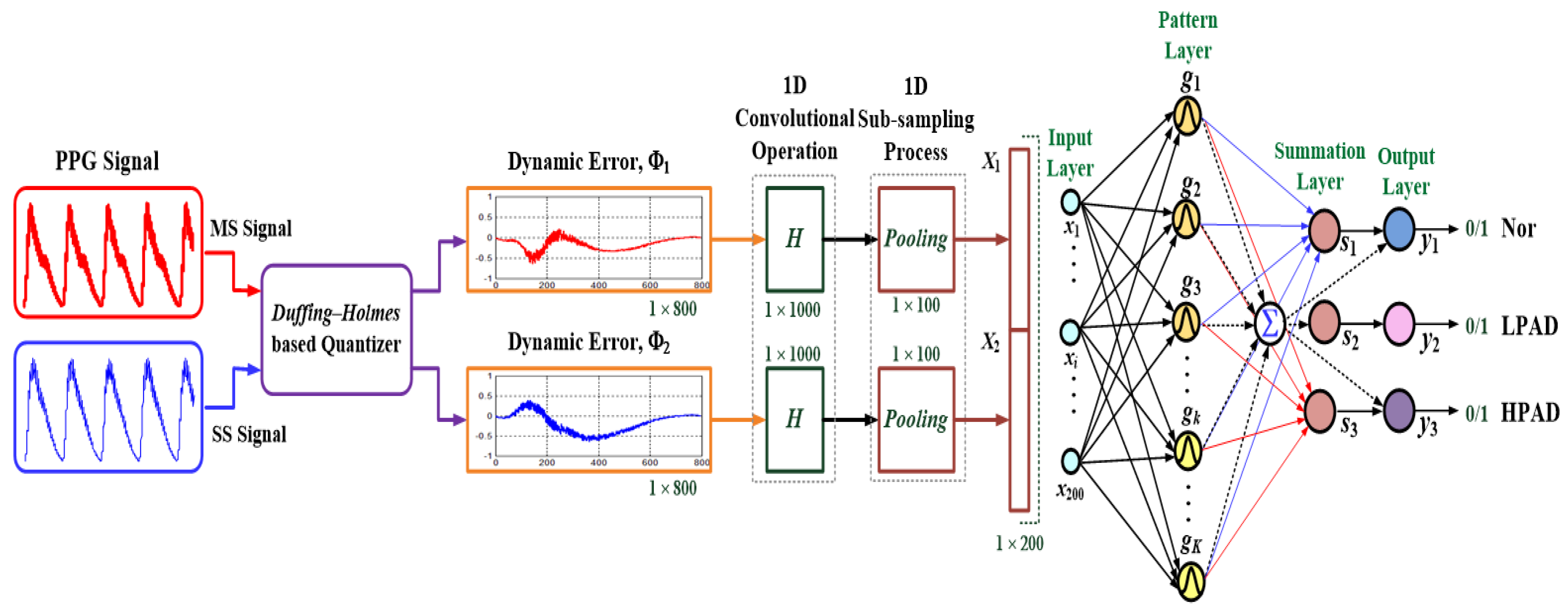
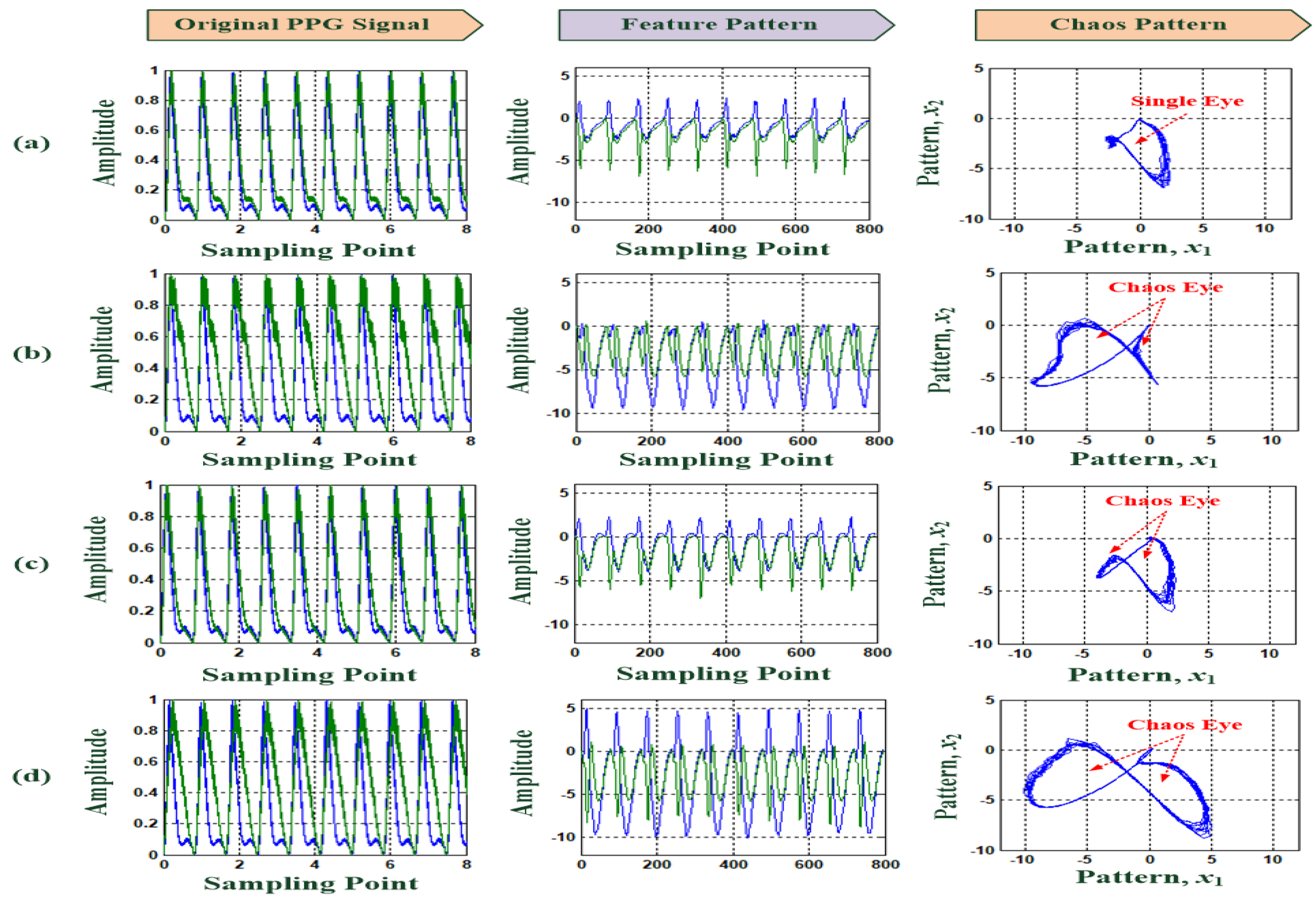
2.2. Duffing–Holmes-Based Quantizer
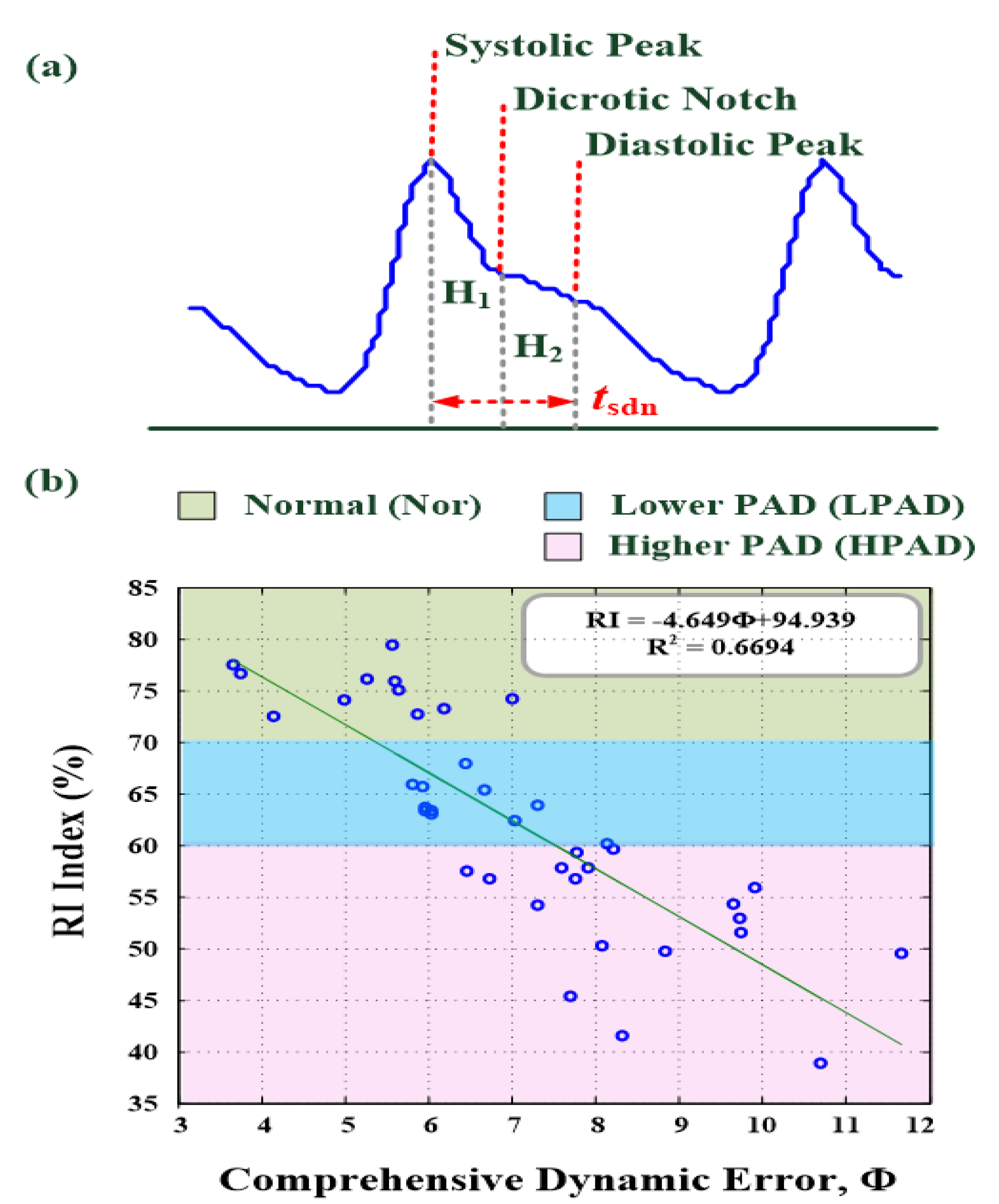
2.3. Time-Domain Analysis with Reflection Index
2.4. 1D CNN-Based Classifier
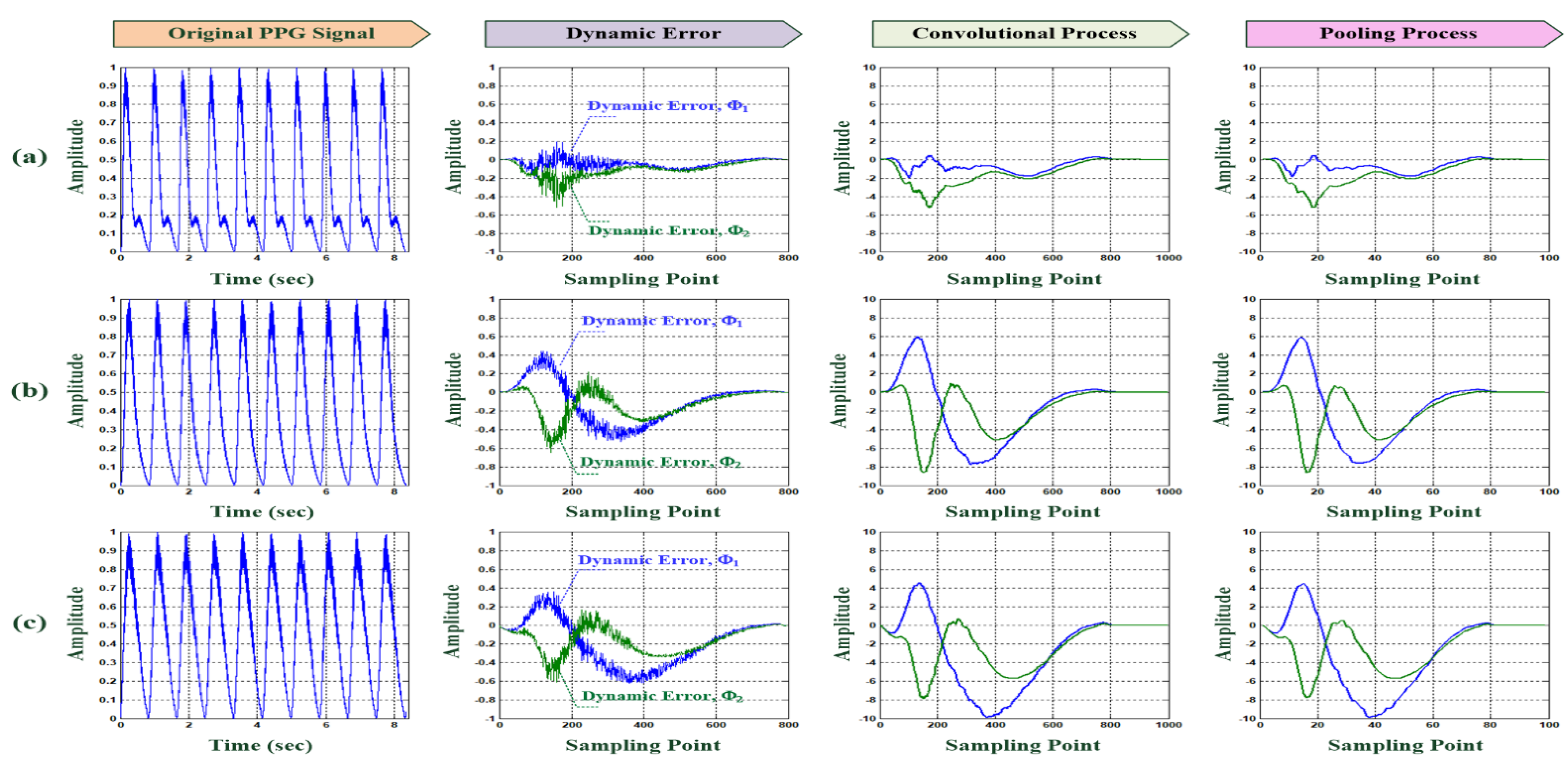
- 1D convolution operations:
- 1D subsampling (pooling) process:
- Multilayer classifier with a fully connected network:
3. Experimental Results and Discussion
3.1. Feasibility Tests Using for PPG Feature Extraction
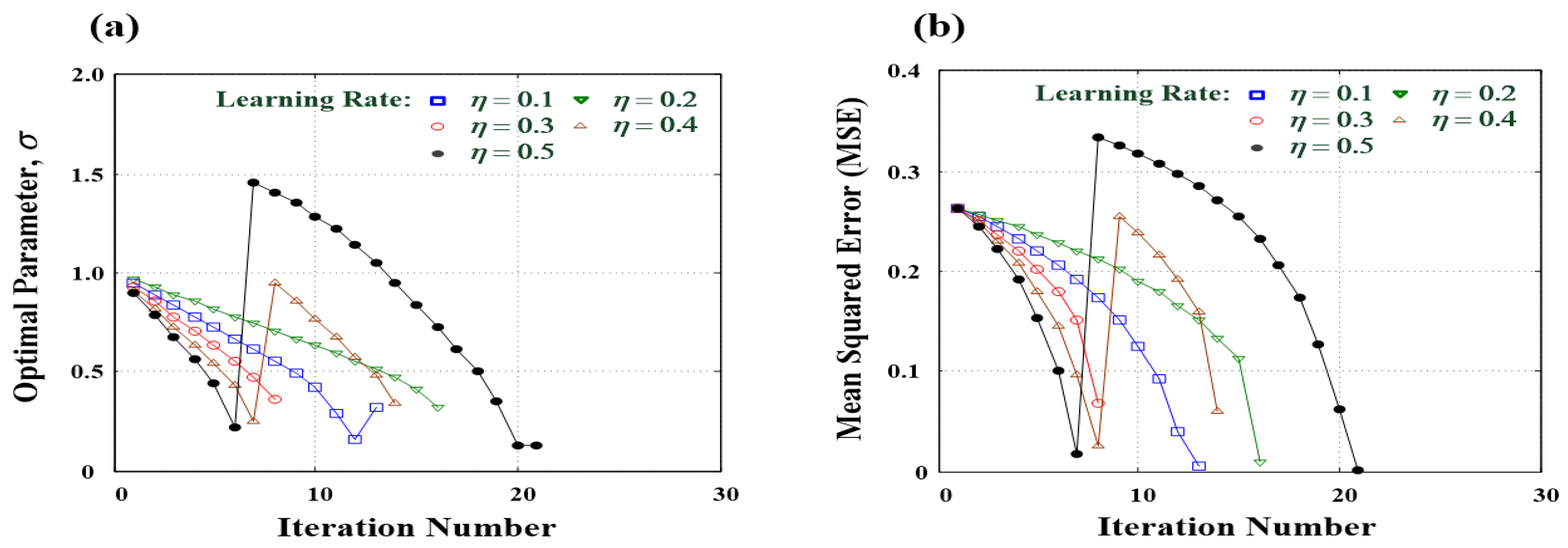
3.2. D CNN-Based Classifier Training and Testing
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chiang, C.-E.; Ueng, K.-C.; Chao, T.-H.; Lin, T.-H.; Wu, Y.-J.; Wang, K.-L.; Sung, S.-H.; Yeh, H.-I.; Li, Y.-H.; Liu, P.-Y.; et al. 2020 Consensus of Taiwan Society of Cardiology on the pharmacological management of patients with type 2 diabetes and cardiovascular diseases. J. Chin. Med. Assoc. 2020, 83, 587–621. [Google Scholar] [CrossRef]
- Wu, J.-X.; Li, C.-M.; Ho, Y.-R.; Wu, M.-J.; Huang, P.-T.; Lin, C.-H. Bilateral Photoplethysmography Analysis for Peripheral Arterial Stenosis Screening with a Fractional-Order Integrator and Info-Gap Decision-Making. IEEE Sens. J. 2016, 16, 2691–2700. [Google Scholar] [CrossRef]
- Upper Extremity Vascular Disease, Johns Hopkins. 2021. Available online: https://www.hopkinsmedicine.org/heart_vascular_institute/conditions_treatments/conditions/upper_extremity_vascular_disease.html (accessed on 19 November 2021).
- Society for Vascular Surgery (SVS). Arm Artery Disease. 2021. Available online: https://vascular.org/patients/vascular-conditions/arm-artery-disease (accessed on 19 November 2021).
- Shu, J.; Santulli, G. Update on peripheral artery disease: Epidemiology and evidence-based facts. Atherosclerosis 2018, 275, 379–381. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, A.U.; Koktzoglou, I.; Edelman, R.R.; Gilkeson, R.; Mihai, G.; Shin, T.; Rajagopalan, S. Noncontrast Magnetic Resonance Angiography for the Diagnosis of Peripheral Vascular Disease. Circ. Cardiovasc. Imaging 2019, 12, e008844. [Google Scholar] [CrossRef]
- Stepansky, F.; Hecht, E.M.; Rivera, R.; Hirsh, L.E.; Taouli, B.; Kaur, M.; Lee, V.S. Dynamic MR Angiography of Upper Extremity Vascular Disease: Pictorial Review1. Radiographics 2008, 28, e28. [Google Scholar] [CrossRef] [PubMed]
- Fujita, D.; Suzuki, A. Evaluation of the Possible Use of PPG Waveform Features Measured at Low Sampling Rate. IEEE Access 2019, 7, 58361–58367. [Google Scholar] [CrossRef]
- Phan, D.; Siong, L.Y.; Pathirana, P.N.; Seneviratne, A. Smartwatch: Performance Evaluation for Long-Term Heart Rate Monitoring. In Proceedings of the 2015 International Symposium on Bioelectronics and Bioinformatics, Beijing, China, 14–17 October 2015. [Google Scholar]
- Jiang, W.; Majumder, S.; Subramaniam, S.; Li, X.; Khedri, R.; Monday, T.; Abolghasemian, M.; Satia, I.; Deen, M.J. A Wearable Tele-Health System towards Monitoring COVID-19 and Chronic Diseases. IEEE Rev. Biomed. Eng. 2021. [Google Scholar] [CrossRef]
- Stojanovic, R.; Skraba, A. Simplified open HW/SW pulse oximetry interface for purpose of COVID-19 symptoms detection and monitoring. In Proceedings of the 2021 10th Mediterranean Conference on Embedded Computing, Budva, Montenegro, 7–10 June 2021. [Google Scholar]
- Dolan, E.; Thijs, L.; Li, Y.; Atkins, N.; Mc-Cormack, P.; McClory, S.; O’Brien, E.; Staessen, J.A.; Stanton, A.V. Ambulatory arterial stiffness index as a predictor of cardiovascular mortality in the ublin outcome study. Hypertension 2006, 47, 365–370. [Google Scholar] [CrossRef] [Green Version]
- Brillante, D.G.; O’Sullivan, A.J.; Howes, L.G. Arterial stiffness indices in healthy volunteers using non-invasive digital photoplethysmography. Blood Press. 2008, 17, 116–123. [Google Scholar] [CrossRef] [Green Version]
- Tomiyama, H.; Komatsu, S.; Shiina, K.; Matsumoto, C.; Kimura, K.; Fujii, M.; Takahashi, L.; Chikamori, T.; Yamashina, A. Effect of Wave Reflection and Arterial Stiffness on the Risk of Development of Hypertension in Japanese Men. J. Am. Hear. Assoc. 2018, 7, e008175. [Google Scholar] [CrossRef] [Green Version]
- Elgendi, M. PPG Signal Analysis: An Introduction Using MATLAB; Taylor & Francis Group, LLC: Abingdon, UK, 2021. [Google Scholar]
- Kana, M.; Holcik, J. Mathematical model-based markers of autonomic nervous system activity during the Valsalva Maneuver and comparison to heart rate variability. Biomed. Signal Process. Control 2011, 6, 251–260. [Google Scholar] [CrossRef]
- Akar, S.A.; Kara, S.; Latifoğlu, F.; Bilgiç, V. Spectral analysis of photoplethysmographic signals: The importance of preprocessing. Biomed. Signal Process. Control 2013, 8, 16–22. [Google Scholar] [CrossRef]
- Bellenger, C.; Miller, D.; Halson, S.; Roach, G.; Sargent, C. Wrist-Based Photoplethysmography Assessment of Heart Rate and Heart Rate Variability: Validation of WHOOP. Sensors 2021, 21, 3571. [Google Scholar] [CrossRef]
- Syntax: Detrend, 1994–2021. Available online: https://www.mathworks.com/help/matlab/ref/detrend.html?s_tid=srchtitle_detrending_1 (accessed on 19 November 2021).
- Tarvainen, M.P.; Ranta-Aho, P.O.; Karjalainen, P. An advanced detrending method with application to HRV analysis. IEEE Trans. Biomed. Eng. 2002, 49, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-N.; Chen, W.-L.; Kan, C.-D.; Pai, C.-C.; Lin, C.-H.; Wu, J.-X.; Pai, N.-S. Rapid in vitro evaluation of hemodynamic performances of customized handmade trileaflet-valved conduits using Duffing–Holmes-based self-synchronization dynamic errors. IET J. Eng. 2021, 2021. [Google Scholar] [CrossRef]
- Butkevich, Y.R.; Afanasiev, V.V.; Loginov, S.S. Communication System Based on Chaotic Masking Binary Phase Manipulation and Nonlinear Filtering. In Proceedings of the 2021 Systems of Signal Synchronization, Generating and Processing in Telecommunications, Kaliningrad, Russia, 30 June–2 July 2021; pp. 1–4. [Google Scholar]
- Zivieri, R.; Vergura, S.; Carpentieri, M. Analytical and numerical solution to the nonlinear cubic Duffing equation: An application to electrical signal analysis of distribution lines. Appl. Math. Model. 2016, 40, 9152–9164. [Google Scholar] [CrossRef]
- Longsuo, L. Suppressing Chaos of Duffing-Holmes System Using Random Phase. Math. Probl. Eng. 2011, 2011, 538202. [Google Scholar] [CrossRef] [Green Version]
- Li, C.M.; Du, Y.C.; Wu, J.X.; Lin, C.H.; Ho, Y.R.; Lin, Y.J.; Chen, T. Synchronizing chaotification with support vector machine and wolf pack search algorithm for estimation of peripheral vascular occlusion in diabetes mellitus. Biomed. Signal Process. Control 2014, 9, 45–55. [Google Scholar] [CrossRef]
- Lao, S.-K.; Chen, H.-K.; Tam, L.-M.; Sheu, L.-J. Microfluidic mixing using chaotic signals from the Chen-Lee system. In Proceedings of the 2015 International Conference on Advanced Robotics and Intelligent Systems (ARIS), Taipei, Taiwan, 29–31 May 2015; pp. 1–5. [Google Scholar]
- Kuo, C.-L.; Lin, C.-H.; Yau, H.-T.; Chen, J.-L. Using Self-Synchronization Error Dynamics Formulation Based Controller for Maximum Photovoltaic Power Tracking in Micro-Grid Systems. IEEE J. Emerg. Sel. Top. Circuits Syst. 2013, 3, 459–467. [Google Scholar] [CrossRef]
- Tamaševičiūtė, E.; Tamaševičius, A.; Mykolaitis, G.; Bumelienė, S. Analogue Electrical Circuit for Simulation of the Duffing-Holmes Equation. Nonlinear Anal. Model. Control 2008, 13, 241–252. [Google Scholar] [CrossRef] [Green Version]
- Kuo, Y.-P.; Kuo, C.-L.; Lin, C.-H.; Pu, Y.-R.; Liang, S.-M. Terminal fuzzy sliding mode control for the Duffing-Holmes system. In Proceedings of the 2011 International Conference on Fluid Power and Mechatronics, Beijing, China, 17–20 August 2011; pp. 473–476. [Google Scholar]
- Kiranyaz, S.; Avci, O.; Abdeljaber, O.; Ince, T.; Gabbouj, M.; Inman, D.J. 1D convolutional neural networks and applications: A survey. Mech. Syst. Signal Process. 2021, 151, 107398. [Google Scholar] [CrossRef]
- Lin, C.-H.; Wu, J.-X.; Kan, C.-D.; Chen, P.-Y.; Chen, W.-L. Arteriovenous shunt stenosis assessment based on empirical mode decomposition and 1D-convolutional neural network: Clinical trial stage. Biomed. Signal Process. Control 2021, 66, 102461. [Google Scholar] [CrossRef]
- Techentin, R.W.; Felton, C.L.; Schlotman, T.E.; Gilbert, B.K.; Joyner, M.J.; Curry, T.B.; Convertino, V.A.; Holmes, D.R.; Haider, C.R. 1D Convolutional Neural Networks for Estimation of Compensatory Reserve from Blood Pressure Waveforms. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Berlin, Germany, 23–27 July 2019; Volume 2019, pp. 2169–2173. [Google Scholar]
- Allen, J.; Liu, H.; Iqbal, S.; Zheng, D.; Stansby, G. Deep learning-based photoplethysmography classification for peripheral arterial disease detection: A proof-of-concept study. Physiol. Meas. 2021, 42, 054002. [Google Scholar] [CrossRef]
- Lee, J.J.; Heo, J.H.; Han, J.H.; Kim, B.R.; Gwon, H.Y.; Yoon, Y.R. Prediction of Ankle Brachial Index with Photoplethysmography Using Convolutional Long Short Term Memory. J. Med. Biol. Eng. 2020, 40, 282–291. [Google Scholar] [CrossRef]
- Panwar, M.; Gautam, A.; Dutt, R.; Acharyya, A. CardioNet: Deep Learning Framework for Prediction of CVD Risk Factors. In Proceedings of the 2020 IEEE International Symposium on Circuits and Systems, Seville, Spain, 12–14 October 2020; pp. 1–5. [Google Scholar]
- Burnham, K.P.; Anderson, D. Model Selection and Multi-Model Inference, 2nd ed.; Springer: New York, NY, USA, 2002. [Google Scholar]
- Kan, C.-D.; Chen, W.-L.; Lin, C.-H.; Wang, J.-N.; Lu, P.-J.; Chan, M.-Y.; Wu, J.-T. Customized Handmade Pulmonary Valved Conduit Reconstruction for Children and Adult Patients Using Meta-Learning Based Intelligent Model. IEEE Access 2018, 6, 21381–21396. [Google Scholar] [CrossRef]
- Wu, J.-X.; Liu, H.-C.; Chen, P.-Y.; Lin, C.-H.; Chou, Y.-H.; Shung, K.K. Enhancement of ARFI-VTI Elastography Images in Order to Preliminary Rapid Screening of Benign and Malignant Breast Tumors Using Multilayer Fractional-Order Machine Vision Classifier. IEEE Access 2020, 8, 164222–164237. [Google Scholar] [CrossRef]
- Lin, C.-H.; Wu, J.-X.; Chen, P.-Y.; Lai, H.-Y.; Li, C.-M.; Kuo, C.-L.; Pai, N.-S. Intelligent Symmetric Cryptography With Chaotic Map and Quantum Based Key Generator for Medical Images Infosecurity. IEEE Access 2021, 9, 118624–118639. [Google Scholar] [CrossRef]
- EVAL-ADPD4000Z-PPG User Guide, 1995–2021. Available online: https://www.Analog.com/media/en/technical-documentation/user-guides/EVAL-ADPD4000Z-PPG-UG-1529.pdf (accessed on 19 November 2021).
- Syntax: Conv, 1994–2021. Available online: https://www.mathworks.com/help/matlab/ref/conv.html (accessed on 19 November 2021).
- Sequence-to-Sequence Classification Using 1-D Convolutions, 1994–2021. Available online: https://www.mathworks.com/help/deeplearning/ug/sequence-to-sequence-classification-using-1-d-convolutions.html (accessed on 19 November 2021).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathology Class | Φ | RI (%) |
|---|---|---|
| Normal (11) | 5.34 ± 0.84 | 75.20 ± 4.17 |
| LPAD (11) | 6.48 ± 0.83 | 64.07 ± 3.91 |
| HPAD (18) | 8.56 ± 0.81 | 52.77 ± 19.64 |
| Layer Function | Manner | Feature Pattern |
|---|---|---|
| Feature Extraction Layer | D–H based Quantizer | Φ1 and Φ2 (1 × 799) |
| Feature Enhancement Layer | 2 1D Convolutional Operations [40] (stride = 1) | X1 and X2 (1 × 998) |
| Simplifying Feature Layer | 2 1D Pooling Processes (stride = 10) | x1 and x2 (1 × 100) |
| Classification Layer | Multilayer Classifier: 200 input nodes, 40 pattern nodes, 4 summation nodes, 3 output nodes | Input Pattern of Fully Connecting Network: [x1|x2] (1 × 200) |
| Learning Algorithm: Gradient Descent Method |
| Cross-Validation | Trained Patterns | Untrained Patterns | Recall (%) | Precision (%) | Accuracy (%) | F1 Score | Youdens Index |
|---|---|---|---|---|---|---|---|
| 1 | Random Selection Normality: 11 patterns Abnormality: 29 patterns Total of Trained Pattern: 40 | Random Selection Normality: 11 patterns Abnormality: 29 patterns Total of Trained Pattern: 40 | 100.00 (TP: 27, FN: 0) | 93.10 (TP: 27, FP: 2) | 95.00 (2 failures) | 0.9643 | 0.8462 |
| 2 | 100.00 (TP: 28, FN: 0) | 96.55 (TP: 28, FP: 1) | 97.50 (1 failures) | 0.9825 | 0.9167 | ||
| 3 | 96.43 (TP: 27, FN: 1) | 93.10 (TP: 27, FP: 2) | 92.50 (3 failures) | 0.9474 | 0.7976 | ||
| 4 | 100.00 (TP: 27, FN: 0) | 93.10 (TP: 27, FP: 2) | 95.00 (2 failures) | 0.9643 | 0.8462 | ||
| 5 | 100.00 (TP: 28, FN: 0) | 96.55 (TP: 28, FP: 1) | 97.50 (1 failures) | 0.9825 | 0.9167 | ||
| 6 | 93.33 (TP: 28, FN: 2) | 96.55 (TP: 28, FP: 1) | 92.50 (3 failures) | 0.9492 | 0.8333 | ||
| 7 | 96.43 (TP: 27, FN: 1) | 93.10 (TP: 27, FP: 2) | 92.50 (3 failures) | 0.9474 | 0.7976 | ||
| 8 | 96.43 (TP: 27, FN: 0) | 93.10 (TP: 27, FP: 2) | 95.00 (2 failures) | 0.9643 | 0.8462 | ||
| 9 | 96.43 (TP: 27, FN: 1) | 93.10 (TP: 27, FP: 2) | 92.50 (3 failures) | 0.9474 | 0.7976 | ||
| 10 | 96.55 (TP: 28, FN: 1) | 96.55 (TP: 28, FP: 1) | 95.00 (2 failures) | 0.9655 | 0.8746 | ||
| Average (%) | 97.92 | 94.48 | 94.50 | 0.9615 | 0.8473 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, P.-Y.; Sun, Z.-L.; Wu, J.-X.; Pai, C.-C.; Li, C.-M.; Lin, C.-H.; Pai, N.-S. Photoplethysmography Analysis with Duffing–Holmes Self-Synchronization Dynamic Errors and 1D CNN-Based Classifier for Upper Extremity Vascular Disease Screening. Processes 2021, 9, 2093. https://doi.org/10.3390/pr9112093
Chen P-Y, Sun Z-L, Wu J-X, Pai C-C, Li C-M, Lin C-H, Pai N-S. Photoplethysmography Analysis with Duffing–Holmes Self-Synchronization Dynamic Errors and 1D CNN-Based Classifier for Upper Extremity Vascular Disease Screening. Processes. 2021; 9(11):2093. https://doi.org/10.3390/pr9112093
Chicago/Turabian StyleChen, Pi-Yun, Zheng-Lin Sun, Jian-Xing Wu, Ching-Chou Pai, Chien-Ming Li, Chia-Hung Lin, and Neng-Sheng Pai. 2021. "Photoplethysmography Analysis with Duffing–Holmes Self-Synchronization Dynamic Errors and 1D CNN-Based Classifier for Upper Extremity Vascular Disease Screening" Processes 9, no. 11: 2093. https://doi.org/10.3390/pr9112093
APA StyleChen, P. -Y., Sun, Z. -L., Wu, J. -X., Pai, C. -C., Li, C. -M., Lin, C. -H., & Pai, N. -S. (2021). Photoplethysmography Analysis with Duffing–Holmes Self-Synchronization Dynamic Errors and 1D CNN-Based Classifier for Upper Extremity Vascular Disease Screening. Processes, 9(11), 2093. https://doi.org/10.3390/pr9112093