
The Effect of Scanning Strategy on Intraoral Scanner’s Accuracy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
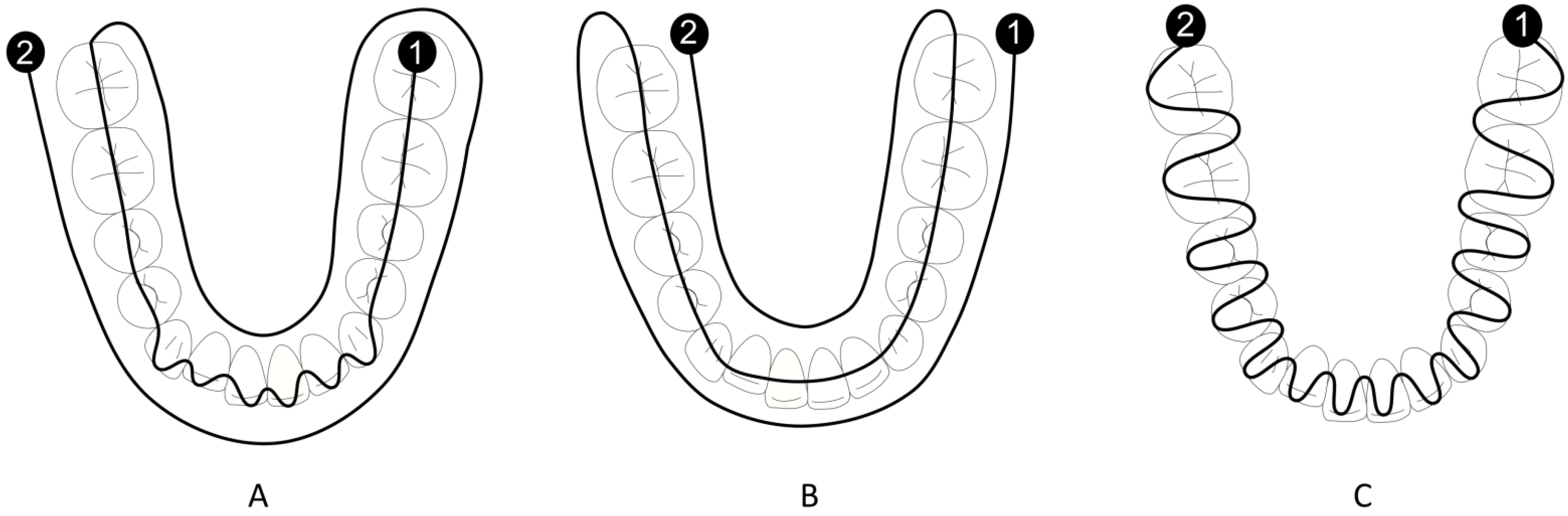
2.2. Scanning Procedure
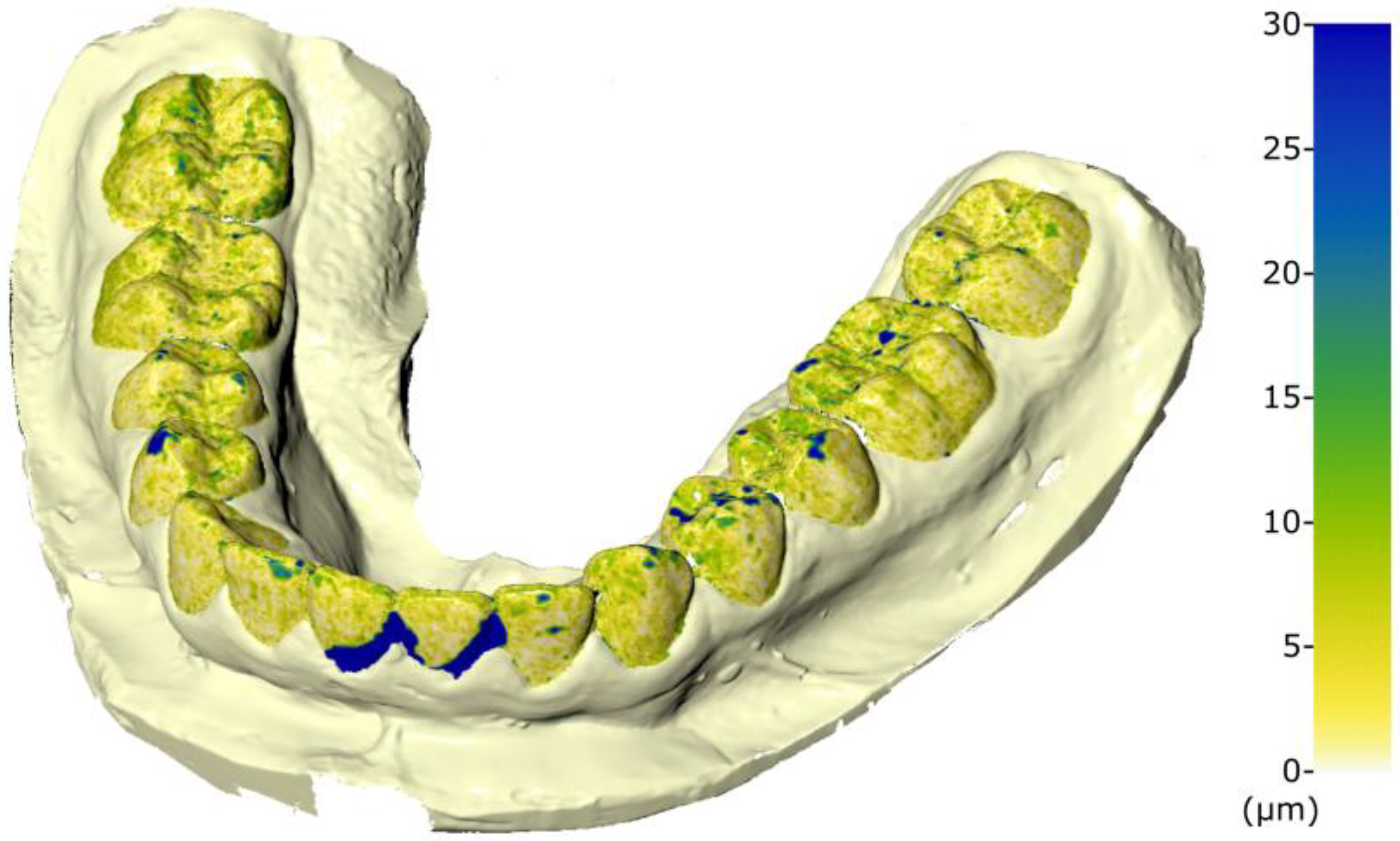
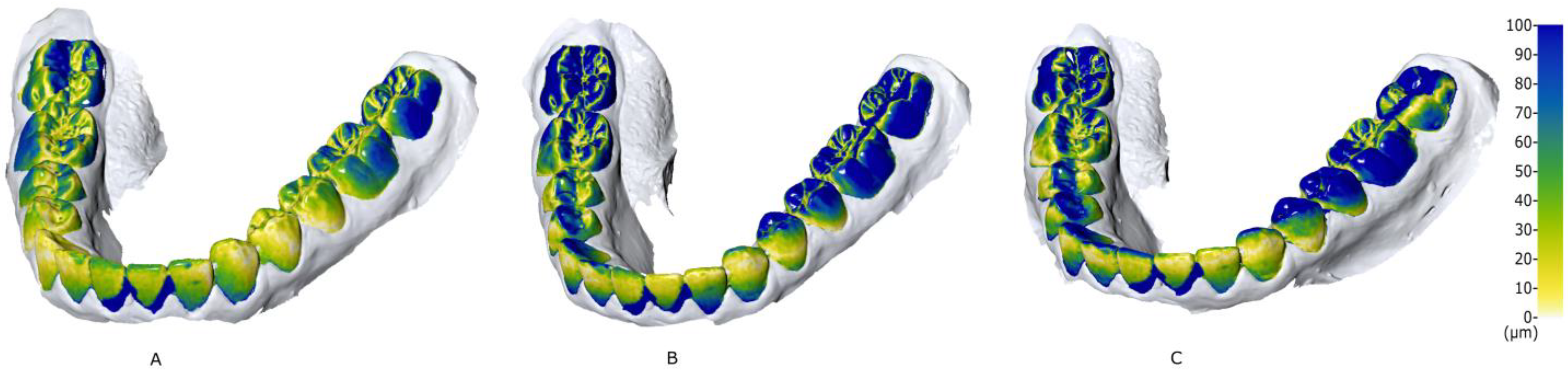
2.3. Mesh Superimposition
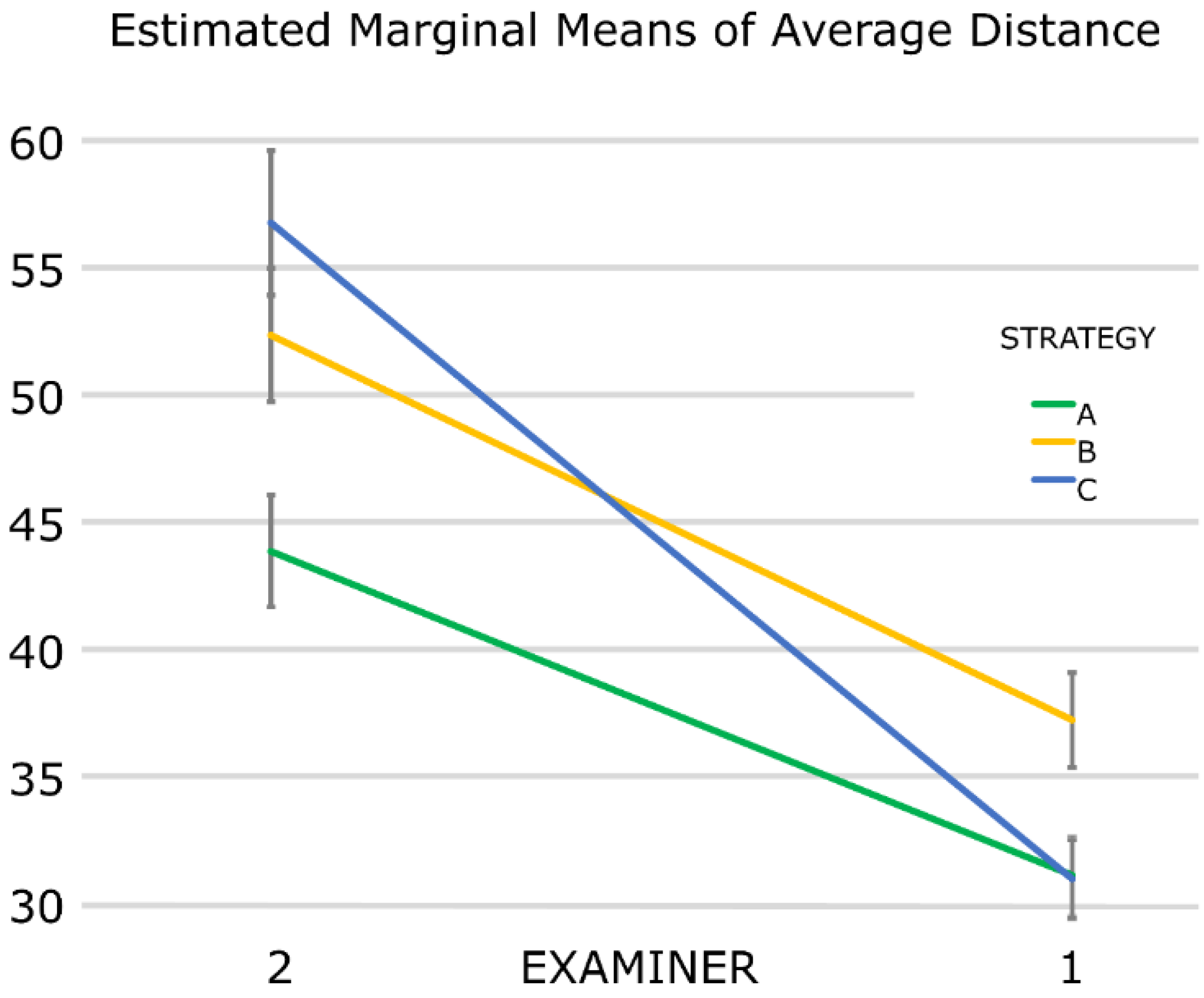
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Afrashtehfar, K.I.; Alnakeb, N.A.; Assery, M.K.M. Accuracy of intraoral scanners versus traditional impressions: A rapid umbrella review. J. Evid. Base Dent. Pract. 2022, 101719. [Google Scholar] [CrossRef]
- Christopoulou, I.; Kaklamanos, E.G.; Makrygiannakis, M.A.; Bitsanis, I.; Perlea, P.; Tsolakis, A.I. Intraoral scanners in Orthodontics: A critical review. Int. J. Environ. Res. Public Health 2022, 19, 1407. [Google Scholar] [CrossRef] [PubMed]
- Goracci, C.; Franchi, L.; Vichi, A.; Ferrari, M. Accuracy, reliability, and efficiency of intraoral scanners for full-arch impressions: A systematic review of the clinical evidence. Eur. J. Orthod. 2016, 38, 422–428. [Google Scholar] [CrossRef]
- Burzynski, J.A.; Firestone, A.R.; Beck, F.M.; Fields, H.W., Jr.; Deguchi, T. Comparison of digital intraoral scanners and alginate impressions: Time and patient satisfaction. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Sfondrini, M.F.; Gandini, P.; Malfatto, M.; Di Corato, F.; Trovati, F.; Scribante, A. Computerized Casts for Orthodontic Purpose Using Powder-Free Intraoral Scanners: Accuracy, Execution Time, and Patient Feedback. Biomed. Res. Int. 2018, 2018, 4103232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, A.; Beretta, M.; Luongo, G.; Mangano, C.; Mangano, F. Conventional Vs Digital Impressions: Acceptability, Treatment Comfort and Stress Among Young Orthodontic Patients. Open Dent. J. 2018, 12, 118–124. [Google Scholar] [CrossRef] [Green Version]
- Mennito, A.S.; Evans, Z.P.; Nash, J.; Bocklet, C.; Lauer, A.; Bacro, T.; Cayouette, M.; Ludlow, M.; Renne, W.G. Evaluation of the trueness and precision of complete arch digital impressions on a human maxilla using seven different intraoral digital impression systems and a laboratory scanner. J. Esthet. Restor. Dent. 2019, 31, 369–377. [Google Scholar] [CrossRef]
- Michelinakis, G.; Apostolakis, D.; Tsagarakis, A.; Kourakis, G.; Pavlakis, E. A comparison of accuracy of 3 intraoral scanners: A single-blinded in vitro study. J. Prosthet. Dent. 2020, 124, 581–588. [Google Scholar] [CrossRef]
- Bohner, L.; Gamba, D.D.; Hanisch, M.; Marcio, B.S.; Neto, P.T.; Laganá, D.C.; Sesma, N. Accuracy of digital technologies for the scanning of facial, skeletal, and intraoral tissues: A systematic review. J. Prosthet. Dent. 2019, 121, 246–251. [Google Scholar] [CrossRef]
- Lee, S.J.; Gallucci, G.O. Digital vs. conventional implant impressions: Efficiency outcomes. Clin. Oral Implant. Res. 2013, 24, 111–115. [Google Scholar] [CrossRef]
- Zimmermann, M.; Mehl, A.; Mörmann, W.H.; Reich, S. Intraoral scanning systems-a current overview. Int. J. Comput. Dent. 2015, 18, 101–129. [Google Scholar] [PubMed]
- Ender, A.; Mehl, A. Influence of scanning strategies on the accuracy of digital intraoral scanning systems. Int. J. Comput. Dent. 2013, 16, 11–21. [Google Scholar] [PubMed]
- Müller, P.; Ender, A.; Joda, T.; Katsoulis, J. Impact of digital intraoral scan strategies on the impression accuracy using the TRIOS Pod scanner. Quintessence Int. 2016, 47, 343–349. [Google Scholar] [PubMed]
- Anh, J.W.; Park, J.M.; Chun, Y.S.; Kim, M.; Kim, M. A comparison of the precision of three-dimensional images acquired by 2 digital intraoral scanners: Effects of tooth irregularity and scanning direction. Korean J. Orthod. 2016, 46, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Oh, K.C.; Park, J.M.; Moon, H.S. Effects of Scanning Strategy and Scanner Type on the Accuracy of Intraoral Scans: A New Approach for Assessing the Accuracy of Scanned Data. J. Prosthodont. 2020, 29, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Medina-Sotomayor, P.; Pascual, M.A.; Camps, A.I. Accuracy of four digital scanners according to scanning strategy in complete-arch impressions. PLoS ONE 2018, 13, e0202916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passos, L.; Meiga, S.; Brigagão, V.; Street, A. Impact of different scanning strategies on the accuracy of two current intraoral scanning systems in complete-arch impressions: An in vitro study. Int. J. Comput. Dent. 2019, 22, 307–319. [Google Scholar]
- Zarone, F.; Ruggiero, G.; Ferrari, M.; Mangano, F.; Joda, T.; Sorrentino, R. Comparison of different intraoral scanning techniques on the completely edentulous maxilla: An in vitro 3-dimensional comparative analysis. J. Prosthet. Dent. 2020, 124, 762.e1–762.e8. [Google Scholar] [CrossRef]
- Flügge, T.V.; Schlager, S.; Nelson, K.; Nahles, S.; Metzger, M.C. Precision of intraoral digital dental impressions with iTero and extraoral digitization with the iTero and a model scanner. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 471–478. [Google Scholar] [CrossRef]
- Richert, R.; Goujat, A.; Venet, L.; Viguie, G.; Viennot, S.; Robinson, P.; Farges, J.C.; Fages, M.; Ducret, M. Intraoral Scanner Technologies: A Review to Make a Successful Impression. J. Healthc. Eng. 2017, 2017, 8427595. [Google Scholar] [CrossRef]
- Haddadi, Y.; Bahrami, G.; Isidor, F. Effect of Software Version on the Accuracy of an Intraoral Scanning Device. Int. J. Prosthodont. 2018, 31, 375–376. [Google Scholar] [CrossRef] [PubMed]
- ISO 5725-1:1994; Accuracy (Trueness and Precision) of Measurement Methods and Results—Part 1: General Principles and Definitions. International Organization for Standardization: Geneva, Switzerland, 1994.
- Patzelt, S.B.; Vonau, S.; Stampf, S.; Att, W. Assessing the feasibility and accuracy of digitizing edentulous jaws. J. Am. Dent. Assoc. 2013, 144, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Arakida, T.; Kanazawa, M.; Iwaki, M.; Suzuki, T.; Minakuchi, S. Evaluating the influence of ambient light on scanning trueness, precision, and time of intra oral scanner. J. Prosthodont. Res. 2018, 62, 324–329. [Google Scholar] [CrossRef]
- Liczmanski, K.; Stamm, T.; Sauerland, C.; Blanck-Lubarsch, M. Accuracy of intraoral scans in the mixed dentition: A prospective non-randomized comparative clinical trial. Head Face Med. 2020, 16, 11. [Google Scholar] [CrossRef] [PubMed]
- Wiranto, M.G.; Engelbrecht, W.P.; Tutein Nolthenius, H.E.; van der Meer, W.J.; Ren, Y. Validity, reliability, and reproducibility of linear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressions. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 140–147. [Google Scholar] [CrossRef]
- Park, J.M.; Choi, S.A.; Myung, J.Y.; Chun, Y.S.; Kim, M. Impact of Orthodontic Brackets on the Intraoral Scan Data Accuracy. Biomed. Res. Int. 2016, 2016, 5075182. [Google Scholar] [CrossRef]
- Dutton, E.; Ludlow, M.; Mennito, A.; Kelly, A.; Evans, Z.; Culp, A.; Kessler, R.; Renne, W. The effect different substrates have on the trueness and precision of eight different intraoral scanners. J. Esthet. Restor. Dent. 2020, 32, 204–218. [Google Scholar] [CrossRef]
- Li, H.; Lyu, P.; Wang, Y.; Sun, Y. Influence of object translucency on the scanning accuracy of a powder-free intraoral scanner: A laboratory study. J. Prosthet. Dent. 2017, 117, 93–101. [Google Scholar] [CrossRef]
- Waldecker, M.; Rues, S.; Trebing, C.; Behnisch, R.; Rammelsberg, P.; Bömicke, W. Effects of Training on the Execution of Complete-Arch Scans. Part 2: Scanning Accuracy. Int. J. Prosthodont. 2021, 34, 27–36. [Google Scholar] [CrossRef]
- Resende, C.C.D.; Barbosa, T.A.Q.; Moura, G.F.; Tavares, L.D.N.; Rizzante, F.A.P.; George, F.M.; Neves, F.D.D.; Mendonça, G. Influence of operator experience, scanner type, and scan size on 3D scans. J. Prosthet. Dent. 2021, 125, 294–299. [Google Scholar] [CrossRef]
- Motel, C.; Kirchner, E.; Adler, W.; Wichmann, M.; Matta, R.E. Impact of Different Scan Bodies and Scan Strategies on the Accuracy of Digital Implant Impressions Assessed with an Intraoral Scanner: An In Vitro Study. J. Prosthodont. 2020, 29, 309–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ender, A.; Zimmermann, M.; Mehl, A. Accuracy of complete- and partial-arch impressions of actual intraoral scanning systems in vitro. Int. J. Comput. Dent. 2019, 22, 11–19. [Google Scholar] [PubMed]
- Lee, J.H.; Yun, J.H.; Han, J.S.; Yeo, I.L.; Yoon, H.I. Repeatability of Intraoral Scanners for Complete Arch Scan of Partially Edentulous Dentitions: An In Vitro Study. J. Clin. Med. 2019, 8, 1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naidu, D.; Freer, T.J. Validity, reliability, and reproducibility of the iOC intraoral scanner: A comparison of tooth widths and Bolton ratios. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 304–310. [Google Scholar] [CrossRef] [PubMed]
- San José, V.; Bellot-Arcís, C.; Tarazona, B.; Zamora, N.; Lagravère, M.O.; Paredes-Gallardo, V. Dental measurements and Bolton index reliability and accuracy obtained from 2D digital, 3D segmented CBCT, and 3d intraoral laser scanner. J. Clin. Exp. Dent. 2017, 9, e1466–e1473. [Google Scholar] [CrossRef]
- Aragón, M.L.; Pontes, L.F.; Bichara, L.M.; Flores-Mir, C.; Normando, D. Validity and reliability of intraoral scanners compared to conventional gypsum models measurements: A systematic review. Eur. J. Orthod. 2016, 38, 429–434. [Google Scholar] [CrossRef]
- Suryajaya, W.; Purbiati, M.; Ismah, N. Accuracy of digital dental models and three-dimensional printed dental models in linear measurements and Bolton analysis. F1000Research 2021, 10, 180. [Google Scholar] [CrossRef]
- De Felice, M.E.; Nucci, L.; Fiori, A.; Flores-Mir, C.; Perillo, L.; Grassia, V. Accuracy of interproximal enamel reduction during clear aligner treatment. Prog. Orthod. 2020, 21, 28. [Google Scholar] [CrossRef]
- Botsford, K.P.; Frazier, M.C.; Ghoneima, A.A.M.; Utreja, A.; Bhamidipalli, S.S.; Stewart, K.T. Precision of the virtual occlusal record. Angle Orthod. 2019, 89, 751–757. [Google Scholar] [CrossRef] [Green Version]
- Gintaute, A.; Keeling, A.J.; Osnes, C.A.; Zitzmann, N.U.; Ferrari, M.; Joda, T. Precision of maxillo-mandibular registration with intraoral scanners in vitro. J. Prosthodont. Res. 2020, 64, 114–119. [Google Scholar] [CrossRef]
- Owens, S.; Buschang, P.H.; Throckmorton, G.S.; Palmer, L.; English, J. Masticatory performance and areas of occlusal contact and near contact in subjects with normal occlusion and malocclusion. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Svanborg, P. A systematic review on the accuracy of zirconia crowns and fixed dental prostheses. Biomater. Investig. Dent. 2020, 7, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keating, A.P.; Knox, J.; Bibb, R.; Zhurov, A.I. A comparison of plaster, digital and reconstructed study model accuracy. J. Orthod. 2008, 35, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Hazeveld, A.; Huddleston Slater, J.J.; Ren, Y. Accuracy and reproducibility of dental replica models reconstructed by different rapid prototyping techniques. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 108–115. [Google Scholar] [CrossRef]
- Sweeney, S.; Smith, D.K.; Messersmith, M. Comparison of 5 types of interocclusal recording materials on the accuracy of articulation of digital models. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 245–252. [Google Scholar] [CrossRef]
- Cole, D.; Bencharit, S.; Carrico, C.K.; Arias, A.; Tüfekçi, E. Evaluation of fit for 3D-printed retainers compared with thermoform retainers. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 592–599. [Google Scholar] [CrossRef] [Green Version]
- Bakdach, W.M.M.; Hadad, R. Linear and angular transfer accuracy of labial brackets using three dimensional-printed indirect bonding trays: A systematic review and meta-analysis. Int. Orthod. 2022, 20, 100612. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mesh | Mean (±SD) | Median |
|---|---|---|
| 1 | 5.1 (±16.8) | 2.8 |
| 2 | 10.0 (±31.4) | 4.7 |
| 3 | 6.6 (±33.5) | 3.3 |
| 4 | 7.5 (±28.6) | 3.7 |
| 5 | 9.6 (±37.7) | 4.0 |
| Strategy A | Strategy B | Strategy C | ||||
|---|---|---|---|---|---|---|
| Examiner 1 | Examiner 2 | Examiner 1 | Examiner 2 | Examiner 1 | Examiner 2 | |
| Session 1 | 26.8 (±6.5) | 39.6 (±14.3) | 29.3 (±6.1) | 47.2 (±15.7) | 27.4 (±8.6) | 48.4 (±17.5) |
| Session 2 | 35.5 (±7.6) | 48.1 (±10.2) | 45.1 (±12.1) | 57.5 (±19.8) | 34.5 (±12.5) | 65.1 (±16.3) |
| Overall | 37.5 (±12.5) | 44.8 (±17.3) | 43.9 (±20.0) | |||
| Parameter | Coefficient Estimate | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Intercept | 36.5 | 31.5 to 41.6 | 0.000 |
| Examiner 2 | 25.8 | 19.2 to 32.4 | 0.000 |
| Strategy A | 0.1 | −6.5 to 6.8 | 0.965 |
| Strategy B | 6.3 | −0.4 to 12.9 | 0.063 |
| Session 1 | −11.2 | −15.0 to −7.4 | 0.000 |
| Examiner 2 × strategy A | −13.0 | −22.4 to −3.7 | 0.006 |
| Examiner 2 × strategy B | −10.7 | −20.0 to −1.3 | 0.026 |
| Source | Type III Sum of Squares | df | Mean Square | F | p-Value |
|---|---|---|---|---|---|
| Corrected Model | 23,355.3 | 6 | 3892.6 | 23.2 | 0.000 |
| Intercept | 318,109.7 | 1 | 318,109.7 | 1893.3 | 0.000 |
| Examiner | 14,398.6 | 1 | 14,398.6 | 85.7 | 0.000 |
| Strategy | 1896.7 | 2 | 948.4 | 5.6 | 0.004 |
| Session | 5611.2 | 1 | 5611.2 | 33.4 | 0.000 |
| Examiner × strategy | 1448.8 | 2 | 724.4 | 4.3 | 0.015 |
| Strategy A | Strategy B | Strategy C | ||||
|---|---|---|---|---|---|---|
| Examiner 1 | Examiner 2 | Examiner 1 | Examiner 2 | Examiner 1 | Examiner 2 | |
| Mean of SDs | 2.9 (±2.5) | 2.4 (±2.3) | 5.4 (±2.2) | 4.0 (±3.5) | 4.0 (±2.6) | 2.7 (±2.7) |
| Overall | 2.7 (±2.4) | 4.7 (±3.0) | 3.4 (±2.7) | |||
| Strategy A | Strategy B | Strategy C | ||||
|---|---|---|---|---|---|---|
| Examiner 1 | Examiner 2 | Examiner 1 | Examiner 2 | Examiner 1 | Examiner 2 | |
| Session 1 | 93 (±16) | 53 (±5) | 84 (±14) | 51 (±5) | 80 (±12) | 49 (±6) |
| Session 2 | 48 (±7) | 52 (±6) | 47 (±6) | 47 (±4) | 42 (±8) | 46 (±6) |
| Overall | 62 (±21) | 57 (±18) | 54 (±17) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gavounelis, N.A.; Gogola, C.-M.C.; Halazonetis, D.J. The Effect of Scanning Strategy on Intraoral Scanner’s Accuracy. Dent. J. 2022, 10, 123. https://doi.org/10.3390/dj10070123
Gavounelis NA, Gogola C-MC, Halazonetis DJ. The Effect of Scanning Strategy on Intraoral Scanner’s Accuracy. Dentistry Journal. 2022; 10(7):123. https://doi.org/10.3390/dj10070123
Chicago/Turabian StyleGavounelis, Nikolaos A., Chrysoula-Maria C. Gogola, and Demetrios J. Halazonetis. 2022. "The Effect of Scanning Strategy on Intraoral Scanner’s Accuracy" Dentistry Journal 10, no. 7: 123. https://doi.org/10.3390/dj10070123
APA StyleGavounelis, N. A., Gogola, C. -M. C., & Halazonetis, D. J. (2022). The Effect of Scanning Strategy on Intraoral Scanner’s Accuracy. Dentistry Journal, 10(7), 123. https://doi.org/10.3390/dj10070123