Medication-Related Osteonecrosis of the Jaws Initiated by Zoledronic Acid and Potential Pathophysiology

Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Eligibility Criteria
- (1)
- In vitro studies.
- (2)
- Publications in the English language.
- (3)
- Only human cells.
- (4)
- MRONJ pathophysiology must be the aim of the study.
- (5)
- Associations to MRONJ must be made in the discussion.
- (1)
- Osteonecrosis of the jaw not related to medication.
- (2)
- Osteonecrosis in other body parts.
- (3)
- Studies including bisphosphonates other than zoledronic acid.
- (4)
- Zoledronic acid in combination with other medications.
- (5)
- Systematic reviews, etiological studies, case series and reports, consensus reports, letters, editorials, doctoral theses, pilot studies and only abstracts.
- (6)
- Studies investigating possible risk factors (i.e., different diseases).
- (7)
- Comparative studies between different kinds of bisphosphonates.
2.2. Information Sources and Search
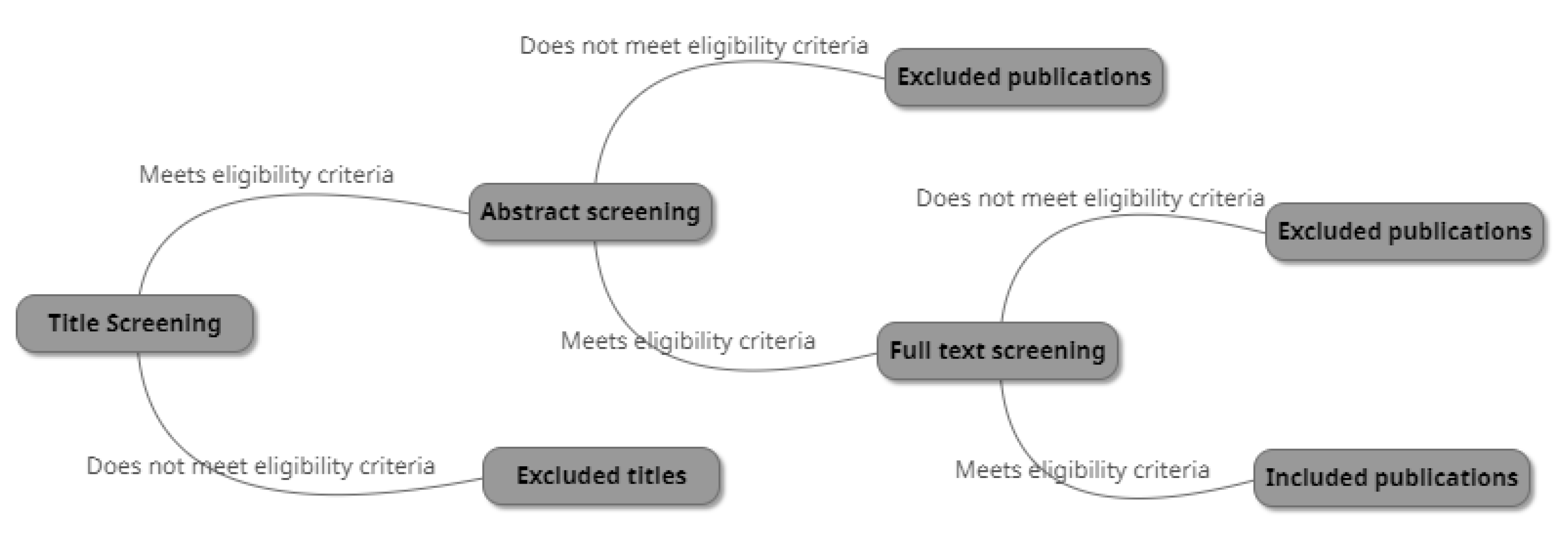
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Strategy for Data Synthesis
3. Results
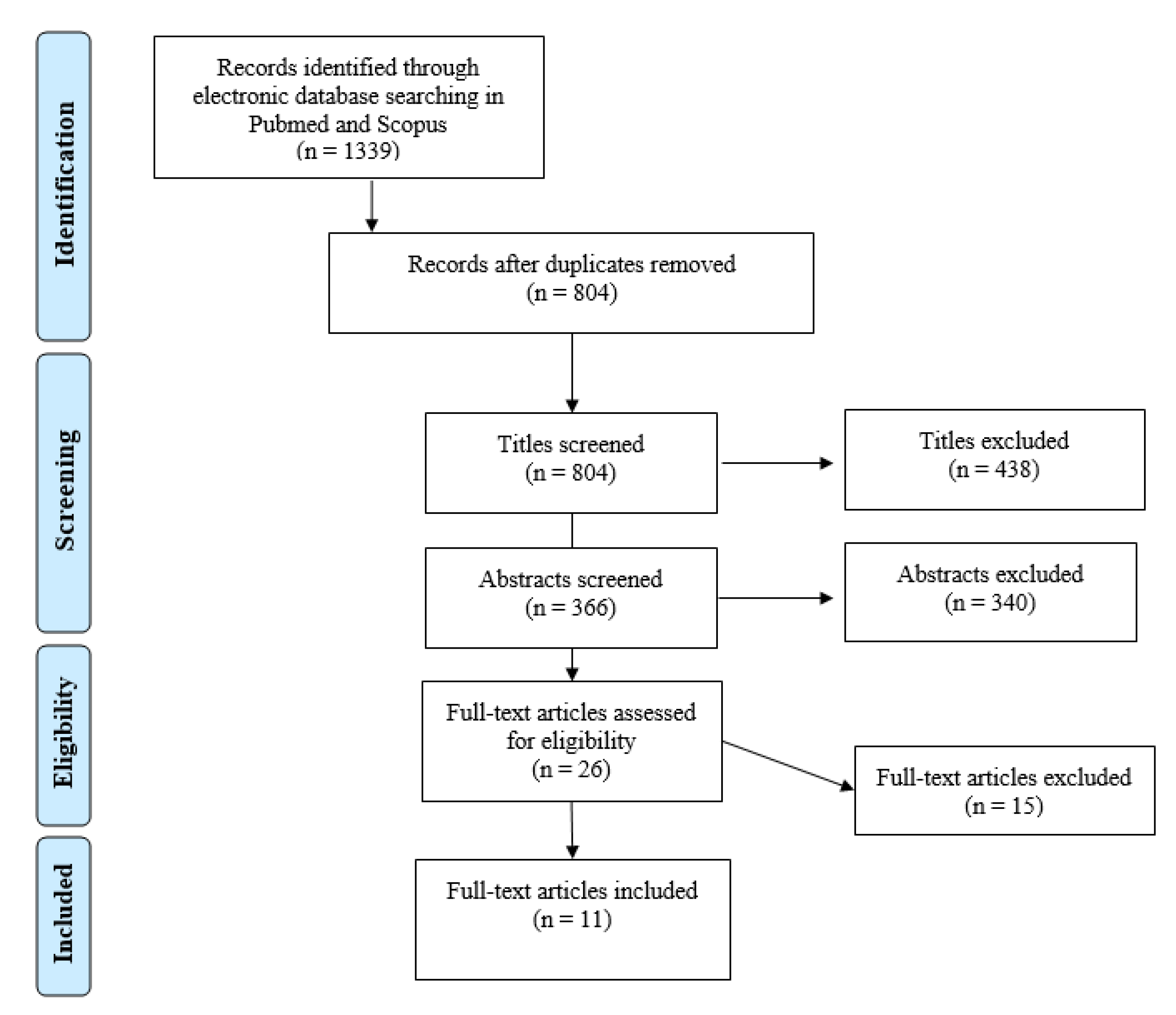
3.1. Study Selection
3.2. ZA Application Methods
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marx, R.E. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: A growing epidemic. J. Oral Maxillofac. Surg. 2003, 61, 1115–1117. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons Position Paper on Medication-Related Osteonecrosis of the Jaw—2014 Update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef]
- King, R.; Tanna, N.; Patel, V. Medication-related osteonecrosis of the jaw unrelated to bisphosphonates and denosumab—A review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Bennardo, F.; Buffone, C.; Giudice, A. New therapeutic opportunities for COVID-19 patients with Tocilizumab: Possible correlation of interleukin-6 receptor inhibitors with osteonecrosis of the jaws. Oral Oncol. 2020, 106, 104659. [Google Scholar] [CrossRef]
- Schiodt, M.; Otto, S.; Fedele, S.; Bedogni, A.; Nicolatou-Galitis, O.; Guggenberger, R.; Brokstad Herlofson, B.; Ristow, O.; Kofod, T. Workshop of European task force on medication-related osteonecrosis of the jaw—Current challenges. Oral Dis. 2019, 25, 1815–1821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallmer, F.; Andersson, G.; Götrick, B.; Warfvinge, G.; Anderud, J.; Bjørnland, T. Prevalence, initiating factor, and treatment outcome of medication-related osteonecrosis of the jaw-a 4-year prospective study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 477–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dodson, T.B. The Frequency of Medication-related Osteonecrosis of the Jaw and its Associated Risk Factors. Oral Maxillofac. Surg. Clin. N. Am. 2015, 27, 509–516. [Google Scholar] [CrossRef]
- Hallmer, F.; Bjørnland, T.; Nicklasson, A.; Becktor, J.P.; Andersson, G. Osteonecrosis of the jaw in patients treated with oral and intravenous bisphosphonates: Experience in Sweden. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 202–208. [Google Scholar] [CrossRef]
- McGowan, K.; McGowan, T.; Ivanovski, S. Risk factors for medication-related osteonecrosis of the jaws: A systematic review. Oral Dis. 2018, 24, 527–536. [Google Scholar] [CrossRef]
- Domah, F.; Shah, N.; Domah, J.; Shah, R. Medication-related osteonecrosis of the jaw—A current review. Oral Surg. 2018, 11, 250–258. [Google Scholar] [CrossRef]
- Fleisch, H.; Graham, R.; Russell, G.; Francis, M.D. Diphosphonates inhibit hydroxyapatite dissolution in vitro and bone resorption in tissue culture and in vivo. Science 1969, 165, 1262–1264. [Google Scholar] [CrossRef]
- Nanci, A. Ten Cate’s Oral Histology: Development, Structure, and Function, 9th ed.; Elsevier: St. Louis, MO, USA, 2018. [Google Scholar]
- Anderson, H.C. Matrix vesicles and calcification. Curr. Rheumatol. Rep. 2003, 5, 222–226. [Google Scholar] [CrossRef]
- Russell, R.G.G.; Watts, N.B.; Ebetino, F.H.; Rogers, M.J. Mechanisms of action of bisphosphonates: Similarities and differences and their potential influence on clinical efficacy. Osteoporos. Int. 2008, 19, 733–759. [Google Scholar] [CrossRef]
- Khan, A.A.; Morrison, A.; Hanley, D.A.; Felsenberg, D.; McCauley, L.K.; O’Ryan, F.; Reid, I.R.; Ruggiero, S.L.; Taguchi, A.; Tetradis, S.; et al. Diagnosis and Management of Osteonecrosis of the Jaw: A Systematic Review and International Consensus. J. Bone Miner. Res. 2015, 30, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Fung, P.; Bedogni, G.; Bedogni, A.; Petrie, A.; Porter, S.; Campisi, G.; Bagan, J.; Fusco, V.; Saia, G.; Acham, S.; et al. Time to onset of bisphosphonate-related osteonecrosis of the jaws: A multicentre retrospective cohort study. Oral Dis. 2017, 23, 477–483. [Google Scholar] [CrossRef] [PubMed]
- PRISMA Guidelines. Available online: http://prisma-statement.org/prismastatement/Checklist.aspx (accessed on 19 March 2019).
- Rayyan QCRI. Available online: https://rayyan.qcri.org/welcome (accessed on 3 June 2019).
- ToxRtool. Available online: https://ec.europa.eu/jrc/en/scientific-tool/toxrtool-toxicological-data-reliability-assessment-tool (accessed on 8 July 2019).
- Scheper, M.; Chaisuparat, R.; Cullen, K.; Meiller, T. A novel soft-tissue in vitro model for bisphosphonate-associated osteonecrosis. Fibrogenesis Tissue Repair 2010, 3, 6. [Google Scholar] [CrossRef] [Green Version]
- Ravosa, M.J.; Ning, J.; Liu, Y.; Stack, M.S. Bisphosphonate effects on the behaviour of oral epithelial cells and oral fibroblasts. Arch. Oral Biol. 2011, 56, 491–498. [Google Scholar] [CrossRef]
- Scheper, M.A.; Badros, A.; Chaisuparat, R.; Cullen, K.J.; Meiller, T.F. Effect of zoledronic acid on oral fibroblasts and epithelial cells: A potential mechanism of bisphosphonate-associated osteonecrosis. Br. J. Haematol. 2009, 144, 667–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Q.; Liu, J.; Guo, T.; Liu, D.; Pan, J. Epidermal Growth Factor Reverses the Inhibitory Effects of the Bisphosphonate, Zoledronic Acid, on Human Oral Keratinocytes and Human Vascular Endothelial Cells In Vitro via the Epidermal Growth Factor Receptor (EGFR)/Akt/Phosphoinositide 3-Kinase (PI3K). Med. Sci. Monit. 2019, 25, 700–710. [Google Scholar] [CrossRef] [PubMed]
- Saracino, S.; Canuto, R.A.; Maggiora, M.; Oraldi, M.; Scoletta, M.; Ciuffreda, L.; Vandone, A.M.; Carossa, S.; Mozzati, M.; Muzio, G. Exposing human epithelial cells to zoledronic acid can mediate osteonecrosis of jaw: An in vitro model. J. Oral Pathol. Med. 2012, 41, 788–792. [Google Scholar] [CrossRef] [PubMed]
- Pourgonabadi, S.; Mousavi, S.H.; Tayarani-Najaran, Z.; Ghorbani, A. Effect of zoledronate, a third-generation bisphosphonate, on proliferation and apoptosis of human dental pulp stem cells. Can. J. Physiol. Pharmacol. 2018, 96, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Anitua, E.; Zalduendo, M.; Troya, M.; Orive, G. PRGF exerts a cytoprotective role in zoledronic acid-treated oral cells. Clin. Oral Investig. 2016, 20, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, Y.; Ibi, M.; Chosa, N.; Kyakumoto, S.; Kamo, M.; Shibata, T.; Sugiyama, Y.; Ishisaki, A. Zoledronic acid suppresses transforming growth factor-β-induced fibrogenesis by human gingival fibroblasts. Int. J. Mol. Med. 2016, 38, 139–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, M.; Zhou, Z.; Shi, L.; Niu, J.; Xu, S.; Lin, W.; Chen, Z.; Wang, Y. Influence of zoledronic acid on proliferation, migration, and apoptosis of vascular endothelial cells. Br. J. Oral Maxillofac. Surg. 2016, 54, 889–893. [Google Scholar] [CrossRef]
- Lu, Y.; Wang, Z.; Han, W.; Li, H. Zoledronate induces autophagic cell death in human umbilical vein endothelial cells via Beclin-1 dependent pathway activation. Mol. Med. Rep. 2016, 14, 4747–4754. [Google Scholar] [CrossRef] [PubMed]
- Thibaut, F.; Watrin, T.; Meary, F.; Tricot, S.; Legros, V.; Pellen-Mussi, P.; Chauvel-Lebret, D. Effects of zoledronic acid on osteoblasts in three-dimensional culture. J. Dent. Sci. 2015, 10, 8–15. [Google Scholar] [CrossRef]
- Ziebart, T.; Pabst, A.; Klein, M.O.; Kämmerer, P.; Gauss, L.; Brüllmann, D.; Al-Nawas, B.; Walter, C. Bisphosphonates: Restrictions for vasculogenesis and angiogenesis: Inhibition of cell function of endothelial progenitor cells and mature endothelial cells in vitro. Clin. Oral Investig. 2011, 15, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, A.C.D.O.; Andrade, Z.D.A.; Costa, T.F.; Medrado, A.R.A.P. Wound healing—A literature review. An. Bras. Dermatol. Soc. Bras. Dermatol. 2016, 91, 614–620. [Google Scholar] [CrossRef] [Green Version]
- Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound repair and regeneration. Nature 2008, 453, 314–321. [Google Scholar] [CrossRef]
- Walter, C.; Pabst, A.; Ziebart, T.; Klein, M.; Al-Nawas, B. Bisphosphonates affect migration ability and cell viability of HUVEC, fibroblasts and osteoblasts in vitro. Oral Dis. 2011, 17, 194–199. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Gaynor, R.B. IκB kinases: Key regulators of the NF-κB pathway. Trends Biochem. Sci. 2004, 29, 72–79. [Google Scholar] [CrossRef]
- Novince, C.M.; Ward, B.B.; McCauley, L.K. Osteonecrosis of the jaw: An update and review of recommendations. Cells Tissues Organs 2008, 189, 275–283. [Google Scholar] [CrossRef]
- Sedghizadeh, P.P.; Kumar, S.K.S.; Gorur, A.; Schaudinn, C.; Shuler, C.F.; Costerton, J.W. Identification of microbial biofilms in osteonecrosis of the jaws secondary to bisphosphonate therapy. J. Oral Maxillofac. Surg. 2008, 66, 767–775. [Google Scholar] [CrossRef]
- Chang, J.; Hakam, A.E.; McCauley, L.K. Current Understanding of the Pathophysiology of Osteonecrosis of the Jaw. Curr. Osteoporos. Rep. 2018, 16, 584–595. [Google Scholar] [CrossRef] [PubMed]
- Sandbo, N.; Dulin, N. Actin cytoskeleton in myofibroblast differentiation: Ultrastructure defining form and driving function. Transl. Res. 2011, 158, 181–196. [Google Scholar] [CrossRef] [Green Version]
- Ledesma-Martínez, E.; Mendoza-Núñez, V.M.; Santiago-Osorio, E. Mesenchymal stem cells derived from dental pulp: A review. Stem Cells Int. 2016, 2016, 4709572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marx, R.E.; Sawatari, Y.; Fortin, M.; Broumand, V. Bisphosphonate-Induced Exposed Bone (Osteonecrosis/Osteopetrosis) of the Jaws: Risk Factors, Recognition, Prevention, and Treatment. J. Oral Maxillofac. Surg. 2005, 63, 1567–1575. [Google Scholar] [CrossRef]
- Chen, T.; Berenson, J.; Vescio, R.; Swift, R.; Gilchick, A.; Goodin, S.; Goodin, S.; LoRusso, P.; Ma, P.; Ravera, C.; et al. Pharmacokinetics and pharmacodynamics of zoledronic acid in cancer patients with bone metastases. J. Clin. Pharmacol. 2002, 42, 1228–1236. [Google Scholar] [CrossRef] [PubMed]
- Green, J.; Clézardin, P. The molecular basis of bisphosphonate activity: A preclinical perspective. Semin. Oncol. 2010, 37, S3–S11. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Article (A) | A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | Overall Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A1 Scheper et al., 2010 [20]. | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 12 |
| A2 Ravosa et al., 2016 [21]. | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 13 |
| A3 Pourgonabadi et al., 2017 [25]. | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 11 |
| A4 Scheper et al., 2009 [22]. | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 12 |
| A5 Thibaut et al., 2014 [30]. | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 12 |
| A6 Wang et al., 2019 [23]. | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 11 |
| A7 Saracino et al., 2012 [24]. | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 10 |
| A8 Lang et al., 2016 [28]. | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 11 |
| A9 Anitua et al., 2016 [26]. | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 14 |
| A10 Lu et al., 2016 [29]. | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 12 |
| A11 Komatsu et al., 2016 [27]. | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 10 |
| Article (A) | ZA-Concentration (µM) | Cell Type | Results |
|---|---|---|---|
| A1 | 0.5, 1, 3, 5, 10 | Human gingival fibroblasts |
|
| Human Keratinocytes |
| ||
| A2 | 5, 10, 30, 50, 75, 100, 300 | Human oral Fibroblasts |
|
| Human oral epithelial cells |
| ||
| A3 | 0.2, 0.4, 0.8 1.5, 3, 6, 12, 25, 50, 100 | Dental pulp stem cells (DPSCs) |
|
| Human gingival fibroblasts |
| ||
| A4 | 0.25, 0.5, 1, 3 | Human gingival fibroblasts |
|
| Human keratinocytes |
| ||
| A5 | 0.1, 10 | Human foetal osteoblasts (hFOB) |
|
| A6 | 5, 50, 100 | Human umbilical vein endothelial cells |
|
| Human oral keratinocytes |
| ||
| A7 | 5, 50 µM 5, 50 CM | Human keratinocytes |
|
| Human osteoblast-like cells |
| ||
| A8 | 0.23, 0.69 2.06, 6.17, 15, 18.52, 50, 55.56, 150, 166.67, 500 | Human umbilical vein endothelial cells |
|
| A9 | 0.1, 1, 2, 3, 4, 5, 10 | Human gingival fibroblasts |
|
| 0.1, 1, 5, 10, 12.5, 15, 17.5, 50 | Human alveolar osteoblasts |
| |
| A10 | 25, 50, 75, 100 | Human umbilical vein endothelial cells |
|
| A11 | 0.147, 1.47, 14.7, 147 | Human gingival fibroblasts |
|
| Cell Type | Article (A) | Apoptosis | Proliferation | Viability | Migration |
|---|---|---|---|---|---|
| Epithelial cells | A1 | + | - | x | x |
| A2 | + | - | - | (+) * | |
| A4 | + | - | - | - | |
| A6 | + | x | - | - | |
| A7 | + | - | x | x | |
| Fibroblasts | A1 | + | x | x | x |
| A2 | + | - | - | - | |
| A3 | x | - | x | x | |
| A4 | + | - | x | x | |
| A9 | + | x | - | x | |
| A11 | x | x | - | x | |
| Osteoblasts | A5 | x | - | +/- | x |
| A7 | x | - | ns | x | |
| A9 | + | x | x | x | |
| Endothelial cells | A6 | + | x | - | - |
| A8 | + | x | - | - | |
| A10 | + | x | - | x | |
| Dental pulp stem cells | A3 | + | - | - | x |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsalih, A.; Dam, A.; Lindberg, P.; Truedsson, A. Medication-Related Osteonecrosis of the Jaws Initiated by Zoledronic Acid and Potential Pathophysiology. Dent. J. 2021, 9, 85. https://doi.org/10.3390/dj9080085
Alsalih A, Dam A, Lindberg P, Truedsson A. Medication-Related Osteonecrosis of the Jaws Initiated by Zoledronic Acid and Potential Pathophysiology. Dentistry Journal. 2021; 9(8):85. https://doi.org/10.3390/dj9080085
Chicago/Turabian StyleAlsalih, Aya, Annica Dam, Pia Lindberg, and Anna Truedsson. 2021. "Medication-Related Osteonecrosis of the Jaws Initiated by Zoledronic Acid and Potential Pathophysiology" Dentistry Journal 9, no. 8: 85. https://doi.org/10.3390/dj9080085
APA StyleAlsalih, A., Dam, A., Lindberg, P., & Truedsson, A. (2021). Medication-Related Osteonecrosis of the Jaws Initiated by Zoledronic Acid and Potential Pathophysiology. Dentistry Journal, 9(8), 85. https://doi.org/10.3390/dj9080085