
Muscular and Kinematic Responses to Unexpected Translational Balance Perturbation: A Pilot Study in Healthy Young Adults


 , , , ,
, , , ,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
- No high-intensity sports within 24 h before the experiment;
- No known neurological or musculoskeletal deficits;
- No history of balance disorders, walking disorders, or dizziness;
- No history of lower-limb injuries within a week;
- No sight or hearing disorders;
- No medication intake that could affect muscle activities.
2.2. Equipment
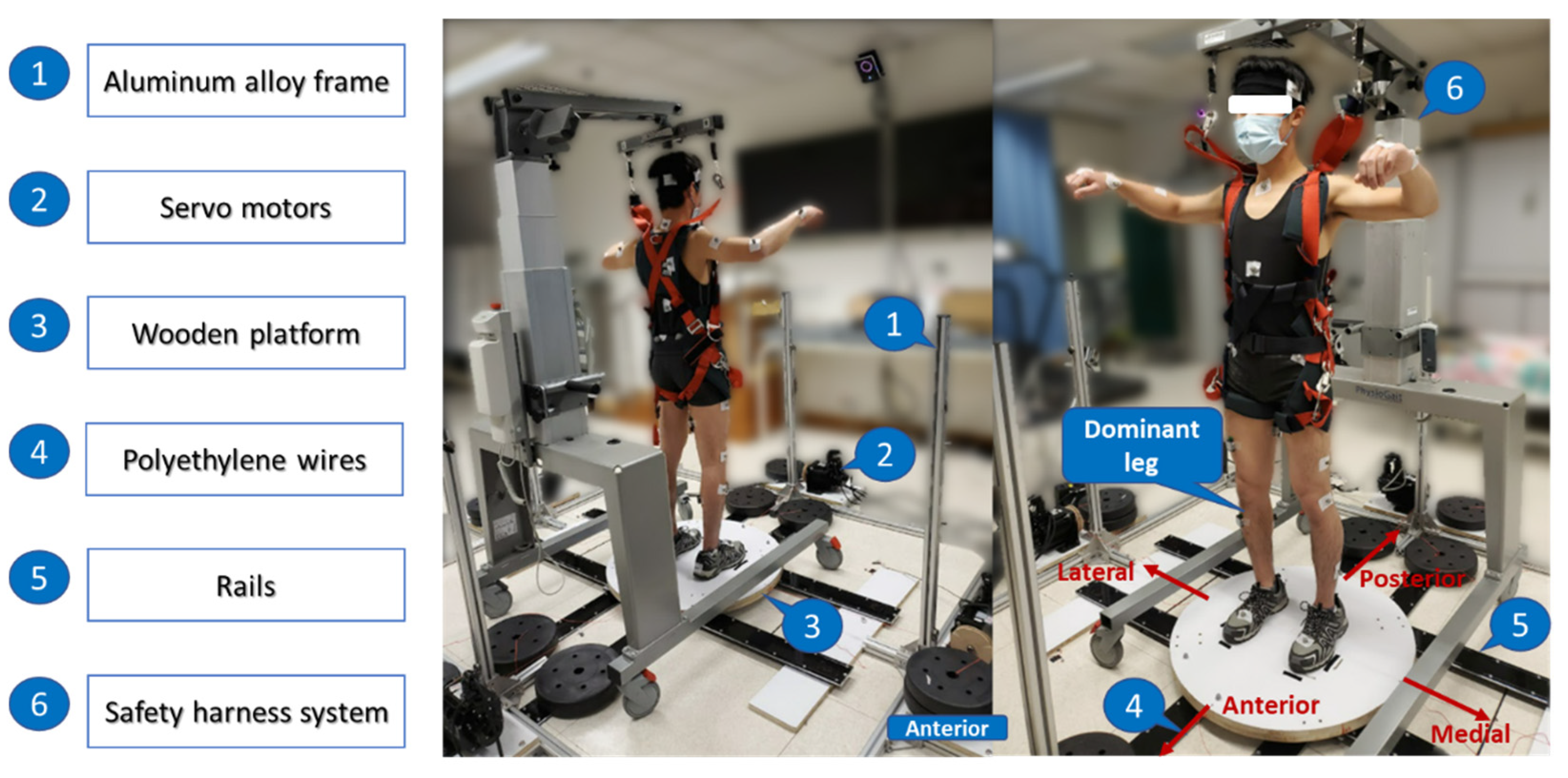
2.2.1. Moving-Platform Perturbation System
2.2.2. Data Sampling Equipment
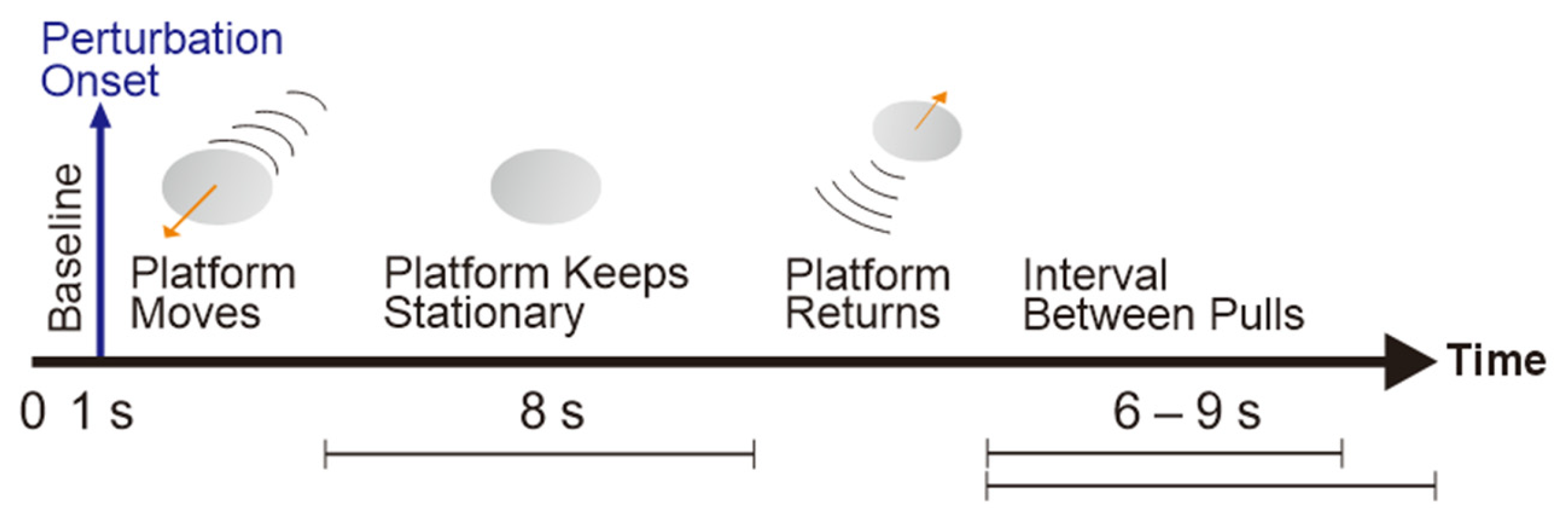
2.3. Protocol
2.3.1. Subjective Assessment
2.3.2. Instrumented Data Collection
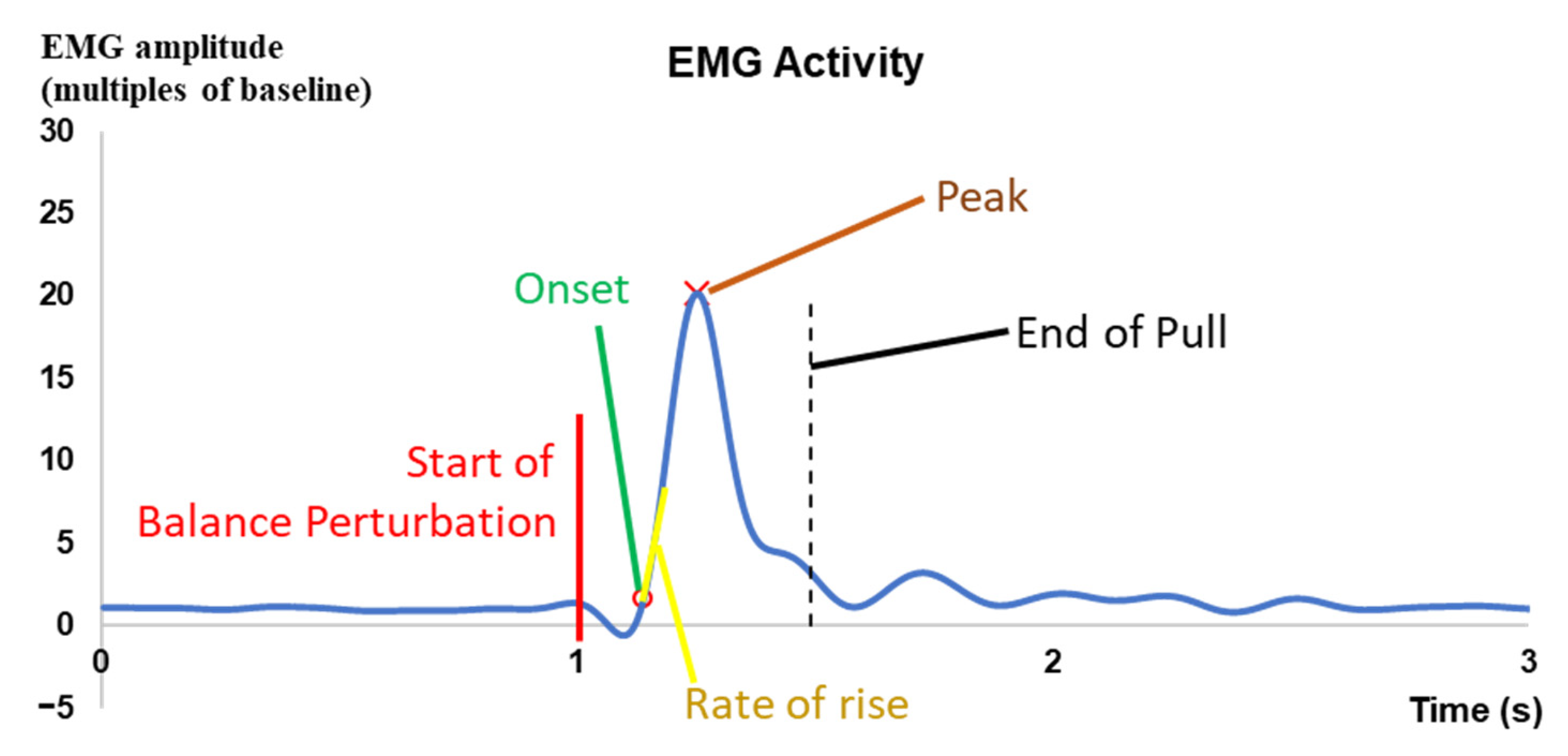
2.4. Data Processing
2.5. Statistical Analyses
- EMG signal difference among the eight different muscles and among the four different perturbation intensities (muscle × perturbation intensity);
- MMG signal difference among the eight different muscles and among the four different perturbation intensities (muscle × perturbation intensity);
- Joint angle difference among the eight different joint motions and among the four different perturbation intensities (joint motion × perturbation intensity);
- COM trajectory difference among the six different postural sway directions and among the four different perturbation intensities (postural sway direction × perturbation intensity).
3. Results
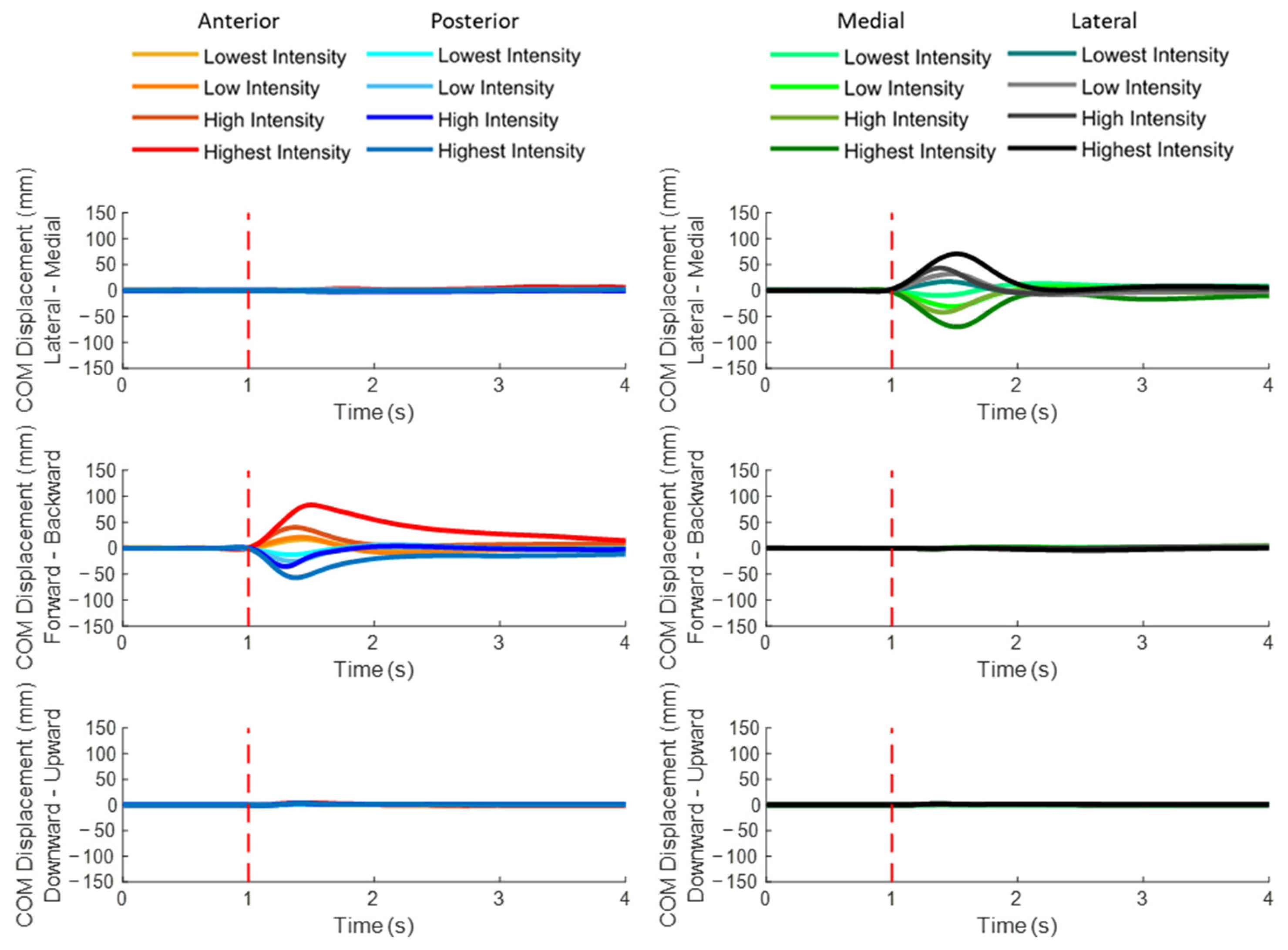
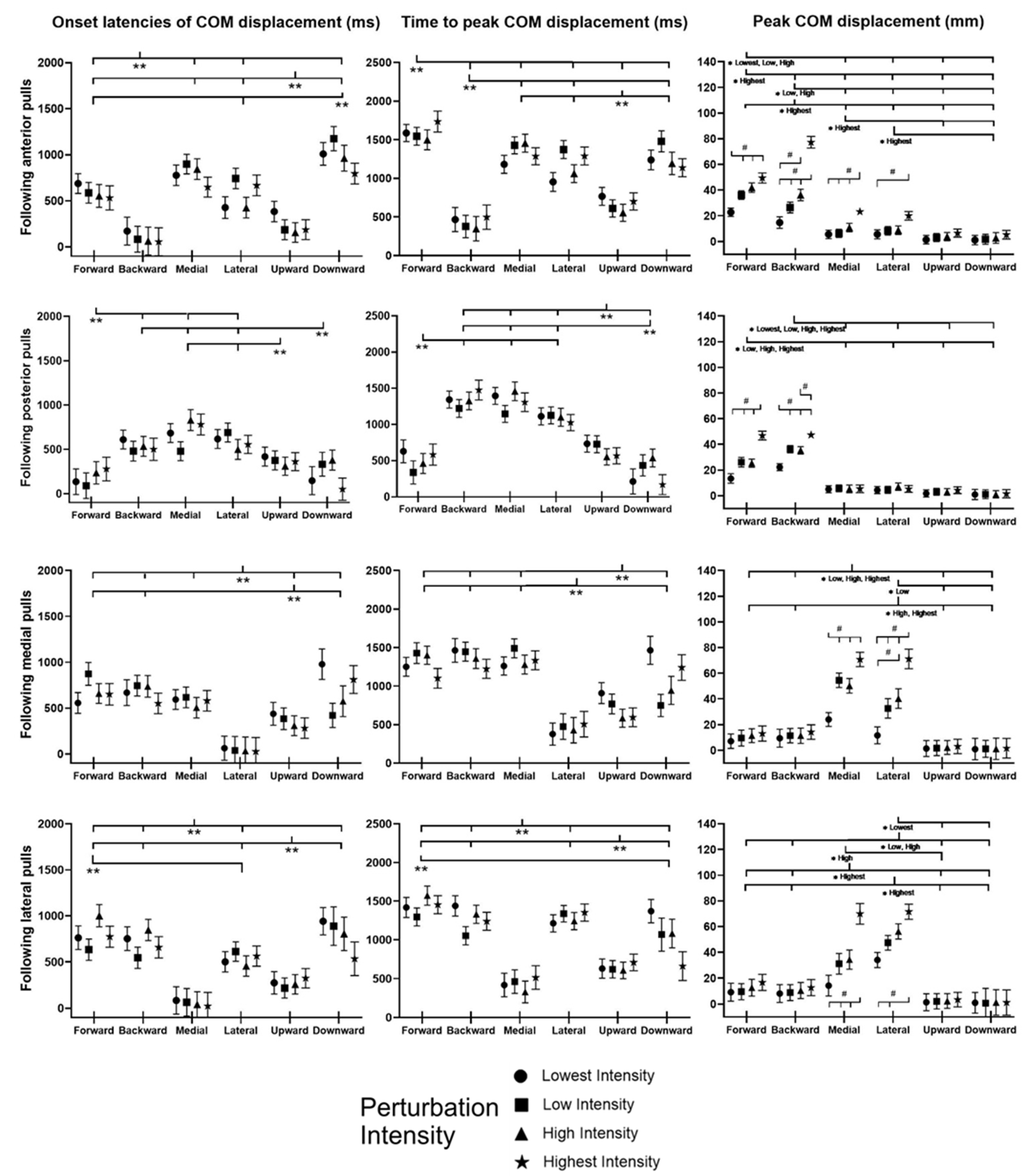
3.1. COM Displacements
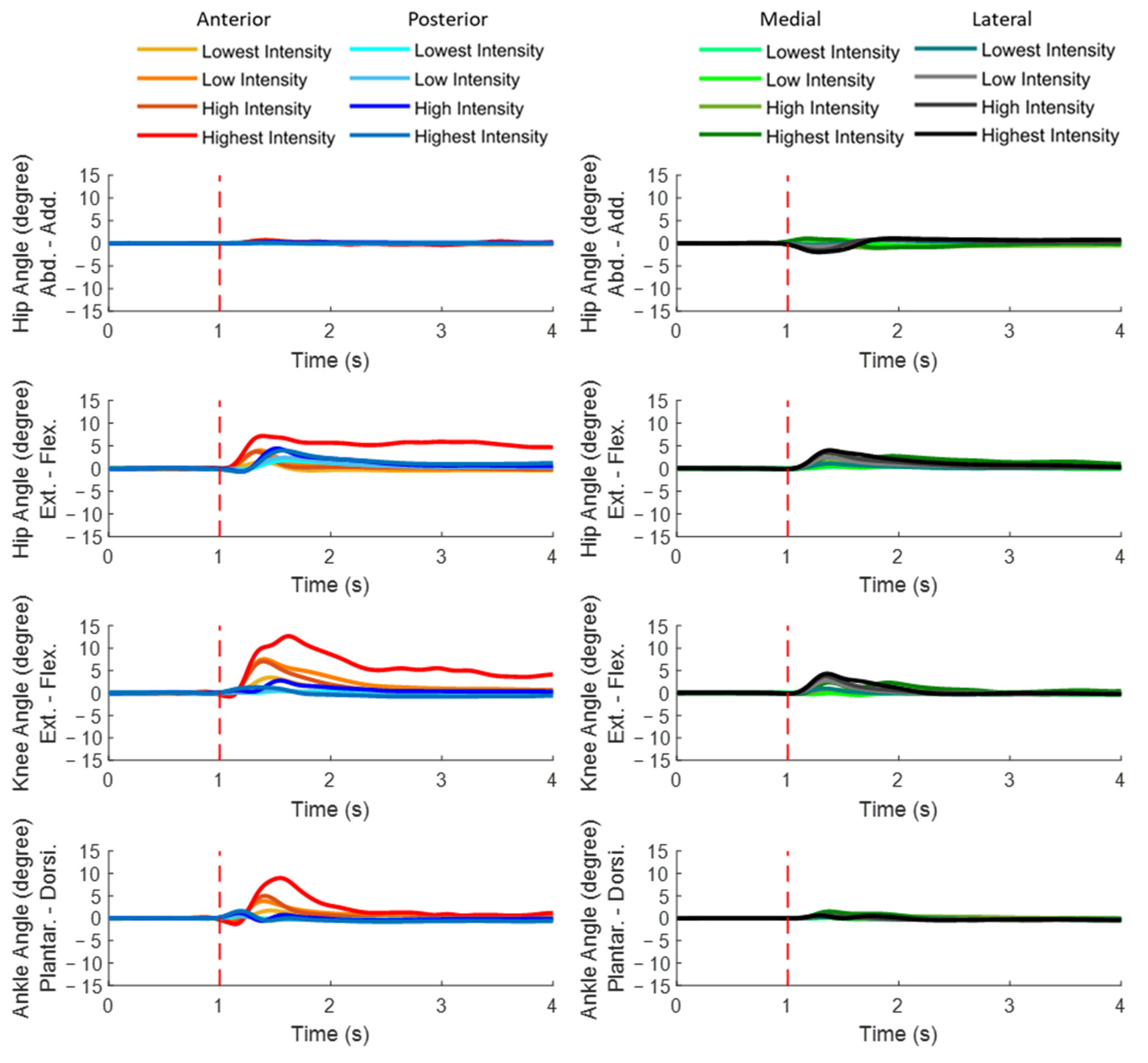
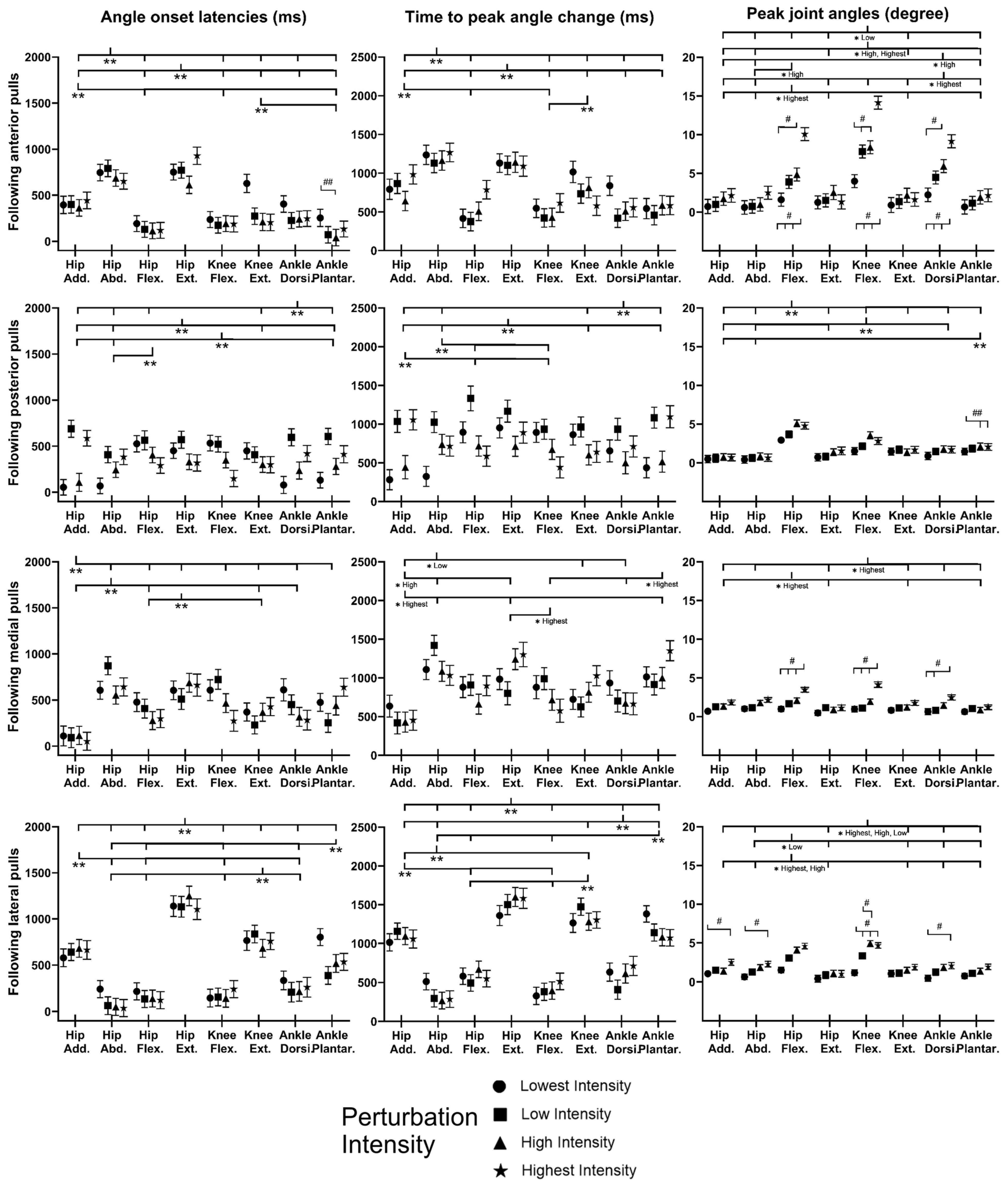
3.2. Dominant-Leg Joint Motions
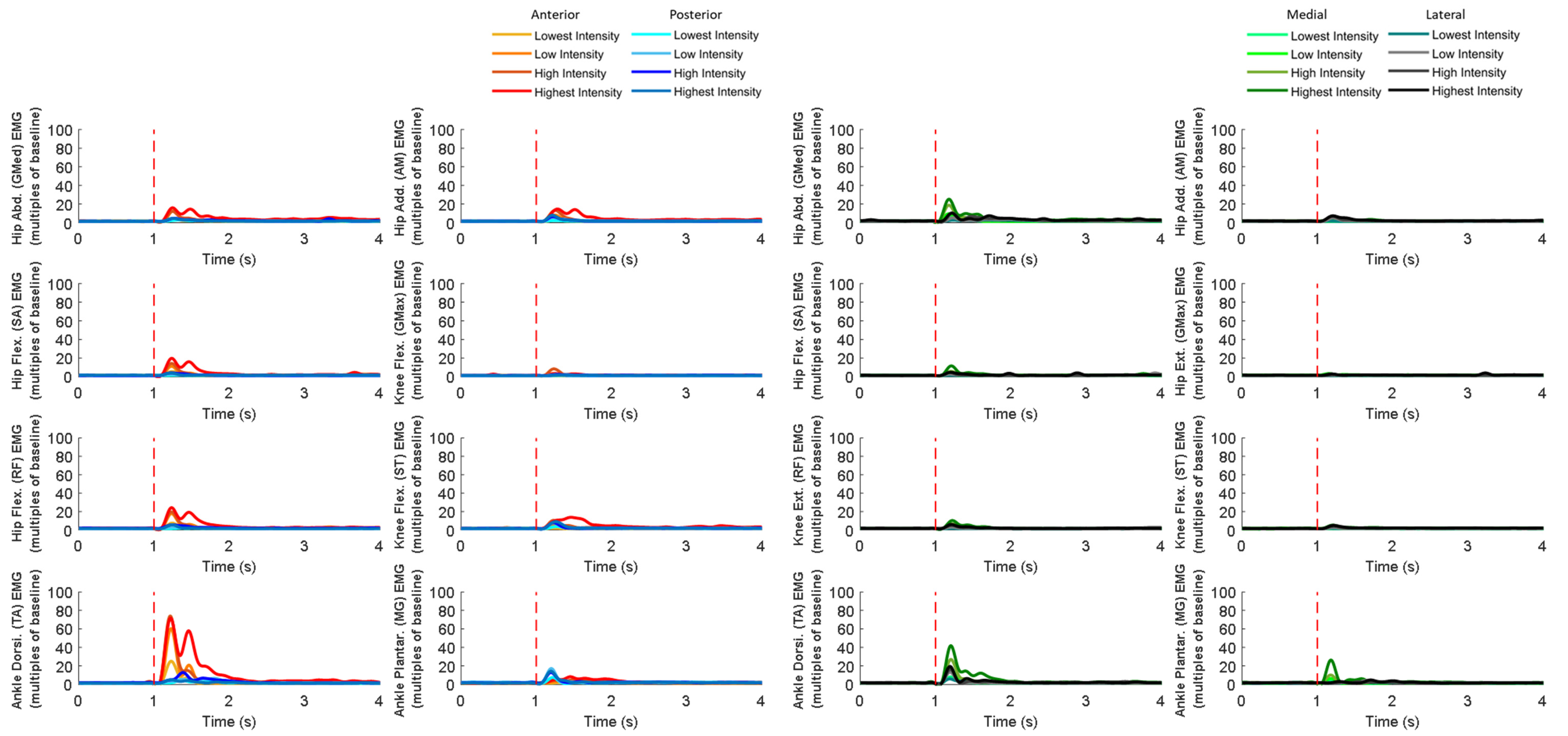
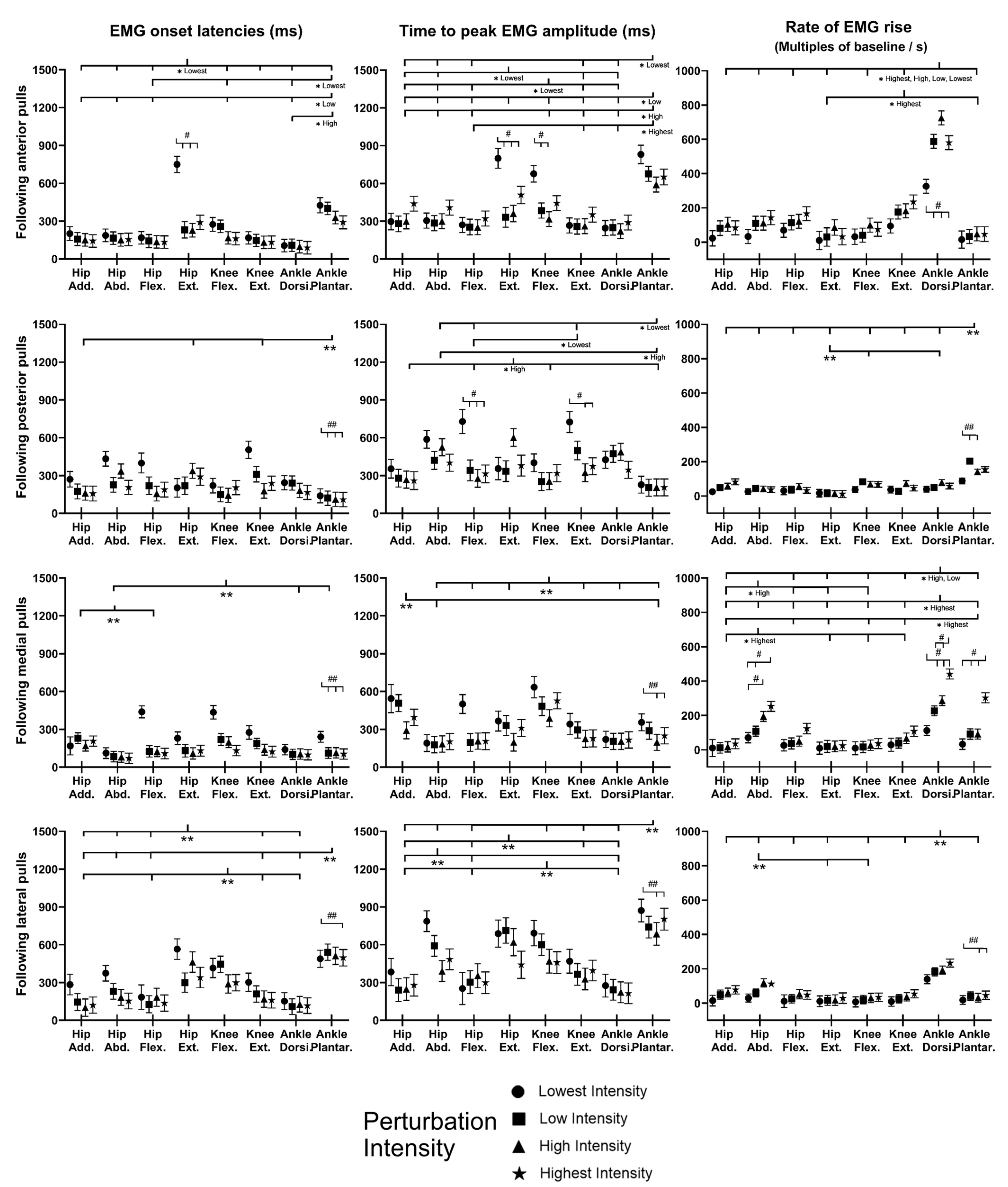
3.3. EMG Signals of Eight Dominant-Leg Muscles
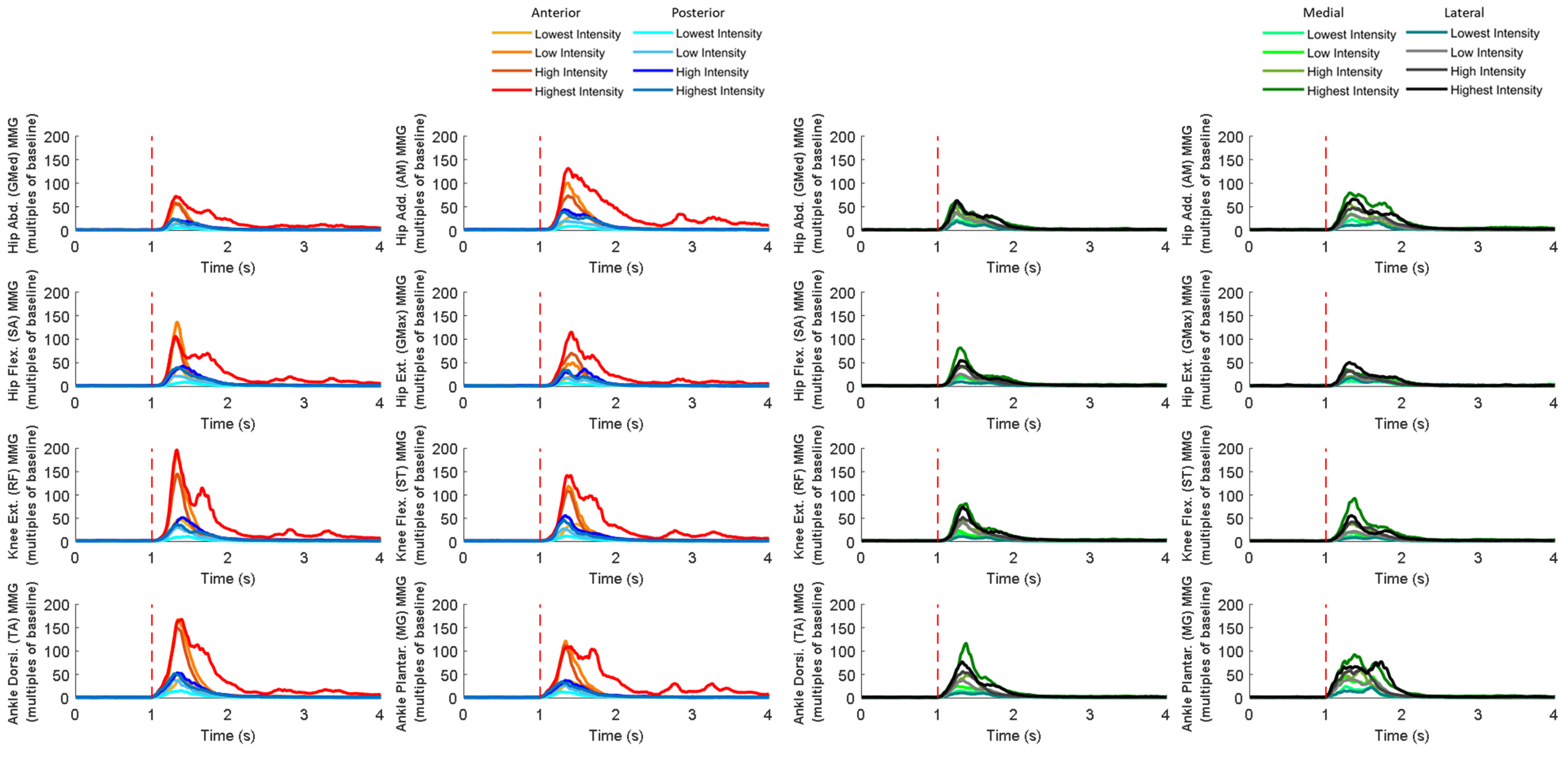
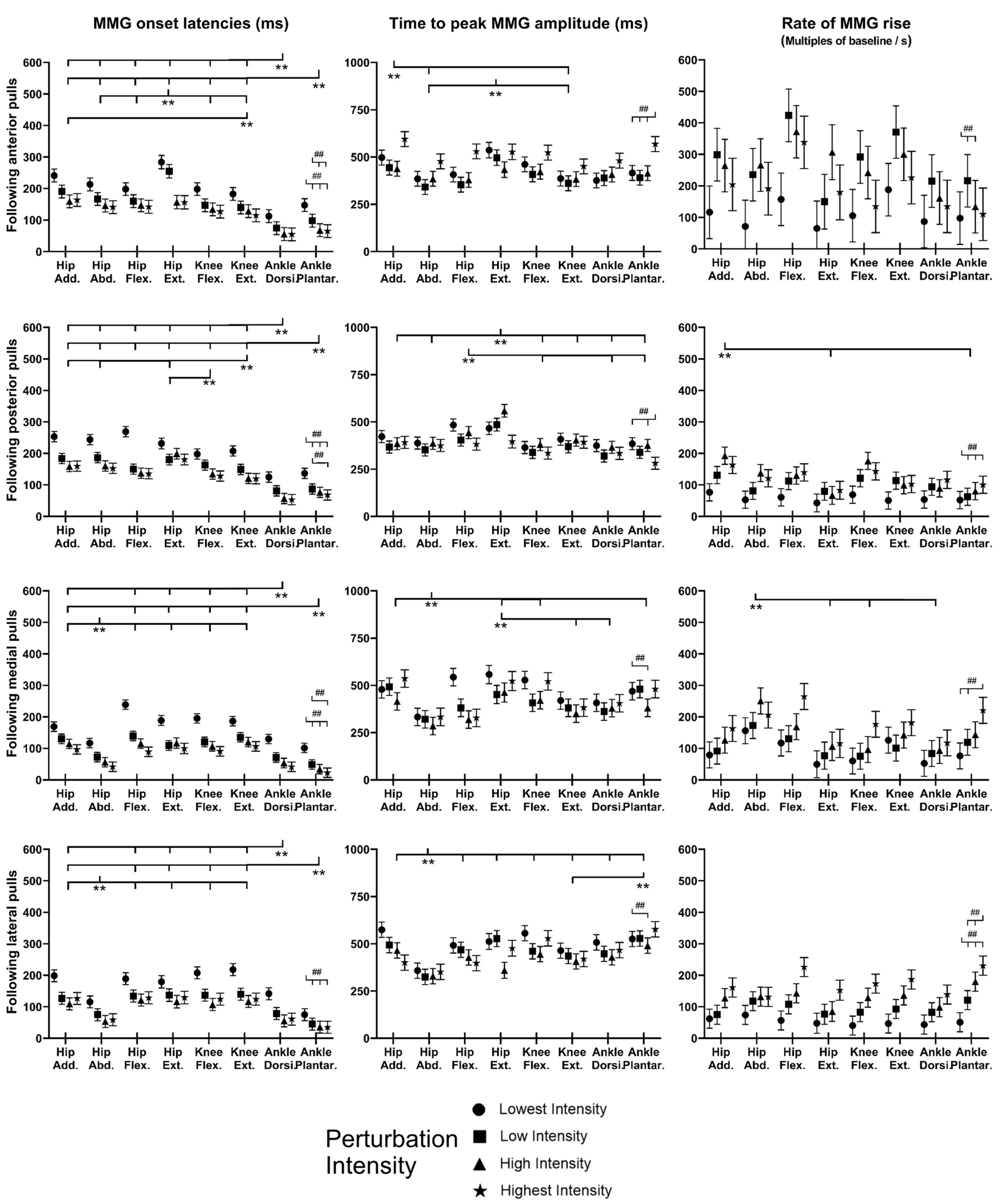
3.4. MMG Signals of Eight Dominant-Leg Muscles
4. Discussion
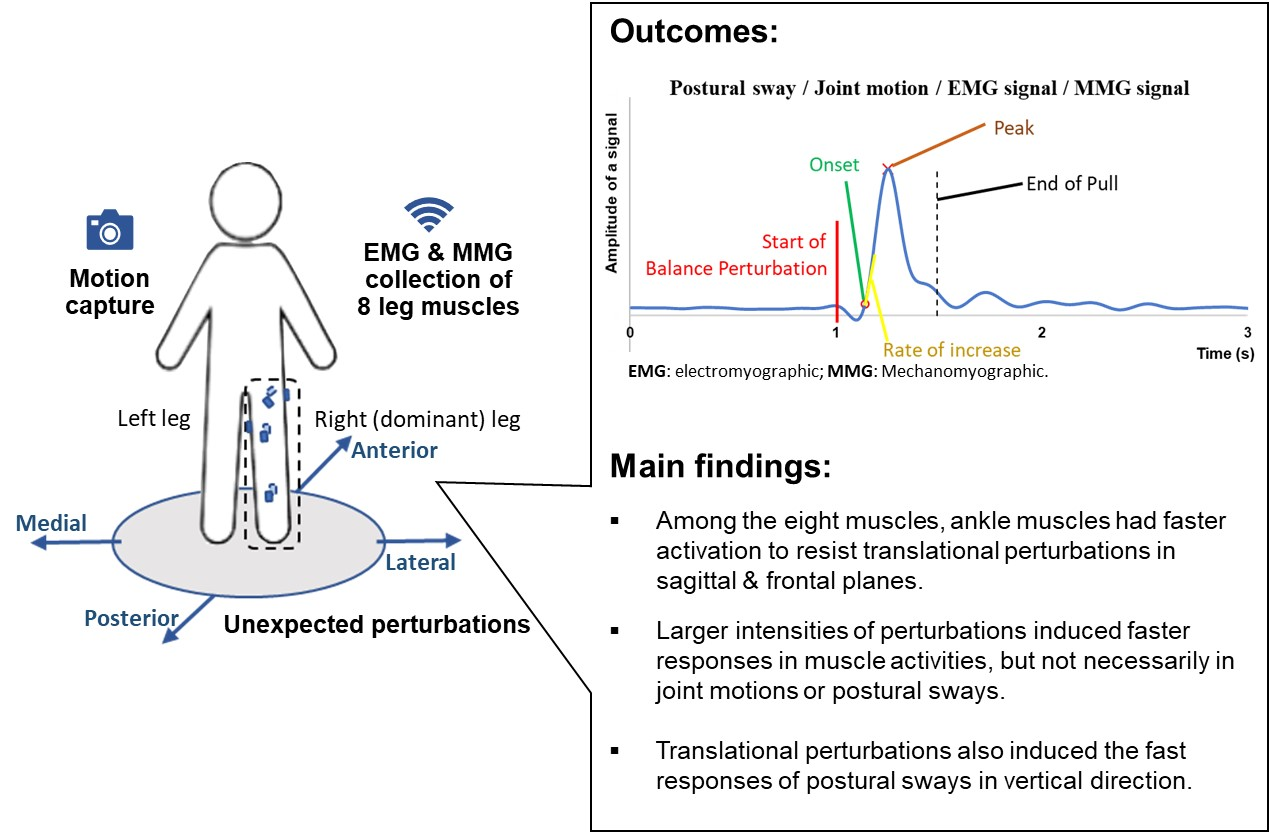
4.1. Faster Activation Existed in Agonist Lower-Limb Muscles, Espaecially Ankle Muscles, to Resist the Induced Postural Sway (Hypothesis 1)
4.2. Rapid Kinematic Responses Varied with the Perturbation Direction (Hypothesis 2)
4.3. Larger Perturbation Intensity Evoked Faster Rosponse in Muscle Activation (Hypothesis 3)
4.4. MMG Signals Following Balance Perturbations Merit Further Study
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Falls. Available online: https://www.who.int/news-room/fact-sheets/detail/falls# (accessed on 30 April 2023).
- Bergen, G.; Stevens, M.R.; Burns, E.R. Falls and fall injuries among adults aged ≥65 years—United States, 2014. Morb. Mortal. Wkly. Rep. 2016, 65, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Solis-Escalante, T.; Stokkermans, M.; Cohen, M.X.; Weerdesteyn, V. Cortical responses to whole-body balance perturbations index perturbation magnitude and predict reactive stepping behavior. Eur. J. Neurosci. 2021, 54, 8120–8138. [Google Scholar] [CrossRef] [PubMed]
- Moreland, B.; Kakara, R.; Henry, A. Trends in nonfatal falls and fall-related injuries among adults aged ≥65 years—United States, 2012–2018. Morb. Mortal. Wkly. Rep. 2020, 69, 875. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubega, M.; Di Marco, R.; Zampini, M.; Formaggio, E.; Menegatti, E.; Bonato, P.; Masiero, S.; Del Felice, A. Muscular and cortical activation during dynamic and static balance in the elderly: A scoping review. Aging Brain 2021, 1, 100013. [Google Scholar] [CrossRef]
- Blenkinsop, G.M.; Pain, M.T.; Hiley, M.J. Balance control strategies during perturbed and unperturbed balance in standing and handstand. R. Soc. Open Sci. 2017, 4, 161018. [Google Scholar] [CrossRef] [Green Version]
- Ono, H.; Sato, T.; Ohnishi, K. Balance Recovery of Ankle Strategy: Using Knee Joint for Biped Robot. In Proceedings of the 2011 1st International Symposium on Access Spaces (ISAS), Yokohama, Japan, 17–19 June 2011; pp. 236–241. [Google Scholar]
- Kochoa, P. Balance Strategy Basics. Available online: https://www.professionalptandtraining.com/balance-strategy-basics/ (accessed on 1 June 2023).
- Runge, C.; Shupert, C.; Horak, F.; Zajac, F. Ankle and hip postural strategies defined by joint torques. Gait Posture 1999, 10, 161–170. [Google Scholar] [CrossRef]
- Bair, W.-N.; Prettyman, M.G.; Beamer, B.A.; Rogers, M.W. Kinematic and behavioral analyses of protective stepping strategies and risk for falls among community living older adults. Clin. Biomech. 2016, 36, 74–82. [Google Scholar] [CrossRef] [Green Version]
- Tsai, Y.-C.; Hsieh, L.-F.; Yang, S. Age-related changes in posture response under a continuous and unexpected perturbation. J. Biomech. 2014, 47, 482–490. [Google Scholar] [CrossRef]
- Chen, C.-L.; Lou, S.-Z.; Wu, H.-W.; Wu, S.-K.; Yeung, K.-T.; Su, F.-C. Effects of the type and direction of support surface perturbation on postural responses. J. Neuroeng. Rehabil. 2014, 11, 50. [Google Scholar] [CrossRef] [Green Version]
- Hwang, S.; Tae, K.; Sohn, R.; Kim, J.; Son, J.; Kim, Y. The Balance Recovery Mechanisms Against Unexpected Forward Perturbation. Ann. Biomed. Eng. 2009, 37, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Baudry, S.; Lecoeuvre, G.; Duchateau, J. Age-related changes in the behavior of the muscle-tendon unit of the gastrocnemius medialis during upright stance. J. Appl. Physiol. 2012, 112, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Błaszczyszyn, M.; Szczęsna, A.; Piechota, K. sEMG activation of the flexor muscles in the foot during balance tasks by young and older women: A pilot study. Int. J. Environ. Res. Public Health 2019, 16, 4307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cattagni, T.; Scaglioni, G.; Laroche, D.; Grémeaux, V.; Martin, A. The involvement of ankle muscles in maintaining balance in the upright posture is higher in elderly fallers. Exp. Gerontol. 2016, 77, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Sawers, A.; Pai, Y.-C.; Bhatt, T.; Ting, L.H. Neuromuscular responses differ between slip-induced falls and recoveries in older adults. J. Neurophysiol. 2017, 117, 509–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faulkner, K.A.; Redfern, M.S.; Cauley, J.A.; Landsittel, D.P.; Studenski, S.A.; Rosano, C.; Simonsick, E.M.; Harris, T.B.; Shorr, R.I.; Ayonayon, H.N. Multitasking: Association between poorer performance and a history of recurrent falls. J. Am. Geriatr. Soc. 2007, 55, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Pijnappels, M.; Bobbert, M.F.; van Dieën, J.H. Control of support limb muscles in recovery after tripping in young and older subjects. Exp. Brain Res. 2005, 160, 326–333. [Google Scholar] [CrossRef]
- Inacio, M.; Creath, R.; Rogers, M.W. Effects of aging on hip abductor-adductor neuromuscular and mechanical performance during the weight transfer phase of lateral protective stepping. J. Biomech. 2019, 82, 244–250. [Google Scholar] [CrossRef]
- Zhu, R.T.-L.; Lyu, P.-Z.; Li, S.; Tong, C.Y.; Ling, Y.T.; Ma, C.Z.-H. How Does Lower Limb Respond to Unexpected Balance Perturbations? New Insights from Synchronized Human Kinetics, Kinematics, Muscle Electromyography (EMG) and Mechanomyography (MMG) Data. Biosensors 2022, 12, 430. [Google Scholar] [CrossRef]
- Cè, E.; Longo, S.; Limonta, E.; Coratella, G.; Rampichini, S.; Esposito, F. Peripheral fatigue: New mechanistic insights from recent technologies. Eur. J. Appl. Physiol. 2020, 120, 17–39. [Google Scholar] [CrossRef]
- Woodward, R.B.; Stokes, M.J.; Shefelbine, S.J.; Vaidyanathan, R. Segmenting mechanomyography measures of muscle activity phases using inertial data. Sci. Rep. 2019, 9, 5569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, C.Z.-H.; Ling, Y.T.; Shea, Q.T.K.; Wang, L.-K.; Wang, X.-Y.; Zheng, Y.-P. Towards Wearable Comprehensive Capture and Analysis of Skeletal Muscle Activity during Human Locomotion. Sensors 2019, 19, 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyu, P.-Z.; Zhu, R.T.; Ling, Y.T.; Wang, L.-K.; Zheng, Y.-P.; Ma, C.Z. How Paretic and Non-Paretic Ankle Muscles Contract during Walking in Stroke Survivors: New Insight Using Novel Wearable Ultrasound Imaging and Sensing Technology. Biosensors 2022, 12, 349. [Google Scholar] [CrossRef] [PubMed]
- Gerards, M.H.; Meijer, K.; Karamanidis, K.; Grevendonk, L.; Hoeks, J.; Lenssen, A.F.; McCrum, C. Adaptability to balance perturbations during walking as a potential marker of falls history in older adults. Front. Sports Act. Living 2021, 3, 132. [Google Scholar] [CrossRef]
- VICON. Full Body Modeling with Plug-In Gait. Available online: https://docs.vicon.com/display/Nexus212/Full+body+modeling+with+Plug-in+Gait (accessed on 20 April 2022).
- Quam, S. Johnson Health Tech: EMG Sensor Holder for Heels and Center of Mass Approximation; University of Wisconsin: Madison, WI, USA, 2020. [Google Scholar]
- SENIAM. The SENIAM Project. Available online: http://seniam.org/sensor_location.htm (accessed on 20 April 2022).
- Jiroumaru, T.; Kurihara, T.; Isaka, T. Measurement of muscle length-related electromyography activity of the hip flexor muscles to determine individual muscle contributions to the hip flexion torque. SpringerPlus 2014, 3, 624. [Google Scholar] [CrossRef] [Green Version]
- Hides, J.A.; Beall, P.; Smith, M.M.F.; Stanton, W.; Miokovic, T.; Richardson, C. Activation of the hip adductor muscles varies during a simulated weight-bearing task. Phys. Ther. Sport 2016, 17, 19–23. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [Green Version]
- Kempen, G.I.J.M.; Yardley, L.; Van Haastregt, J.C.M.; Zijlstra, G.A.R.; Beyer, N.; Hauer, K.; Todd, C. The Short FES-I: A shortened version of the falls efficacy scale-international to assess fear of falling. Age Ageing 2008, 37, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Swanenburg, J.; Nevzati, A.; Hager, A.G.M.; de Bruin, E.D.; Klipstein, A. The maximal width of the base of support (BSW): Clinical applicability and reliability of a preferred-standing test for measuring the risk of falling. Arch. Gerontol. Geriatr. 2013, 57, 204–210. [Google Scholar] [CrossRef]
- Shao, X.R.; Wang, Z.; Luan, L.J.; Sheng, Y.L.; Yu, R.N.; Pranata, A.; Adams, R.; Zhang, A.R.; Han, J. Impaired ankle inversion proprioception during walking is associated with fear of falling in older adults. Front. Aging Neurosci. 2022, 14, 946509. [Google Scholar] [CrossRef]
- Franchignoni, F.; Horak, F.; Godi, M.; Nardone, A.; Giordano, A. Using psychometric techniques to improve the Balance Evaluation Systems Test: The mini-BESTest. J. Rehabil. Med. 2010, 42, 323–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, M.; Schrader, J.; Applegate, T.; Koceja, D. Unilateral postural control of the functionally dominant and nondominant extremities of healthy subjects. J. Athl. Train. 1998, 33, 319–322. [Google Scholar] [PubMed]
- Pai, Y.-C.; Rogers, M.W.; Patton, J.; Cain, T.D.; Hanke, T.A. Static versus dynamic predictions of protective stepping following waist–pull perturbations in young and older adults. J. Biomech. 1998, 31, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Luchies, C.W.; Alexander, N.B.; Schultz, A.B.; Ashton-Miller, J. Stepping responses of young and old adults to postural disturbances: Kinematics. J. Am. Geriatr. Soc. 1994, 42, 506–512. [Google Scholar] [CrossRef] [Green Version]
- Singh, H.; Sanders, O.; McCombe Waller, S.; Bair, W.-N.; Beamer, B.; Creath, R.A.; Rogers, M.W. Relationship Between Head-Turn Gait Speed and Lateral Balance Function in Community-Dwelling Older Adults. Arch. Phys. Med. Rehabil. 2017, 98, 1955–1961. [Google Scholar] [CrossRef]
- Caulcrick, C.; Huo, W.; Hoult, W.; Vaidyanathan, R. Human Joint Torque Modelling With MMG and EMG During Lower Limb Human-Exoskeleton Interaction. IEEE Robot. Autom. Lett. 2021, 6, 7185–7192. [Google Scholar] [CrossRef]
- Borrelli, J.R.; Zabukovec, J.; Jones, S.; Junod, C.A.; Maki, B.E. Age-related changes in the capacity to select early-onset upper-limb reactions to either recover balance or protect against impact. Exp. Gerontol. 2019, 125, 110676. [Google Scholar] [CrossRef]
- Cronin, N.J.; Barrett, R.S.; Lichtwark, G.; Mills, P.M.; Carty, C.P. Decreased lower limb muscle recruitment contributes to the inability of older adults to recover with a single step following a forward loss of balance. J. Electromyogr. Kinesiol. 2013, 23, 1139–1144. [Google Scholar] [CrossRef]
- de Freitas, P.B.; Knight, C.A.; Barela, J.A. Postural reactions following forward platform perturbation in young, middle-age, and old adults. J. Electromyogr. Kinesiol. 2010, 20, 693–700. [Google Scholar] [CrossRef]
- Krašna, S.; Keller, A.; Linder, A.; Silvano, A.P.; Xu, J.-C.; Thomson, R.; Klug, C. Human response to longitudinal perturbations of standing passengers on public transport during regular operation. Front. Bioeng. Biotechnol. 2021, 9, 680883. [Google Scholar] [CrossRef]
- Afschrift, M.; Pitto, L.; Aerts, W.; van Deursen, R.; Jonkers, I.; De Groote, F. Modulation of gluteus medius activity reflects the potential of the muscle to meet the mechanical demands during perturbed walking. Sci. Rep. 2018, 8, 11675. [Google Scholar] [CrossRef] [Green Version]
- Gilles, M.; Wing, A.M.; Kirker, S.G. Lateral balance organisation in human stance in response to a random or predictable perturbation. Exp. Brain Res. 1999, 124, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Jeon, W.; Griffin, L.; Hsiao, H.-Y. Effects of initial foot position on postural responses to lateral standing surface perturbations in younger and older adults. Gait Posture 2021, 90, 449–456. [Google Scholar] [CrossRef]
- Freyler, K.; Gollhofer, A.; Colin, R.; Brüderlin, U.; Ritzmann, R. Reactive balance control in response to perturbation in unilateral stance: Interaction effects of direction, displacement and velocity on compensatory neuromuscular and kinematic responses. PLoS ONE 2015, 10, e0144529. [Google Scholar] [CrossRef]
- Winter, D.A.; Patla, A.E.; Frank, J.S.; Walt, S.E. Biomechanical walking pattern changes in the fit and healthy elderly. Phys. Ther. 1990, 70, 340–347. [Google Scholar] [CrossRef]
- Kovacikova, Z.; Zemkova, E.; Neumannova, K.; Jelen, M.; Jelen, K.; Janura, M. The role of lateral preference of lower limbs in a postural stabilization task. Neuroendocrinol. Lett. 2015, 36, 91–95. [Google Scholar] [PubMed]
- Ma, C.Z.-H.; Chung, A.K.-L.; Ling, Y.T.; Huang, Z.-H.; Cheng, C.L.-K.; Zheng, Y.-P. A Newly-Developed Smart Insole System with Instant Reminder: Paves the Way towards Integrating Artificial Intelligence (AI) Technology to Improve Balance and Prevent Falls. Age Ageing 2019, 48, iv28–iv33. [Google Scholar] [CrossRef]
- Ma, C.Z.-H.; Bao, T.; DiCesare, C.A.; Harris, I.; Chambers, A.; Shull, P.B.; Zheng, Y.-P.; Cham, R.; Sienko, K.H. Reducing Slip Risk: A Feasibility Study of Gait Training with Semi-Real-Time Feedback of Foot–Floor Contact Angle. Sensors 2022, 22, 3641. [Google Scholar] [CrossRef]
- Ma, C.Z.-H.; Lam, W.-K.; Chang, B.-C.; Lee, W.C.-C. Can Insoles Be Used to Improve Static and Dynamic Balance of Community-Dwelling Older Adults? A Systematic Review on Recent Advances and Future Perspectives. J. Aging Phys. Act. 2020, 28, 971–986. [Google Scholar] [CrossRef]
- Ma, C.Z.-H.; Zheng, Y.-P.; Lee, W.C.-C. Changes in gait and plantar foot loading upon using vibrotactile wearable biofeedback system in patients with stroke. Top. Stroke Rehabil. 2018, 25, 20–27. [Google Scholar] [CrossRef]
- Ma, C.Z.-H.; Wong, D.W.-C.; Wan, A.H.-P.; Lee, W.C.-C. Effects of orthopedic insoles on static balance of older adults wearing thick socks. Prosthet. Orthot. Int. 2018, 42, 357–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, C.Z.-H.; Lee, W.C.-C. A wearable vibrotactile biofeedback system improves balance control of healthy young adults following perturbations from quiet stance. Hum. Mov. Sci. 2017, 55, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.Z.-H.; Wong, D.W.-C.; Lam, W.K.; Wan, A.H.-P.; Lee, W.C.-C. Balance improvement effects of biofeedback systems with state-of-the-art wearable sensors: A systematic review. Sensors 2016, 16, 434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, A.H.; Wong, D.W.; Ma, C.Z.; Zhang, M.; Lee, W.C. Wearable vibrotactile biofeedback device allowing identification of different floor conditions for lower-limb amputees. Arch. Phys. Med. Rehabil. 2016, 97, 1210–1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, C.Z.-H.; Wan, A.H.-P.; Wong, D.W.-C.; Zheng, Y.-P.; Lee, W.C.-C. A vibrotactile and plantar force measurement-based biofeedback system: Paving the way towards wearable balance-improving devices. Sensors 2015, 15, 31709–31722. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Gao, C.; Fu, H.; Ma, C.Z.-H.; Wang, Q.; He, Z.; Li, M. Automated Student Classroom Behaviors’ Perception and Identification Using Motion Sensors. Bioengineering 2023, 10, 127. [Google Scholar] [CrossRef]
- Huang, Z.-H.; Ma, C.Z.-H.; Wang, L.-K.; Wang, X.-Y.; Fu, S.-N.; Zheng, Y.-P. Real-time visual biofeedback via wearable ultrasound imaging can enhance the muscle contraction training outcome of young adults. J. Strength Cond. Res. 2022, 36, 941. [Google Scholar] [CrossRef]
- Elhadi, M.M.O.; Ma, C.Z.-H.; Lam, W.K.; Lee, W.C.-C. Biomechanical approach in facilitating long-distance walking of elderly people using footwear modifications. Gait Posture 2018, 64, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Rietdyk, S.; Patla, A.; Winter, D.; Ishac, M.; Little, C. Balance recovery from medio-lateral perturbations of the upper body during standing. J. Biomech. 1999, 32, 1149–1158. [Google Scholar] [CrossRef]
- Lin, S.-I.; Woollacott, M.H. Postural muscle responses following changing balance threats in young, stable older, and unstable older adults. J. Mot. Behav. 2002, 34, 37–44. [Google Scholar] [CrossRef]
- Gerards, M.; Marcellis, R.; Senden, R.; Poeze, M.; de Bie, R.; Meijer, K.; Lenssen, A. The effect of perturbation-based balance training on balance control and fear of falling in older adults: A single-blind randomised controlled trial. BMC Geriatr. 2023, 23, 305. [Google Scholar] [CrossRef]
- Cè, E.; Coratella, G.; Bisconti, A.V.; Venturelli, M.; Limonta, E.; Doria, C.; Rampichini, S.; Longo, S.; Esposito, F. Neuromuscular versus mechanical stretch-induced changes in contralateral versus ipsilateral muscle. Med. Sci. Sports Exerc. 2020, 52, 1294–1306. [Google Scholar] [CrossRef] [PubMed]
- Cè, E.; Rampichini, S.; Agnello, L.; Limonta, E.; Veicsteinas, A.; Esposito, F. Effects of temperature and fatigue on the electromechanical delay components. Muscle Nerve 2013, 47, 566–576. [Google Scholar] [CrossRef]
- Uchiyama, T.; Hori, Y.; Suzuki, K. Estimation of Tibialis Anterior Muscle Stiffness during the Swing Phase of Walking with Various Footwear. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, South Korea, 11–15 July 2017; pp. 4131–4134. [Google Scholar]
- Fukawa, T.; Uchiyama, T. System Identification of Evoked Mechanomyogram to Clarify Lower Limb Muscle Stiffness in Treadmill Walking. Adv. Biomed. Eng. 2016, 5, 1–6. [Google Scholar] [CrossRef]
- Smith, C.M.; Housh, T.J.; Hill, E.C.; Johnson, G.O.; Schmidt, R.J. Dynamic versus isometric electromechanical delay in non-fatigued and fatigued muscle: A combined electromyographic, mechanomyographic, and force approach. J. Electromyogr. Kinesiol. 2017, 33, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Ling, Y.T.; Ma, C.Z.-H.; Shea, Q.T.K.; Zheng, Y.-P. Sonomechanomyography (SMMG): Mapping of Skeletal Muscle Motion Onset during Contraction Using Ultrafast Ultrasound Imaging and Multiple Motion Sensors. Sensors 2020, 20, 5513. [Google Scholar] [CrossRef] [PubMed]




 or
or  indicates post hoc pairwise comparison; SE, standard error; # indicates significant simple main effects of intensity factor; ** indicates significant main effects of postural sway factor; * indicates significant simple main effects of postural sway factor.)
or indicates post hoc pairwise comparison; SE, standard error; # indicates significant simple main effects of intensity factor; ** indicates significant main effects of postural sway factor; * indicates significant simple main effects of postural sway factor.)
indicates post hoc pairwise comparison; SE, standard error; # indicates significant simple main effects of intensity factor; ** indicates significant main effects of postural sway factor; * indicates significant simple main effects of postural sway factor.)
or indicates post hoc pairwise comparison; SE, standard error; # indicates significant simple main effects of intensity factor; ** indicates significant main effects of postural sway factor; * indicates significant simple main effects of postural sway factor.)
 or indicates post hoc pairwise comparison; SE, standard error. ## indicates significant main effects of intensity factor; # indicates significant simple main effects of intensity factor; ** indicates significant main effects of joint motion factor; * indicates significant simple main effects of joint motion factor.)
or indicates post hoc pairwise comparison; SE, standard error. ## indicates significant main effects of intensity factor; # indicates significant simple main effects of intensity factor; ** indicates significant main effects of joint motion factor; * indicates significant simple main effects of joint motion factor.)
or indicates post hoc pairwise comparison; SE, standard error. ## indicates significant main effects of intensity factor; # indicates significant simple main effects of intensity factor; ** indicates significant main effects of joint motion factor; * indicates significant simple main effects of joint motion factor.)
or indicates post hoc pairwise comparison; SE, standard error. ## indicates significant main effects of intensity factor; # indicates significant simple main effects of intensity factor; ** indicates significant main effects of joint motion factor; * indicates significant simple main effects of joint motion factor.)
 or represents post hoc pairwise comparison; SE, standard error; ## indicates significant main effects of intensity factor; # indicates significant simple main effects of intensity factor; ** indicates significant main effects of muscle factor; * indicates significant simple main effects of muscle factor.)
or represents post hoc pairwise comparison; SE, standard error; ## indicates significant main effects of intensity factor; # indicates significant simple main effects of intensity factor; ** indicates significant main effects of muscle factor; * indicates significant simple main effects of muscle factor.)
or represents post hoc pairwise comparison; SE, standard error; ## indicates significant main effects of intensity factor; # indicates significant simple main effects of intensity factor; ** indicates significant main effects of muscle factor; * indicates significant simple main effects of muscle factor.)
or represents post hoc pairwise comparison; SE, standard error; ## indicates significant main effects of intensity factor; # indicates significant simple main effects of intensity factor; ** indicates significant main effects of muscle factor; * indicates significant simple main effects of muscle factor.)
 or represents post hoc pairwise comparison; SE, standard error; ## indicates significant main effects of intensity factor; ** indicates significant main effects of muscle factor.)
or represents post hoc pairwise comparison; SE, standard error; ## indicates significant main effects of intensity factor; ** indicates significant main effects of muscle factor.)
or represents post hoc pairwise comparison; SE, standard error; ## indicates significant main effects of intensity factor; ** indicates significant main effects of muscle factor.)
or represents post hoc pairwise comparison; SE, standard error; ## indicates significant main effects of intensity factor; ** indicates significant main effects of muscle factor.)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Muscle | EMG/MMG Sensor Placement |
|---|---|
| Ankle dorsiflexor: tibialis anterior (TA) |
|
| Ankle plantarflexor: medial gastrocnemius (MG) |
|
| Knee extensor: rectus femoris (RF) |
|
| Knee flexor: semitendinosus (ST) |
|
| Hip flexor: sartorius (SA) |
|
| Hip extensor: gluteus maximus (GMax) |
|
| Hip abductor: gluteus medius (GMed) |
|
| Hip adductor: adductor maximus (AM) |
|
| Male (n = 6) | Female (n = 6) | Total (n = 12) | |
|---|---|---|---|
| Age (year) | 21.2 ± 1.2 | 21.5 ± 0.5 | 21.3 ± 0.9 |
| Height (cm) | 174.8 ± 5.8 | 166.1 ± 4.9 | 170.4 ± 6.9 |
| Body Mass (kg) | 59.2 ± 8.9 | 56.8 ± 3.6 | 58.0 ± 6.6 |
| BMI (kg/m²) | 19.3 ± 2.2 | 20.6 ± 1.0 | 20.0 ± 1.7 |
| Dominant Leg | Right (n = 6) | Right (n = 6) | Right (n = 12) |
| Leg Length (cm) | 88.8 ± 4.6 | 85.0 ± 3.2 | 86.9 ± 4.3 |
| IPAQ-S (Kcal/week) | 2017.3 ± 1253.3 | 1238.2 ± 883.6 | 1627.8 ± 1111.0 |
| FES-I Short Version | 10.8 ± 3.4 | 10.0 ± 2.8 | 10.4 ± 3.0 |
| Mini-BEST Score | 27.0 ± 0 | 27.5 ± 0.5 | 27.3 ± 0.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tong, C.Y.; Zhu, R.T.-L.; Ling, Y.T.; Scheeren, E.M.; Lam, F.M.H.; Fu, H.; Ma, C.Z.-H. Muscular and Kinematic Responses to Unexpected Translational Balance Perturbation: A Pilot Study in Healthy Young Adults. Bioengineering 2023, 10, 831. https://doi.org/10.3390/bioengineering10070831
Tong CY, Zhu RT-L, Ling YT, Scheeren EM, Lam FMH, Fu H, Ma CZ-H. Muscular and Kinematic Responses to Unexpected Translational Balance Perturbation: A Pilot Study in Healthy Young Adults. Bioengineering. 2023; 10(7):831. https://doi.org/10.3390/bioengineering10070831
Chicago/Turabian StyleTong, Cheuk Ying, Ringo Tang-Long Zhu, Yan To Ling, Eduardo Mendonça Scheeren, Freddy Man Hin Lam, Hong Fu, and Christina Zong-Hao Ma. 2023. "Muscular and Kinematic Responses to Unexpected Translational Balance Perturbation: A Pilot Study in Healthy Young Adults" Bioengineering 10, no. 7: 831. https://doi.org/10.3390/bioengineering10070831
APA StyleTong, C. Y., Zhu, R. T. -L., Ling, Y. T., Scheeren, E. M., Lam, F. M. H., Fu, H., & Ma, C. Z. -H. (2023). Muscular and Kinematic Responses to Unexpected Translational Balance Perturbation: A Pilot Study in Healthy Young Adults. Bioengineering, 10(7), 831. https://doi.org/10.3390/bioengineering10070831