






Fetal Heart Rate Preprocessing Techniques: A Scoping Review





Abstract
:1. Introduction
1.1. Methods for FHR Acquisition
1.1.1. External Ultrasound Doppler
1.1.2. Transabdominal Fetal Electrocardiogram
1.1.3. Fetal Phonocardiography
1.1.4. Fetal Electrocardiogram
1.1.5. Fetal Electrocardiogram with STAN
1.2. FHR Signal Contamination
1.2.1. Outliers/Artifacts
1.2.2. Missing Samples
1.2.3. Maternal–Fetal Ambiguities
1.2.4. Other Signal Interference
1.3. FHR Monitoring
1.4. Purpose and Study Contributions
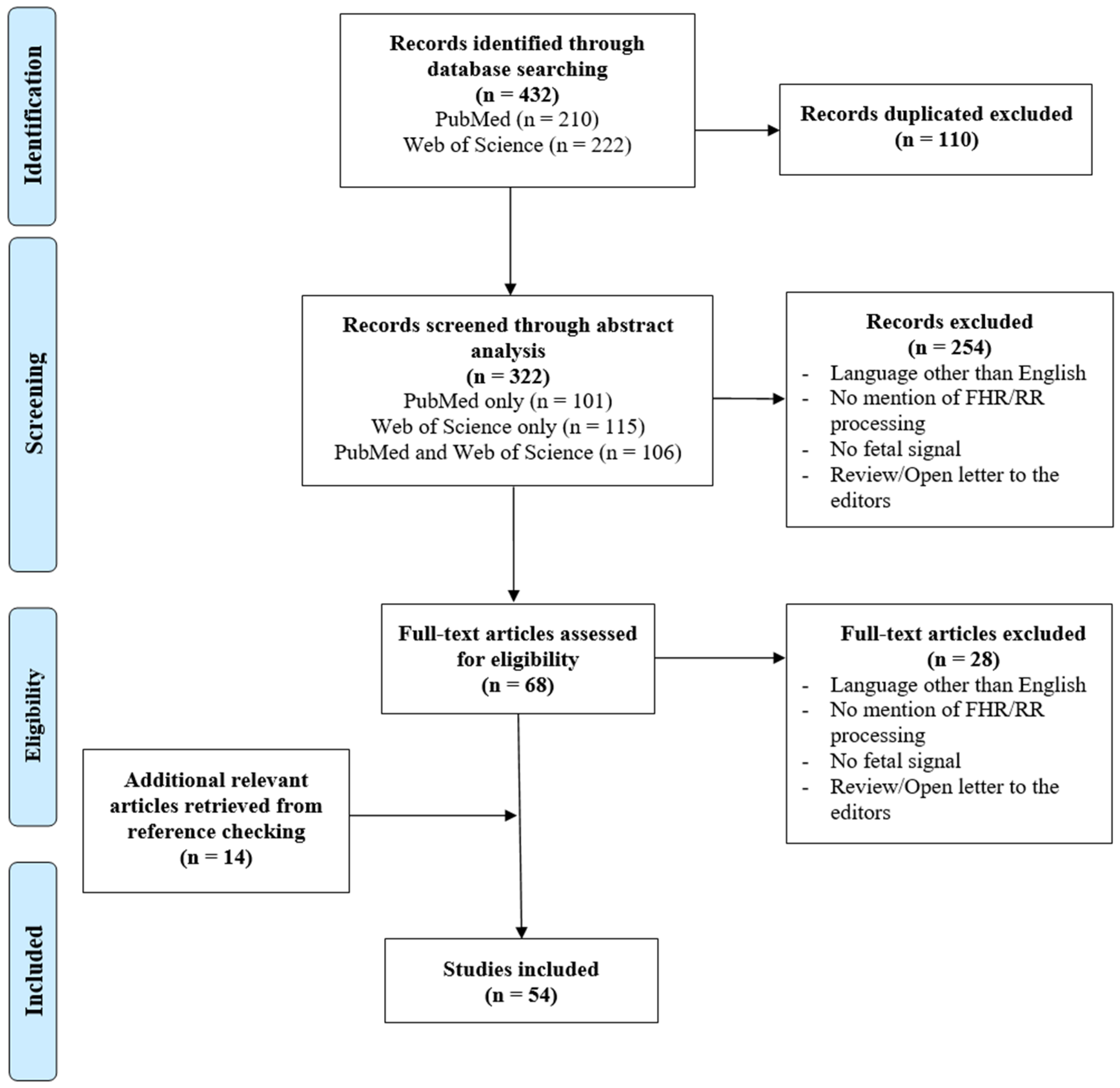
2. Materials and Methods
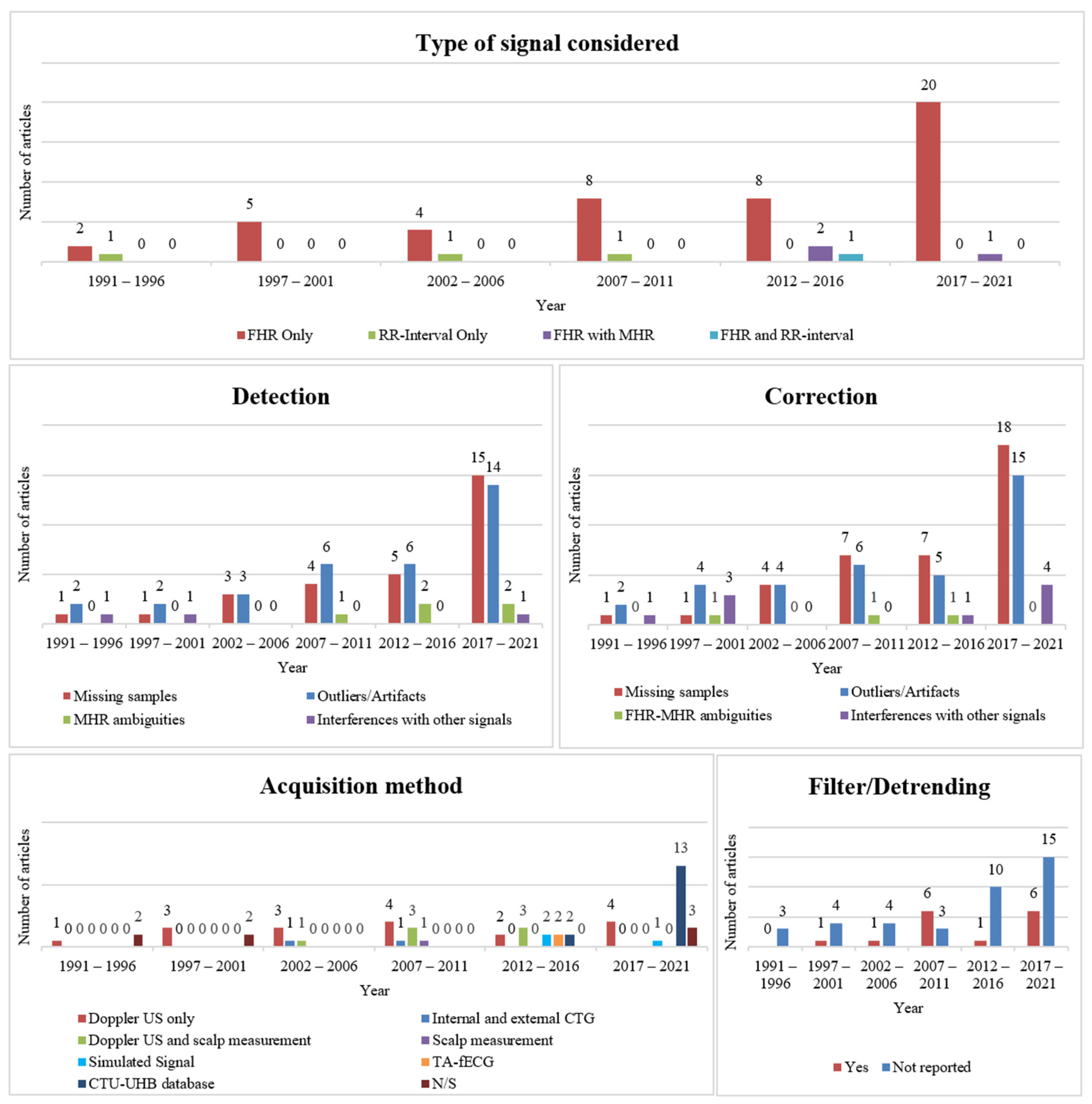
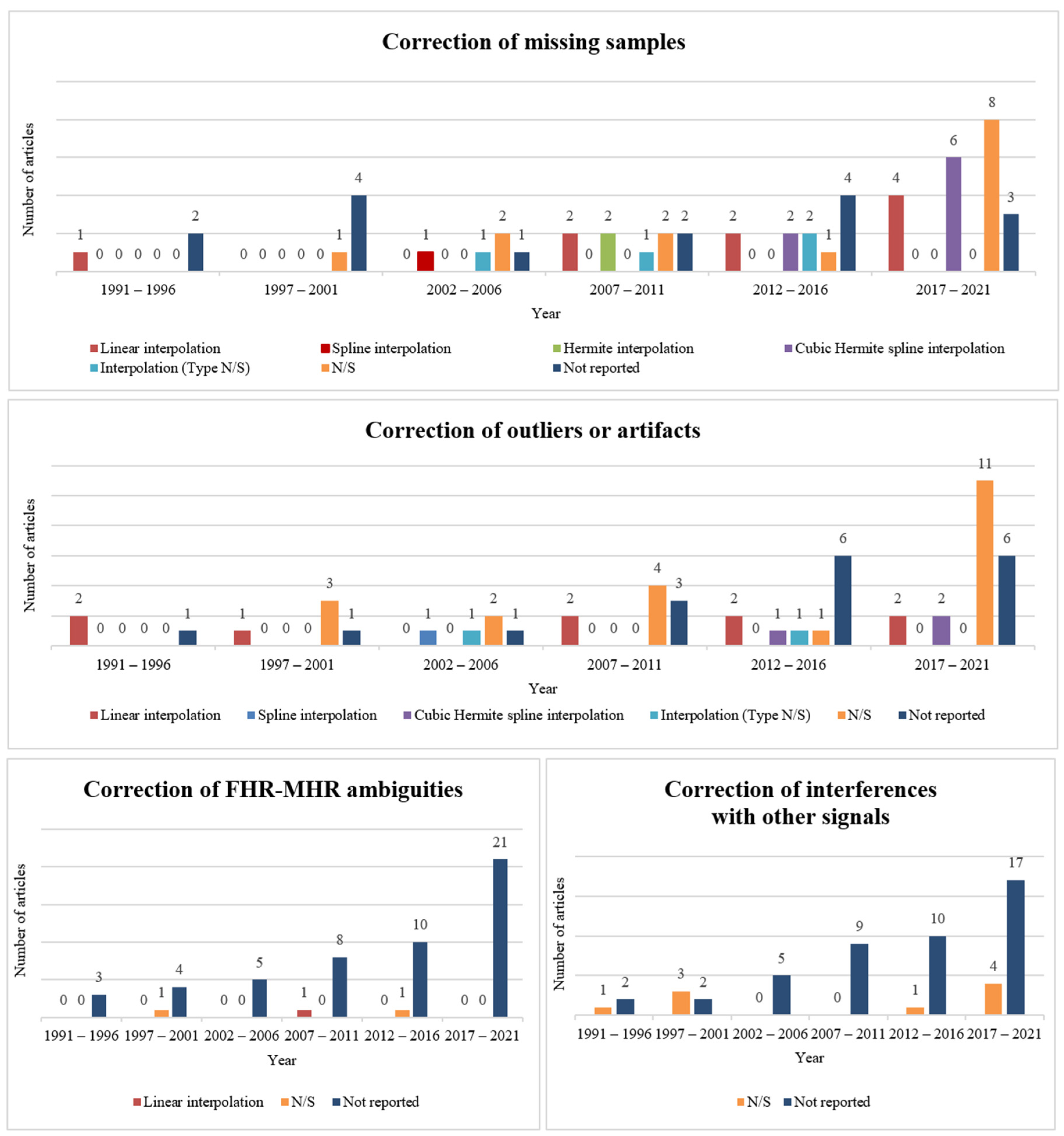
3. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year, Authors (Ref) | Type of Signal Considered | Detection | Correction | Filtering/Detrending | Acquisition Method or Selected Dataset | ||||
|---|---|---|---|---|---|---|---|---|---|
| Missing Samples | Outliers/ Artifacts | MHR Ambiguities| Interferences with Other Signals | Missing Samples | Outliers/ Artifacts | MHR Ambiguities| Interferences with Other Signals | ||||
| Boudet et al. 2020 [44] | FHR only | - | Yes, N/S | Yes, N/S|- | Linear interpolation | Yes, N/S | - | - | - |
| Guijarro-Berdiñas et al. 1997 [37] | FHR only | - | Yes, N/S | -|- | Yes, N/S | Yes, N/S | Yes, N/S|- | - | Doppler ultrasound |
| Cömert et al. 2017 [45] | FHR only | Yes, N/S | Yes, N/S | -|- | Cubic Hermite spline interpolation | Cubic Hermite spline interpolation | -|Yes, N/S | - | CTU-UHB database |
| Cömert et al. 2019 [46] | FHR only | Yes, N/S | Yes, N/S | -|- | Cubic Hermite spline interpolation | Yes, N/S | -|- | - | CTU-UHB database |
| Spilka et al. 2009 [47] | FHR only | - | Yes, N/S | -|- | Hermite interpolation | Yes, N/S | -|- | Third order polynomial | Doppler ultrasound and scalp measurement |
| Agostinelli et al. 2017 [48] | FHR only | - | - | -|- | Linear interpolation | Yes, N/S | -|- | - | CTU-UHB database |
| Frigo et al. 2017 [49] | FHR only | - | - | -|- | Yes, N/S | - | -|- | Yes, N/S | CTU-UHB database |
| Marques et al. 2019 [50] | FHR only | Yes, N/S | Yes, N/S | -|- | Linear interpolation | Linear interpolation | -|- | Low pass filter and Hilbert Transform | Doppler ultrasound |
| Cesarelli et al. 2007 [51] | FHR only | - | Yes, N/S | -|- | Linear interpolation | Linear interpolation | -|- | Fifth-order median filter | Doppler ultrasound |
| Moczko et al. 2002 [52] | FHR only | - | - | -|- | - | - | -|- | Digital bidirectional autoregressive first-order filter | Doppler ultrasound |
| Lu et al. 2020 [53] | FHR only | Yes, N/S | - | -|- | Cubic spline interpolation | - | -|Yes, N/S | - | CTU-UHB database |
| Wrobel et al. 2015 [54] | FHR only | - | - | -|- | Linear interpolation | - | -|- | - | CTU-UHB database |
| Chudáček et al. 2009 [55] | FHR only | Yes, N/S | Yes, N/S | -|- | Hermite interpolation | Yes, N/S | -|- | Third-order polynomial | Doppler ultrasound and scalp measurement |
| Papadimitriou et al. 1996 [25] | FHR only | - | - | -|Yes, N/S | - | - | -|Yes, N/S | - | Doppler ultrasound |
| Nokas et al. 2002 [56] | FHR only | Yes, N/S | Yes, N/S | -|- | Yes | Yes, N/S | -|- | - | Doppler ultrasound |
| Cömert et al. 2019 [57] | FHR only | Yes, N/S | Yes, N/S | -|- | Cubic Hermite spline interpolation | Yes, N/S | -|- | Median filter | CTU-UHB database |
| Fergus et al. 2018 [58] | FHR only | - | - | -|- | Cubic Hermite spline interpolation | Cubic Hermite spline interpolation | -|- | Finite Impulse Response sixth-order high-pass filter | CTU-UHB database |
| Cömert et al. 2018 [59] | FHR only | Yes, N/S | Yes, N/S | -|- | Cubic Hermite spline interpolation | Yes, N/S | -|Yes, N/S | Median filter | CTU-UHB database |
| Feng et al. 2017 [60] | FHR only | - | - | -|- | Yes | - | -|- | - | CTU-UHB database |
| Spilka et al. 2012 [18] | FHR only | - | Yes, N/S | -|- | Linear interpolation | Yes, N/S | -|- | - | CTU-UHB database |
| Tan et al. 2021 [61] | FHR only | Yes, N/S | Yes, N/S | -|- | - | - | -|- | - | - |
| Feng et al. 2021 [15] | FHR only | Yes, N/S | - | -|- | Yes, N/S | - | -|- | - | CTU-UHB database |
| Zhao et al. 2019 [62] | FHR only | Yes, N/S | Yes, N/S | -|- | Yes, N/S | Yes, N/S | -|- | - | CTU-UHB database |
| Tang et al. 2018 [63] | FHR only | Yes, N/S | Yes, N/S | -|- | Yes, N/S | Yes, N/S | -|- | Savitzky–Golay filter | Doppler ultrasound |
| Georgoulas et al. 2017 [64] | FHR only | Yes, N/S | Yes, N/S | -|- | Yes, N/S | Yes, N/S | -|- | - | CTU-UHB database |
| Krupa et al. 2009 [65] | FHR only | Yes, N/S | - | -|- | Yes, N/S | - | -|- | Butterworth low-pass filtering | Doppler ultrasound |
| Jezewski et al. 2008 [66] | FHR only | - | Yes, N/S | -|- | - | Yes, N/S | -|- | - | Doppler ultrasound |
| Papadimitriou et al. 1999 [67] | FHR only | - | - | -|- | - | Yes, N/S | -|Yes, N/S | Low-pass filter | - |
| Papadimitriou et al. 1997 [68] | FHR only | - | - | -|- | - | Yes, N/S | -|Yes, N/S | - | Doppler ultrasound |
| Ayres-de-Campos et al. 2017 [35] | FHR only | Yes, N/S | Yes, N/S | -|- | - | Yes, N/S | -|- | - | - |
| Agostinelli et al. 2017 [48] | FHR only | Yes, N/S | Yes, N/S | -|- | Linear interpolation | Linear interpolation | -|- | - | CTU-UHB database |
| Warrick et al. 2011 [69] | FHR only | - | - | -|- | - | - | -|- | Low-order Chebyshev polynomial | Internal and external CTG |
| Papadimitriou et al. 1997 [70] | FHR only | - | - | -|Yes, N/S | - | - | -|Yes, N/S | - | Doppler ultrasound |
| Spilka et al. 2012 [71] | FHR only | - | Yes, N/S | -|- | Cubic Hermite spline interpolation | Linear interpolation | -|- | Second-order polynomial | Doppler ultrasound and scalp electrode |
| Bernardes et al. 1991 [34] | FHR only | - | Yes, N/S | -|- | - | Linear interpolation | -|- | - | - |
| Romano et al. 2016 [72] | FHR only | Yes, N/S | Yes, N/S | -|- | Interpolation | - | -|- | - | Doppler ultrasound |
| Ayres-de-Campos et al. 2000 [14] | FHR only | Yes, N/S | Yes, N/S | -|- | - | Linear interpolation | -|- | - | - |
| Romano et al. 2013 [19] | FHR only | Yes, N/S | Yes, N/S | -|- | Interpolation | Interpolation | -|- | - | Simulated signal |
| Spilka et al. 2013 [20] | FHR only | Yes, N/S | Yes, N/S | -|- | Cubic Hermite spline interpolation | Cubic Hermite spline interpolation | -|- | - | Doppler ultrasound and scalp electrode |
| Urdal et al. 2019 [73] | FHR only | Yes, N/S | Yes, N/S | -|- | Yes, N/S | Yes, N/S | -|- | - | Doppler ultrasound |
| Oikonomou et al. 2013 [74] | FHR only | Yes, N/S | - | -|- | Yes, N/S | - | -|- | - | Simulated signal |
| Gonçalves et al. 2006 [7] | FHR only | Yes, N/S | Yes, N/S | -|- | Spline interpolation | Spline interpolation | -|- | - | Doppler ultrasound and scalp electrode |
| Nunes et al. 2014 [75] | FHR only | Yes, N/S | - | -|- | - | - | -|- | - | Doppler ultrasound and scalp electrode |
| Warrick et al. 2009 [76] | FHR only | Yes, N/S | Yes, N/S | Yes, N/S |- | Linear interpolation | Linear interpolation | Linear interpolation |- | High- and low-pass filters | Doppler ultrasound |
| Urdal et al. 2021 [77] | FHR only | - | - | -|- | - | - | -|- | - | Simulated signal |
| Cesarelli et al. 2007 [78] | FHR only | Yes, N/S | Yes, N/S | -|- | Yes, N/S | Yes, N/S | -|- | - | Doppler ultrasound and scalp electrode |
| Cao et al. 2003 [79] | FHR only | - | - | -|- | Yes, N/S | Yes, N/S | -|- | - | Doppler ultrasound |
| Felgueiras et al. 1996 [80] | RR-interval only | Yes, N/S | Yes, N/S | -|- | Linear interpolation | Linear interpolation | -|- | - | - |
| Peters et al. 2004 [81] | RR-interval only | Yes, N/S | Yes, N/S | -|- | Interpolation | Interpolation | -|- | - | Internal and external CTG |
| Peters et al. 2011 [82] | RR-interval only | - | - | -|- | Interpolation | - | -|- | - | Scalp measurement |
| Casati et al. 2014 [83] | RR-interval and FHR | - | Yes, N/S | -|- | - | Linear interpolation | -|Yes, N/S | - | TA-fECG |
| Reinhard et al. 2013 [21] | FHR with MHR | - | - | Yes, N/S |- | - | - | -|- | - | External measurements TA-fECG |
| Pinto et al. 2015 [5] | FHR with MHR | - | - | Yes, N/S |- | - | - | Yes, N/S |- | - | Doppler ultrasound |
| Barzideh et al. 2018 [17] | FHR with MHR | Yes, N/S | Yes, N/S | Yes, N/S|Yes, N/S | Yes, N/S | Yes, N/S | -|Yes, N/S | - | Doppler ultrasound |
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AECG | Abdominal electrocardiogram |
| bpm | Beats per minute |
| CTG | Cardiotocography |
| CTU-UHB | Czech Technical University and University Hospital in Brno |
| fECG | Fetal electrocardiogram |
| FHR | Fetal heart rate |
| FIGO | International Federation of Gynecology and Obstetrics |
| mECG | Maternal electrocardiogram |
| MHR | Maternal heart rate |
| STAN | ST analysis |
| TA-fECG | Transabdominal fetal electrocardiogram |
References
- Ayres-de-Campos, D.; Spong, C.Y.; Chandraharan, E. FIGO consensus guidelines on intrapartum fetal monitoring: Cardiotocography. Int. J. Gynecol. Obstet. 2015, 131, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Chez, B.F.; Baird, S.M. Electronic Fetal Heart Rate Monitoring. J. Perinat. Neonatal Nurs. 2011, 25, 180–192. [Google Scholar] [CrossRef]
- Abdulhay, E.W.; Oweis, R.J.; Alhaddad, A.M.; Sublaban, F.N.; Radwan, M.A.; Almasaeed, H.M. Review Article: Non-Invasive Fetal Heart Rate Monitoring Techniques. Biomed. Sci. Eng. 2014, 2, 53–67. [Google Scholar]
- Marzbanrad, F.; Stroux, L.; Clifford, G.D. Cardiotocography and beyond: A review of one-dimensional Doppler ultrasound application in fetal monitoring. Physiol. Meas. 2018, 39, 08TR01. [Google Scholar] [CrossRef]
- Pinto, P.; Costa-Santos, C.; Gonçalves, H.; Ayres-De-Campos, D.; Bernardes, J. Improvements in fetal heart rate analysis by the removal of maternal-fetal heart rate ambiguities. BMC Pregnancy Childbirth 2015, 15, 301. [Google Scholar] [CrossRef]
- Kahankova, R.; Mikolasova, M.; Jaros, R.; Barnova, K.; Ladrova, M.; Martinek, R. A Review of Recent Advances and Future Developments in Fetal Phonocardiography. IEEE Rev. Biomed. Eng. 2023, 16, 653–671. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, H.; Rocha, A.P.; Ayres-de-Campos, D.; Bernardes, J. Internal versus external intrapartum foetal heart rate monitoring: The effect on linear and nonlinear parameters. Physiol. Meas. 2006, 27, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Bakker, P.C.A.M.; Colenbrander, G.J.; Verstraeten, A.A.; Van Geijn, H.P. The quality of intrapartum fetal heart rate monitoring. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 116, 22–27. [Google Scholar] [CrossRef]
- Euliano, T.Y.; Nguyen, M.T.; Darmanjian, S.; McGorray, S.P.; Euliano, N.; Onkala, A.; Gregg, A.R. Monitoring uterine activity during labor: A comparison of 3 methods. Am. J. Obstet. Gynecol. 2013, 208, 66.e1–66.e6. [Google Scholar] [CrossRef]
- Amer-Wahlin, I.; Arulkumaran, S.; Hagberg, H.; Maršál, K.; Visser, G. Fetal electrocardiogram: ST waveform analysis in intrapartum surveillance. BJOG 2007, 114, 1191–1193. [Google Scholar] [CrossRef]
- Amer-Wåhlin, I.; Ingemarsson, I.; Marsal, K.; Herbst, A. Fetal heart rate patterns and ECG ST segment changes preceding metabolic acidaemia at birth. BJOG 2005, 112, 160–165. [Google Scholar] [CrossRef]
- Saccone, G.; Schuit, E.; Amer-Wåhlin, I.; Xodo, S.; Berghella, V. Electrocardiogram ST Analysis During Labor. Obstet. Gynecol. 2016, 127, 127–135. [Google Scholar] [CrossRef]
- Ayres-de-Campos, D. Electronic fetal monitoring or cardiotocography, 50 years later: What’s in a name? Am. J. Obstet. Gynecol. 2018, 218, 545–546. [Google Scholar] [CrossRef] [PubMed]
- Ayres-de-Campos, D.; Bernardes, J.; Garrido, A.; Marques-de-Sá, J.; Pereira-Leite, L. Sisporto 2.0: A program for automated analysis of cardiotocograms. J. Matern. Fetal Med. 2000, 9, 311–318. [Google Scholar] [CrossRef]
- Feng, G.; Quirk, J.G.; Heiselman, C.; Djuric, P.M. Estimation of Consecutively Missed Samples in Fetal Heart Rate Recordings. In Proceedings of the 28th European Signal Processing Conference (EUSIPCO), Amsterdam, The Netherlands, 18–21 January 2021; pp. 1080–1084. [Google Scholar] [CrossRef]
- Peters, C.; Vullings, R.; Bergmans, J.; Oei, G.; Wijn, P. The effect of artifact correction on spectral estimates of heart rate variability. In Proceedings of the 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; IEEE: Piscataway, NJ, USA, 2008; pp. 2669–2672. [Google Scholar] [CrossRef]
- Barzideh, F.; Urdal, J.; Hussein, K.; Engan, K.; Skretting, K.; Mdoe, P.; Kamala, B.; Brunner, S. Estimation of Missing Data in Fetal Heart Rate Signals Using Shift-Invariant Dictionary. In Proceedings of the 26th European Signal Processing Conference (EUSIPCO), Rome, Italy, 3–7 September 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 762–766. [Google Scholar] [CrossRef]
- Spilka, J.; Chudáček, V.; Burša, M.; Zach, L.; Huptych, M.; Lhotská, L.; Janků, P.; Hruban, L. Stability of variability features computed from fetal heart rate with artifcially infused missing data. In Proceedings of the 2010 Computing in Cardiology, Belfast, UK, 26–29 September 2010; IEEE: Piscataway, NJ, USA, 2012; Volume 39, pp. 917–920. [Google Scholar]
- Romano, M.; Faiella, G.; Bifulco, P.; D’Addio, G.; Clemente, F.; Cesarelli, M. Outliers Detection and Processing in CTG Monitoring. In Proceedings of the XIII Mediterranean Conference on Medical and Biological Engineering and Computing, Seville, Spain, 25–28 September 2013; Springer: Berlin/Heidelberg, Germany, 2014; pp. 651–654. [Google Scholar] [CrossRef]
- Spilka, J.; Georgoulas, G.; Karvelis, P.; Oikonomou, V.P.; Chudáček, V.; Stylios, C.; Lhotská, L.; Janků, P. Automatic Evaluation of FHR Recordings from CTU-UHB CTG Database. In Information Technology in Bio-and Medical Informatics: 4th International Conference, ITBAM 2013, Prague, Czech Republic, 28 August 2013. Proceedings 4; Springer: Berlin/Heidelberg, Germany, 2013; pp. 47–61. [Google Scholar] [CrossRef]
- Reinhard, J.; Hayes-Gill, B.R.; Schiermeier, S.; Hatzmann, H.; Heinrich, T.M.; Louwen, F. Intrapartum Heart Rate Ambiguity: A Comparison of Cardiotocogram and Abdominal Fetal Electrocardiogram with Maternal Electrocardiogram. Gynecol. Obstet. Investig. 2013, 75, 101–108. [Google Scholar] [CrossRef]
- Ramsey, P.S.; Johnston, B.W.; Welter, V.E.; Ogburn, P.L., Jr. Artifactual fetal electrocardiographic detection using internal monitoring following intrapartum fetal demise during VBAC trial. J. Matern. Fetal Med. 2000, 9, 360–361. [Google Scholar] [CrossRef]
- Neilson, D.R.; Freeman, R.K.; Mangan, S. Signal ambiguity resulting in unexpected outcome with external fetal heart rate monitoring. Am. J. Obstet. Gynecol. 2008, 198, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Herman, A.; Ron-El, R.; Arieli, S.; Schreyer, P.; Caspi, E. Maternal ECG recorded by internal monitoring closely mimicking fetal heart rate in a recent fetal death. Int. J. Gynecol. Obstet. 1990, 33, 269–271. [Google Scholar] [CrossRef]
- Papadimitriou, S.; Gatzounas, D.; Papadopoulos, V.; Tzigounis, V.; Bezerianos, A. Fetal heart rate signal denoising by processing the wavelet transform modulus maxima. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Amsterdam, The Netherlands, 31 October–3 November 1996; Volume 3, pp. 1029–1030. [Google Scholar] [CrossRef]
- Nunes, I.; Ayres-de-Campos, D.; Figueiredo, C.; Bernardes, J. An overview of central fetal monitoring systems in labour. J. Perinat. Med. 2013, 41, 93–99. [Google Scholar] [CrossRef]
- Gonçalves, H.; Costa, A.; Ayres-de-Campos, D.; Costa-Santos, C.; Rocha, A.P.; Bernardes, J. Comparison of real beat-to-beat signals with commercially available 4 Hz sampling on the evaluation of foetal heart rate variability. Med. Biol. Eng. Comput. 2013, 51, 665–676. [Google Scholar] [CrossRef]
- Dawes, G.S.; Moulden, M.; System, C.W.G.R. 8000: Computerized antenatal FHR analysis. J. Perinat. Med. 1991, 19, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Bernardes, J. Computerized analysis of cardiotocograms in clinical practice and the SisPorto ® system thirty-two years after: Technological, physiopathological and clinical studies. J. Perinat. Med. 2023, 51, 145–160. [Google Scholar] [CrossRef]
- Bracero, L.A.; Morgan, S.; Byrne, D.W. Comparison of visual and computerized interpretation of nonstress test results in a randomized controlled trial. Am. J. Obstet. Gynecol. 1999, 181, 1254–1258. [Google Scholar] [CrossRef] [PubMed]
- Steyn, D.; Odendaal, H. Routine or computerized cardiotocography in severe preeclampsia? A randomized controlled trial. J. Matern. Fetal Investig. 1997, 7, 166–171. [Google Scholar]
- Grivell, R.M.; Alfirevic, Z.; Gyte, G.M.; Devane, D. Antenatal cardiotocography for fetal assessment. Cochrane Database Syst. Rev. 2015, 9, CD007863. [Google Scholar] [CrossRef]
- Baker, H.; Pilarski, N.; Hodgetts-Morton, V.A.; Morris, R.K. Comparison of visual and computerised antenatal cardiotocography in the prevention of perinatal morbidity and mortality. A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 263, 33–43. [Google Scholar] [CrossRef]
- Bernardes, J.; Moura, C.; de Sa, J.P.M.; Leite, L.P. The Porto system for automated cardiotocographic signal analysis. J. Perinat. Med. 1991, 19, 61–65. [Google Scholar] [CrossRef]
- Ayres-de-Campos, D.; Rei, M.; Nunes, I.; Sousa, P.; Bernardes, J. SisPorto 4.0—Computer analysis following the 2015 FIGO Guidelines for intrapartum fetal monitoring. J. Matern.-Fetal Neonatal Med. 2017, 30, 62–67. [Google Scholar] [CrossRef]
- Dawes, N.W.; Dawes, G.S.; Moulden, M.; Redman, C.W.G. Fetal heart rate patterns in term labor vary with sex, gestational age, epidural analgesia, and fetal weight. Am. J. Obstet. Gynecol. 1999, 180, 181–187. [Google Scholar] [CrossRef]
- Guijarro-Berdiñas, B.; Alonso-Betanzos, A.; Prados-Méndez, S.; Fernández-Chaves, O.; Alvarez-Seoane, M.; Ucieda-Pardinas, F. A hybrid intelligent system for the pre-processing of Fetal Heart rate signals in antenatal testing. In Biological and Artificial Computation: From Neuroscience to Technology: International Work-Conference on Artificial and Natural Neural Networks, IWANN'97 Lanzarote, Canary Islands, Spain, June 4–6, 1997 Proceedings 4; Springer: Berlin/Heidelberg, Germany, 1997; pp. 628–633. [Google Scholar] [CrossRef]
- Ponsiglione, A.M.; Cosentino, C.; Cesarelli, G.; Amato, F.; Romano, M. A Comprehensive Review of Techniques for Processing and Analyzing Fetal Heart Rate Signals. Sensors 2021, 21, 6136. [Google Scholar] [CrossRef]
- Castro, L.; Loureiro, M.; Henriques, T.S.; Nunes, I. Systematic Review of Intrapartum Fetal Heart Rate Spectral Analysis and an Application in the Detection of Fetal Acidemia. Front Pediatr. 2021, 9, 661400. [Google Scholar] [CrossRef]
- Kahankova, R.; Martinek, R.; Jaros, R.; Behbehani, K.; Matonia, A.; Jezewski, M.; Behar, J.A. A Review of Signal Processing Techniques for Non-Invasive Fetal Electrocardiography. IEEE Rev. Biomed. Eng. 2020, 13, 51–73. [Google Scholar] [CrossRef] [PubMed]
- Mendis, L.; Palaniswami, M.; Brownfoot, F.; Keenan, E. Computerised Cardiotocography Analysis for the Automated Detection of Fetal Compromise during Labour: A Review. Bioengineering 2023, 10, 1007. [Google Scholar] [CrossRef]
- Al-Yousif, S.; Jaenul, A.; Al-Dayyeni, W.; Alamoodi, A.; Najm, I.; Tahir, N.M.; Alrawi, A.A.A.; Cömert, Z.; Al-Shareefi, N.A.; Saleh, A.H.; et al. A systematic review of automated pre-processing, feature extraction and classification of cardiotocography. PeerJ Comput. Sci. 2021, 7, e452. [Google Scholar] [CrossRef]
- Chudáček, V.; Spilka, J.; Burša, M.; Janků, P.; Hruban, L.; Huptych, M.; Lhotská, L. Open access intrapartum CTG database. BMC Pregnancy Childbirth 2014, 14, 16. [Google Scholar] [CrossRef]
- Boudet, S.; L’aulnoit, A.H.; Demailly, R.; Delgranche, A.; Peyrodie, L.; Beuscart, R.; de L’aulnoit, D.H. A fetal heart rate morphological analysis toolbox for MATLAB. SoftwareX 2020, 11, 100428. [Google Scholar] [CrossRef]
- Comert, Z.; Kocamaz, A.F. A novel software for comprehensive analysis of cardiotocography signals ‘CTG-OAS’. In Proceedings of the 2017 International Artificial Intelligence and Data Processing Symposium (IDAP), Malatya, Turkey, 16–17 September 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Cömert, Z.; Şengür, A.; Akbulut, Y.; Budak, Ü.; Kocamaz, A.F.; Güngör, S. A Simple and Effective Approach for Digitization of the CTG Signals from CTG Traces. IRBM 2019, 40, 286–296. [Google Scholar] [CrossRef]
- Spilka, J.; Chudacek, V.; Koucky, M.; Lhotska, L. Assessment of non-linear features for intrapartal fetal heart rate classification. In Proceedings of the 2009 9th International Conference on Information Technology and Applications in Biomedicine, Larnaka, Cyprus, 4–7 November 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 1–4. [Google Scholar] [CrossRef]
- Agostinelli, A.; Braccili, E.; Marchegiani, E.; Rosati, R.; Sbrollini, A.; Burattini, L.; Morettini, M.; Di Nardo, F.; Fioretti, S.; Burattini, L. Statistical baseline assessment in cardiotocography. In Proceedings of the 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Republic of Korea, 11–15 July 2017; pp. 3166–3169. [Google Scholar] [CrossRef]
- Frigo, G.; Giorgi, G. Comparative evaluation of on-line missing data regression techniques in intrapartum FHR measurements. In Proceedings of the IEEE International Instrumentation and Measurement Technology Conference (I2MTC 2017), Turin, Italy, 22–25 May 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Marques, J.A.L.; Cortez, P.C.; Madeiro, J.P.D.V.; Fong, S.J.; Schlindwein, F.S.; De Albuquerque, V.H.C. Automatic Cardiotocography Diagnostic System Based on Hilbert Transform and Adaptive Threshold Technique. IEEE Access 2019, 7, 73085–73094. [Google Scholar] [CrossRef]
- Cesarelli, M.; Romano, M.; Bifulco, P.; Fratini, A. Cardiac arrhythmias and artifacts in fetal heart rate signals: Detection and correction. In Proceedings of the 11th Mediterranean Conference on Medical and Biomedical Engineering and Computing 2007, Ljubljana, Slovenia, 26–30 June 2007; pp. 789–792. [Google Scholar] [CrossRef]
- Moczko, J.A.; Jezewski, J.; Gacek, A. Detection of fetal breathing movements with joint time-frequency analysis of cardiotocogram records. In Proceedings of the 20th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Hong Kong, China, 1 November 1998; Biomedical Engineering Towards the Year 2000 and Beyond (Cat. No.98CH36286). 1998; Volume 20, pp. 1501–1504. [Google Scholar] [CrossRef]
- Lu, Y.; Zhang, X.; Jing, L.; Li, X.; Fu, X. Estimation of the foetal heart rate baseline based on singular spectrum analysis and empirical mode decomposition. Future Gener. Comput. Syst. 2020, 112, 126–135. [Google Scholar] [CrossRef]
- Wrobel, J.; Roj, D.; Jezewski, J.; Horoba, K.; Kupka, T.; Jezewski, M. Evaluation of the Robustness of Fetal Heart Rate Variability Measures to Low Signal Quality. J. Med. Imaging Health Inform. 2015, 5, 1311–1318. [Google Scholar] [CrossRef]
- Chudacek, V.; Huptych, M.; Koucky, M.; Spilka, J.; Bauer, L.; Lhotska, L. Fetal heart rate data pre-processing and annotation. In Proceedings of the 2009 9th International Conference on Information Technology and Applications in Biomedicine, Larnaka, Cyprus, 4–7 November 2009; pp. 5–7. [Google Scholar] [CrossRef]
- Nokas, G.; Koutras, A.; Christoyannis, I.; Georgoulas, G.; Stylios, C.H.; Groumpos, P. Prediction of Missing Data in Cardiotocograms Using the Expectation Maximization AlgorithmTION ALGORITHM. In Scattering And Biomedical Engineering; World Scientific: Singapore, 2002; pp. 354–362. [Google Scholar] [CrossRef]
- Cömert, Z.; Kocamaz, A.F. Fetal Hypoxia Detection Based on Deep Convolutional Neural Network with Transfer Learning Approach. Adv. Intell. Syst. Comput. 2019, 763, 239–248. [Google Scholar] [CrossRef]
- Fergus, P.; Selvaraj, M.; Chalmers, C. Machine learning ensemble modelling to classify caesarean section and vaginal delivery types using Cardiotocography traces. Comput. Biol. Med. 2018, 93, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Comert, Z.; Yang, Z.; Velappan, S.; Boopathi, A.M.; Kocamaz, A.F. Performance evaluation of Empirical Mode Decomposition and Discrete Wavelet Transform for computerized hypoxia detection and prediction. In Proceedings of the 26th Signal Processing and Communications Applications Conference (SIU), Malatya, Turkey, 16–17 September 2017; pp. 1–4. [Google Scholar] [CrossRef]
- Feng, G.; Quirk, J.G.; Djuric, P.M. Recovery of missing samples in fetal heart rate recordings with Gaussian processes. In Proceedings of the 25th European Signal Processing Conference (EUSIPCO), Kos, Greece, 28 August–2 September 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 261–265. [Google Scholar] [CrossRef]
- Tan, W.; Liu, L. Truncated normal distribution-based EWMA control chart for monitoring the process mean in the presence of outliers. J. Stat. Comput. Simul. 2021, 91, 2276–2288. [Google Scholar] [CrossRef]
- Zhao, Z.; Deng, Y.; Zhang, Y.; Zhang, Y.; Zhang, X.; Shao, L. DeepFHR: Intelligent prediction of fetal Acidemia using fetal heart rate signals based on convolutional neural network. BMC Med. Inform. Decis. Mak. 2019, 19, 286. [Google Scholar] [CrossRef]
- Tang, H.; Wang, T.; Li, M.; Yang, X. The Design and Implementation of Cardiotocography Signals Classification Algorithm Based on Neural Network. Comput. Math. Methods Med. 2018, 2018, 8568617. [Google Scholar] [CrossRef]
- Georgoulas, G.; Karvelis, P.; Spilka, J.; Chudáček, V.; Stylios, C.D.; Lhotská, L. Investigating pH based evaluation of fetal heart rate (FHR) recordings. Health Technol. 2017, 7, 241–254. [Google Scholar] [CrossRef]
- Krupa, B.N.; Ali, M.A.M.; Zahedi, E. The application of empirical mode decomposition for the enhancement of cardiotocograph signals. Physiol. Meas. 2009, 30, 729–743. [Google Scholar] [CrossRef]
- Jezewski, J.; Kupka, T.; Horoba, K. Extraction of Fetal Heart-Rate Signal as the Time Event Series From Evenly Sampled Data Acquired Using Doppler Ultrasound Technique. IEEE Trans. Biomed. Eng. 2008, 55, 805–810. [Google Scholar] [CrossRef]
- Papadimitriou, S.; Bezerianos, A. Nonlinear analysis of the performance and reliability of wavelet singularity detection based denoising for doppler ultrasound fetal heart rate signals. Int. J. Med. Inform. 1999, 53, 43–60. [Google Scholar] [CrossRef]
- Papadimitriou, S.; Gatzounas, D.; Papadopoulos, V.; Tzigounis, V.; Bezerianos, A. Denoising of the fetal heart rate signal with non-linear filtering of the wavelet transform maxima. Int. J. Med. Inform. 1997, 44, 177–192. [Google Scholar] [CrossRef] [PubMed]
- Warrick, P.A.; Hamilton, E.F. Subspace detection of the impulse response function from intra-partum cardiotocography. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 5678–5681. [Google Scholar] [CrossRef]
- Papadimitriou, S.; Papadopoulos, V.; Gatzounas, D.; Tzigounis, V.; Bezerianos, A. The Performance and Reliability of Wavelet Denoising for Doppler Ultrasound Fetal Heart Rate Signal Preprocessing. Stud. Health Technol. Inform. 1997, 43, 561–565. [Google Scholar]
- Spilka, J.; Chudáček, V.; Koucký, M.; Lhotská, L.; Huptych, M.; Janků, P.; Georgoulas, G.; Stylios, C. Using nonlinear features for fetal heart rate classification. Biomed. Signal Process Control 2012, 7, 350–357. [Google Scholar] [CrossRef]
- Romano, M.; Bifulco, P.; Ruffo, M.; Improta, G.; Clemente, F.; Cesarelli, M. Software for computerised analysis of cardiotocographic traces. Comput. Methods Programs Biomed. 2016, 124, 121–137. [Google Scholar] [CrossRef] [PubMed]
- Urdal, J.; Engan, K.; Eftestol, T.C.; Yarrot, L.B.; Hussein, K.; Ersdal, H.L. Noise and Contraction Detection using Fetal Heart Rate and Accelerometer Signals During Labour. In Proceedings of the 17th Scandinavian Conference on Health Informatics, Oslo, Norway, 12–13 November 2019. [Google Scholar]
- Oikonomou, V.P.; Spilka, J.; Stylios, C.; Lhostka, L. An adaptive method for the recovery of missing samples from FHR time series. In Proceedings of the 26th IEEE International Symposium on Computer-Based Medical Systems, Porto, Portugal, 20–22 June 2013; IEEE: Piscataway, NJ, USA, 2013; pp. 337–342. [Google Scholar] [CrossRef]
- Nunes, I.; Ayres-de-Campos, D.; Costa-Santos, C.; Bernardes, J. Differences between external and internal fetal heart rate monitoring during the second stage of labor: A prospective observational study. J. Perinat. Med. 2014, 42, 493–498. [Google Scholar] [CrossRef]
- Warrick, P.A.; Hamilton, E.F.; Precup, D.; Kearney, R.E. Identification of the Dynamic Relationship Between Intrapartum Uterine Pressure and Fetal Heart Rate for Normal and Hypoxic Fetuses. IEEE Trans. Biomed. Eng. 2009, 56, 1587–1597. [Google Scholar] [CrossRef] [PubMed]
- Urdal, J.; Engan, K.; Eftestøl, T.; Haaland, S.H.; Kamala, B.; Mdoe, P.; Kidanto, H.; Ersdal, H. Fetal heart rate development during labour. Biomed. Eng. Online 2021, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Cesarelli, M.; Romano, M.; Bifulco, P.; Fedele, F.; Bracale, M. An algorithm for the recovery of fetal heart rate series from CTG data. Comput. Biol. Med. 2007, 37, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.; Lake, D.E.; Chrisholm, C.A.; Ferguson, J.E.; Griffin, M.P.; Moorman, J.R. Toward quantitative monitoring of human cardiotocography during labor. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (IEEE Cat. No.03CH37439), Cancun, Mexico, 17–21 September 2003; IEEE: Piscataway, NJ, USA, 2003; pp. 236–239. [Google Scholar] [CrossRef]
- Felgueiras, C.S.; de Sá, J.P.M.; Bernardes, J.; Gama, S. On the Reconstruction of Fetal Heart Rate Sequences. In Proceedings of the IV Portuguese Conf. on Biomedical Engineering. BIOENG’96, Aveiro, Portugal, 18–19 April 1996. [Google Scholar]
- Peters, C.H.L.; Broeke, E.D.M.T.; Andriessen, P.; Vermeulen, B.; Berendsen, R.C.M.; Wijn, P.F.F.; Oei, S.G. Beat-to-beat detection of fetal heart rate: Doppler ultrasound cardiotocography compared to direct ECG cardiotocography in time and frequency domain. Physiol. Meas. 2004, 25, 585–593. [Google Scholar] [CrossRef]
- Peters, C.H.L.; Vullings, R.; Rooijakkers, M.J.; Bergmans, J.W.M.; Oei, S.G.; Wijn, P.F.F. A continuous wavelet transform-based method for time-frequency analysis of artefact-corrected heart rate variability data. Physiol. Meas. 2011, 32, 1517–1527. [Google Scholar] [CrossRef]
- Casati, D.; Stampalija, T.; Rizas, K.; Ferrazzi, E.; Mastroianni, C.; Rosti, E.; Bauer, A. Assessment of Coupling between Trans-Abdominally Acquired Fetal ECG and Uterine Activity by Bivariate Phase-Rectified Signal Averaging Analysis. PLoS ONE 2014, 9, 4. [Google Scholar] [CrossRef]
- Hasan, M.; Reaz, M.; Ibrahimy, M.; Hussain, M.; Uddin, J. Detection and Processing Techniques of FECG Signal for Fetal Monitoring. Biol. Proced. Online 2009, 11, 263–295. [Google Scholar] [CrossRef]
- Sarafan, S.; Le, T.; Naderi, A.M.; Nguyen, Q.D.; Kuo BT, Y.; Ghirmai, T.; Han, H.D.; Lau, M.P.H.; Cao, H. Investigation of Methods to Extract Fetal Electrocardiogram from the Mother’s Abdominal Signal in Practical Scenarios. Technologies 2020, 8, 33. [Google Scholar] [CrossRef]
- Sbrollini, A.; Strazza, A.; Caragiuli, M.; Mozzoni, C.; Tomassini, S.; Agostinelli, A.; Morettini, M.; Fioretti, S.; Di Nardo, F.; Burattini, L. Fetal Phonocardiogram Denoising by Wavelet Transformation: Robustness to Noise. In Proceedings of the 2017 Computing in Cardiology (CinC), Rennes, France, 24–27 September 2017; IEEE: Piscataway, NJ, USA, 2017. [Google Scholar] [CrossRef]
- Jaros, R.; Martinek, R.; Kahankova, R.; Fajkus, M.; Nedoma, J. Use of a FIR filter for fetal phonocardiography processing. In Proceedings of the 2018 IEEE 20th International Conference on e-Health Networking, Applications and Services (Healthcom), Ostrava, Czech Republic, 17–20 September 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 1–6. [Google Scholar] [CrossRef]
- Ibrahim, E.A.; Al Awar, S.; Balayah, Z.H.; Hadjileontiadis, L.J.; Khandoker, A.H. A Comparative Study on Fetal Heart Rates Estimated from Fetal Phonography and Cardiotocography. Front. Physiol. 2017, 8, 302279. [Google Scholar] [CrossRef]
- Chourasia, V.S.; Mittra, A.K. Selection of mother wavelet and denoising algorithm for analysis of foetal phonocardiographic signals. J. Med. Eng. Technol. 2009, 33, 442–448. [Google Scholar] [CrossRef]
- Koutsiana, E.; Hadjileontiadis, L.; Khandoker, A.; Chouvarda, I. A Comparative Phonocardiography Study: Two Wavelet Based Methods for Fetal Heart Sound Detection. In Proceedings of the 2018 Computing in Cardiology Conference (CinC), Maastricht, The Netherlands, 23–26 September 2018. [Google Scholar] [CrossRef]
- Tomassini, S.; Sbrollini, A.; Strazza, A.; Sameni, R.; Marcantoni, I.; Morettini, M.; Burattini, L. AdvFPCG-Delineator: Advanced delineator for fetal phonocardiography. Biomed. Signal. Process Control 2020, 61, 102021. [Google Scholar] [CrossRef]
- Wang, Z.; Wei, J.; Li, X.; Liu, Z.; Su, F. Adaptive SVR Denoising Algorithm for Fetal Monitoring System. In Proceedings of the 2018 10th International Conference on Wireless Communications and Signal Processing (WCSP), Hangzhou, China, 18–20 October 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 1–5. [Google Scholar] [CrossRef]
- Martinek, R.; Barnova, K.; Jaros, R.; Kahankova, R.; Kupka, T.; Jezewski, M.; Czabanski, R.; Matonia, A.; Jezewski, J.; Horoba, K. Passive Fetal Monitoring by Advanced Signal Processing Methods in Fetal Phonocardiography. IEEE Access 2020, 8, 221942–221962. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campos, I.; Gonçalves, H.; Bernardes, J.; Castro, L. Fetal Heart Rate Preprocessing Techniques: A Scoping Review. Bioengineering 2024, 11, 368. https://doi.org/10.3390/bioengineering11040368
Campos I, Gonçalves H, Bernardes J, Castro L. Fetal Heart Rate Preprocessing Techniques: A Scoping Review. Bioengineering. 2024; 11(4):368. https://doi.org/10.3390/bioengineering11040368
Chicago/Turabian StyleCampos, Inês, Hernâni Gonçalves, João Bernardes, and Luísa Castro. 2024. "Fetal Heart Rate Preprocessing Techniques: A Scoping Review" Bioengineering 11, no. 4: 368. https://doi.org/10.3390/bioengineering11040368
APA StyleCampos, I., Gonçalves, H., Bernardes, J., & Castro, L. (2024). Fetal Heart Rate Preprocessing Techniques: A Scoping Review. Bioengineering, 11(4), 368. https://doi.org/10.3390/bioengineering11040368