
A Comparison of Heart Pulsations Provided by Forcecardiography and Double Integration of Seismocardiogram





Abstract
:1. Introduction
2. Materials and Methods
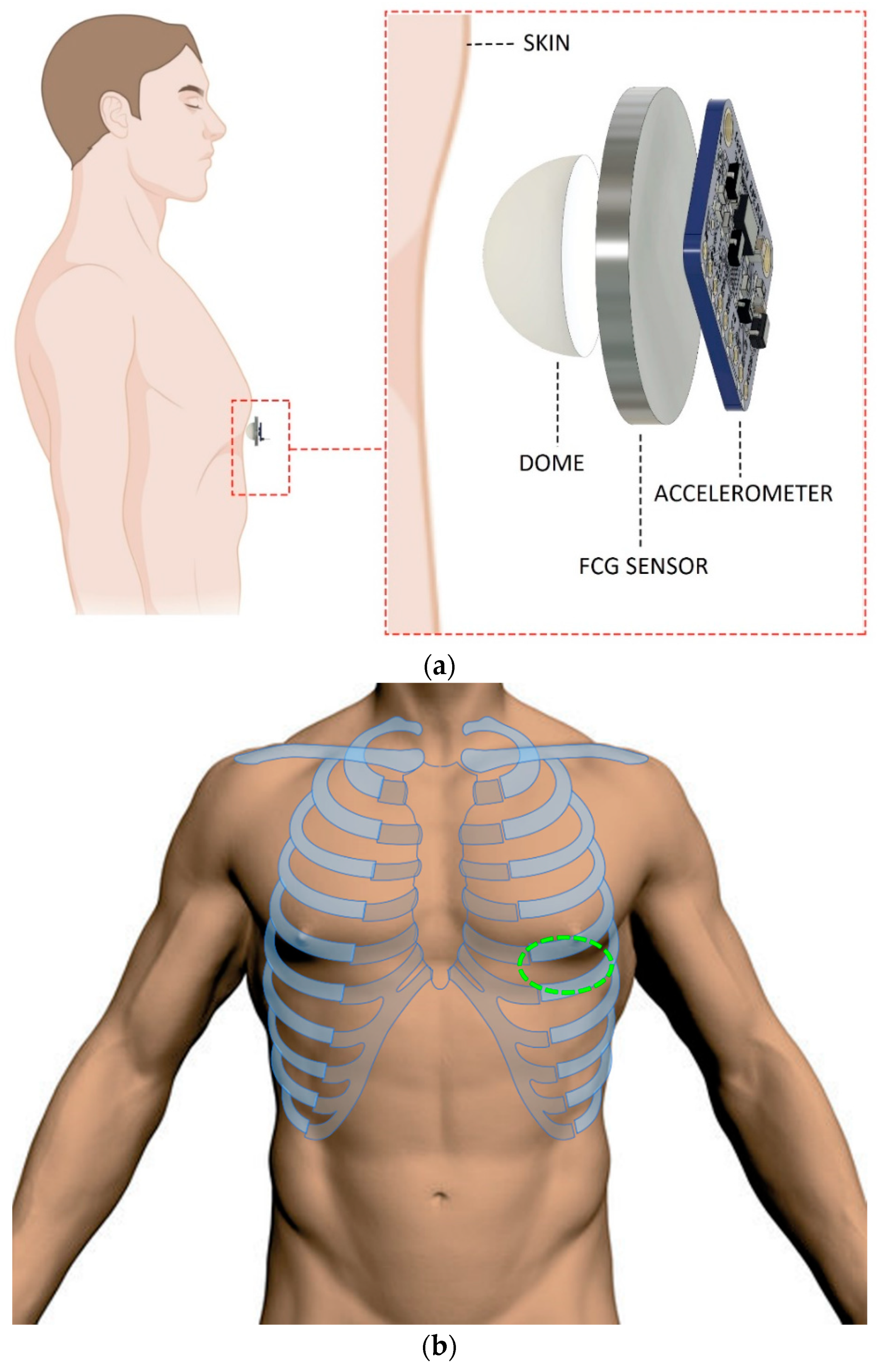
2.1. FCG and SCG Sensors
2.2. Measurement Setup and Protocol
2.3. Signals Processing
2.3.1. FCG Sensor Signals Processing
2.3.2. SCG Signals Processing
2.4. Morphological Comparison
2.5. Statistical Analyses
3. Results
3.1. Morphological Comparison of LF-FCG and LF-DSCG Signals
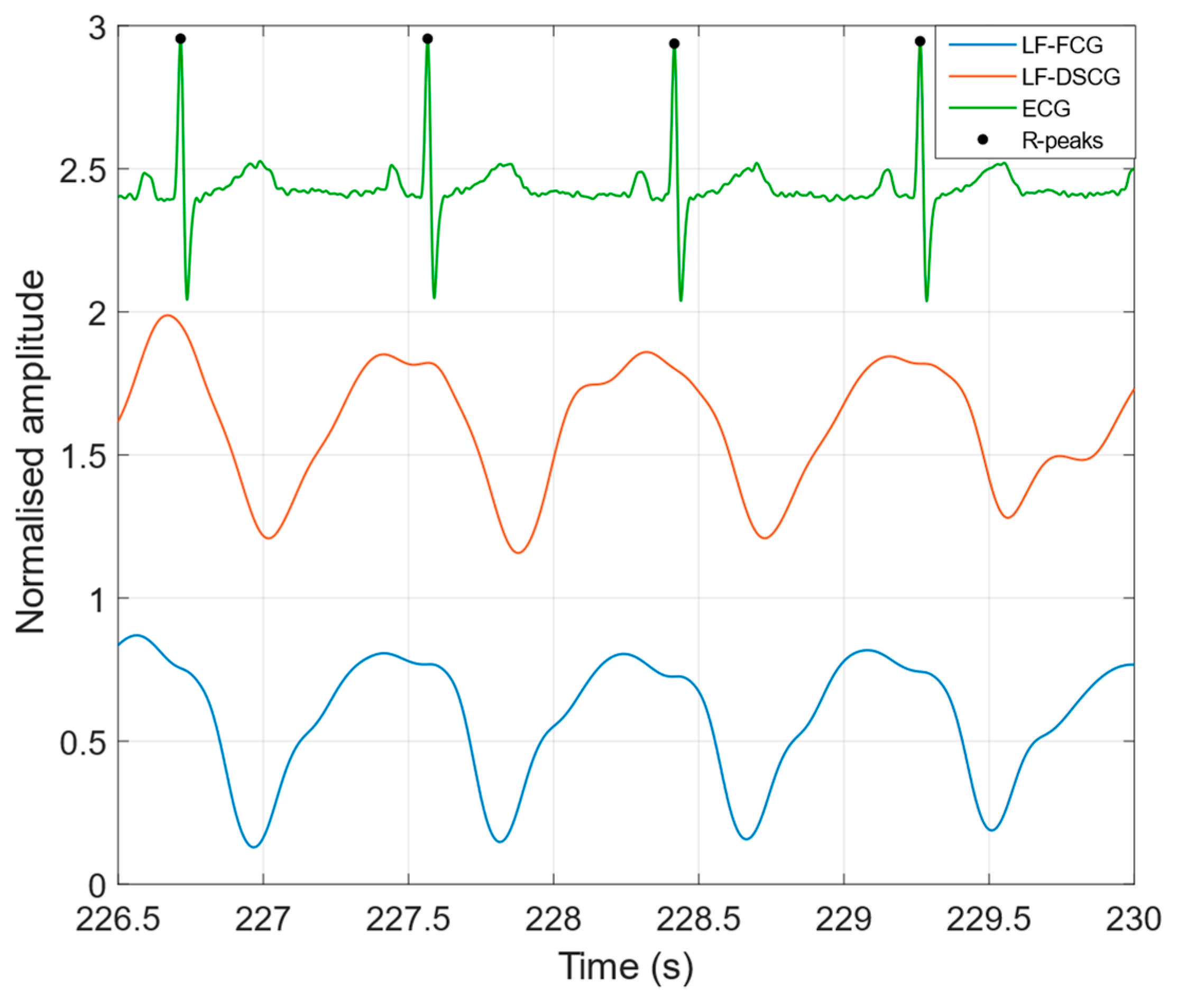
3.1.1. Apnea
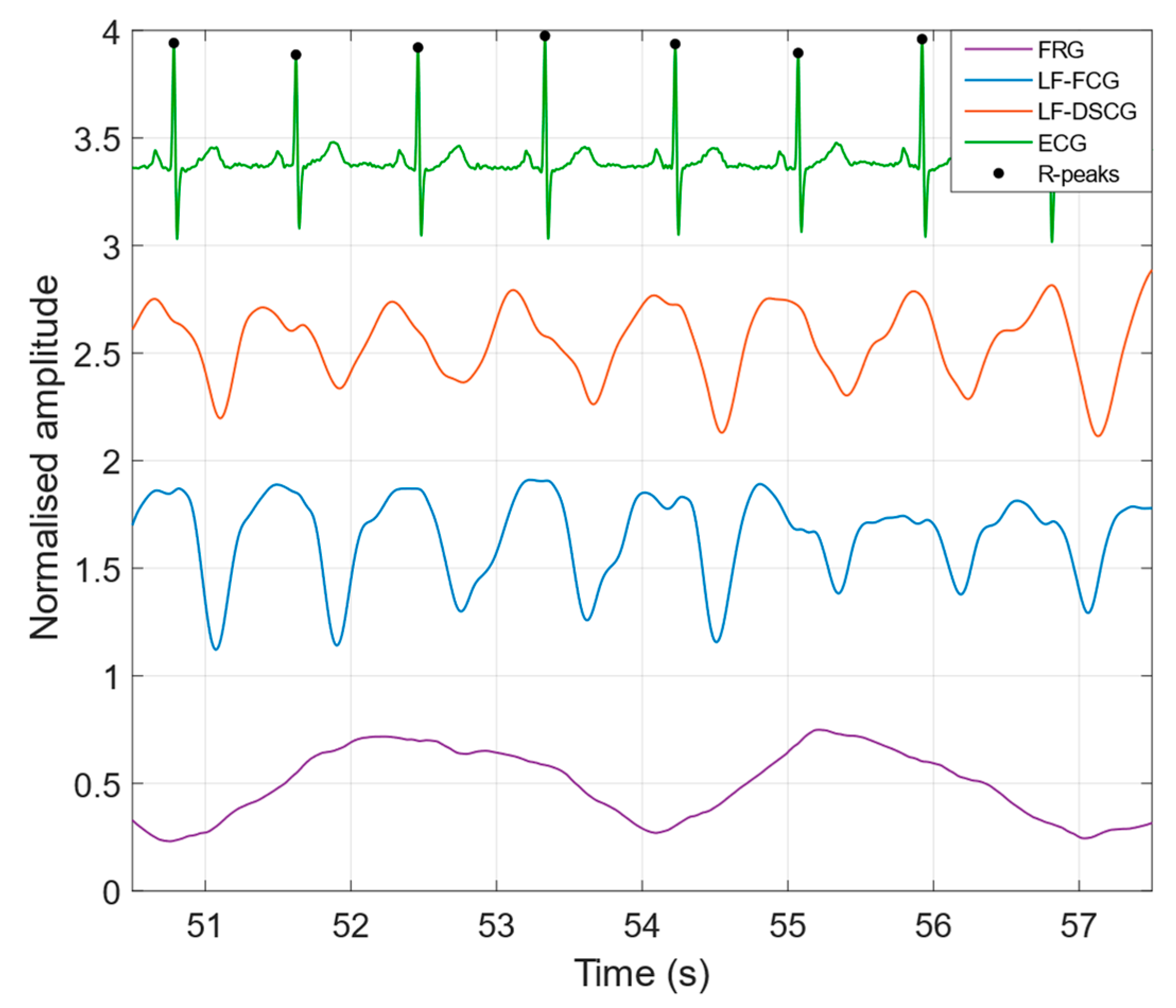
3.1.2. Quiet Breathing
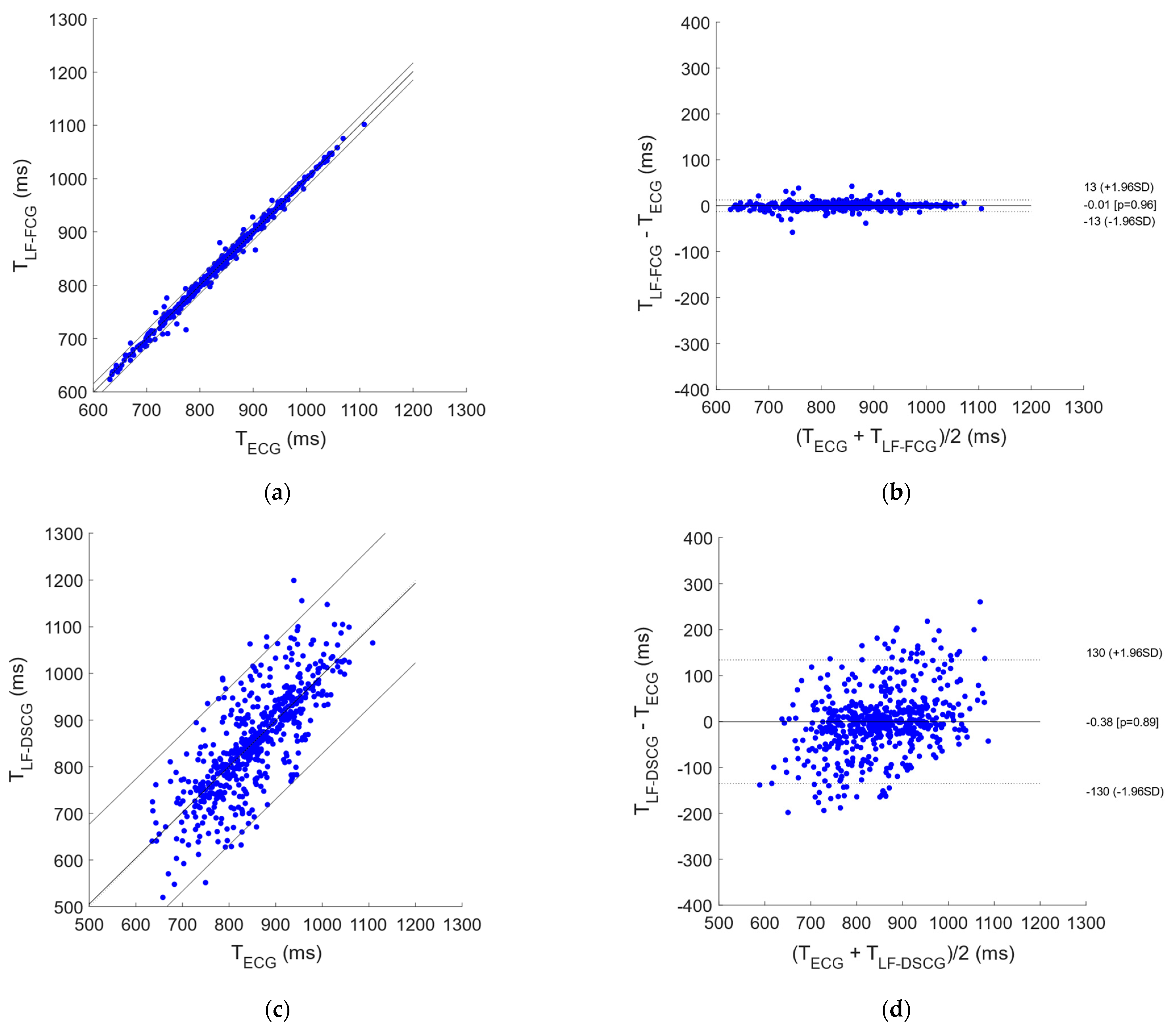
3.2. Statistical Analyses
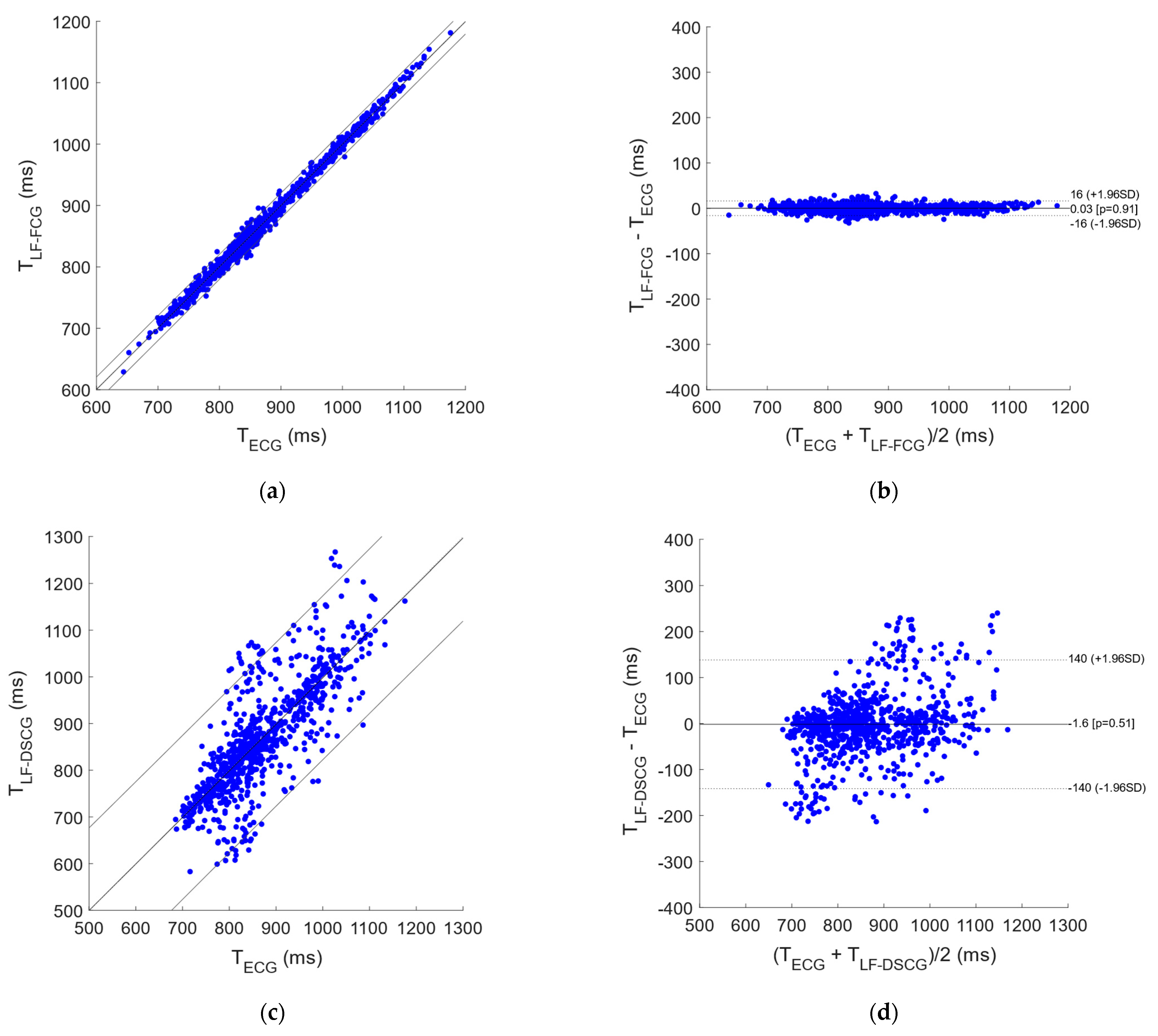
3.2.1. Apnea
3.2.2. Quiet Breathing
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marey, E.J. La Méthode Graphique dans les Sciences Expérimentales; Masson: Paris, France, 1878. [Google Scholar]
- Gordon, J.W. On Certain Molar Movements of the Human Body Produced by the Circulation of Blood. J. Anat. Physiol. 1877, 11, 533–536. [Google Scholar] [PubMed]
- Knoop, A.A. Experimental Investigations on Ultra-Low Frequency Displacement Ballistocardiography. NASA TT F-269. NASA Contract Rep. NASA CR. National Aeronautics and Space Administration: Washington, DC, USA, 1965; pp. 1–107. Translation of: Experimentele Onderzoekingen over de Ultra-Laagfrequente Verplaatsingballistocardiografie. Master’s Thesis, Free University of Amsterdam, Amsterdam, The Netherlands, 1962. [Google Scholar]
- Luisada, A.A.; Singhal, A.; Portaluppi, F. Assessment of Left Ventricular Function by Noninvasive Methods. Adv. Cardiol. 1985, 32, 111–141. [Google Scholar] [PubMed]
- Benchimol, A.; Dimond, E.G. The Apex Cardiogram in Ischaemic Heart Disease. Heart 1962, 24, 581–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starr, I.; Rawson, A.J.; Schroeder, H.A.; Joseph, N.R. Studies on the estimation of cardiac output in man, and of abnormalities in cardiac function, from the heart’s recoil and the blood’s impacts; the ballistocardiogram. Am. J. Physiol. 1939, 127, 1–28. [Google Scholar] [CrossRef]
- Zanetti, J.; Salerno, D. Seismocardiography: A new technique for recording cardiac vibrations. Concept, method, and initial observations. J. Cardiovasc. Technol. 1990, 9, 111–118. [Google Scholar]
- Inan, O.T.; Migeotte, P.F.; Park, K.S.; Etemadi, M.; Tavakolian, K.; Casanella, R.; Zanetti, J.; Tank, J.; Funtova, I.; Prisk, G.K.; et al. Ballistocardiography and Seismocardiography: A Review of Recent Advances. IEEE J. Biomed. Health Inform. 2015, 19, 1414–1427. [Google Scholar] [CrossRef] [Green Version]
- Taebi, A.; Solar, B.E.; Bomar, A.J.; Sandler, R.H.; Mansy, H.A. Recent Advances in Seismocardiography. Vibration 2019, 2, 64–86. [Google Scholar] [CrossRef] [Green Version]
- Bifulco, P.; Gargiulo, G.D.; D’Angelo, G.; Liccardo, A.; Romano, M.; Clemente, F.; Cesarelli, M. Monitoring of respiration, seismocardiogram and heart sounds by a PVDF piezo film sensor. In Proceedings of the 20th IMEKO TC4 Symposium on Measurements of Electrical Quantities: Research on Electrical and Electronic Measurement for the Economic Upturn, Together with 18th TC4 International Workshop on ADC and DCA Modeling and Testing, Benevento, Italy, 15–17 September 2014; pp. 786–789. [Google Scholar]
- Andreozzi, E.; Fratini, A.; Esposito, D.; Naik, G.; Polley, C.; Gargiulo, G.D.; Bifulco, P. Forcecardiography: A Novel Technique to Measure Heart Mechanical Vibrations onto the Chest Wall. Sensors 2020, 20, 3885. [Google Scholar] [CrossRef]
- Esposito, D.; Andreozzi, E.; Fratini, A.; Gargiulo, G.; Savino, S.; Niola, V.; Bifulco, P. A Piezoresistive Sensor to Measure Muscle Contraction and Mechanomyography. Sensors 2018, 18, 2553. [Google Scholar] [CrossRef] [Green Version]
- Esposito, D.; Andreozzi, E.; Gargiulo, G.D.; Fratini, A.; D’Addio, G.; Naik, G.R.; Bifulco, P. A Piezoresistive Array Armband with Reduced Number of Sensors for Hand Gesture Recognition. Front. Neurorobot. 2020, 13. [Google Scholar] [CrossRef] [Green Version]
- Esposito, D.; Gargiulo, G.D.; Parajuli, N.; Cesarelli, G.; Andreozzi, E.; Bifulco, P. Measurement of muscle contraction timing for prosthesis control: A comparison between electromyography and force-myography. In Proceedings of the 2020 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Bari, Italy, 1 June–1 July 2020. [Google Scholar] [CrossRef]
- Andreozzi, E.; Centracchio, J.; Punzo, V.; Esposito, D.; Polley, C.; Gargiulo, G.D.; Bifulco, P. Respiration Monitoring via Forcecardiography Sensors. Sensors 2021, 21, 3996. [Google Scholar] [CrossRef] [PubMed]
- Andreozzi, E.; Gargiulo, G.D.; Esposito, D.; Bifulco, P. A Novel Broadband Forcecardiography Sensor for Simultaneous Monitoring of Respiration, Infrasonic Cardiac Vibrations and Heart Sounds. Front. Physiol. 2021, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Centracchio, J.; Andreozzi, E.; Esposito, D.; Gargiulo, G.D.; Bifulco, P. Detection of Aortic Valve Opening and Estimation of Pre-Ejection Period in Forcecardiography Recordings. Bioengineering 2022, 9, 89. [Google Scholar] [CrossRef]
- Savitzky, A.; Golay, M.J.E. Smoothing and Differentiation of Data by Simplified Least Squares Procedures. Anal. Chem. 1964, 36, 1627–1639. [Google Scholar] [CrossRef]
- Sedghamiz, H. BioSigKit: A Matlab Toolbox and Interface for Analysis of BioSignals. J. Open Source Softw. 2018, 3, 671. [Google Scholar] [CrossRef]
- Ran, K. Bland-Altman and Correlation Plot, MATLAB Central File Exchange. 2020. Available online: https://www.mathworks.com/matlabcentral/fileexchange/45049-bland-altman-and-correlation-plot (accessed on 28 May 2020).
- Coulshed, N.; Epstein, E.J. The apex cardiogram: Its normal features explained by those found in heart disease. Heart 1963, 25, 697–708. [Google Scholar] [CrossRef] [Green Version]
- Rios, J.C.; Massumi, R.A. Correlation between the apex cardiogram and left ventricular pressure. Am. J. Cardiol. 1965, 15, 647–655. [Google Scholar] [CrossRef]
- Tavel, M.E.; Campbell, R.W.; Feigenbaum, H.; Steinmetz, E.F. The apex cardiogram and its relationship to haemodynamic events within the left heart. Heart 1965, 27, 829–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voigt, G.C.; Friesinger, G.C. The Use of Apexcardiography in the Assessment of Left Ventricular Diastolic Pressure. Circulation 1970, 41, 1015–1024. [Google Scholar] [CrossRef] [Green Version]
- Willems, J.L.; De Geest, H.; Kesteloot, H. On the value of apex cardiography for timing intracardiac events. Am. J. Cardiol. 1971, 28, 59–66. [Google Scholar] [CrossRef]
- Manolas, J.; Rutishauser, W.; Wirz, P.; Arbenz, U. Time relation between apex cardiogram and left ventricular events using simultaneous high-fidelity tracings in man. Heart 1975, 37, 1263–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manolas, J.; Krayenbuehl, H.P. Comparison between apexcardiographic and angiographic indexes of left ventricular performance in patients with aortic incompetence. Circulation 1978, 57, 692–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manolas, J.; Rutishauser, W. Diastolic amplitude time index: A new apexcardiographic index of left ventricular diastolic function in human beings. Am. J. Cardiol. 1981, 48, 736–745. [Google Scholar] [CrossRef]
- Thong, Y.K.; Woolfson, M.S.; Crowe, J.A.; Hayes-Gill, B.R.; Jones, D.A. Numerical double integration of acceleration measurements in noise. Measurement 2004, 36, 73–92. [Google Scholar] [CrossRef]
- Migeotte, P.-F.; Mucci, V.; Delière, Q.; Lejeune, L.; van de Borne, P. Multi-dimensional Kineticardiography a New Approach for Wearable Cardiac Monitoring Through Body Acceleration Recordings. In Proceedings of the XIV Mediterranean Conference on Medical and Biological Engineering and Computing 2016, MEDICON 2016, Paphos, Cyprus, 31 March–2 April 2016; Springer International Publishing: Cham, Switzerland, 2016; pp. 1119–1124. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Whole Signals | Single Heartbeats | Ensemble Averages | |
|---|---|---|---|---|
| Mean | SD | |||
| #1 | 0.6003 | 0.7782 | 0.1574 | 0.9647 |
| #2 | 0.8961 | 0.9132 | 0.04177 | 0.9470 |
| #3 | 0.9315 | 0.9423 | 0.02863 | 0.9507 |
| #4 | 0.9473 | 0.9496 | 0.01551 | 0.9556 |
| #5 | 0.7300 | 0.7932 | 0.07253 | 0.8341 |
| Subject | Whole Signals | Single Heartbeats | Ensemble Averages | |
|---|---|---|---|---|
| Mean | SD | |||
| #1 | 0.7125 | 0.7919 | 0.1232 | 0.8728 |
| #2 | 0.7840 | 0.8248 | 0.1085 | 0.9262 |
| #3 | 0.8060 | 0.8244 | 0.1195 | 0.9251 |
| #4 | 0.7649 | 0.8145 | 0.1040 | 0.9012 |
| #5 | 0.5166 | 0.7739 | 0.1306 | 0.8728 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andreozzi, E.; Centracchio, J.; Esposito, D.; Bifulco, P. A Comparison of Heart Pulsations Provided by Forcecardiography and Double Integration of Seismocardiogram. Bioengineering 2022, 9, 167. https://doi.org/10.3390/bioengineering9040167
Andreozzi E, Centracchio J, Esposito D, Bifulco P. A Comparison of Heart Pulsations Provided by Forcecardiography and Double Integration of Seismocardiogram. Bioengineering. 2022; 9(4):167. https://doi.org/10.3390/bioengineering9040167
Chicago/Turabian StyleAndreozzi, Emilio, Jessica Centracchio, Daniele Esposito, and Paolo Bifulco. 2022. "A Comparison of Heart Pulsations Provided by Forcecardiography and Double Integration of Seismocardiogram" Bioengineering 9, no. 4: 167. https://doi.org/10.3390/bioengineering9040167
APA StyleAndreozzi, E., Centracchio, J., Esposito, D., & Bifulco, P. (2022). A Comparison of Heart Pulsations Provided by Forcecardiography and Double Integration of Seismocardiogram. Bioengineering, 9(4), 167. https://doi.org/10.3390/bioengineering9040167