
Influenza- and COVID-19-Associated Pulmonary Aspergillosis: Are the Pictures Different?

 , , , , , , , , ,
, , , , , , , , ,  , ,
, ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. Populations
2.2. Detection of Aspergillus in Respiratory Samples by Culture and PCR
2.3. Detection of Aspergillus Galactomannan (GM) in Blood and Respiratory Samples
2.4. Imaging
2.5. Therapeutic Drug Monitoring
2.6. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Taccone, F.S.; Van den Abeele, A.-M.; Bulpa, P.; Misset, B.; Meersseman, W.; Cardoso, T.; Paiva, J.-A.; Blasco-Navalpotro, M.; De Laere, E.; Dimopoulos, G.; et al. Epidemiology of Invasive Aspergillosis in Critically Ill Patients: Clinical Presentation, Underlying Conditions, and Outcomes. Crit. Care 2015, 19, 7. [Google Scholar] [CrossRef] [Green Version]
- Blot, S.I.; Taccone, F.S.; Van den Abeele, A.-M.; Bulpa, P.; Meersseman, W.; Brusselaers, N.; Dimopoulos, G.; Paiva, J.A.; Misset, B.; Rello, J.; et al. A Clinical Algorithm to Diagnose Invasive Pulmonary Aspergillosis in Critically Ill Patients. Am. J. Respir. Crit. Care Med. 2012, 186, 56–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loughlin, L.; Hellyer, T.P.; White, P.L.; McAuley, D.F.; Conway Morris, A.; Posso, R.B.; Richardson, M.D.; Denning, D.W.; Simpson, A.J.; McMullan, R. Pulmonary Aspergillosis in Patients with Suspected Ventilator-Associated Pneumonia in UK ICUs. Am. J. Respir. Crit. Care Med. 2020, 202, 1125–1132. [Google Scholar] [CrossRef] [PubMed]
- Maertens, J.; Theunissen, K.; Verbeken, E.; Lagrou, K.; Verhaegen, J.; Boogaerts, M.; Eldere, J.V. Prospective Clinical Evaluation of Lower Cut-Offs for Galactomannan Detection in Adult Neutropenic Cancer Patients and Haematological Stem Cell Transplant Recipients. Br. J. Haematol. 2004, 126, 852–860. [Google Scholar] [CrossRef]
- Bassetti, M.; Giacobbe, D.R.; Grecchi, C.; Rebuffi, C.; Zuccaro, V.; Scudeller, L. FUNDICU investigators Performance of Existing Definitions and Tests for the Diagnosis of Invasive Aspergillosis in Critically Ill, Adult Patients: A Systematic Review with Qualitative Evidence Synthesis. J. Infect. 2020, 81, 131–146. [Google Scholar] [CrossRef]
- Verweij, P.E.; Rijnders, B.J.A.; Brüggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Calandra, T.; Clancy, C.J.; Cornely, O.A.; Chiller, T.; et al. Review of Influenza-Associated Pulmonary Aspergillosis in ICU Patients and Proposal for a Case Definition: An Expert Opinion. Intensive Care Med. 2020, 46, 1524–1535. [Google Scholar] [CrossRef] [PubMed]
- Schauwvlieghe, A.F.A.D.; Rijnders, B.J.A.; Philips, N.; Verwijs, R.; Vanderbeke, L.; Van Tienen, C.; Lagrou, K.; Verweij, P.E.; Van de Veerdonk, F.L.; Gommers, D.; et al. Invasive Aspergillosis in Patients Admitted to the Intensive Care Unit with Severe Influenza: A Retrospective Cohort Study. Lancet Respir. Med. 2018, 6, 782–792. [Google Scholar] [CrossRef]
- Rutsaert, L.; Steinfort, N.; Van Hunsel, T.; Bomans, P.; Naesens, R.; Mertes, H.; Dits, H.; Van Regenmortel, N. COVID-19-Associated Invasive Pulmonary Aspergillosis. Ann. Intensive Care 2020, 10, 71. [Google Scholar] [CrossRef]
- Maes, M.; Higginson, E.; Pereira-Dias, J.; Curran, M.D.; Parmar, S.; Khokhar, F.; Cuchet-Lourenço, D.; Lux, J.; Sharma-Hajela, S.; Ravenhill, B.; et al. Ventilator-Associated Pneumonia in Critically Ill Patients with COVID-19. Crit. Care 2021, 25, 25. [Google Scholar] [CrossRef]
- Wauters, J.; Baar, I.; Meersseman, P.; Meersseman, W.; Dams, K.; De Paep, R.; Lagrou, K.; Wilmer, A.; Jorens, P.; Hermans, G. Invasive Pulmonary Aspergillosis Is a Frequent Complication of Critically Ill H1N1 Patients: A Retrospective Study. Intensive Care Med. 2012, 38, 1761–1768. [Google Scholar] [CrossRef]
- White, P.L.; Dhillon, R.; Cordey, A.; Hughes, H.; Faggian, F.; Soni, S.; Pandey, M.; Whitaker, H.; May, A.; Morgan, M.; et al. A National Strategy to Diagnose COVID-19 Associated Invasive Fungal Disease in the ICU. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Bartoletti, M.; Pascale, R.; Cricca, M.; Rinaldi, M.; Maccaro, A.; Bussini, L.; Fornaro, G.; Tonetti, T.; Pizzilli, G.; Francalanci, E.; et al. Epidemiology of Invasive Pulmonary Aspergillosis among COVID-19 Intubated Patients: A Prospective Study. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Cornely, O.A.; Böttiger, B.W.; Dusse, F.; Eichenauer, D.A.; Fuchs, F.; Hallek, M.; Jung, N.; Klein, F.; Persigehl, T.; et al. COVID-19 Associated Pulmonary Aspergillosis. Mycoses 2020, 63, 528–534. [Google Scholar] [CrossRef]
- van Arkel, A.L.E.; Rijpstra, T.A.; Belderbos, H.N.A.; van Wijngaarden, P.; Verweij, P.E.; Bentvelsen, R.G. COVID-19-Associated Pulmonary Aspergillosis. Am. J. Respir. Crit. Care Med. 2020, 202, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Gangneux, J.P. Characterization of fungal infections in COVID-19 infected and mechanically ventilated patients in ICU: The MY-CO-VID clinical trial. In Proceedings of the Data Presented during the Réunion Interdisciplinaire de Chimiothérapie Infectieuse (RICAI Congress), Paris, France, 14–15 December 2020. [Google Scholar]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and Managing COVID-19-Associated Pulmonary Aspergillosis: The 2020 ECMM/ISHAM Consensus Criteria for Research and Clinical Guidance. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Verweij, P.E.; Gangneux, J.-P.; Bassetti, M.; Brüggemann, R.J.M.; Cornely, O.A.; Koehler, P.; Lass-Flörl, C.; van de Veerdonk, F.L.; Chakrabarti, A.; Hoenigl, M.; et al. Diagnosing COVID-19-Associated Pulmonary Aspergillosis. Lancet Microbe 2020, 1, e53–e55. [Google Scholar] [CrossRef]
- Gangneux, J.-P.; Bougnoux, M.-E.; Dannaoui, E.; Cornet, M.; Zahar, J.R. Invasive Fungal Diseases during COVID-19: We Should Be Prepared. J. Mycol. Med. 2020, 30, 100971. [Google Scholar] [CrossRef] [PubMed]
- Gangneux, J.-P.; Reizine, F.; Guegan, H.; Pinceaux, K.; Le Balch, P.; Prat, E.; Pelletier, R.; Belaz, S.; Le Souhaitier, M.; Le Tulzo, Y.; et al. Is the COVID-19 Pandemic a Good Time to Include Aspergillus Molecular Detection to Categorize Aspergillosis in ICU Patients? A Monocentric Experience. J. Fungi (Basel) 2020, 6, 105. [Google Scholar] [CrossRef] [PubMed]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Cassagne, C.; Ranque, S.; Normand, A.-C.; Fourquet, P.; Thiebault, S.; Planard, C.; Hendrickx, M.; Piarroux, R. Mould Routine Identification in the Clinical Laboratory by Matrix-Assisted Laser Desorption Ionization Time-of-Flight Mass Spectrometry. PLoS ONE 2011, 6, e28425. [Google Scholar] [CrossRef] [PubMed]
- Normand, A.C.; Becker, P.; Gabriel, F.; Cassagne, C.; Accoceberry, I.; Gari-Toussaint, M.; Hasseine, L.; De Geyter, D.; Pierard, D.; Surmont, I.; et al. Validation of a New Web Application for Identification of Fungi by Use of Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry. J. Clin. Microbiol. 2017, 55, 2661–2670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guegan, H.; Robert-Gangneux, F.; Camus, C.; Belaz, S.; Marchand, T.; Baldeyrou, M.; Gangneux, J.-P. Improving the Diagnosis of Invasive Aspergillosis by the Detection of Aspergillus in Broncho-Alveolar Lavage Fluid: Comparison of Non-Culture-Based Assays. J. Infect. 2018, 76, 196–205. [Google Scholar] [CrossRef]
- Abdul-Aziz, M.H.; Alffenaar, J.-W.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.-A.; Pea, F.; Sjovall, F.; et al. Antimicrobial Therapeutic Drug Monitoring in Critically Ill Adult Patients: A Position Paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef] [PubMed]
- Rijnders, B.J.A.; Schauwvlieghe, A.F.A.D.; Wauters, J. Influenza-Associated Pulmonary Aspergillosis: A Local or Global Lethal Combination? Clin. Infect. Dis. 2020, 71, 1764–1767. [Google Scholar] [CrossRef]
- Herbrecht, R.; Guffroy, B.; Danion, F.; Venkatasamy, A.; Simand, C.; Ledoux, M.-P. Validation by Real-Life Data of the New Radiological Criteria of the Revised and Updated Consensus Definition for Invasive Fungal Diseases. Clin. Infect. Dis. 2020, 71, 2773–2774. [Google Scholar] [CrossRef]
- Nyga, R.; Maizel, J.; Nseir, S.; Chouaki, T.; Milic, I.; Roger, P.-A.; Van Grunderbeeck, N.; Lemyze, M.; Totet, A.; Castelain, S.; et al. Invasive Tracheobronchial Aspergillosis in Critically Ill Patients with Severe Influenza. A Clinical Trial. Am. J. Respir. Crit. Care Med. 2020, 202, 708–716. [Google Scholar] [CrossRef]
- Reizine, F.; Lesouhaitier, M.; Gregoire, M.; Pinceaux, K.; Gacouin, A.; Maamar, A.; Painvin, B.; Camus, C.; Le Tulzo, Y.; Tattevin, P.; et al. SARS-CoV-2-Induced ARDS Associates with MDSC Expansion, Lymphocyte Dysfunction, and Arginine Shortage. J. Clin. Immunol. 2021, 41, 515–525. [Google Scholar] [CrossRef]
- Le Balc’h, P.; Pinceaux, K.; Pronier, C.; Seguin, P.; Tadié, J.-M.; Reizine, F. Herpes Simplex Virus and Cytomegalovirus Reactivations among Severe COVID-19 Patients. Crit. Care 2020, 24, 530. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Imataki, O.; Yamaguchi, K.; Uemura, M.; Fukuoka, N. Voriconazole Concentration Is Inversely Correlated with Corticosteroid Usage in Immunocompromised Patients. Transpl. Infect. Dis. 2018, 20, e12886. [Google Scholar] [CrossRef]
- Maertens, J.A.; Raad, I.I.; Marr, K.A.; Patterson, T.F.; Kontoyiannis, D.P.; Cornely, O.A.; Bow, E.J.; Rahav, G.; Neofytos, D.; Aoun, M.; et al. Isavuconazole versus Voriconazole for Primary Treatment of Invasive Mould Disease Caused by Aspergillus and Other Filamentous Fungi (SECURE): A Phase 3, Randomised-Controlled, Non-Inferiority Trial. Lancet 2016, 387, 760–769. [Google Scholar] [CrossRef]
- Maertens, J.A.; Rahav, G.; Lee, D.-G.; Ponce-de-León, A.; Ramírez Sánchez, I.C.; Klimko, N.; Sonet, A.; Haider, S.; Diego Vélez, J.; Raad, I.; et al. Posaconazole versus Voriconazole for Primary Treatment of Invasive Aspergillosis: A Phase 3, Randomised, Controlled, Non-Inferiority Trial. Lancet 2021, 397, 499–509. [Google Scholar] [CrossRef]
- Gao, C.A.; Bailey, J.I.; Walter, J.M.; Coleman, J.M.; Malsin, E.S.; Argento, A.C.; Prickett, M.H.; Wunderink, R.G.; Smith, S.B. NU COVID Investigators Bronchoscopy on Intubated COVID-19 Patients Is Associated with Low Infectious Risk to Operators. Ann. Am. Thorac. Soc. 2021. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All Patients (n = 120) | All Aspergillosis Patients (n = 27) | Non Aspergillosis Patients (n = 93) | p Value | IAPA (n = 17) | CAPA (n = 10) | p Value | |
|---|---|---|---|---|---|---|---|
| Baseline characteristics | |||||||
| Age (years) | 59 (52–67) | 60 (52–69) | 59 (52–67) | 0.54 | 58 (52–63) | 72 (57–77) | 0.036 |
| Male sex | 80 (66.4%) | 17 (63%) | 63 (67.7%) | 0.21 | 11 (64.7%) | 6 (60.0%) | >0.99 |
| Current smoking | 31 (26%) | 10 (37%) | 21 (22.6%) | 0.13 | 9 (52.9%) | 1 (10.0%) | 0.12 |
| Obesity | 20 (16.6%) | 4 (15.4%) | 30 (32.3%) | 0.09 | 3 (17.6%) | 1 (10.0%) | >0.99 |
| Diabetes | 33 (27.5%) | 4 (14.8%) | 29 (31.2%) | 0.14 | 2 (11.8%) | 2 (20.0%) | 0.61 |
| Alcoholism | 20 (16.6%) | 6 (22.2%) | 14 (15.1%) | 0.39 | 5 (29.4%) | 1 (10.0%) | 0.36 |
| Immunodepression (including neoplasia) | 29 (24.1%) | 10 (37%) | 19 (20.4%) | 0.12 | 8 (47.1%) | 2 (20.0%) | 0.23 |
| Neoplasia | 19 (15.8%) | 7 (25.9%) | 12 (12.9%) | 0.13 | 6 (35.3%) | 1 (10.0%) | 0.2 |
| - Solid cancer | 3 (2.5%) | 1 (3.7%) | 2 (2.2%) | 0.53 | 1 (5.9%) | 0 (0.0%) | >0.99 |
| - HM | 16 (13.3%) | 6 (22.2%) | 10 (10.7%) | 0.19 | 5 (29.4%) | 1 (10.0%) | 0.36 |
| Chronic obstructive pulmonary disease | 17 (14.2%) | 6 (22.2%) | 11 (11.8%) | 0.17 | 6 (35.3%) | 0 (0.0%) | 0.057 |
| Chronic kidney disease | 10 (8.3%) | 2 (7.4%) | 8 (8.6%) | >0.99 | 1 (5.9%) | 1 (10.0%) | >0.99 |
| Cirrhosis | 8 (6.7%) | 4 (14.8%) | 4 (4.3%) | 0.07 | 4 (23.5%) | 0 (0.0%) | 0.26 |
| ARDS etiology | NA | NA | NA | ||||
| - Influenza | 71 (59.2%) | 17 (63%) | 54 (58.1%) | 0.65 | |||
| - COVID-19 | 49 (40.8%) | 10 (37%) | 39 (41.9%) | ||||
| Clinical and biological admission ICU data | |||||||
| Neutrophil (109/L) | 6.9 (3.9–11.4) | 8.2 (3.8–13.2) | 6.9 (4.1–11) | 0.67 | 8.0 (3.6–17.7) | 8.5 (4.1–11.0) | 0.72 |
| Lymphocyte (109/L) | 0.56 (0.32–0.87) | 0.54 (0.36–0.72) | 0.59 (0.32–0.93) | 0.44 | 0.38 (0.29–0.55) | 0.83 (0.72–0.92) | <0.0001 |
| Ratio of PaO2 to FiO2 on day 1 | 98 (67–147) | 98 (74–143) | 105 (67–148) | 0.96 | 86 (69–98) | 143 (109–154) | 0.01 |
| SAPS II score on day 1 | 44 (35–61) | 48 (36–64) | 43 (34–60) | 0.22 | 58 (42–64) | 40 (34–68) | 0.48 |
| SOFA score on day 1 | 8 (5–10) | 9 (5–12) | 7 (4–10) | 0.19 | 10 (7–13) | 5 (2–8) | 0.012 |
| Clinical course data | |||||||
| Duration of mechanical ventilation (days) | 18 (11–27) | 23 (17–40) | 17 (9–25) | 0.038 | 23 (16–49) | 23 (19–30) | 0.56 |
| ECMO | 45 (37.5%) | 13 (48.1%) | 32 (34.4%) | 0.19 | 12 (70.6%) | 1 (10.0%) | 0.004 |
| SOFA score on day 5 | 8 (6–12) | 11 (7–14) | 7 (5–11) | 0.003 | 10 (6–14) | 12 (8–13) | 0.83 |
| RRT use | 37 (30.8%) | 13 (48.1%) | 24 (25.8%) | 0.027 | 8 (47.1%) | 5 (50.0%) | >0.99 |
| Corticosteroids use | 55 (45.8%) | 19 (70.4%) | 36 (38.7%) | 0.004 | 12 (70.6%) | 7 (70.0%) | >0.99 |
| - before day 7 | 45 (81.8%) | 16 (84.2%) | 29 (80.6%) | 0.008 | 12 (100%) | 4 (57.1%) | 0.22 |
| - after day 7 | 10 (18.2%) | 3 (15.8%) | 7 (19.4%) | 0.14 | 0 (0.0%) | 3 (42.9%) | 0.04 |
| ICU length of stay (days) | 22 (12–33) | 25 (19–48) | 19 (12–30) | 0.044 | 29 (12–48) | 24 (22–29) | 0.97 |
| Death in the ICU | 28 (23.3%) | 9 (33.3%) | 19 (20.4%) | 0.16 | 6 (35.3%) | 3 (30.0%) | >0.99 |
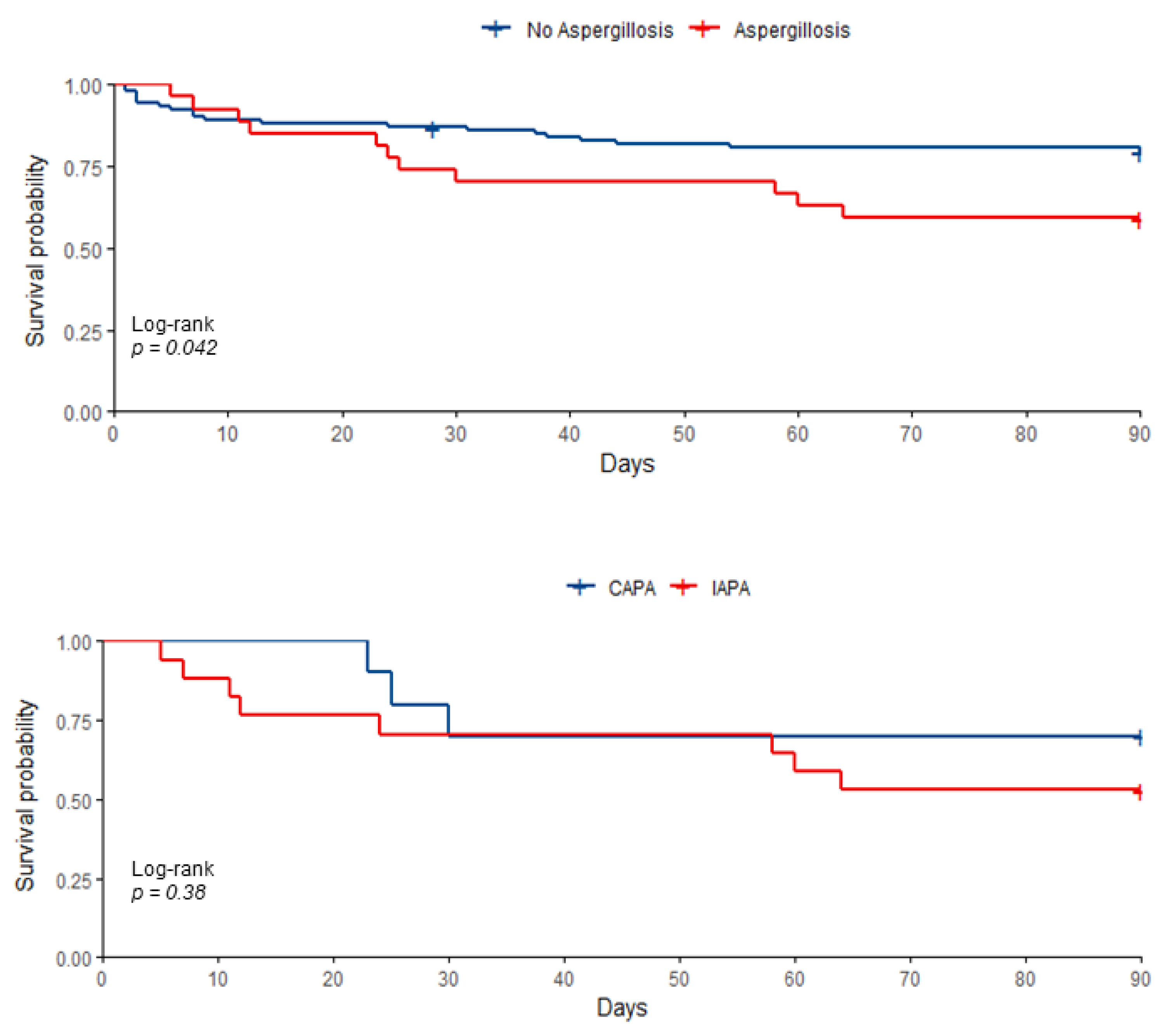
| 90-day survival | 89 (74.2%) | 16 (59.3%) | 74 (79.6%) | 0.032 | 9 (52.9%) | 7 (70.0%) | 0.44 |
| Death in hospital | 31 (25.8%) | 12 (44.4%) | 19 (20.4%) | 0.012 | 8 (47.1%) | 4 (40.0%) | 0.45 |
| All Aspergillosis Patients (n = 27) | IAPA (n = 17) | CAPA (n = 10) | p Value | |
|---|---|---|---|---|
| Temperature (°C) | 38.2 (38.0–39.0) | 38.0 (37.8–38.8) | 38.9 (38.1–39.0) | 0.19 |
| Systolic pressure (mmHg) | 92 (81–102) | 92 (85–102) | 90 (78–101) | 0.95 |
| Neutrophil count (109/L) | 9.6 (4.5–16.5) | 13.2 (5.5–19.5) | 7.6 (4.0–10.3) | 0.18 |
| Lymphocyte count (109/L) | 0.72 (0.51–1.03) | 0.80 (0.50–1.22) | 0.72 (0.55–0.80) | 0.56 |
| Ratio of PaO2 to FiO2 | 134 (102–179) | 108 (86–165) | 162 (147–208) | 0.04 |
| Septic shock | 17 (63.0%) | 12 (70.6%) | 5 (50.0%) | 0.41 |
| Need for vasopressors | 19 (70.4%) | 12 (70.6%) | 7 (70.0%) | >0.99 |
| Delay between admission and aspergillosis onset (days) | 4 (2–8) | 3 (2–5) | 6 (3–13) | 0.14 |
| Mechanical ventilation duration after aspergillosis onset (days) | 20 (9–36) | 22 (8–46) | 17 (11–23) | 0.64 |
| Antifungal therapy | 25 (92.6%) | 17 (100%) | 8 (80%) | 0.13 |
| Time to VCZ therapeutic range (days) * | 6 (4–9) | 4 (2–8) | 7 (6–32) | 0.096 |
| Delayed VCZ therapeutic range (>5 days) * | 9/18 (50%) | 4/12 (33.3%) | 5/6 (83.3%) | 0.045 |
| VTC (mg/L) * | 2.8 (1.5–5) | 3.9 (2–5.7) | 2.2 (1.1–4.4) | 0.01 |
| VTC min (mg/L) * | 1.6 (0.5–3.8) | 3.5 (1–5) | 0.8 (0.2–0.8) | 0.038 |
| VTC max (mg/L) * | 5.8 (4.5–7.2) | 6.1 (5.4–7.6) | 5.2 (3–7) | 0.23 |
| Antifungal treatment duration (days) | 42 (14–42) | 17 (14–47) | 42 (37–42) | 0.49 |
| All Aspergillosis Patients (n = 24) | IAPA (n = 14) | CAPA (n = 10) | p Value | |
|---|---|---|---|---|
| Delay between ICU admission and CT scan | 10 (4–15) | 9 (4–15) | 10 (3–15) | 0.99 |
| Delay between IPA diagnosis and CT scan | 5 (0–9) | 4 (0–9) | 7 (0–9) | 0.75 |
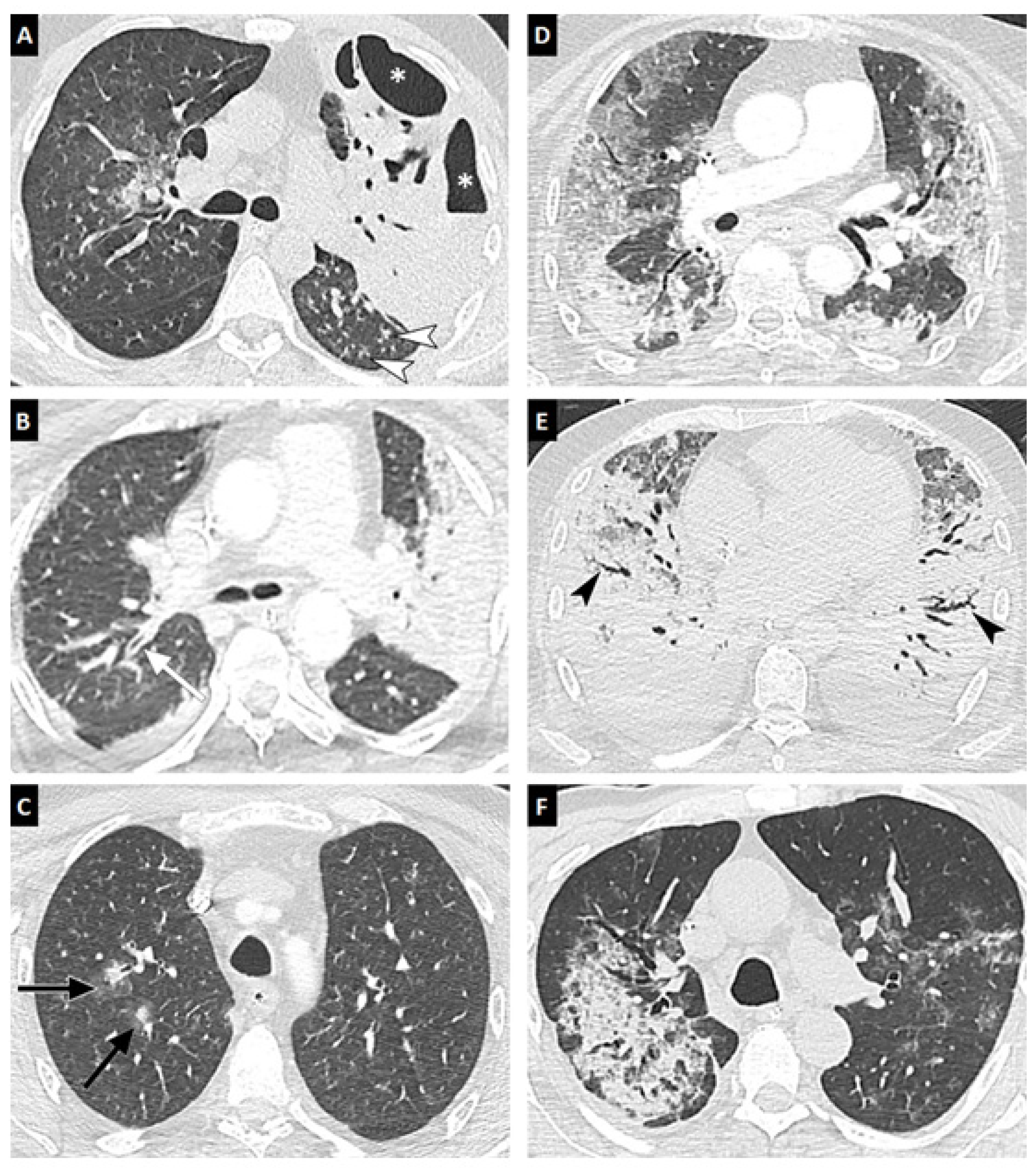
| Diffuse reticular or alveolar opacities | 24 (100%) | 14 (100%) | 10 (100%) | 0.99 |
| Wedge-shaped segmental or lobar consolidation | 17 (70.8%) | 10 (71.4%) | 7 (70.0%) | 0.99 |
| Well-circumscribed nodule(s) | 6 (25.0%) | 6 (42.9%) | 0 (0.0%) | 0.024 |
| Halo sign | 3 (12.5%) | 2 (14.3%) | 1 (10.0%) | 0.68 |
| Cavitation | 5 (20.8%) | 5 (35.7%) | 0 (0.0%) | 0.053 |
| Air-crescent sign | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0.99 |
| Tree in bud | 7 (29.2%) | 7 (50.0%) | 0 (0.0%) | 0.019 |
| Bronchial wall thickening | 8 (33.3%) | 8 (57.1%) | 1 (10.0%) | 0.03 |
| Pleural effusion | 9 (37.5%) | 5 (35.7%) | 4 (40.0%) | 0.99 |
| Similarities between CAPA and IAPA | Differences between CAPA and IAPA |
|---|---|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reizine, F.; Pinceaux, K.; Lederlin, M.; Autier, B.; Guegan, H.; Gacouin, A.; Luque-Paz, D.; Boglione-Kerrien, C.; Bacle, A.; Le Daré, B.; et al. Influenza- and COVID-19-Associated Pulmonary Aspergillosis: Are the Pictures Different? J. Fungi 2021, 7, 388. https://doi.org/10.3390/jof7050388
Reizine F, Pinceaux K, Lederlin M, Autier B, Guegan H, Gacouin A, Luque-Paz D, Boglione-Kerrien C, Bacle A, Le Daré B, et al. Influenza- and COVID-19-Associated Pulmonary Aspergillosis: Are the Pictures Different? Journal of Fungi. 2021; 7(5):388. https://doi.org/10.3390/jof7050388
Chicago/Turabian StyleReizine, Florian, Kieran Pinceaux, Mathieu Lederlin, Brice Autier, Hélène Guegan, Arnaud Gacouin, David Luque-Paz, Christelle Boglione-Kerrien, Astrid Bacle, Brendan Le Daré, and et al. 2021. "Influenza- and COVID-19-Associated Pulmonary Aspergillosis: Are the Pictures Different?" Journal of Fungi 7, no. 5: 388. https://doi.org/10.3390/jof7050388
APA StyleReizine, F., Pinceaux, K., Lederlin, M., Autier, B., Guegan, H., Gacouin, A., Luque-Paz, D., Boglione-Kerrien, C., Bacle, A., Le Daré, B., Launey, Y., Lesouhaitier, M., Painvin, B., Camus, C., Mansour, A., Robert-Gangneux, F., Belaz, S., Le Tulzo, Y., Tadié, J. -M., ... Gangneux, J. -P. (2021). Influenza- and COVID-19-Associated Pulmonary Aspergillosis: Are the Pictures Different? Journal of Fungi, 7(5), 388. https://doi.org/10.3390/jof7050388