

Proniosomal Gel-Loaded Phosphodiesterase Inhibitors (Sildenafil, Vardenafil, and Tadalafil): Prospects for Topical Penile Therapy of Tadalafil for Treatment of Erectile Dysfunction

 ,
,  and
and 
Abstract
:
1. Introduction
2. Results and Discussion
2.1. EE% and Drug Loading
2.2. Size, PDI, and Zeta Potential
2.3. Morphology
2.4. In Vitro Release Studies and Kinetics of Release
2.5. Ex Vivo Skin Permeation Studies
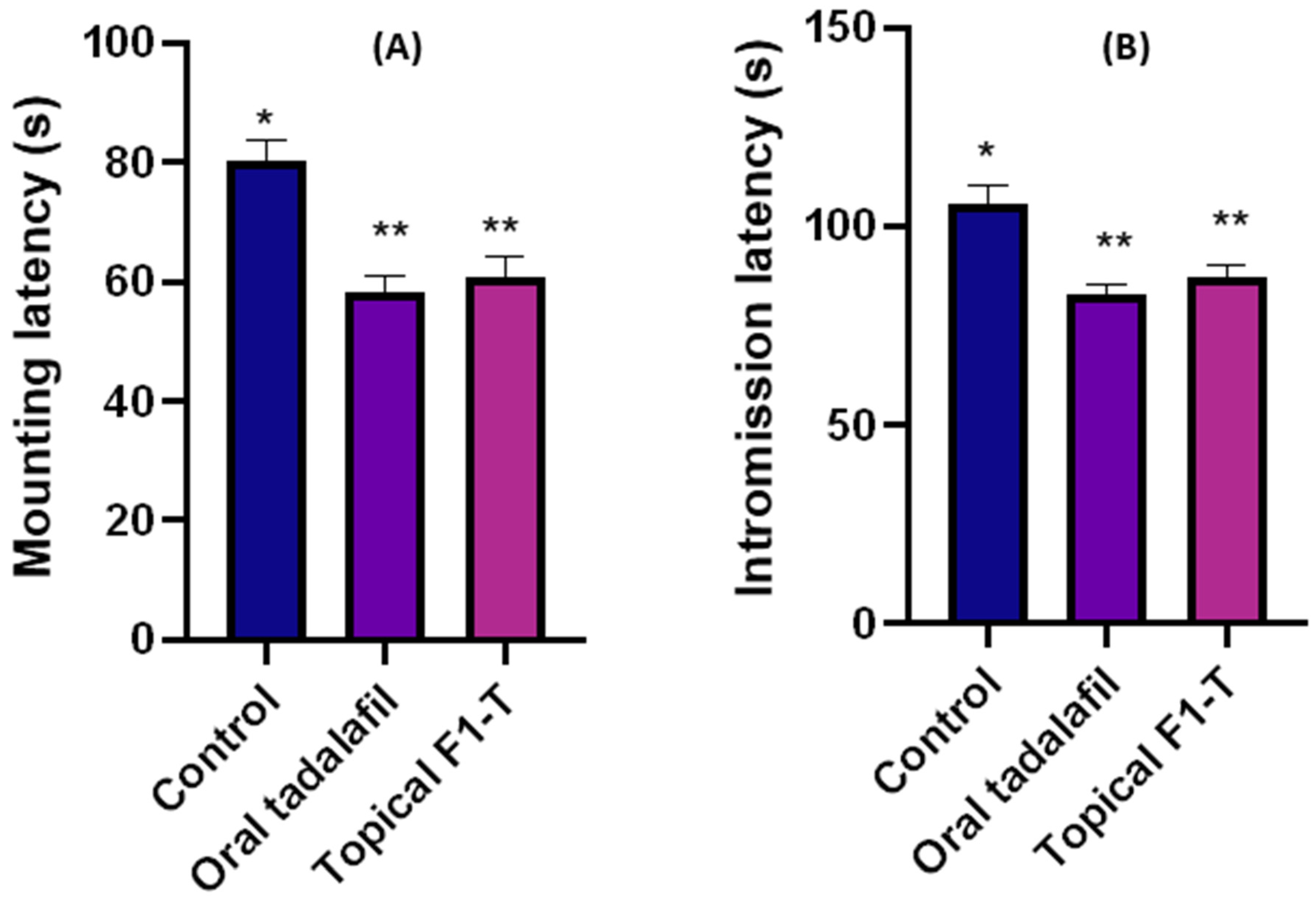
2.6. Mating Behavior Studies and Sexual-Parameter Estimation
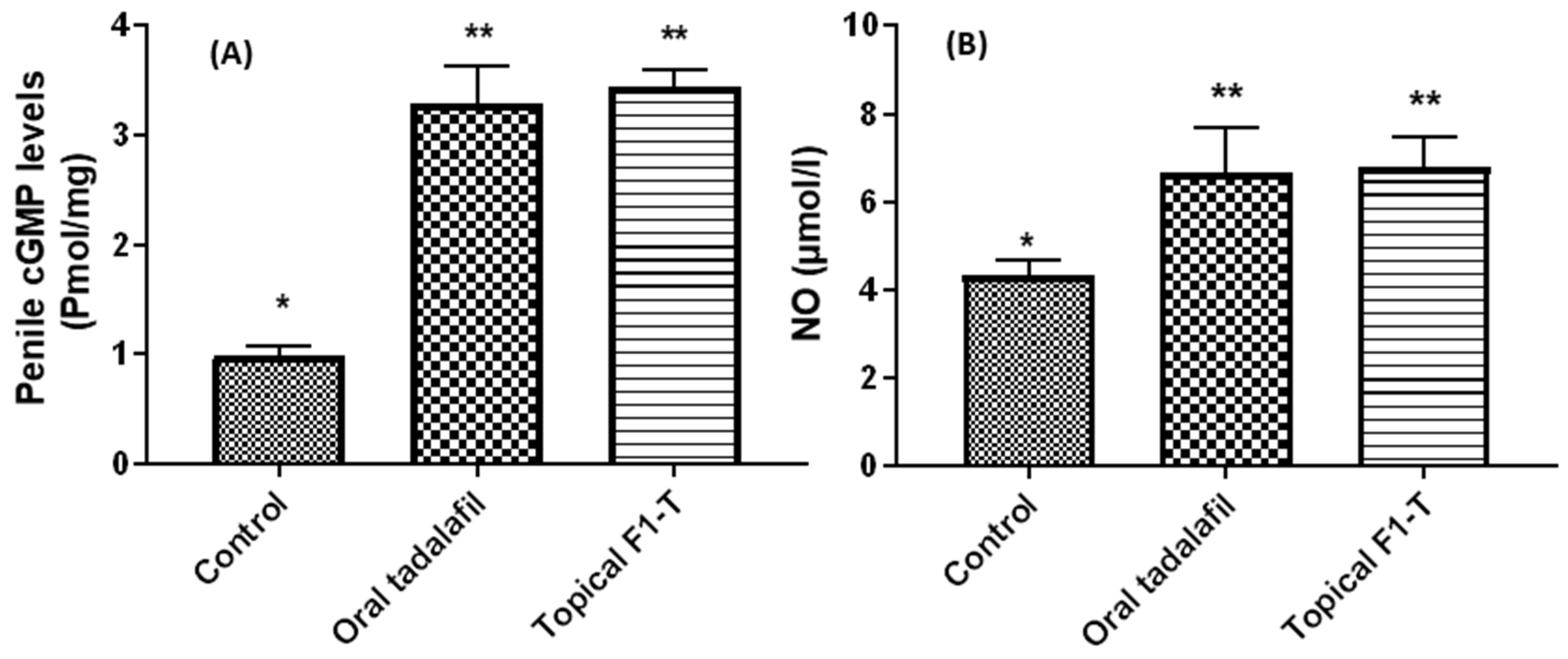
2.7. Biochemical Assays for the Excised and Homogenized Penile Tissues
3. Conclusions
4. Materials and Methods
4.1. Methods
Preparation of Proniosomes
4.2. Encapsulation Efficiency (EE%)
4.3. Size and Zeta-Potential Measurements
4.4. Scanning-Electron-Microscope Imaging of Proniosomal Formulations
4.5. In Vitro Release and Dissolution Kinetics of the Free-Tadalafil and Optimum-Tadalafil Proniosomal Gel (F1T)
4.6. Ex Vivo Permeability
4.7. In Vivo Studies
4.7.1. Animals and Grouping
4.7.2. Mating Behavior Assay
4.8. Biochemical Tests
4.8.1. Nitric Oxide (NO)
4.8.2. Cyclic Guanosine Monophosphate (cGMP)
4.9. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wright, L.; Moghalu, O.I.; Das, R.; Horns, J.; Campbell, A.; Hotaling, J. Erectile Dysfunction and Treatment: An Analysis of Associated Chronic Health Conditions. Urology 2021, 57, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Beecken, W.D.; Kersting, M.; Kunert, W.; Blume, G.; Bacharidis, N.; Cohen, D.S.; Shabeeh, H.; Allen, M.S. Thinking About Pathomechanisms and Current Treatment of Erectile Dysfunction—“The Stanley Beamish Problem.” Review, Recommendations, and Proposals. Sex. Med. Rev. 2021, 9, 445–463. [Google Scholar] [CrossRef] [PubMed]
- Hatzimouratidis, K.; Amar, E.; Eardley, I.; Giuliano, F.; Hatzichristou, D.; Montorsi, F.; Vardi, Y.; Wespes, E. Guidelines on male sexual dysfunction: Erectile dysfunction and premature ejaculation. Eur. Urol. 2010, 57, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Ayta, I.A.; McKinlay, J.B.; Krane, R.J. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU Int. 1999, 84, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.A.; Lie, J.D. Phosphodiesterase-5 (PDE5) Inhibitors In the Management of Erectile Dysfunction. Pharm. Ther. 2013, 38, 414–419. [Google Scholar]
- Patel, C.K.; Bennett, N. Advances in the treatment of erectile dysfunction: What’s new and upcoming? F1000Research 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Evans, J.D.; Hill, S.R. A comparison of the available phosphodiesterase-5 inhibitors in the treatment of erectile dysfunction: A focus on avanafil. Patient Prefer. Adherence 2015, 9, 1159–1164. [Google Scholar] [CrossRef] [Green Version]
- Kloner, R.A.; Zusman, R.M. Cardiovascular effects of sildenafil citrate and recommendations for its use. Am. J. Cardiol. 1999, 84, 11–17. [Google Scholar] [CrossRef]
- Wang, C.C.; Gómez, R.A.; Fernandez, L.P. Determination of sildenafil by preconcentration on surfactant coated polymeric resin followed by spectrofluorimetry. J. Pharm. Anal. 2013, 3, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Ralph, D.; Eardley, I.; Taubel, J.; Terrill, P.; Holland, T. Efficacy and safety of MED2005, a topical glyceryl trinitrate formulation in the treatment of erectile dysfunction: A randomized crossover study. J. Sex. Med. 2018, 15, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Steidle, C.; Nathan, H.; Salem, S.; Tayse, N.; Thwing, D.; Fendl, J.; Yeager, J.; Harning, R. Topical alprostadil cream for the treatment of erectile dysfunction: A combined analysis of the phase II program. Urology 2002, 60, 1077–1082. [Google Scholar] [CrossRef] [PubMed]
- Muzzalupo, R. Niosomes and proniosomes for enhanced skin delivery. In Percutaneous Penetration Enhancers Chemical Methods in Penetration Enhancement; Dragicevic, N., Maibach, H.I., Eds.; Springer: New York, NY, USA, 2016; pp. 147–158. [Google Scholar]
- Bhavani, D.; Lakshmi, V. Recent advances of non-ionic surfactantbased nano-vesicles (niosomes and proniosomes): A brief review of these in enhancing transdermal delivery of drug. Future J. Pharm. Sci. 2020, 6, 100. [Google Scholar]
- Kawar, D.; Abdelkader, H. Hyaluronic acid gel-core liposomes (hyaluosomes) enhance skin permeation of ketoprofen. Pharm. Dev. Technol. 2019, 24, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Aburahma, M.; Badr-Eldin, S. Compritol 888 ATO: Amutifunctional lipid excipients in drug delivery systems and nanopharmaceuticals. Expert. Opin. Drug. Deliv. 2014, 11, 1865–1883. [Google Scholar] [CrossRef] [PubMed]
- Mohamad, S.; Mustafa, W.; Salem, H.; Elrehany, M.; Rofaeil, R.; Abdelkader, H. Physicochemical characteristics and ex vivo skin permeability for three phosphodiesterase 5 inhibitors (sildenafil, tadalafil and vardenafil): A proof-of-concept study for topical penile therapy. J. Drug. Deliv. Sci. Technol. 2022, 70, 103166. [Google Scholar] [CrossRef]
- Abdallah, M.; Sabry, S.; Hasan, A. Enhancing transdermal delivery of glimepiride via entrapment in proniosomal gel. J. Young Pharm. 2016, 8, 335–340. [Google Scholar] [CrossRef] [Green Version]
- Eldeeb, A.; Salah, S.; Ghorab, M. Proniosomal gel-derived niosomes: An approach to sustain and improve the ocular delivery of brimonidine tartrate; formulation, in vitro characterization and in vivo pharmacodynamic study. Drug. Deliv. Transl. Res. 2019, 26, 509–521. [Google Scholar] [CrossRef] [Green Version]
- Abdelkader, H.; Ismail, S.; Kamal, A.; Alany, R. Preparation of niosomes as an ocular delivery system for naltrexone hydrochloride:physicochemical characterization. Pharmazie 2010, 65, 811–817. [Google Scholar]
- Farid, R.; El-Salamouni, N.; El-Kamel, A.; El-Gamal, S. Lipid-based nanocarriers for ocular drug delivery. In Nanostructures for Drug Delivery; Andronescu, E., Grumezescu, A., Eds.; Elsevier: New York, NY, USA, 2017; pp. 495–522. [Google Scholar]
- Mura, P.; Maestrelli, F.; D’Ambrosio, M.; Luceri, C.; Cirri, M. Evaluation and Comparison of Solid Lipid Nanoparticles (SLNs) and Nanostructured Lipid Carriers (NLCs) as Vectors to Develop Hydrochlorothiazide Effective and Safe Pediatric Oral Liquid Formulations. Pharmaceutics 2021, 13, 437. [Google Scholar] [CrossRef]
- Wang, L.; Wang, X.; Shen, L.; Alrobaian, M.; Panda, S.; Almasmoum, H.; Ghaith, M.; Almaimani, R.; Ibrahim, A.; Singh, T.; et al. Paclitaxel and naringenin-loaded solid lipid nanoparticles surface modified with cyclic peptides with improved tumor targeting ability in glioblastoma multiforme. Biomed. Pharmacother. 2021, 138, 111461. [Google Scholar] [CrossRef]
- Abdelkader, H.; Ismail, S.; Kamal, A.; Wu, Z.; Al-Kassas; Alany, R. Conjunctival and corneal tolerability assessment of ocular naltrexone niosomes and their ingredients on the hen’s egg chorioallantoic membrane and excised bovine cornea models. Int. J. Pharm. 2012, 432, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Heijkoop, R.; Huijgens, P.T.; Snoeren, E.M.S. Assessment of sexual behavior in rats: The potentials and pitfalls. Behav. Brain Res. 2018, 352, 70–80. [Google Scholar] [CrossRef] [Green Version]
- Agmo, A. Male rat sexual behavior. Brain Res. Brain Res. Protoc. 1997, 1, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Law, O.T.; Skinner, J. Sexual behavior: Postcopulatory heart rate male and female rat. Prychon. Sci. 1964, 1, 235–236. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Salamone, J.; Sachs, B. Lesions in Medial Preoptic Area and Bed Nucleus of Stria Terminalis: Differential Effects on Copulatory Behavior and Noncontact Erection in Male Rats. J. Neurosci. 1997, 17, 5245–5253. [Google Scholar] [CrossRef]
- Rew, K.T.; Heidelbaugh, J.J. Erectile Dysfunction. Am. Fam. Physician 2016, 94, 820–827. [Google Scholar] [PubMed]
- Sontag, A.; Ni, X.; Althof, S.E.; Rosen, R.C. Relationship between erectile function and sexual self-confidence: A path analytic model in men being treated with tadalafil. Int. J. Impot. Res. 2014, 26, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Escrig, A.; Gonzalez-Mora, J.L.; Mas, M. Nitric oxide release in penile corpora cavernosa in a rat model of erection. J. Physiol. 1999, 516, 261–269. [Google Scholar] [CrossRef]
- Madan, J.; Ghuge, N.; Dua, K. Formulation and evaluation of proniosomes containing lornoxicam. Drug Deliv. Transl. Res. 2016, 6, 511–518. [Google Scholar] [CrossRef]
- Gajbhiye, S.V.; Jadhav, K.S.; Marathe, P.A.; Pawar, D.B. Animal models of erectile dysfunction. Indian J. Urol. IJU J. Urol. Soc. India 2015, 31, 15–21. [Google Scholar] [CrossRef]
- Tavukçu, H.H.; Sener, T.E.; Tinay, I.; Akbal, C.; Erşahin, M.; Cevik, O.; Cadirci, S.; Reiter, R.J.; Sener, G. Melatonin and tadalafil treatment improves erectile dysfunction after spinal cord injury in rats. Clin. Exp. Pharmacol. Physiol. 2014, 41, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Westwood, F.R. The female rat reproductive cycle: A practical histological guide to staging. Toxicol. Pathol. 2008, 36, 375–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gauthaman, K.; Adaikan, P.G.; Prasad, R.N. Aphrodisiac properties of Tribulus Terrestris extract (Protodioscin) in normal and castrated rats. Life Sci. 2002, 71, 1385–1396. [Google Scholar] [CrossRef] [PubMed]
- Guohua, H.; Yanhua, L.; Rengang, M.; Dongzhi, W.; Zhengzhi, M.; Hua, Z. Aphrodisiac properties of Allium tuberosum seeds extract. J. Ethnopharmacol. 2009, 122, 579–582. [Google Scholar] [CrossRef]
- Miranda, K.M.; Espey, M.G.; Wink, D.A. A rapid, simple spectrophotometric method for simultaneous detection of nitrate and nitrite. Biol. Chem. 2001, 5, 62–71. [Google Scholar] [CrossRef]
- Preedapirom, W.; Changwichit, K.; Srisawang, P.; Ingkaninan, K.; Taepavarapruk, P. Aphrodisiac Activity of Eulophia macrobulbon Extract on Erectile Dysfunction in Male Aged Rats. BioMed Res. Int. 2018, 2018, 6217029. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | EE% | Drug Loading Capacity (%) | Particle Size (µm) | PDI | Zeta Potential (mV) | Flux (mg·h−1 cm−2) | Apparent Permeability Papp·10−3 (cm h−1) |
|---|---|---|---|---|---|---|---|
| F1-S | 93 ± 2.0 | 0.62 | 1.89 ± 0.10 | 0.29 ± 0.01 | −43.9 ± 2.5 | 0.77 ± 0.02 | 77.0 ± 2.0 |
| F2-S | 65 ± 3.0 | 0.26 | 1.83 ± 0.16 | 0.25 ± 0.02 | −43.0 ± 2.0 | 0.23 ± 0.03 | 23.0 ± 2.5 |
| F3-S | 45 ± 4.0 | 0.18 | 4.50 ± 0.30 | 0.19 ± 0.03 | −42.4 ± 2.3 | 0.17 ± 0.02 | 17.0 ± 3.0 |
| F1-V | 95 ± 5.0 | 0.63 | 1.81 ± 0.17 | 0.29 ± 0.01 | −38.9 ± 2.5 | 0.18 ± 0.01 | 90.0 ± 8.0 |
| F2-V | 70 ± 3.0 | 0.28 | 1.83 ± 0.16 | 0.5 ± 0.02 | −39.9 ± 3.0 | 0.17 ± 0.02 | 84.0 ± 4.0 |
| F3-V | 58 ± 2.0 | 0.23 | 4.50 ± 0.45 | 0.19 ± 0.03 | −40.9 ± 3.2 | 0.12 ± 0.02 | 62.0 ± 3.0 |
| F1-T | 97 ± 2.0 | 0.64 | 1.80 ± 0.15 | 0.39 ± 0.01 | −38.0 ± 3.0 | 0.25 ± 0.03 | 125.0 ± 1.5 |
| F2-T | 90 ± 1.0 | 0.36 | 1.83 ± 0.16 | 0.3 ± 0.02 | −37.9 ± 2.6 | 0.19 ± 0.02 | 96.0 ± 5.0 |
| F3-T | 82 ± 3.0 | 0.32 | 4.50 ± 0.22 | 0.19 ± 0.03 | −37.7 ± 2.6 | 0.23 ± 0.02 | 110.0 ± 4.0 |
| Zero | First | Second | Higuchi | Hixon | Baker | |
|---|---|---|---|---|---|---|
| a | 21.67742 | 21.67742 | 21.67742 | 2.938152 | 21.67742 | 0.020172 |
| b | 0.727398 | 0.727398 | 0.727398 | 56.40955 | 0.727398 | 0.104645 |
| r | 0.797727 | −0.79773 | 0.797727 | 0.956945 | 0.797727 | 0.904567 |
| k | 0.727398 | −1.6752 | 0.727398 | 56.40955 | 0.727398 | 0.104645 |
| t (1/2) | 68.73817 | −0.41368 | 0.013748 | 0.78566 | 1.314504 | 0.525584 |
| Formulation Code | Sildenafil (mg) | Tadalafil (mg) | Vardenafil (mg) | Span 60 (mg) | Lecithin (mg) | Cholesterol (mg) | Compritol 888 ATO (mg) | Precirol ATO 5 (mg) |
|---|---|---|---|---|---|---|---|---|
| F1-S | 20 | - | - | 400 | 100 | 50 | - | - |
| F2-S | 20 | - | - | 300 | 100 | 50 | 100 | - |
| F3-S | 20 | - | - | 300 | 100 | 50 | - | 100 |
| F1-T | - | 4 | - | 400 | 100 | 50 | - | - |
| F2-T | - | 4 | - | 300 | 100 | 50 | 100 | - |
| F3-T | - | 4 | - | 300 | 100 | 50 | - | 100 |
| F1-V | - | - | 4 | 400 | 100 | 50 | - | - |
| F2-V | - | - | 4 | 300 | 100 | 50 | 100 | - |
| F3-V | - | - | 4 | 300 | 100 | 50 | - | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohamed, S.A.; Rofaeil, R.R.; Salem, H.; Elrehany, M.; Asiri, Y.I.; Al Fatease, A.; Abdelkader, H. Proniosomal Gel-Loaded Phosphodiesterase Inhibitors (Sildenafil, Vardenafil, and Tadalafil): Prospects for Topical Penile Therapy of Tadalafil for Treatment of Erectile Dysfunction. Gels 2023, 9, 597. https://doi.org/10.3390/gels9080597
Mohamed SA, Rofaeil RR, Salem H, Elrehany M, Asiri YI, Al Fatease A, Abdelkader H. Proniosomal Gel-Loaded Phosphodiesterase Inhibitors (Sildenafil, Vardenafil, and Tadalafil): Prospects for Topical Penile Therapy of Tadalafil for Treatment of Erectile Dysfunction. Gels. 2023; 9(8):597. https://doi.org/10.3390/gels9080597
Chicago/Turabian StyleMohamed, Soad A., Remon Roshdy Rofaeil, Hesham Salem, Mahmoud Elrehany, Yahya I. Asiri, Adel Al Fatease, and Hamdy Abdelkader. 2023. "Proniosomal Gel-Loaded Phosphodiesterase Inhibitors (Sildenafil, Vardenafil, and Tadalafil): Prospects for Topical Penile Therapy of Tadalafil for Treatment of Erectile Dysfunction" Gels 9, no. 8: 597. https://doi.org/10.3390/gels9080597
APA StyleMohamed, S. A., Rofaeil, R. R., Salem, H., Elrehany, M., Asiri, Y. I., Al Fatease, A., & Abdelkader, H. (2023). Proniosomal Gel-Loaded Phosphodiesterase Inhibitors (Sildenafil, Vardenafil, and Tadalafil): Prospects for Topical Penile Therapy of Tadalafil for Treatment of Erectile Dysfunction. Gels, 9(8), 597. https://doi.org/10.3390/gels9080597