Comparing Radar-Based Breast Imaging Algorithm Performance with Realistic Patient-Specific Permittivity Estimation



Abstract
:1. Introduction
2. Background
- calculating a separate weighting factor to reward points where tumors are more likely based either on epidemiological studies or on characteristics of the scattered signals ( from Equation (1));
- prioritizing scattered signals collected at certain locations based on the relative locations of the antennas and points of interest or on the antenna radiation patterns ( in Equation (1));
- by improving the quality of the input signals prior to imaging through improved artefact removal algorithms or other noise reduction techniques.
Evaluation Metrics
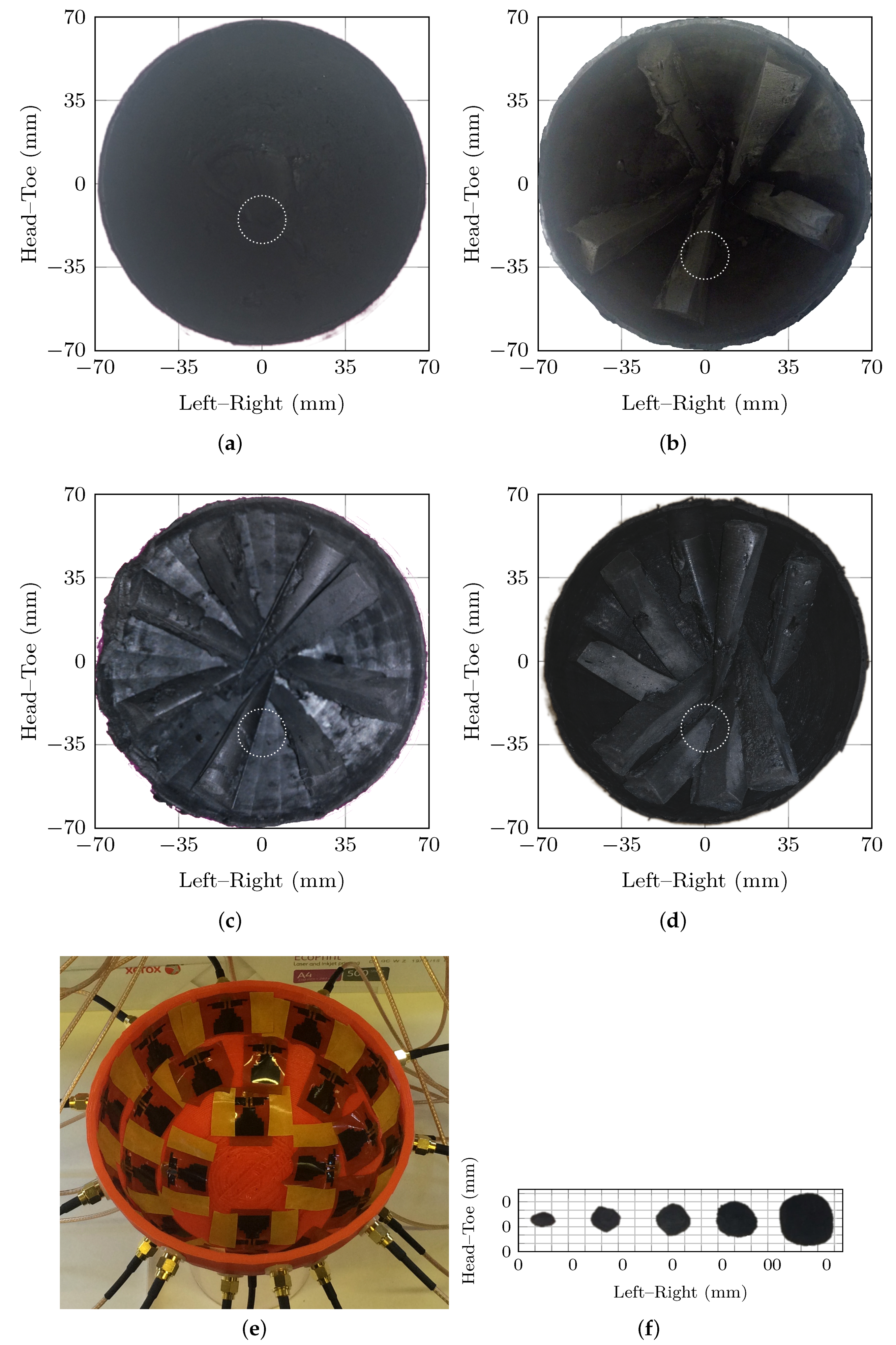
3. Experimental Methods
- a hemispherical skin which varied between 1 to 3 in thickness with relative permittivity of and electrical conductivity of at 3 ;
- conical glandular structures to model breast lobes radiating from the areola with relative permittivity of and electrical conductivity of at 3 ;
- an adipose layer with relative permittivity of and electrical conductivity of .
4. Results
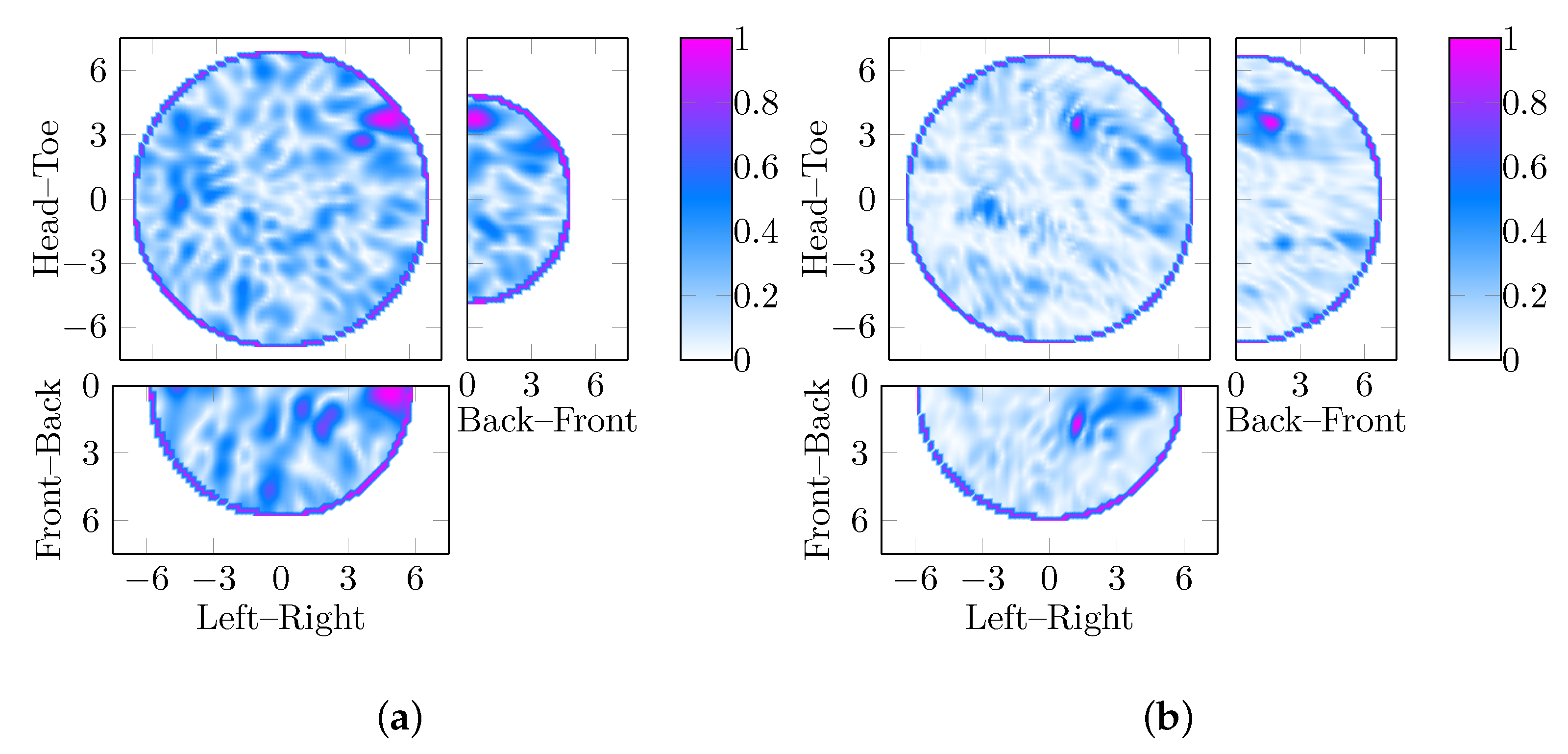
- first, the impact of permittivity estimation in phantoms without abnormalities is discussed in Section 4.1, considering both beamformers and the four breast phantoms;
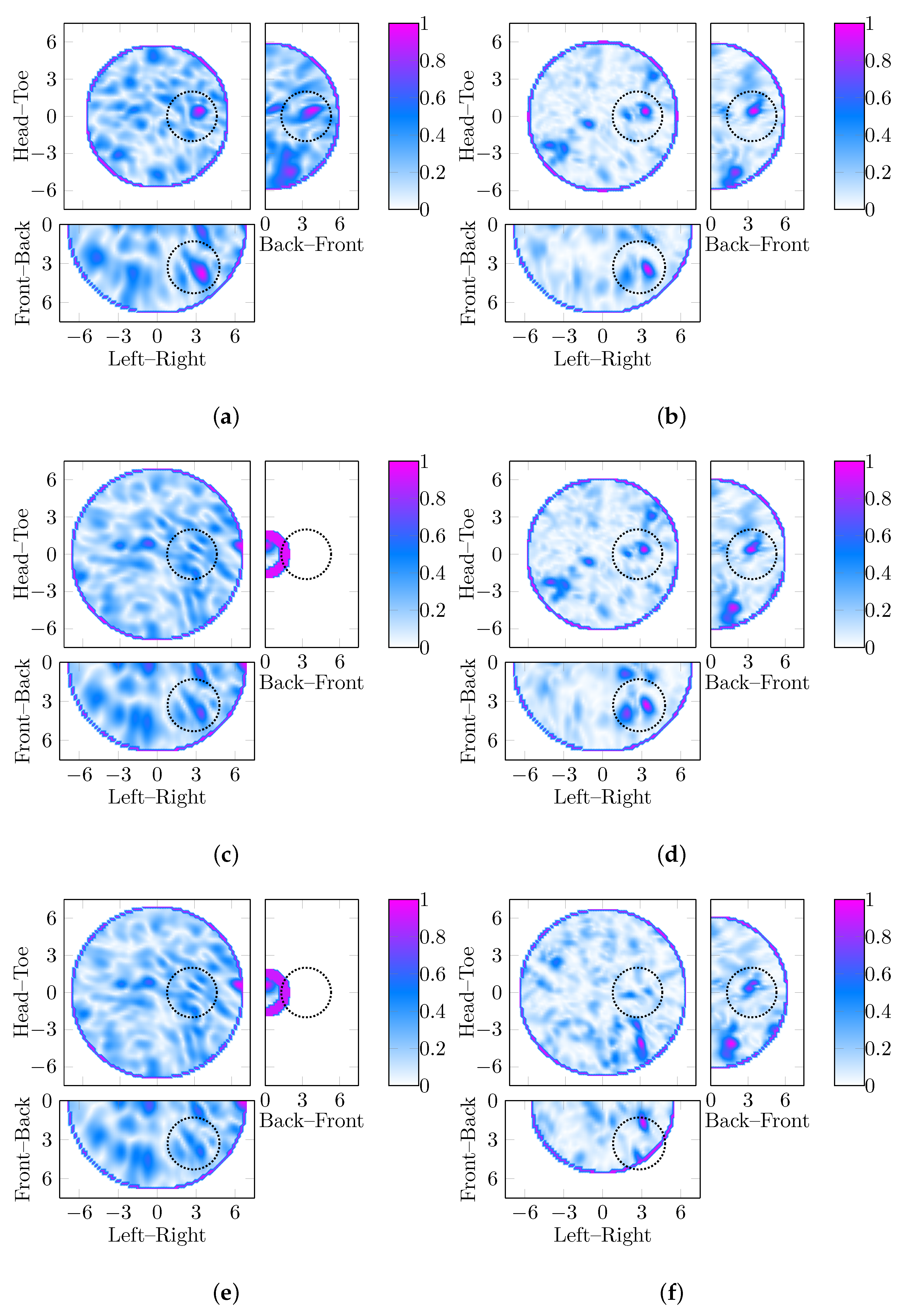
- secondly, the ability of DMAS to compensate for errors in the permittivity estimation process is considered in Section 4.2;
- thirdly, the permittivity estimation algorithms are applied to images of the same scene reconstructed with different beamformers to estimate if the characteristics of the images are different in Section 4.3.
4.1. Algorithm Performance in Test Cases without Abnormalities
4.2. Effects of Permittivity Estimation on Performance
4.3. Parameter Search Performance Using both Beamformers
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- O’Loughlin, D.; O’Halloran, M.; Moloney, B.M.; Glavin, M.; Jones, E.; Elahi, M.A. Microwave Breast Imaging: Clinical Advances and Remaining Challenges. Trans. Biomed. Eng. 2018, 65, 2580–2590. [Google Scholar] [CrossRef] [PubMed]
- Preece, A.W.; Craddock, I.J.; Shere, M.; Jones, L.; Winton, H.L. MARIA M4: Clinical Evaluation of a Prototype Ultrawideband Radar Scanner for Breast Cancer Detection. J. Med. Imaging 2016, 3, 033502. [Google Scholar] [CrossRef] [PubMed]
- Porter, E.; Coates, M.; Popović, M. An Early Clinical Study of Time-Domain Microwave Radar for Breast Health Monitoring. IEEE Trans. Biomed. Eng. 2016, 63, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Sasada, S.; Kadoya, T.; Okada, M.; Arihiro, K.; Xiao, X.; Kikkawa, T. Detectability of Breast Tumor by a Hand-Held Impulse-Radar Detector: Performance Evaluation and Pilot Clinical Study. Sci. Rep. 2017, 7, 16353. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Sun, L.; Hu, Z.; Wang, H.; Pan, D.; Wu, R.; Zhang, X.; Chen, Y.; Zhang, Q. A Large-Scale Clinical Trial of Radar-Based Microwave Breast Imaging for Asian Women: Phase I. In Proceedings of the International Symposium on Antennas and Propagation (APSURSI), San Diego, CA, USA, 9–14 July 2017; IEEE: San Diego, CA, USA, 2017; pp. 781–783. [Google Scholar] [CrossRef]
- Song, H.; Sasada, S.; Masumoto, N.; Kadoya, T.; Shiroma, N.; Orita, M.; Arihiro, K.; Okada, M.; Kikkawa, T. Detectability of Breast Tumors in Excised Breast Tissues of Total Mastectomy by IR-UWB-Radar-Based Breast Cancer Imaging. IEEE Trans. Biomed. Eng. 2018, 66, 2296–2305. [Google Scholar] [CrossRef] [PubMed]
- Wörtge, D.; Moll, J.; Krozer, V.; Bazrafshan, B.; Hübner, F.; Park, C.; Vogl, T. Comparison of X-ray Mammography and Planar UWB Microwave Imaging of the Breast: First Results from a Patient Study. Diagnostics 2018, 8, 54. [Google Scholar] [CrossRef]
- Fasoula, A.; Anwar, S.; Toutain, Y.; Duchesne, L. Microwave Vision: From RF Safety to Medical Imaging. In Proceedings of the 11th European Conference on Antennas and Propagation (EuCAP), Paris, France, 19–24 March 2017; IEEE: Paris, France, 2017; pp. 2746–2750. [Google Scholar] [CrossRef]
- Fasoula, A.; Duchesne, L.; Gil Cano, J.; Lawrence, P.; Robin, G.; Bernard, J.G. On-Site Validation of a Microwave Breast Imaging System, before First Patient Study. Diagnostics 2018, 8, 53. [Google Scholar] [CrossRef]
- Duchesne, L.; Fasoula, A.; Kaverine, E.; Robin, G.; Bernard, J.G. Wavelia Microwave Breast Imaging: Identification and Mitigation of Possible Sources of Measurement Uncertainty. In Proceedings of the 13th European Conference on Antennas and Propagation (EuCAP), Kraków, Poland, 31 March–5 April 2019. [Google Scholar]
- Bolomey, J.C. Crossed Viewpoints on Microwave-Based Imaging for Medical Diagnosis: From Genesis to Earliest Clinical Outcomes. In The World of Applied Electromagnetics; Lakhtakia, A., Furse, C.M., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 369–414. [Google Scholar] [CrossRef]
- Nikolova, N.K. Microwave Biomedical Imaging. In Wiley Encyclopedia of Electric and Electronics Engineering; John Wiley & Sons, Inc.: New York, NY, USA, 2014; pp. 1–22. [Google Scholar]
- Conceição, R.C.; Mohr, J.J.; O’Halloran, M. (Eds.) An Introduction to Microwave Imaging for Breast Cancer Detection, 1st ed.; Biological and Medical Physics, Biomedical Engineering; Springer International Publishing: Cham, Switzerland, 2016. [Google Scholar]
- Nikolova, N.K. (Ed.) Introduction to Microwave Imaging; EuMA High Frequency Technologies Series; Cambridge University Press: Cambridge, UK, 2017. [Google Scholar] [CrossRef]
- O’Loughlin, D.; Elahi, M.A.; Porter, E.; Shahzad, A.; Oliveira, B.L.; Glavin, M.; Jones, E.; O’Halloran, M. Open-Source Software for Microwave Radar-Based Image Reconstruction. In Proceedings of the 12th European Conference on Antennas and Propagation (EuCAP), London, UK, 9–13 April 2018. [Google Scholar]
- Klemm, M.; Craddock, I.J.; Leendertz, J.A.; Preece, A.W.; Benjamin, R. Radar-Based Breast Cancer Detection Using a Hemispherical Antenna Array—Experimental Results. IEEE Trans. Antennas Propag. 2009, 57, 1692–1704. [Google Scholar] [CrossRef]
- Xie, Y.; Guo, B.; Xu, L.; Li, J.; Stoica, P. Multistatic Adaptive Microwave Imaging for Early Breast Cancer Detection. IEEE Trans. Biomed. Eng. 2006, 53, 1647–1657. [Google Scholar] [CrossRef]
- O’Halloran, M.; Glavin, M.; Jones, E. Effects of Fibroglandular Tissue Distribution on Data-Independent Beamforming Algorithms. Prog. Electromagn. Res. 2009, 97, 141–158. [Google Scholar] [CrossRef]
- Byrne, D.; O’Halloran, M.; Glavin, M.; Jones, E. Data Independent Radar Beamforming Algorithms for Breast Cancer Detection. Prog. Electromagn. Res. 2010, 107, 331–348. [Google Scholar] [CrossRef]
- Moll, J.; Kexel, C.; Krozer, V. A Comparison of Beamforming Methods for Microwave Breast Cancer Detection in Homogeneous and Heterogeneous Tissue. In Proceedings of the Microwave Conference (EuMC), Nuremberg, Germany, 6–10 October 2013; pp. 1839–1842. [Google Scholar]
- Elahi, M.A.; Lavoie, B.R.; Porter, E.; Glavin, M.; Jones, E.; Fear, E.C.; O’Halloran, M. Comparison of Radar-Based Microwave Imaging Algorithms Applied to Experimental Breast Phantoms. In Proceedings of the 32nd International Union of Radio Science (URSI) General Assembly and Scientific Symposium, Montreal, QC, Canada, 19–26 August 2017; Union of Radio Science (URSI): Montréal, QC, Canada, 2017. [Google Scholar]
- Elahi, M.A.; O’Loughlin, D.; Lavoie, B.R.; Glavin, M.; Jones, E.; Fear, E.C.; O’Halloran, M. Evaluation of Image Reconstruction Algorithms for Confocal Microwave Imaging: Application to Patient Data. Sensors 2018, 18, 1678. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, D.; Oliveira, B.L.; Elahi, M.A.; Glavin, M.; Jones, E.; Popović, M.; O’Halloran, M. Parameter Search Algorithms for Microwave Radar-Based Breast Imaging: Focal Quality Metrics as Fitness Functions. Sensors 2017, 17, 2823. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, D.; Oliveira, B.L.; Santorelli, A.; Porter, E.; Glavin, M.; Jones, E.; Popović, M.; O’Halloran, M. Sensitivity and Specificity Estimation Using Patient-Specific Microwave Imaging in Diverse Experimental Breast Phantoms. IEEE Trans. Med. Imaging 2019, 38, 303–311. [Google Scholar] [CrossRef]
- O’Loughlin, D.; Krewer, F.; Glavin, M.; Jones, E.; O’Halloran, M. Focal Quality Metrics for the Objective Evaluation of Confocal Microwave Images. Int. J. Microw. Wirel. Technol. 2017, 9, 1365–1372. [Google Scholar] [CrossRef]
- Lavoie, B.R.; Okoniewski, M.; Fear, E.C. Estimating the Effective Permittivity for Reconstructing Accurate Microwave-Radar Images. PLoS ONE 2016, 11, 0160849. [Google Scholar] [CrossRef]
- O’Loughlin, D.; Glavin, M.; Jones, E.; O’Halloran, M. Evaluation of Experimental Microwave Radar-Based Images: Evaluation Criteria. In Proceedings of the Antennas and Propagation Society International Symposium (APSURSI), Boston, MA, USA, 8–13 July 2018; IEEE: Boston, MA, USA, 2018. [Google Scholar]
- Iskander, M.F.; Durney, C.H. Electromagnetic Techniques for Medical Diagnosis: A Review. Proc. IEEE 1980, 68, 126–132. [Google Scholar] [CrossRef]
- Larsen, L.; Jacobi, J. Microwaves Offer Promise as Imaging Modality. Diagn. Imaging 1982, 11, 44–47. [Google Scholar]
- Fear, E.C.; Hagness, S.C.; Meaney, P.M.; Okoniewski, M.; Stuchly, M.A. Enhancing Breast Tumor Detection with Near-Field Imaging. IEEE Microw. Mag. 2002, 3, 48–56. [Google Scholar] [CrossRef]
- Fear, E.C. Microwave Imaging of the Breast. Technol. Cancer Res. Treat. 2005, 4, 69–82. [Google Scholar] [CrossRef]
- Nikolova, N.K. Microwave Imaging for Breast Cancer. IEEE Microw. Mag. 2011, 12, 78–94. [Google Scholar] [CrossRef]
- Meaney, P.M. Microwave Imaging: Perception and Reality. Expert Rev. Med. Devices 2013, 10, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Crocco, L. Microwaves for Medical Imaging: Some Possible Pathways for an Accelerated Progress towards Clinical Practice. New Horizons Transl. Med. 2015, 2, 62. [Google Scholar] [CrossRef]
- Chandra, R.; Zhou, H.; Balasingham, I.; Narayanan, R.M. On the Opportunities and Challenges in Microwave Medical Sensing and Imaging. IEEE Trans. Biomed. Eng. 2015, 62, 1667–1682. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Lee, S. Recent Advances in Microwave Imaging for Breast Cancer Detection. Int. J. Biomed. Imaging 2016, 2016, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Modiri, A.; Goudreau, S.; Rahimi, A.; Kiasaleh, K. Review of Breast Screening: Towards Clinical Realization of Microwave Imaging. Med. Phys. 2017, 44, e446–e458. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Hagness, S.C. A Confocal Microwave Imaging Algorithm for Breast Cancer Detection. Microw. Wirel. Components Lett. IEEE 2001, 11, 130–132. [Google Scholar]
- Nilavalan, R.; Gbedemah, A.; Craddock, I.J.; Li, X.; Hagness, S.C. Numerical Investigation of Breast Tumour Detection Using Multi-Static Radar. Electron. Lett. 2003, 39, 1787–1789. [Google Scholar] [CrossRef]
- Fear, E.C.; Bourqui, J.; Curtis, C.F.; Mew, D.; Docktor, B.; Romano, C. Microwave Breast Imaging With a Monostatic Radar-Based System: A Study of Application to Patients. IEEE Trans. Microw. Theory Tech. 2013, 61, 2119–2128. [Google Scholar] [CrossRef]
- Shao, W.; Edalati, A.; McCollough, T.R.; McCollough, W.J. A Time-Domain Measurement System for UWB Microwave Imaging. IEEE Trans. Microw. Theory Tech. 2018, 66, 2265–2275. [Google Scholar] [CrossRef]
- Islam, M.; Samsuzzaman, M.; Islam, M.; Kibria, S. Experimental Breast Phantom Imaging with Metamaterial-Inspired Nine-Antenna Sensor Array. Sensors 2018, 18, 4427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, H.B.; Nhung, N.T.T.; Li, E.P.; Thang, N.D. Confocal Microwave Imaging for Breast Cancer Detection: Delay-Multiply-and-Sum Image Reconstruction Algorithm. IEEE Trans. Biomed. Eng. 2008, 55, 1697–1704. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, D.; Krewer, F.; Glavin, M.; Jones, E.; O’Halloran, M. Estimating Average Dielectric Properties for Microwave Breast Imaging Using Focal Quality Metrics. In Proceedings of the 10th European Conference on Antennas and Propagation (EuCAP), Davos, Switzerland, 10–15 April 2016; IEEE: Davos, Switzerland, 2016; pp. 1–5. [Google Scholar] [CrossRef]
- O’Loughlin, D.; Glavin, M.; Jones, E.; O’Halloran, M. Optimisation of Confocal Microwave Breast Images Using Image Focal Metrics. In Proceedings of the 22nd Bioengineering in Ireland (BINI), Galway, Ireland, 22–23 January 2016; Royal Academy of Medicine in Ireland: Galway, Ireland, 2016; p. 39. [Google Scholar]
- O’Loughlin, D.; Oliveira, B.L.; Glavin, M.; Jones, E.; O’Halloran, M. Advantages and Disadvantages of Parameter Search Algorithms for Permittivity Estimation for Microwave Breast Imaging. In Proceedings of the 13th European Conference on Antennas and Propagation (EuCAP), Krakow, Poland, 31 March–5 April 2019; IEEE: Kraków, Poland, 2019. [Google Scholar]
- O’Loughlin, D.; Oliveira, B.L.; Glavin, M.; Jones, E.; O’Halloran, M. Effects of Interpatient Variance on Microwave Breast Images: Experimental Evaluation. In Proceedings of the 40th Annual International Conference of the Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; IEEE: Honolulu, HI, USA, 2018. [Google Scholar]
- Oliveira, B.L.; O’Loughlin, D.; O’Halloran, M.; Porter, E.; Glavin, M.; Jones, E. Microwave Breast Imaging: Experimental Tumour Phantoms for the Evaluation of New Breast Cancer Diagnosis Systems. Biomed. Phys. Eng. Express 2018, 4, 025036. [Google Scholar] [CrossRef]
- Garrett, J.; Fear, E.C. A New Breast Phantom With a Durable Skin Layer for Microwave Breast Imaging. IEEE Trans. Antennas Propag. 2015, 63, 1693–1700. [Google Scholar] [CrossRef]
- Santorelli, A.; Laforest, O.; Porter, E.; Popović, M. Image Classification for a Time-Domain Microwave Radar System: Experiments with Stable Modular Breast Phantoms. In Proceedings of the 9th European Conference on Antennas and Propagation (EuCAP), Lisbon, Portugal, 13–17 April 2015; IEEE: Lisbon, Portugal, 2015; pp. 1–5. [Google Scholar]
- Lazebnik, M.; McCartney, L.; Popović, D.; Watkins, C.B.; Lindstrom, M.J.; Harter, J.; Sewall, S.; Magliocco, A.; Booske, J.H.; Okoniewski, M.; et al. A Large-Scale Study of the Ultrawideband Microwave Dielectric Properties of Normal Breast Tissue Obtained from Reduction Surgeries. Phys. Med. Biol. 2007, 52, 2637–2656. [Google Scholar] [CrossRef] [Green Version]
- Lazebnik, M.; Popović, D.; McCartney, L.; Watkins, C.B.; Lindstrom, M.J.; Harter, J.; Sewall, S.; Ogilvie, T.; Magliocco, A.; Breslin, T.M.; et al. A Large-Scale Study of the Ultrawideband Microwave Dielectric Properties of Normal, Benign and Malignant Breast Tissues Obtained from Cancer Surgeries. Phys. Med. Biol. 2007, 52, 6093–6115. [Google Scholar] [CrossRef]
- Sugitani, T.; Kubota, S.; Kuroki, S.; Sogo, K.; Arihiro, K.; Okada, M.; Kadoya, T.; Hide, M.; Oda, M.; Kikkawa, T. Complex Permittivities of Breast Tumor Tissues Obtained from Cancer Surgeries. Appl. Phys. Lett. 2014, 104, 253702. [Google Scholar] [CrossRef]
- Huang, S.Y.; Boone, J.M.; Yang, K.; Packard, N.J.; McKenney, S.E.; Prionas, N.D.; Lindfors, K.K.; Yaffe, M.J. The Characterization of Breast Anatomical Metrics Using Dedicated Breast CT. Med. Phys. 2011, 38, 2180–2191. [Google Scholar] [CrossRef] [Green Version]
- Bahramiabarghouei, H.; Porter, E.; Santorelli, A.; Gosselin, B.; Popović, M.; Rusch, L.A. Flexible 16 Antenna Array for Microwave Breast Cancer Detection. IEEE Trans. Biomed. Eng. 2015, 62, 2516–2525. [Google Scholar] [CrossRef]
- Porter, E.; Bahrami, H.; Santorelli, A.; Gosselin, B.; Rusch, L.A.; Popović, M. A Wearable Microwave Antenna Array for Time-Domain Breast Tumor Screening. IEEE Trans. Med. Imaging 2016, 35, 1501–1509. [Google Scholar] [CrossRef]
- Kuwahara, Y. Microwave Imaging for Early Breast Cancer Detection. In New Perspectives in Breast Imaging; Malik, A.M., Ed.; InTechOpen: London, UK, 2017. [Google Scholar] [CrossRef] [Green Version]
- Shere, M.; Lyburn, I.; Sidebottom, R.; Massey, H.; Gillett, C.; Jones, L. MARIA® M5: A Multicentre Clinical Study to Evaluate the Ability of the Micrima Radio-Wave Radar Breast Imaging System (MARIA®) to Detect Lesions in the Symptomatic Breast. Eur. J. Radiol. 2019, 116, 61–67. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SCR () | FWHM () | |||||||
|---|---|---|---|---|---|---|---|---|
| 0% VGF | 10% VGF | 0% VGF | 10% VGF | |||||
| DAS | 2.6 | 1.5 | 1.6 | 0.75 | 10 | 12 | 13 | 7 |
| DMAS | 0.7 | 1.8 | 2.6 | 2.0 | 7 | 6 | 9 | 10 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Loughlin, D.; Oliveira, B.L.; Glavin, M.; Jones, E.; O’Halloran, M. Comparing Radar-Based Breast Imaging Algorithm Performance with Realistic Patient-Specific Permittivity Estimation. J. Imaging 2019, 5, 87. https://doi.org/10.3390/jimaging5110087
O’Loughlin D, Oliveira BL, Glavin M, Jones E, O’Halloran M. Comparing Radar-Based Breast Imaging Algorithm Performance with Realistic Patient-Specific Permittivity Estimation. Journal of Imaging. 2019; 5(11):87. https://doi.org/10.3390/jimaging5110087
Chicago/Turabian StyleO’Loughlin, Declan, Bárbara L. Oliveira, Martin Glavin, Edward Jones, and Martin O’Halloran. 2019. "Comparing Radar-Based Breast Imaging Algorithm Performance with Realistic Patient-Specific Permittivity Estimation" Journal of Imaging 5, no. 11: 87. https://doi.org/10.3390/jimaging5110087
APA StyleO’Loughlin, D., Oliveira, B. L., Glavin, M., Jones, E., & O’Halloran, M. (2019). Comparing Radar-Based Breast Imaging Algorithm Performance with Realistic Patient-Specific Permittivity Estimation. Journal of Imaging, 5(11), 87. https://doi.org/10.3390/jimaging5110087