The Presence of Behavioral Traps in U.S. Airline Accidents: A Qualitative Analysis

Abstract
:1. Introduction
- Aircraft are machines subject to malfunction and we pilots who operate them are humans subject to human error. As a pilot who plans on remaining on the line, I have learned a valuable lesson—monitor the auto-flight system like a hawk.
- I was making a rushed approach to land. I have learned that when I am rushed is when I really need to take the time for the checklist.
- We thought we had a pretty good handle on our fuel state. Another minute or two of fuel and we would have made it safely to the airfield.
- I blame the mistake on simple overconfidence. Experience, it seems, is no replacement for doing one’s homework.
1.1. Defining Behavioral Traps and Other Decision Making Fallibilities
1.2. Crew Resource Management and Behavioral Traps
1.3. Aims and Objectives
2. Materials and Methods
2.1. Sources of Data
2.2. Data Collection
2.3. Treatment of the Data
2.4. Reliability and Validity of the Data
3. Results
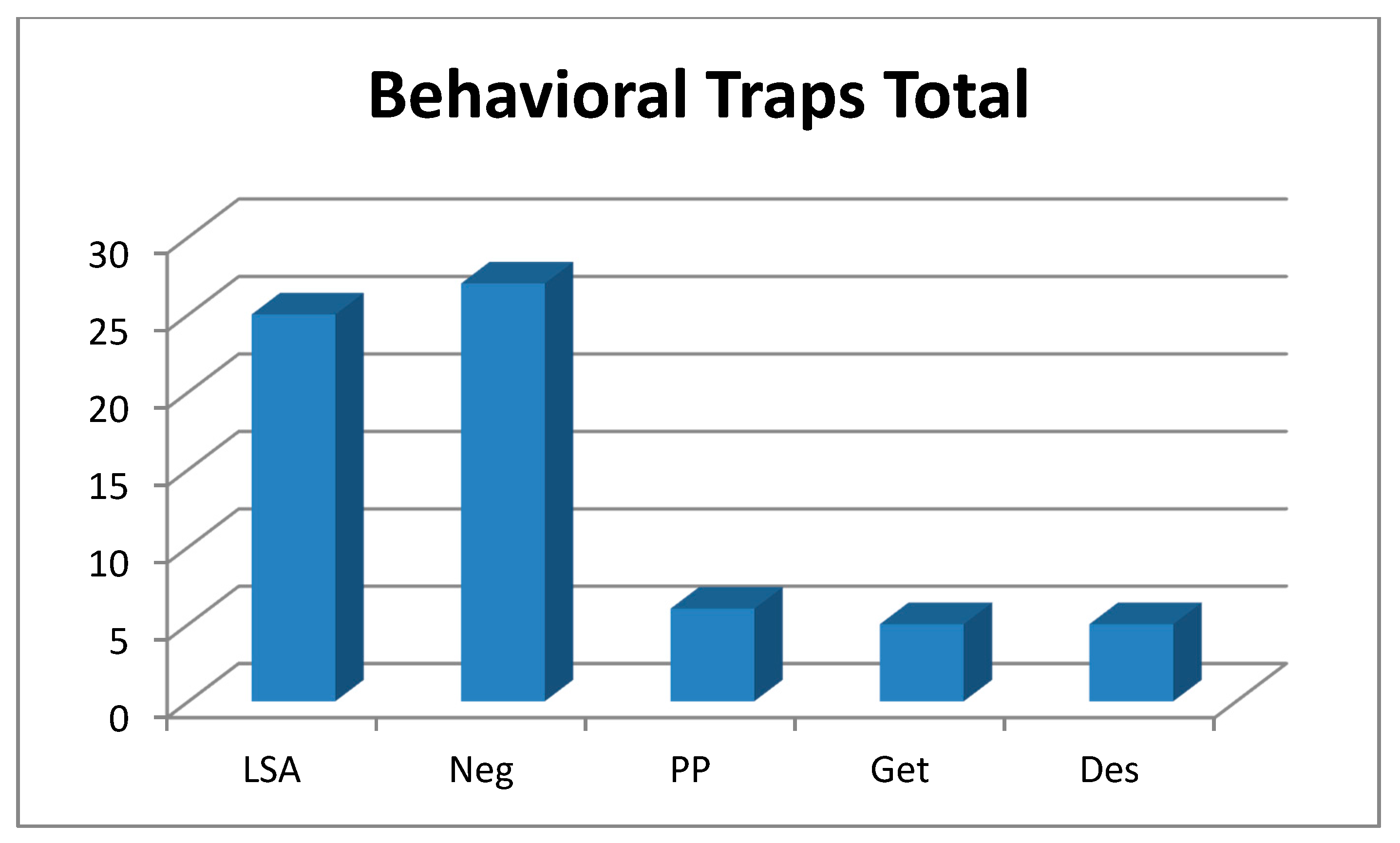
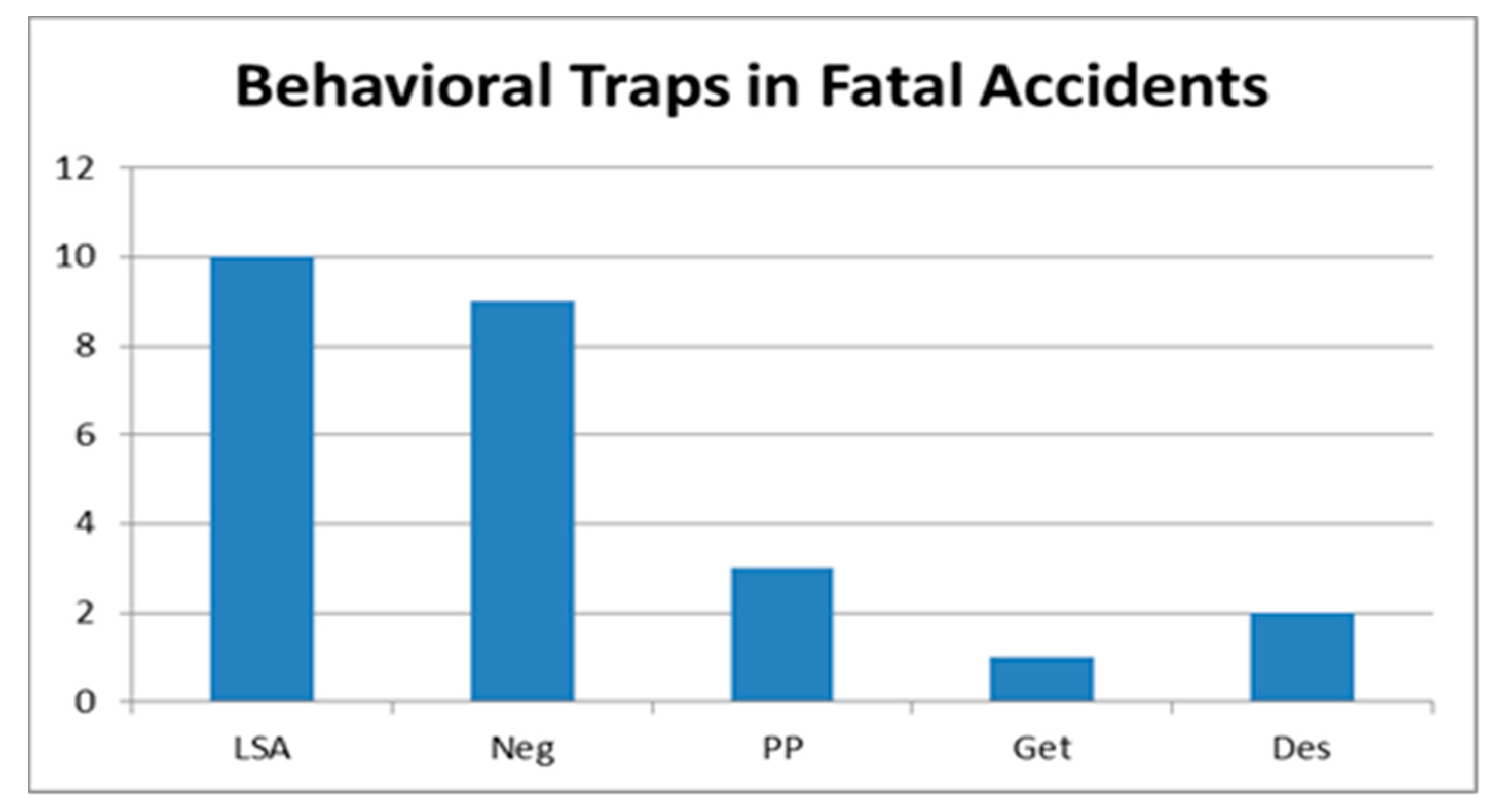
3.1. Descriptive Statistics
3.2. Qualitative Data
3.3. The Top Behavioral Traps
3.4. Additional Contributing Factors Such as Airline Management, CRM Issues, and Fatigue
4. Discussion
4.1. Neglect of Flight Planning, Preflight Inspections, and Checklists
4.2. Loss of Situational Awareness
4.3. Peer Pressure
4.4. Get-There-Itis
4.5. Unauthorized Descent below an IFR Altitude
4.6. CRM Issues
5. Conclusions and Recommendations
5.1. Conclusions
5.2. Recommendations
5.2.1. Recommendations for Further Study
5.2.2. Recommendations for Industry
Acknowledgments
Conflicts of Interest
References
- Federal Aviation Administration (FAA). Risk Management Handbook; Government Printing Office: Washington, DC, USA, 2009.
- Federal Aviation Administration (FAA). Aeronautical Decision Making (Advisory Circular 60-22); Government Printing Office: Washington, DC, USA, 1991.
- Sanderson, J. Private Pilot; Englewood, CO, USA, 2013. [Google Scholar]
- Federal Aviation Administration (FAA). Aviation Instructor’s Handbook; Government Printing Office: Washington, DC, USA, 2008.
- Murata, A.; Nakamura, T.; Karwowski, W. Influence of Cognitive Biases in Distorting Decision Making and Leading to Critical Unfavorable Incidents. Safety 2015, 1, 44–58. [Google Scholar] [CrossRef]
- Dismukes, R.K.; Berman, B.A.; Loukopoulos, L.D. The Limits of Expertise: Rethinking Pilot Error and the Causes of Airline Accidents; Ashgate Publishing Limited: Aldershot, UK, 2007. [Google Scholar]
- Block, E.E.; Sabin, E.J.; Patankar, M.S. The structure of safety climate for accident free flight crews. Int. J. Appl. Aviat. Stud. 2007, 7, 46–59. [Google Scholar]
- Federal Aviation Administration (FAA). Crew Resource Management Training (Advisory Circular AC 120-51e); Government Printing Office: Washington, DC, USA, 2004.
- Helmreich, R.L.; Merritt, A.C.; Wilhelm, J.A. The evolution of crew resource management training in commercial aviation. Int. J. Aviat. Psychol. 1999, 9, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Velazquez, J.; Bier, N. SMS and CRM: Parallels and opposites in their evolution. J. Aviat./Aerosp. Educ. Res. 2015, 24, 55–78. [Google Scholar] [CrossRef]
- Jeppesen. Flight Instructor; JeppDirect: Englewood, CO, USA, 2014. [Google Scholar]
- Bazeley, P. Qualitative Data Analysis: Practical Strategies; Sage: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage: Beverly Hills, CA, USA, 1985. [Google Scholar]
- Creswell, J.W. Educational Research: Planning, Conducting, and Evaluating Quantitative and Qualitative Research; Pearson Education, Inc.: Upper Saddle River, NJ, USA, 2005. [Google Scholar]
- Goglia, J. Torqued: Is Gulfstream IV Crash Corporate Aviation’s Wakeup Call? Available online: http://www.ainonline.com/aviation-news/blogs/torqued-gulfstream-iv-crash-corporate-aviations-wakeup-call (accessed on 1 December 2015).
- Rapp, R. Bedford and the Normalization of Deviance. Available online: http://www.rapp.org/archives/2015/12/normalization-of-deviance/ (accessed on 12 December 2015).
- Veillette, P.R. Watching and waning. Bus. Commer. Aviat. 2006, 98, 60–63. [Google Scholar]
- Klinect, J.R.; Wilhelm, J.A.; Helmreich, R.L. Threat and error management: Data from line operations safety audits (LOSA). In Proceedings of the 10th International Symposium on Aviation Psychology; The Ohio State University: Columbus, OH, USA, 2001. [Google Scholar]
- Velazquez, J.; Peck, A.G.; Sestak, T. Behavioral traps in crew-related aviation accidents. In Proceedings of the 18th International Symposium on Aviation Psychology; Wright State University: Dayton, OH, USA, May 2015; pp. 372–377. [Google Scholar]
- Kern, T. Flight Discipline; McGraw-Hill Professional: Columbus, OH, USA, 1998. [Google Scholar]
- Broome, D.P. Accident reduction through crew resource management. J. Aviat./Aeros. Educ. Res. 2011, 20, 13–21. [Google Scholar] [CrossRef]
- Wagener, F.; Ison, D.C. Crew resource management application in commercial aviation. J. Aviat. Technol. Eng. 2014, 3, 2–13. [Google Scholar] [CrossRef]
- Cook, J.S. Analysis of Hazardous Pilot Behaviors and Causal Factors in Part 121 and Part 135 Aircraft Accidents and Incidents. Master’s Thesis, Retrieved from ProQuest Dissertations and Theses database, (UMI No. 1409570). Arizona State University, Tempe, AZ, USA, 2002. [Google Scholar]
- Mosier, K.L.; Fischer, U.; Cunningham, K.; Munc, A.; Reich, K.; Tomko, L.; Orasanu, J. Aviation decision making issues and outcomes: Evidence from ASRS and NTSB reports. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting; Sage: Los Angeles, CA, USA, October 2012; pp. 1794–1798. [Google Scholar] [CrossRef]
- Shappell, S.; Detwiler, C.; Holcomb, K.; Hackworth, C.; Boquet, A.; Wiegmann, D.A. Human error and commercial aviation accidents: An analysis using the human factors and classification system. Hum. Factors J. Hum. Factors Ergon. Soc. 2007, 49, 227–242. [Google Scholar] [CrossRef] [PubMed]
- Wetmore, M.; Lu, C. The effects of hazardous attitudes on crew resource management skills. Int. J. Appl. Aviat. Stud. 2006, 6, 165–182. [Google Scholar]
- Reason, J. Human Error; Cambridge University Press: Cambridge, UK, 1990. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hazardous Attitude | Characteristics | Antidote |
|---|---|---|
| Anti-authority | Pilots with this attitude dislike following the rules or having someone else tell them what to do. To these pilots, rules and procedures are a waste of time and effort. | “Follow the rules; they are usually right.” |
| Impulsivity | This attitude belongs to pilots who feel they must do something, anything, and immediately. They seldom take a moment to reflect or evaluate all the possibilities. Their actions are the result of whatever comes first to mind. | “Not so fast; think first.” |
| Macho | Macho pilots are risk takers, people overconfident about their skills and constantly proving that they are better than everybody else. To them, they are the best pilots out there. | “Taking chances is foolish.” |
| Invulnerability | Similar to macho-type pilots, these pilots also take risks but only because in their mind accidents happen to others and not to them. They are untouchable. | “It could happen to me.” |
| Resignation | People with this attitude feel they are incapable of making a difference. Pilots with resignation-type attitudes are passive and inactive throughout their flights. To these pilots, when something bad happens it is due to bad luck or the fault of others; someone else is responsible. | “I am not helpless; I can make a difference.” |
| Behavioral Trap | Definition |
|---|---|
| Peer Pressure | Poor decision-making may be based upon an emotional response to peers, rather than evaluating a situation objectively. |
| Mind Set | A pilot displays Mind Set through an inability to recognize and cope with changes in a given situation. |
| Get-There-Itis | This disposition impairs pilot judgment through a fixation on the original goal or destination, combined with a disregard for any alternative course of action. |
| Duck-Under Syndrome | A pilot may be tempted to make it into an airport by descending below minimums during an approach. A pilot may believe that there is a built-in margin of error in every approach procedure, or a pilot may not want to admit that the landing cannot be completed and a missed approach must be initiated. |
| Scud Running | This occurs when a pilot tries to maintain visual contact with the terrain at low altitudes while instrument conditions exist. |
| Continuing Visual Flight Rules (VFR) into Instrument Conditions | Spatial disorientation or collision with ground/obstacles may occur when a pilot continues VFR into instrument conditions. This can be even more dangerous if the pilot is not instrument rated or current. |
| Getting Behind the Aircraft | This pitfall can be caused by allowing events or the situation to control pilot actions. A constant state of surprise at what happens next may be exhibited when the pilot is Getting Behind the Aircraft. |
| Loss of Positional/Situational Awareness | In extreme cases, when a pilot gets behind the aircraft, a loss of positional or situational awareness may result. The pilot may not know the aircraft’s geographical location or may be unable to recognize deteriorating circumstances. |
| Operating Without Adequate Fuel Reserves | Ignoring minimum fuel reserve requirements is generally the result of overconfidence, lack of flight planning, or disregarding applicable regulations. |
| Descent Below the Minimum En Route Altitude (MEA) | The Duck-Under Syndrome, as mentioned above, can also occur during the en route portion of an Instrument Flight Rules (IFR) flight. |
| Flying Outside the Envelope | The assumed high-performance capability of a particular aircraft may cause a mistaken belief that it can meet the demands imposed by a pilot’s overestimated flying skills. |
| Neglect of Flight Planning, Preflight Inspections, and Checklists | A pilot may rely on short- and long-term memory, regular flying skills, and familiar routes instead of established procedures and published checklists. This can be particularly true of experienced pilots. |
| Behavioral Trap | Determination |
|---|---|
| Peer Pressure | One of the commercial behavioral traps according to Jeppesen [11]. Therefore, it was included in this study |
| One of the VFR or GA behavioral traps according to Jeppesen [11]. Therefore, it was not included in this study. | |
| Get-There-Itis | One of the commercial behavioral traps according to Jeppesen [11]. Therefore, it was included in this study |
| Duck-Under Syndrome | One of the instrument behavioral traps according to Jeppesen [11]. Because Part 121 operations are conducted under IFR, it was included in this study. However, this concept was merged with Descent Below the Minimum En Route Altitude (see below) into a new behavioral trap called: Unauthorized Descent Below an IFR Altitude. |
| One of the VFR or GA behavioral traps according to Jeppesen [11]. Therefore, it was not included in this study. | |
| One of the VFR or GA behavioral traps according to Jeppesen [11]. Therefore, it was not included in this study. | |
| Jeppesen merged this commercial behavioral trap with Loss of Situational Awareness (see below) and for good reason. The FAA [1] explains that, in extreme cases, when a pilot gets behind the aircraft, a loss of positional or situational awareness may result. | |
| Loss of | One of the commercial behavioral traps according to Jeppesen [11]. Therefore, it is included in this study |
| One of the VFR or GA behavioral traps according to Jeppesen [11]. Therefore, it was not included in this study. | |
| Descent Below the Minimum En Route Altitude | One of the instrument behavioral traps according to Jeppesen [11]. Because Part 121 operations are conducted under IFR, it is included in this study. However, this trap has been merged with Duck-Under Syndrome (see above) into a new behavioral trap called: Unauthorized Descent Below and IFR Altitude. |
| One of the VFR or GA behavioral traps according to Jeppesen [11]. Therefore, it was not included in this study. | |
| Neglect of Flight Planning, Preflight Inspections, and Checklists | One of the commercial behavioral traps according to Jeppesen [11]. Therefore, it was included in this study |
| Accident Report | Examples |
|---|---|
| 00-02 | Although the airplane speed was within the target range, the airplane did not meet FedEx’s criteria for a stabilized approach because its rate of descent was greater than FedEx’s recommended 1000 feet per minute (fpm). |
| 09-03 | Investigation revealed that the flight crew did not perform several of the appropriate checklists and interrupted an emergency fire-related checklist. |
| 11-02 | Had the captain complied with standard operating procedures in response to the flap anomaly, unstabilized approach, stick shaker, and terrain awareness and warning system warning and initiated a go around maneuver, the accident likely would not have occurred. |
| 93-02 | The captain returned about 10 min after officer, and neither of them performed a walk around inspection of the airplane, nor were they required to do so by USAir procedures. |
| 97-01 | He said that a “norm” existed for the first officer to make hydraulic system configuration changes; he was aware that this was not standard operating practice, which assigned the task to the pilot not flying at all times. He said he conducted his cockpit according to standard operating practice, because he was new to the airplane, and he did not expect first officers to configure the hydraulic pumps. |
| 07-05 | The abbreviated briefing was contrary to company policy, and the Safety Board notes that it is prudent for pilots to fully conduct taxi briefings according to standard operating procedures. |
| 08-02 | The first officer stated that he thought that pilots were required to (and should) check landing distances with a contaminated runway. He said that he believed 4000 feet was the required landing distance but indicated that they did not check the landing distance charts. |
| 10-01 | The reason the first officer retracted the flaps and suggested raising the gear could not be determined from the available information, these actions were inconsistent with company stall recovery procedures and training. |
| 91-02 | “I’ll just do a quick procedure turn headed back in, so I’m not going to straighten out on the thing, the localizer, just teardrop and come right back around and land.” The FO [First Officer] simply responded “OK”. |
| 94-06 | The captain actively moved the power levers from the flight idle gate into the beta range for undetermined reasons. Operation of the propellers in the beta range while in flight is prohibited by the airplane flight manual. |
| 06-01 | About 1912:02, the captain transmitted a burp over the ARTCC [Air Route Traffic Control Center] radio frequency that would have been heard by other pilots and air traffic controllers. An unknown voice on the radio frequency responded to the captain’s burp, stating, “nice tone”, and the [cockpit voice recorder] CVR recorded the accident pilot’s chuckling. About 1912:53, the captain talked about deliberately dropping a flight manual on a passenger whose foot had intruded into the cockpit. The first officer engaged in banter with the captain, and both pilots used informal, nonstandard terminology during the flight. |
| 96-07 | The captain was not authorized under the COM to allow the first officer to fly the airplane. The captain told investigators that he was not familiar with the section of the COM that indicated that he was not supposed to share flying duties with the first officer. |
| Accident Report | Examples |
|---|---|
| 94-01 | Fifty feet, the first officer stated, “I’m gonna go around.” The captain stated, “No, no, no I got it” The first officer responded, “You got the airplane” As the first officer said the world “airplane”. The automatic voice said “thirty”. The captain took control and landed the airplane. |
| 11-02 | Following the application of power, the airspeed began increasing. At 0435:40, the first officer asked, “should I go around,” and the captain replied, “no,” and then stated, “keep descending.” |
| 91-05 | The captain became overly reliant on the first officer. This contributed to the runway incursion. The captain knew there was something wrong, he even questioned but acknowledged the FO’s instructions. |
| 06-01 | After hearing the weather observation, the captain commented, “we’re not getting in...we don’t have an ILS [instrument landing system].” The first officer responded, “I know...go all this [expletive] way. Well, let’s try it.” The captain responded, “yeah, we’ll try it.” About 30 s later, the captain said, “I don’t want to...go all the way out here for nothing tonight,” and moments later said, “I’ll be so happy when we have an ILS everywhere we go.” The first officer concurred, and the captain continued, “I thought we were gonna have it easy tonight.” |
| 97-01 | The first officer told Safety Board investigators that his goal after recognizing that the flaps were not extended was to get the captain to initiate a go-around. Thirty seconds before touchdown, the first officer stated “want to take it around?” and the captain replied “no that’s alright. * keep your speed up here about uh.” When the captain denied the first officer’s request to go around and told him to keep his speed up, the first officer did not challenge the captain’s statement. He also did not question the captain to determine his reason(s) for continuing the approach. The first officer stated that there was no time for discussion with the captain because the approach was so fast. The first officer’s failure to question the captain’s decision to continue the approach was inconsistent with the CRM training he had received that emphasized the importance of sharing doubts with other crewmembers and quickly resolving conflicts. |
| 95-03 | During the course of performing the missed approach procedure, the first officer acted, without challenge, to a command from the captain to “down, push it down.” |
| Accident Report | Examples |
|---|---|
| 01-02 | The cockpit voice recorder indicated that flight crew had discussed the weather and the needed to expedite the Approach. The captain stated “we got to get over there quick.” |
| 95-01 | The pilots failed to conduct a prestart checklist properly and, subsequently, failed to observe the illuminated light on the annunciator panel. A second opportunity to detect the status of the pitot heat knob was the annunciator panel check just before takeoff. In this case, the first officer called checklist items without the captain’s request and without using normal challenge and response procedures as the airplane was being taxied into position for takeoff. The pilots appeared to be rushed, and there is no evidence that the first officer actually observed the annunciator panel. |
| 94-06 | The captain stated “man we’re almost the speed of heat here, two sixty four or two sixty three… sixty two” he said “gosh, we gonna come down.” |
| 94-01 | The flight crew ignored the present weather conditions and continued the approach to land even during the unestablished approach, the Captain took the flight controls at the last moment when it was too late to correct or execute a go around. |
| 05-02 | The Captain fixated on landing the airplane with a disregard for any alternative course of action such as performing a go-around. |
| Accident Report | Examples |
|---|---|
| 14-02 | The airplane continued to descend at 1500 fpm and passed through and continued below the desired glidepath. |
| 91-02 | Captain descended below 3000 feet prior to establishing the airplane on final approach course, contrary to directions on the approach plate and establish requirements […] captain did not have the runway environment in sight when he told the first officer to continue the approach. |
| 06-01 | The captain, while acting as pilot flying, descended below the MDA [minimum descent altitude] after supposedly having the approach lights in sight. The airplane struck trees and crashed just short of the runway. |
| 08-01 | The MDA for the localizer (glideslope out) approach to runway 28 was 429 feet [above ground level] agl. No CVR evidence or post-accident interview information indicated that either crewmember had the runway environment in sight by that altitude. |
| 96-05 | The captain initially did not recognize the descent below MDA, and he failed to react immediately when he was alerted to the altitude deviation by the first officer. |
| Accident Report | Examples |
|---|---|
| 04-04 | Investigation determined that pilots have generally had little exposure to, and therefore may not fully understand, the effect of large rudder pedals inputs in normal flight or the mechanism by which rudder deflections induce roll on a transport category airplane. |
| 01-02 | An unidentified voice in the cockpit stated, “a…. we’ are off course.” In a post-accident interview, the first officer stated that he thought the airplane was stabilized until about 400 feet above the field elevation, at which point the airplane drifted to the right. |
| 05-02 | A review of the first officer’s medical record from his personal psychiatrist revealed that, in July 2001, he began seeing the psychiatrist for treatment of various anxiety-related symptoms. The psychiatrist prescribed alprazolam to treat the first officer condition. Common side effects of alprazolam include drowsiness and light-headedness. |
| 11-02 | Flight crew’s failure to monitor and maintain a minimum safe airspeed while executing an instrument approach in icing conditions, which resulted in an aerodynamic stall at low altitude. |
| 91-05 | About ½ min later, the first officer stated, “guess we turn here.” When the captain expressed some doubt about this left turn, the first officer replied, “Near as I can tell. Man, I can’t see out here.” |
| 91-05 | A lack of proper crew coordination, including a virtual reversal of roles by the DC9 pilots, which led to their failure to stop taxing their airplane and alert ground controller of their positional uncertainty in a timely manner before and after intruding onto the active runway. |
| 93-02 | He believed that the snow had “all but stopped” and was more concerned about the amount of vehicular traffic, such as sweepers and plows, than he was about the snowfall. |
| 06-01 | Captain asked, “what do you think?,” and the first officer responded, “I can’t see [expletive].” About 2 s later, as the airplane continued to descend, the captain stated, “yeah, oh there it is. Approach lights in sight.” Almost immediately, the GPWS annunciated “two hundred” feet. |
| 97-01 | According to the first officer, the captain reached up to the overhead panel as the GPWS was alerting. The captain did not recall doing this and stated that he had interpreted the GPWS alerts as a high sink rate warning. The Captain decided to continue to land from an unstable approach without realizing the gear was up and flaps were up. The result was a wheels up landing at the Houston airport. |
| 06-03 | About 1 min later, the first officer stated, “something’s messed up with this thing,” and, at 0039:07, he asked “why is this thing?” At 0041:21, the first officer stated that the control wheel felt “funny.” He added, “feels like I need a lot of force. It is pushing to the right for some reason. I don’t know why...I don’t know what’s going on.” The first officer then repeated twice that it felt like he needed “a lot of force.” The CVR did not record the captain responding to any of these comments. |
| 10-01 | The reason the captain did not recognize the impending onset of the stick shaker could not be determined from the available evidence but that the first officer’s tasks at the time the low-speed cue was visible would have likely reduced opportunities for her timely recognition of the impending event; the failure of both pilots to detect this situation was the result of a significant breakdown in their monitoring responsibilities and workload management. |
| 06-03 | The flight crew did not monitor the fuel quantity gauges or respond properly to the airplane’s changing handling characteristics. |
| 91-09 | Flight crew’s failure to detect and remove ice contamination from the wings was a causal factor in this accident. |
| Accident Report | Examples |
|---|---|
| 04-04 | The probable cause of this accident was the in-flight separation of the vertical stabilizer as a result of the loads beyond ultimate design that were created by the first officer’s unnecessary and excessive rudder pedal inputs. |
| 01-02 | Continuation of the approach to a landing when the company’s max crosswind was exceeded and use of reverse thrust greater than 1.3 engine per ratio after landing. |
| 05-01 | The excessive vertical and lateral forces on the right main landing gear during the landing exceeded those that the gear was designed to withstand and resulted in the fracture of the outer cylinder and the collapse of the right main landing gear. |
| 06-03 | The captain’s calculations showed the airplane outside of acceptable weight and balance limits. |
| Accident Report | Examples |
|---|---|
| 00-02 | According to flight plan and release documents, the airplane was dispatched to ANC [airport code for Anchorage, Alaska] with left engine thrust reverser inoperative. |
| 05-02 | Executive airline’s manager of training and standards stated that, before the accident, the company did not teach its pilots bounced landing recovery techniques. The manager also stated that he would not want to conduct bounced landing recovery training in the simulator because it was very difficult to demonstrate. |
| 09-03 | Maintenance personnel use of an inappropriate manual engine star procedure, which led to the uncommanded opening of the left engine air turbine starter valve, and subsequent left engine fire. |
| 95-01 | The checklist deviations and other pilot procedural deficiencies noted by the FAA during a special inspection, which included numerous en route inspections about one month before the accident, suggest that the problems identified in this accident regarding improper checklist procedures were systemic at COA [Continental Airlines]. If pilots fail to adhere to procedures during en route inspections by FAA inspectors, they most likely behave in a similar manner when no inspector is present. |
| 96-07 | The first officer stated that when he and his classmates questioned the absence of the [manual], the Flight Safety International simulator instructors informed them that ValuJet wanted them to use the QRH [quick reference handbook] “like a Bible” for abnormal procedures. The first officer indicated that he and his classmates stopped their first simulator session and called the company to get an official determination as to what guidance they should use for abnormal and emergency procedures during routine flight operations; he stated that ValuJet management advised them to use the QRH instead of the manual. |
| 91-09 | The DC-9 Operations Manuals were basically developed by Ryan from the airplane’s previous owner’s Operations Manuals, and certain purported Ryan practices were not incorporated into them. The requirement to conduct an exterior inspection of the airplane at intermediate stops was one of those practices not incorporated. In fact, the preflight inspection requirement in the Ryan DC-9 manual clearly indicated that exterior inspections were required only on originating flights or after the airplane had been left unattended. |
| Accident Report | Examples |
|---|---|
| 05-01 | Proper CRM was not present. The captain never made a comment regarding the deviations or helped the First Officer before landing. |
| 11-02 | The captain commented about the flap problem, neither crewmember discussed a procedure or checklist to address it. The flight crew’s poor communication and failure to follow operating procedures regarding flap asymmetry, showed the lack of proper Crew Resource Management and Negligence as a Flight Crew during the approach. |
| 14-02 | The captain changed the autopilot mode from the previously briefed profile approach to vertical speed mode, initially setting the vertical descend rate to about 700 fpm, then increasing it to 1000 fpm; however, he did not brief the first officer about the autopilot mode change |
| 91-05 | A lack of proper crew coordination, including a virtual reversal of roles by the DC9 pilots, which led to their failure to stop taxing their airplane and alert ground controller of their positional uncertainty in a timely manner before and after intruding onto the active runway. |
| 98-03 | The captain did not adequately manage his crew resources when he failed to call for checklist or to monitor and facilitate the accomplishment of required checklist items. |
| 97-01 | The first officer told Safety Board investigators that his goal after recognizing that the flaps were not extended was to get the captain to initiate a go-around. Thirty seconds before touchdown, the first officer stated “want to take it around?” and the captain replied “no that’s alright, keep your speed up here about uh.” When the captain denied the first officer’s request to go around and told him to keep his speed up, the first officer did not challenge the captain’s statement. He also did not question the captain to determine his reason(s) for continuing the approach. The first officer stated that there was no time for discussion with the captain because the approach was so fast. The first officer’s failure to question the captain’s decision to continue the approach was inconsistent with the CRM training he had received that emphasized the importance of sharing doubts with other crewmembers and quickly resolving conflicts. |
| 92-05 | The flight engineer brought to the captain’s attention the airspeed deviation but the captain never corrected; neither the first officer nor the flight engineer called for a go-around. |
| 95-03 | During the course of performing the missed approach procedure, the first officer acted, without challenge, to a command from the captain to “down, push it down.” |
| 94-01 | The flight crew ignored the present weather conditions and continued the approach to land even during the unestablished approach, the captain took the flight controls at the last moment when it was too late to correct or execute a go around. |
| 92-05 | Shortly thereafter, the cockpit voice recorder CVR revealed comments by the captain on the first officer’s flying technique, such as “If you’re gonna fly that slow you gotta have more flaps,” and “[unintelligible words] still don’t have enough flaps for this speed...add power...you’re not on the glidepath...bring it up to the glidepath,” and “You’re not even on the [expletive] localizer at all.” At 03 13, the captain stated “Okay, we’re gonna have to go around...cause we’re not anywhere near the localizer ... anywhere near it.” |
| 93-04 | Inexplicably, the first officer reacted to the stick shaker by immediately deciding that the captain should be flying and abandoning control of the airplane to the captain without warning or proper coordination. |
| 06-03 | About 1 min later, the first officer stated, “something’s messed up with this thing,” and, at 0039:07, he asked “why is this thing?” At 0041:21, the first officer stated that the control wheel felt “funny.” He added, “feels like I need a lot of force. It is pushing to the right for some reason. I don’t know why...I don’t know what’s going on.” The first officer then repeated twice that it felt like he needed “a lot of force.” The CVR did not record the captain responding to any of these comments. |
| 10-01 | The reason the captain did not recognize the impending onset of the stick shaker could not be determined from the available evidence but that the first officer’s tasks at the time the low-speed cue was visible would have likely reduced opportunities for her timely recognition of the impending event; the failure of both pilots to detect this situation was the result of a significant breakdown in their monitoring responsibilities and workload management. |
| 92-05 | Failure of the crew to recognize and recover from an unusual attitude after experiencing spatial disorientation or an attitude indicator failure during the second missed approach. |
| 06-03 | The flight crew did not monitor the fuel quantity gauges or respond properly to the airplane’s changing handling characteristics. |
| 91-09 | Flight crew’s failure to detect and remove ice contamination from the wings was a causal factor in this accident. |
| Accident Report | Examples |
|---|---|
| 06-01 | The pilots were flying their sixth flight of the day and had flown about 6 h and 14 min in 14 h and 31 min of duty time when the accident occurred. CVR recorded a yawn on the first officer’s channel. |
| 10-01 | Each pilot made an inappropriate decision to use the crew room to obtain rest before the accident flight. |
| 92-05 | There were several obvious “misspeaks” by both pilots (drift vs. crab, and 25 degrees flaps vs. 23 degrees flaps) that may have indicated some degree of fatigue. Notwithstanding the fact that the crewmembers of flight 805 were air cargo operations veterans and had adapted to these types of disrupted work/sleep schedules many times, this experience did not make them immune to the possible adverse effects of fatigue or their ability to function effectively. |
| 08-01 | The captain reported that he received only about 1 h of sleep during the night before the accident and, as a result, asked the first officer to be the flying pilot for the flight. |
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velazquez, J. The Presence of Behavioral Traps in U.S. Airline Accidents: A Qualitative Analysis. Safety 2018, 4, 2. https://doi.org/10.3390/safety4010002
Velazquez J. The Presence of Behavioral Traps in U.S. Airline Accidents: A Qualitative Analysis. Safety. 2018; 4(1):2. https://doi.org/10.3390/safety4010002
Chicago/Turabian StyleVelazquez, Jonathan. 2018. "The Presence of Behavioral Traps in U.S. Airline Accidents: A Qualitative Analysis" Safety 4, no. 1: 2. https://doi.org/10.3390/safety4010002
APA StyleVelazquez, J. (2018). The Presence of Behavioral Traps in U.S. Airline Accidents: A Qualitative Analysis. Safety, 4(1), 2. https://doi.org/10.3390/safety4010002