

Photon Counting Computed Tomography for Accurate Cribriform Plate (Lamina Cribrosa) Imaging in Adult Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Collective
2.2. Computed Tomography Scans
2.3. Image Preparation—Multiplanar Reconstructions
2.4. Image Preparation—Volume Rendering Technique
2.5. Evaluation of Quantitative Parameters
2.6. Evaluation of Qualitative Parameters
2.7. Statistical Analysis
2.8. AI-Assisted Tools
3. Results
3.1. Evaluation of Quantitative Parameters
3.1.1. Signal-to-Noise Ratio
3.1.2. Radiation Dose
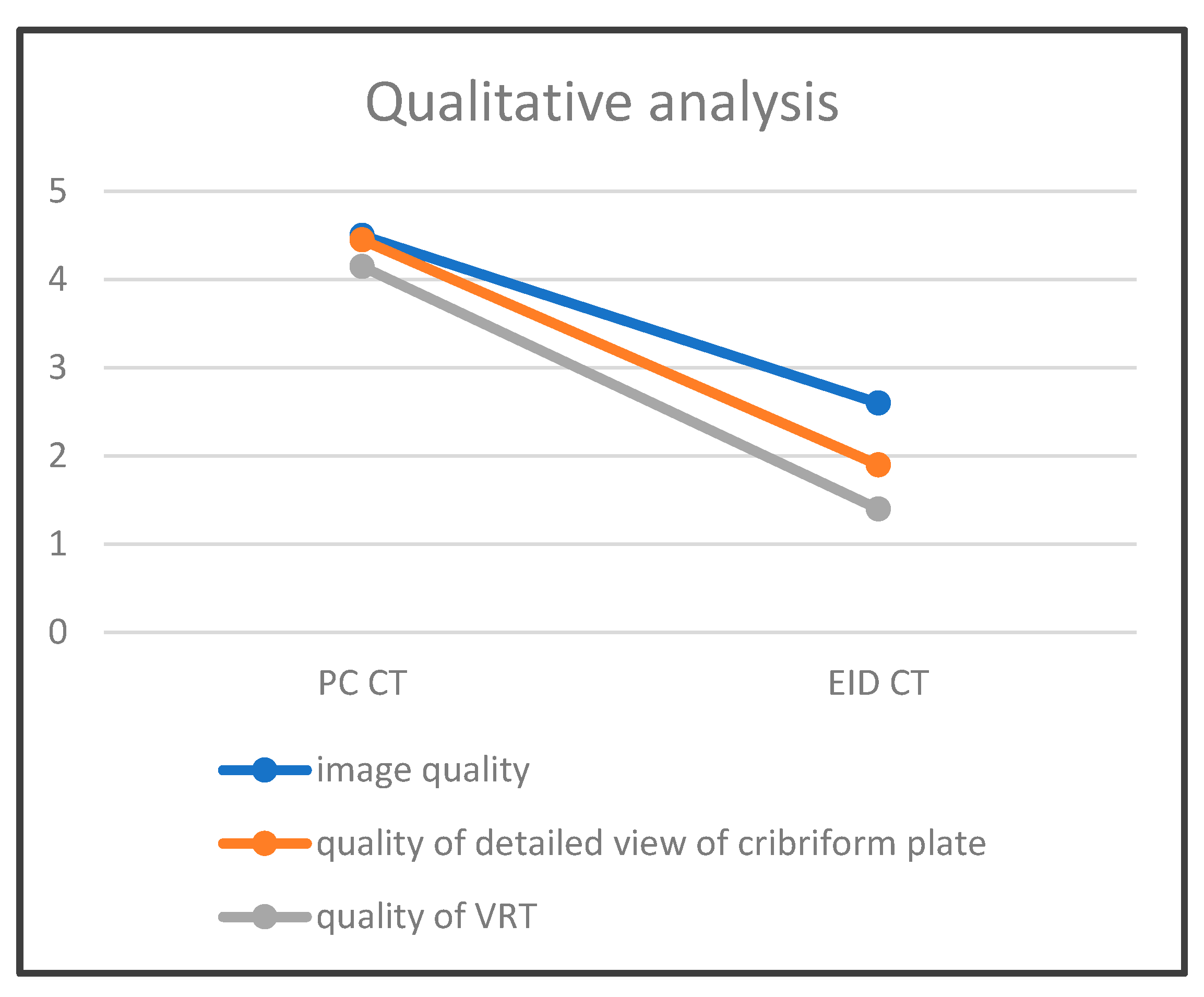
3.2. Evaluation of Qualitative Parameters
3.2.1. Image Quality of CT Scan
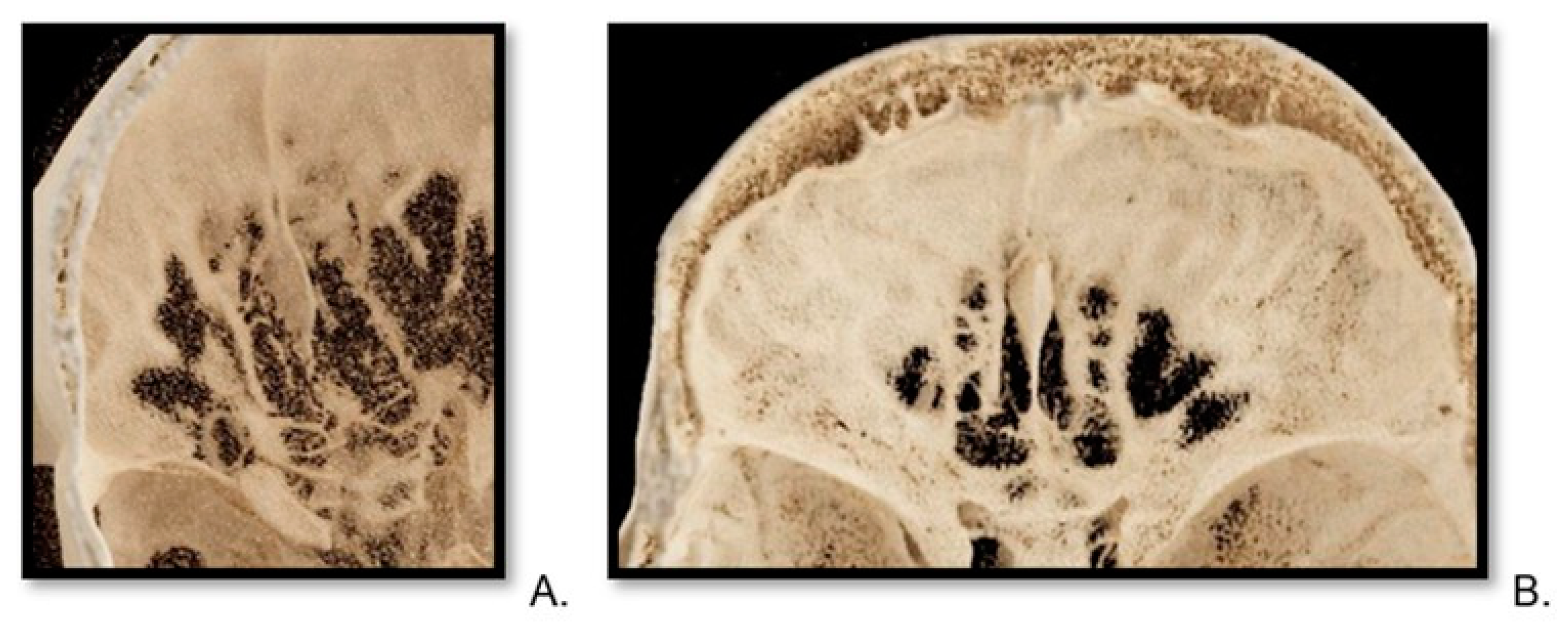
3.2.2. Image Quality of Cribriform Plate Imaging on CT Scan
3.2.3. Quality of VRT Reconstructions
3.2.4. Interobserver Agreement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rydberg, J.; Buckwalter, K.A.; Caldemeyer, K.S.; Phillips, M.D.; Conces, D.J., Jr.; Aisen, A.M.; Persohn, S.A.; Kopecky, K.K. Multisection CT: Scanning techniques and clinical applications. Radiographics 2000, 20, 1787–1806. [Google Scholar] [CrossRef] [PubMed]
- Lell, M.M.; Kachelrieß, M. Recent and Upcoming Technological Developments in Computed Tomography: High Speed, Low Dose, Deep Learning, Multienergy. Investig. Radiol. 2020, 55, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Lell, M.M.; Wildberger, J.E.; Alkadhi, H.; Damilakis, J.; Kachelriess, M. Evolution in Computed Tomography: The Battle for Speed and Dose. Investig. Radiol. 2015, 50, 629–644. [Google Scholar] [CrossRef] [PubMed]
- Lell, M.; Kachelrieß, M. Computed Tomography 2.0: New Detector Technology, AI, and Other Developments. Investig. Radiol. 2023, 58, 587–601. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, S.S.; Leng, S.; Rajendran, K.; Tao, S.; McCollough, C.H. Photon Counting CT: Clinical Applications and Future Developments. IEEE Trans. Radiat. Plasma Med. Sci. 2021, 5, 441–452. [Google Scholar] [CrossRef] [PubMed]
- Willemink, M.J.; Persson, M.; Pourmorteza, A.; Pelc, N.J.; Fleischmann, D. Photon-counting CT: Technical Principles and Clinical Prospects. Radiology 2018, 289, 293–312. [Google Scholar] [CrossRef] [PubMed]
- Esquivel, A.; Ferrero, A.; Mileto, A.; Baffour, F.; Horst, K.; Rajiah, P.S.; Inoue, A.; Leng, S.; McCollough, C.; Fletcher, J.G. Photon-Counting Detector CT: Key Points Radiologists Should Know. Korean J. Radiol. 2022, 23, 854–865. [Google Scholar] [CrossRef]
- Abel, F.; Schubert, T.; Winklhofer, S. Advanced Neuroimaging with Photon-Counting Detector CT. Investig. Radiol. 2023, 58, 472–481. [Google Scholar] [CrossRef]
- So, A.; Nicolaou, S. Spectral Computed Tomography: Fundamental Principles and Recent Developments. Korean J. Radiol. 2021, 22, 86–96. [Google Scholar] [CrossRef]
- Tortora, M.; Gemini, L.; D’Iglio, I.; Ugga, L.; Spadarella, G.; Cuocolo, R. Spectral Photon-Counting Computed Tomography: A Review on Technical Principles and Clinical Applications. J. Imaging. 2022, 8, 112. [Google Scholar] [CrossRef]
- Takahashi, Y.; Higaki, F.; Sugaya, A.; Asano, Y.; Kojima, K.; Morimitsu, Y.; Akagi, N.; Itoh, T.; Matsui, Y.; Hiraki, T. Evaluation of the ear ossicles with photon-counting detector CT. Jpn. J. Radiol. 2024, 42, 158–164. [Google Scholar] [CrossRef]
- Sartoretti, T.; Wildberger, J.E.; Flohr, T.; Alkadhi, H. Photon-counting detector CT: Early clinical experience review. Br. J. Radiol. 2023, 96, 20220544. [Google Scholar] [CrossRef] [PubMed]
- Vasvári, G.; Reisch, R.; Patonay, L. Surgical anatomy of the cribriform plate and adjacent areas. Minim. Invasive Neurosurg. 2005, 48, 25–33. [Google Scholar] [CrossRef]
- Coelho, D.H.; Pence, T.S.; Abdel-Hamid, M.; Costanzo, R.M. Cribriform plate width is highly variable within and between subjects. Auris Nasus Larynx. 2018, 45, 1000–1005. [Google Scholar] [CrossRef]
- Smith, T.D.; Bhatnagar, K.P. Anatomy of the olfactory system. Handb. Clin. Neurol. 2019, 164, 17–28. [Google Scholar] [CrossRef]
- Ganjaei, K.G.; Soler, Z.M.; Mappus, E.D.; Taylor, R.J.; Worley, M.L.; Mulligan, J.K.; Mattos, J.L.; Rowan, N.R.; Garcia, G.J.M.; Dubno, J.R.; et al. Novel Radiographic Assessment of the Cribriform Plate. Am. J. Rhinol. Allergy 2018, 32, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Keros, P. On the practical value of differences in the level of the lamina cribrosa of the ethmoid. Z. Laryngol. Rhinol. Otol. 1962, 41, 809–813. [Google Scholar] [PubMed]
- Preti, A.; Mozzanica, F.; Gera, R.; Gallo, S.; Zocchi, J.; Bandi, F.; Guidugli, G.; Ambrogi, F.; Yakirevitch, A.; Schindler, A.; et al. Horizontal lateral lamella as a risk factor for iatrogenic cerebrospinal fluid leak. Clinical retrospective evaluation of 24 cases. Rhinology 2018, 56, 358–363. [Google Scholar] [CrossRef]
- Abdullah, B.; Chew, S.C.; Aziz, M.E.; Shukri, N.M.; Husain, S.; Joshua, S.W.; Wang, Y.; Snidvongs, K. A new radiological classification for the risk assessment of anterior skull base injury in endoscopic sinus surgery. Sci. Rep. 2020, 10, 4600. [Google Scholar] [CrossRef]
- Fadda, G.L.; Petrelli, A.; Martino, F.; Succo, G.; Castelnuovo, P.; Bignami, M.; Cavallo, G. Anatomic Variations of Ethmoid Roof and Risk of Skull Base Injury in Endoscopic Sinus Surgery: Statistical Correlations. Am. J. Rhinol. Allergy 2021, 35, 871–878. [Google Scholar] [CrossRef]
- Robert, T.; Blanc, R.; Smajda, S.; Ciccio, G.; Redjem, H.; Bartolini, B.; Fahed, R.; Piotin, M. Endovascular treatment of cribriform plate dural arteriovenous fistulas: Technical difficulties and complications avoidance. J. Neurointerv. Surg. 2016, 8, 954–958. [Google Scholar] [CrossRef]
- Patron, V.; Roussel, L.M.; Moreau, S.; Hitier, M. How to identify the anterior cribriform plate in the medial approach to the frontal sinus. Eur. Ann. Otorhinolaryngol. Head. Neck Dis. 2021, 138, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Spera, I.; Cousin, N.; Ries, M.; Kedracka, A.; Castillo, A.; Aleandri, S.; Vladymyrov, M.; Mapunda, J.A.; Engelhardt, B.; Luciani, P.; et al. Open pathways for cerebrospinal fluid outflow at the cribriform plate along the olfactory nerves. EBioMedicine 2023, 91, 104558. [Google Scholar] [CrossRef] [PubMed]
- Rai, R.; Iwanaga, J.; Loukas, M.; Oskouian, R.J.; Tubbs, R.S. Brain Herniation Through the Cribriform Plate: Review and Comparison to Encephaloceles in the Same Region. Cureus 2018, 10, e2961. [Google Scholar] [CrossRef] [PubMed]
- Krmpotić-Nemanić, J.; Padovan, I.; Vinter, I.; Jalsovec, D. Development of the cribriform plate and of the lamina mediana. Ann. Anat. 1998, 180, 555–559. [Google Scholar] [CrossRef]
- Şahan, M.H.; Inal, M.; Muluk, N.B.; Şimşek, G. Cribriform Plate, Crista Galli, Olfactory Fossa and Septal Deviation. Curr. Med. Imaging Rev. 2019, 15, 319–325. [Google Scholar] [CrossRef]
- Appel, E.; Kröpil, P.; Bethge, O.T.; Aissa, J.; Thomas, C.; Antoch, G.; Boos, J. Quality assurance in CT: Implementation of the updated national diagnostic reference levels using an automated CT dose monitoring system. Clin. Radiol. 2018, 73, 677.e13–677.e20. [Google Scholar] [CrossRef]
- Weiss, S.; Westermann, R. Differentiable Direct Volume Rendering. IEEE Trans. Vis. Comput. Graph. 2022, 28, 562–572. [Google Scholar] [CrossRef]
- Hsieh, S.S.; Leng, S.; Yu, L.; Huber, N.R.; McCollough, C.H. A minimum SNR criterion for computed tomography object detection in the projection domain. Med. Phys. 2022, 49, 4988–4998. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Artino, A.R., Jr. Analyzing and interpreting data from likert-type scales. J. Grad. Med. Educ. 2013, 5, 541–542. [Google Scholar] [CrossRef]
- Bishara, A.J.; Li, J.; Conley, C. Informal versus formal judgment of statistical models: The case of normality assumptions. Psychon. Bull. Rev. 2021, 28, 1164–1182. [Google Scholar] [CrossRef] [PubMed]
- Svider, P.F.; Setzen, M.; Baredes, S.; Liu, J.K.; Eloy, J.A. Overview of Sinonasal and Ventral Skull Base Malignancy Management. Otolaryngol. Clin. N. Am. 2017, 50, 205–219. [Google Scholar] [CrossRef]
- Bamimore, M.A.; Marenco-Hillembrand, L.; Ravindran, K.; Perdikis, B.; Rosado-Philippi, J.; Jeevaratnam, S.; Donaldson, A.M.; Olomu, O.U.; Chaichana, K.L. Smell Outcomes in Olfactory Groove Meningioma Resection Through Unilateral versus Bilateral Transcranial Approaches: A Systematic Review and Meta-analysis. World Neurosurg. 2022, 160, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.J.; Lee, M.; Thamboo, A.V. Spatial analysis of transnasal olfactory cleft access: A computed tomography study. Acta Otorhinolaryngol. Ital. 2023, 43, 197–202. [Google Scholar] [CrossRef]
- de Notaris, M.; Topczewski, T.; de Angelis, M.; Enseñat, J.; Alobid, I.; Gondolbleu, A.M.; Soria, G.; Gonzalez, J.B.; Ferrer, E.; Prats-Galino, A. Anatomic skull base education using advanced neuroimaging techniques. World Neurosurg. 2013, 79 (Suppl. S2), S16.e9–S16.e13. [Google Scholar] [CrossRef] [PubMed]
- Yamaoka, H.; Sugawara, T.; Hirabayashi, T.; Wanibuchi, M.; Maehara, T. A Three-Dimensional Anterior and Middle Cranial Fossa Model for Skull Base Surgical Training with Two Layers of the Colored Dura Mater. World Neurosurg. 2023, 176, e575–e586. [Google Scholar] [CrossRef] [PubMed]
- Low, C.M.; Choby, G.; Viozzi, M.; Morris, J.M. Construction of three-dimensional printed anatomic models for frontal sinus education. Neuroradiol. J. 2020, 33, 80–84. [Google Scholar] [CrossRef]
- Gibelli, D.; Cellina, M.; Gibelli, S.; Floridi, C.; Termine, G.; Sforza, C. Anatomical Variations of Anterior Ethmoidal Foramen and Cribriform Plate: Relations with Sex. J. Craniofac. Surg. 2022, 33, e2–e4. [Google Scholar] [CrossRef]
- Ganjaei, K.G.; Soler, Z.M.; Mappus, E.D.; Worley, M.L.; Rowan, N.R.; Garcia, G.J.M.; Matthews, L.J.; Dubno, J.R.; Eckert, M.A.; Schlosser, R.J. Radiologic changes in the aging nasal cavity. Rhinology 2019, 57, 117–124. [Google Scholar] [CrossRef]
- Brady, M.; Rahman, A.; Combs, A.; Venkatraman, C.; Kasper, R.T.; McQuaid, C.; Kwok, W.E.; Wood, R.W.; Deane, R. Cerebrospinal fluid drainage kinetics across the cribriform plate are reduced with aging. Fluids Barriers CNS 2020, 17, 71. [Google Scholar] [CrossRef]
- Tripathi, M.; Kamal Ahuja, C.; Gupta, A.; Kumar Mukherjee, K.; Batish, A.; Buddhiraja, M. Recurrent epistaxis due to cribriform plate dural arteriovenous fistula: Are they related? Should the treatment be from venous, pial or arterial side? Br. J. Neurosurg. 2022, 36, 277–279. [Google Scholar] [CrossRef]
- Erdem, G.; Erdem, T.; Miman, M.C.; Ozturan, O. A radiological anatomic study of the cribriform plate compared with constant structures. Rhinology 2004, 42, 225–229. [Google Scholar]
- Erdogan, S.; Keskin, I.G.; Topdag, M.; Ozturk, M.; Sari, F.; Mutlu, F. Ethmoid roof radiology; analysis of lateral lamella of cribriform plate. Otolaryngol. Pol. 2015, 69, 53–57. [Google Scholar] [CrossRef]
- van Dijk, J.M.; Korsten-Meijer, A.G.; Mazuri, A. Epistaxis caused by a dural AV-fistula at the cribriform plate. Laryngoscope 2014, 124, 2476–2477. [Google Scholar] [CrossRef]
- Rosenberger, E.; Kriet, J.D.; Humphrey, C. Management of nasoethmoid fractures. Curr. Opin. Otolaryngol. Head Neck Surg. 2013, 21, 410–416. [Google Scholar] [CrossRef]
- Wei, J.J.; Tang, Z.L.; Liu, L.; Liao, X.J.; Yu, Y.B.; Jing, W. The management of naso-orbital-ethmoid (NOE) fractures. Chin. J. Traumatol. 2015, 18, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Wrazidlo, R.; Walder, L.; Estler, A.; Gutjahr, R.; Schmidt, B.; Faby, S.; Fritz, J.; Nikolaou, K.; Horger, M.; Hagen, F. Radiation Dose Reduction in Contrast-Enhanced Abdominal CT: Comparison of Photon-Counting Detector CT with 2nd Generation Dual-Source Dual-Energy CT in an oncologic cohort. Acad. Radiol. 2023, 30, 855–862. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H.; Rajendran, K.; Leng, S. Standardization and Quantitative Imaging with Photon-Counting Detector CT. Investig. Radiol. 2023, 58, 451–458. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nr. | Age/Gender | Indication to Conduct Temporal Bone CT | Keros Classification |
|---|---|---|---|
| 1 1 | 21/female | Post-cochlear implantation follow-up | 1 |
| 2 1 | 26/female | Post-cholesteatoma with progressive hearing loss | 3 |
| 3 1 | 30/female | Tympanic membrane perforation | 3 * |
| 4 1 | 43/male | Bilateral external auditory canal atresia | 2 |
| 5 1 | 53/female | Semicircular canal dehiscence | 2 |
| 6 1 | 54/male | Sudden hearing loss | 3 |
| 7 1 | 66/male | Before left-side cochlear implantation | 2 |
| 8 1 | 66/female | Cholesteatoma surgery, suspected recurrence | 2 |
| 9 1 | 67/male | Before a cochlear implantation | 2 |
| 10 1 | 75/male | Before a cochlear implantation | 2 |
| 11 1 | 67/female | Cholesteatoma, otosklerose | 3 |
| 12 1 | 27/female | Cholesteatoma and before cochlear implantation | 3 |
| 13 1 | 23/male | Otorrhoea right, after tympanoplastic | 2 |
| 14 1 | 39/female | Surditas right | 2 |
| 15 1 | 67/female | Tinnitus | 1 |
| 16 1 | 48/male | Before cochlear implantation | 2 |
| 17 1 | 64/female | Before cochlear implantation | 2 |
| 18 1 | 56/female | Postoperative control after petrosal meningioma | 3 |
| 19 1 | 70/female | Before cochlear implantation | 2 |
| 20 1 | 57/female | Before cochlear implantation | 1 |
| 21 2 | 29/female | Suspicion of cholesteatoma | 3 |
| 22 2 | 33/male | Status post-mastoidectomy, suspected complications | 2 |
| 23 2 | 53/male | Before a cochlear implantation | 2 |
| 24 2 | 60/female | Before a cochlear implantation | 2 |
| 25 2 | 61/female | Before a cochlear implantation | 2 |
| 26 2 | 62/male | Bone erosion by squamous cell carcinoma Infiltration | 3 |
| 27 2 | 63/female | Before a cochlear implantation | 2 |
| 28 2 | 65/male | Before a cochlear implantation | 2 |
| 29 2 | 74/male | Revision of a cochlear implantation | 3 |
| 30 2 | 90/female | Malignant external otitis | 2 |
| 31 2 | 43/female | Before a cochlear implantation | 2 |
| 32 2 | 57/female | Cholesteatoma left | 2 |
| 33 2 | 59/female | Cholesteatoma left | 2 |
| 34 2 | 73/female | Glomus tympanicum right | 2 |
| 35 2 | 46/male | Suspicion of otitis externa maligna left | 3 |
| 36 2 | 52/male | Before a cochlear implantation | 2 |
| 37 2 | 82/female | Surtitas bds before a cochlear implantation | 1 |
| 38 2 | 75/female | Before a cochlear implantation | 2 |
| 39 2 | 41/male | Suspicion of cholesteatoma | 3 |
| 40 2 | 34/female | Suspicion of cholesteatoma | 2 |
| Nr. | CTDTI mGy | SNR |
|---|---|---|
| 1 1 | 15.0 | 51.1 |
| 2 1 | 15.2 | 21.3 |
| 3 1 | 13.9 | 30.8 |
| 4 1 | 17.8 | 30.7 |
| 5 1 | 13.7 | 35.4 |
| 6 1 | 14.5 | 34.2 |
| 7 1 | 16.6 | 32.4 |
| 8 1 | 19.4 | 37.4 |
| 9 1 | 16.2 | 33.8 |
| 10 1 | 16.6 | 34.8 |
| 11 1 | 14.6 | 38.8 |
| 12 1 | 15.7 | 48.4 |
| 13 1 | 16.1 | 22.7 |
| 14 1 | 12.3 | 24.0 |
| 15 1 | 14.0 | 35.9 |
| 16 1 | 16.1 | 32.5 |
| 17 1 | 16.2 | 23.3 |
| 18 1 | 14.4 | 25.8 |
| 19 1 | 15.8 | 6.4 |
| 20 1 | 14.8 | 24.4 |
| 21 2 | 32.32 | 5.4 |
| 22 2 | 32.32 | 8.7 |
| 23 2 | 32.32 | 7.2 |
| 24 2 | 32.32 | 12.2 |
| 25 2 | 32.32 | 8.4 |
| 26 2 | 32.32 | 8.9 |
| 27 2 | 32.32 | 9.8 |
| 28 2 | 32.32 | 9.3 |
| 29 2 | 32.32 | 7.9 |
| 30 2 | 32.32 | 8.9 |
| 31 2 | 32.32 | 4.9 |
| 32 2 | 32.32 | 8.2 |
| 33 2 | 32.32 | 8.0 |
| 34 2 | 32.32 | 8.5 |
| 35 2 | 32.32 | 9.8 |
| 36 2 | 32.32 | 7.6 |
| 37 2 | 32.32 | 10.3 |
| 38 2 | 32.32 | 9.6 |
| 39 2 | 32.32 | 5.0 |
| 40 2 | 32.32 | 5.4 |
| Nr. | Image Quality of Imaging of CT Scan | Image Quality of Cribriform Plate on CT Scan | Quality of VRT Reconstructions |
|---|---|---|---|
| 1 1 | 5/4 | 5/4 | 5/5 |
| 2 1 | 5/5 | 5/5 | 5/5 |
| 3 1 | 5/4 | 5/4 | 5/5 |
| 4 1 | 5/5 | 5/4 | 5/5 |
| 5 1 | 5/5 | 5/5 | 5/4 |
| 6 1 | 5/5 | 5/4 | 5/5 |
| 7 1 | 5/5 | 5/5 | 4/4 |
| 8 1 | 5/5 | 5/5 | 5/5 |
| 9 1 | 5/5 | 5/5 | 5/3 |
| 10 1 | 5/5 | 5/4 | 5/5 |
| 11 1 | 5/5 | 5/5 | 5/4 |
| 12 1 | 5/5 | 5/5 | 5/5 |
| 13 1 | 5/5 | 5/4 | 5/4 |
| 14 1 | 5/5 | 4/5 | 5/5 |
| 15 1 | 5/5 | 4/4 | 4/3 |
| 16 1 | 5/4 | 4/3 | 4/4 |
| 17 1 | 5/5 | 5/4 | 3/3 |
| 18 1 | 5/4 | 5/3 | 3/2 |
| 19 1 | 4/3 | 3/2 | 2/2 |
| 20 1 | 5/5 | 5/4 | 4/4 |
| 21 2 | 4/3 | 4/2 | 1/1 |
| 22 2 | 4/3 | 4/3 | 2/2 |
| 23 2 | 2/1 | 2/1 | 3/1 |
| 24 2 | 3/2 | 3/1 | 3/2 |
| 25 2 | 3/2 | 3/1 | 2/1 |
| 26 2 | 3/1 | 3/1 | 2/1 |
| 27 2 | 2/2 | 2/2 | 4/3 |
| 28 2 | 3/3 | 3/2 | 2/2 |
| 29 2 | 2/2 | 2/1 | 2/1 |
| 30 2 | 2/3 | 2/1 | 3/1 |
| 31 2 | 3/3 | 2/2 | 1/1 |
| 32 2 | 3/3 | 2/1 | 1/1 |
| 33 2 | 3/3 | 2/2 | 1/1 |
| 34 2 | 3/4 | 3/2 | 2/1 |
| 35 2 | 3/3 | 2/2 | 2/1 |
| 36 2 | 3/3 | 2/1 | 1/1 |
| 37 2 | 3/3 | 2/2 | 1/2 |
| 38 2 | 2/3 | 2/1 | 1/1 |
| 39 2 | 3/3 | 2/2 | 1/1 |
| 40 2 | 3/3 | 2/2 | 1/1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klempka, A.; Ackermann, E.; Clausen, S.; Groden, C. Photon Counting Computed Tomography for Accurate Cribriform Plate (Lamina Cribrosa) Imaging in Adult Patients. Tomography 2024, 10, 400-414. https://doi.org/10.3390/tomography10030031
Klempka A, Ackermann E, Clausen S, Groden C. Photon Counting Computed Tomography for Accurate Cribriform Plate (Lamina Cribrosa) Imaging in Adult Patients. Tomography. 2024; 10(3):400-414. https://doi.org/10.3390/tomography10030031
Chicago/Turabian StyleKlempka, Anna, Eduardo Ackermann, Sven Clausen, and Christoph Groden. 2024. "Photon Counting Computed Tomography for Accurate Cribriform Plate (Lamina Cribrosa) Imaging in Adult Patients" Tomography 10, no. 3: 400-414. https://doi.org/10.3390/tomography10030031
APA StyleKlempka, A., Ackermann, E., Clausen, S., & Groden, C. (2024). Photon Counting Computed Tomography for Accurate Cribriform Plate (Lamina Cribrosa) Imaging in Adult Patients. Tomography, 10(3), 400-414. https://doi.org/10.3390/tomography10030031