
A Systematic Review and Meta-Analysis of Exercise Beneficial for Locomotion in Community-Dwelling Elderly People with Sarcopenia




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy and Selection of Studies
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.2.3. Literature Search Strategy
2.2.4. Study Selection and Data Extraction
2.2.5. Quality Assessment
2.3. Strategy for Data Synthesis
3. Results
3.1. Literature Search and Characteristics of the Included Randomized Clinical Trials
3.2. Risk of Bias Assessment
3.3. Exercise for Individuals with Sarcopenia
3.4. Effectiveness of Exercise on Muscle Mass
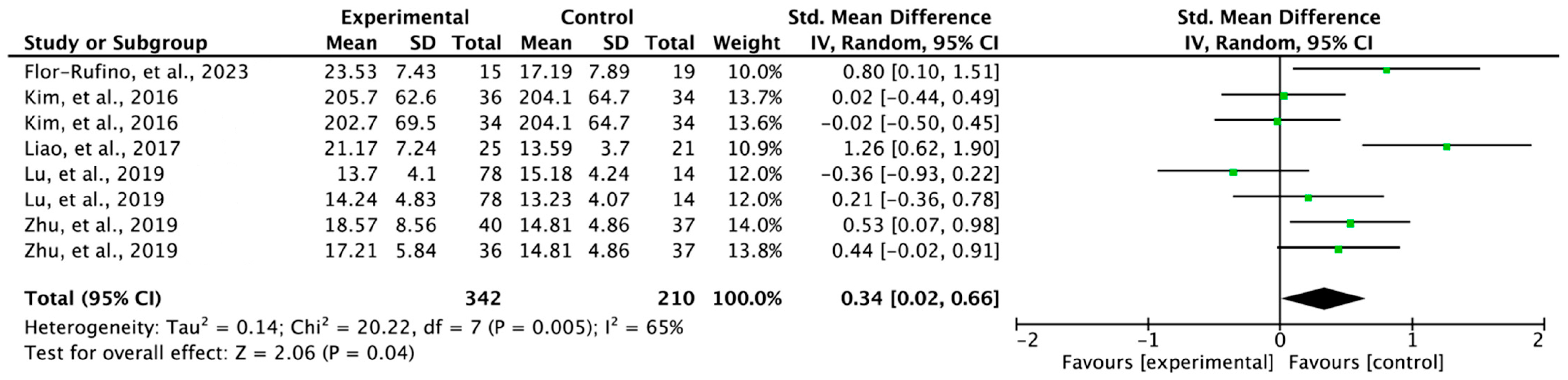
3.5. Effectiveness of Exercise on Lower Extremity Strength
3.6. Effectiveness of Exercise on Gait Speed
3.7. Publication Bias
4. Discussion
4.1. Muscle Mass in Individuals with Sarcopenia
4.2. Lower Extremity Strength in Individuals with Sarcopenia
4.3. Gait Speed in Individuals with Sarcopenia
4.4. Exercise Intervention for Locomotion in Sarcopenic Individuals
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef] [PubMed]
- Deschenes, M.R. Effects of aging on muscle fibre type and size. Sport. Med. 2004, 34, 809–824. [Google Scholar] [CrossRef]
- An, H.Y.; Chen, W.; Wang, C.W.; Yang, H.F.; Huang, W.T.; Fan, S.Y. The Relationships between Physical Activity and Life Satisfaction and Happiness among Young, Middle-Aged, and Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 4817. [Google Scholar] [CrossRef]
- Rosenberg, I.H. Sarcopenia: Origins and clinical relevance. J. Nutr. 1997, 127, 990s–991s. [Google Scholar] [CrossRef] [Green Version]
- Vellas, B.; Fielding, R.A.; Bens, C.; Bernabei, R.; Cawthon, P.M.; Cederholm, T.; Cruz-Jentoft, A.J.; Del Signore, S.; Donahue, S.; Morley, J.; et al. Implications of ICD-10 for Sarcopenia Clinical Practice and Clinical Trials: Report by the International Conference on Frailty and Sarcopenia Research Task Force. J. Frailty Aging 2018, 7, 2–9. [Google Scholar] [CrossRef]
- Wang, H.; Huang, W.Y.; Zhao, Y. Efficacy of Exercise on Muscle Function and Physical Performance in Older Adults with Sarcopenia: An Updated Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8212. [Google Scholar] [CrossRef]
- Billot, M.; Calvani, R.; Urtamo, A.; Sánchez-Sánchez, J.L.; Ciccolari-Micaldi, C.; Chang, M.; Roller-Wirnsberger, R.; Wirnsberger, G.; Sinclair, A.; Vaquero-Pinto, N. Preserving mobility in older adults with physical frailty and sarcopenia: Opportunities, challenges, and recommendations for physical activity interventions. Clin. Interv. Aging 2020, 15, 1675–1690. [Google Scholar] [CrossRef]
- Groessl, E.J.; Kaplan, R.M.; Rejeski, W.J.; Katula, J.A.; Glynn, N.W.; King, A.C.; Anton, S.D.; Walkup, M.; Lu, C.J.; Reid, K.; et al. Physical Activity and Performance Impact Long-term Quality of Life in Older Adults at Risk for Major Mobility Disability. Am. J. Prev. Med. 2019, 56, 141–146. [Google Scholar] [CrossRef]
- Kim, H.; Jung, J.; Park, S.; Joo, Y.; Lee, S.; Lee, S. Effects of Repetitive Transcranial Magnetic Stimulation on the Primary Motor Cortex of Individuals with Fibromyalgia: A Systematic Review and Meta-Analysis. Brain Sci. 2022, 12, 570. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G.; Group, C.S.M. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; pp. 241–284. [Google Scholar]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Lu, Y.; Niti, M.; Yap, K.B.; Tan, C.T.Y.; Zin Nyunt, M.S.; Feng, L.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; et al. Assessment of Sarcopenia Among Community-Dwelling At-Risk Frail Adults Aged 65 Years and Older Who Received Multidomain Lifestyle Interventions: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open. 2019, 2, e1913346. [Google Scholar] [CrossRef] [Green Version]
- Yuenyongchaiwat, K.; Akekawatchai, C. Beneficial effects of walking-based home program for improving cardio-respiratory performance and physical activity in sarcopenic older people: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2022, 58, 838–844. [Google Scholar] [CrossRef]
- Morawin, B.; Tylutka, A.; Chmielowiec, J.; Zembron-Lacny, A. Circulating Mediators of Apoptosis and Inflammation in Aging; Physical Exercise Intervention. Int. J. Environ. Res. Public Health 2021, 18, 3165. [Google Scholar] [CrossRef]
- Chang, K.V.; Wu, W.T.; Huang, K.C.; Han, D.S. Effectiveness of early versus delayed exercise and nutritional intervention on segmental body composition of sarcopenic elders—A randomized controlled trial. Clin. Nutr. 2021, 40, 1052–1059. [Google Scholar] [CrossRef]
- Seo, M.W.; Jung, S.W.; Kim, S.W.; Lee, J.M.; Jung, H.C.; Song, J.K. Effects of 16 Weeks of Resistance Training on Muscle Quality and Muscle Growth Factors in Older Adult Women with Sarcopenia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 6762. [Google Scholar] [CrossRef]
- Vasconcelos, K.S.; Dias, J.M.; Araújo, M.C.; Pinheiro, A.C.; Moreira, B.S.; Dias, R.C. Effects of a progressive resistance exercise program with high-speed component on the physical function of older women with sarcopenic obesity: A randomized controlled trial. Braz. J. Phys. Ther. 2016, 20, 432–440. [Google Scholar] [CrossRef]
- Liao, C.D.; Tsauo, J.Y.; Lin, L.F.; Huang, S.W.; Ku, J.W.; Chou, L.C.; Liou, T.H. Effects of elastic resistance exercise on body composition and physical capacity in older women with sarcopenic obesity: A CONSORT-compliant prospective randomized controlled trial. Medicine 2017, 96, e7115. [Google Scholar] [CrossRef]
- Zhu, L.Y.; Chan, R.; Kwok, T.; Cheng, K.C.; Ha, A.; Woo, J. Effects of exercise and nutrition supplementation in community-dwelling older Chinese people with sarcopenia: A randomized controlled trial. Age Ageing 2019, 48, 220–228. [Google Scholar] [CrossRef]
- Kim, H.; Kim, M.; Kojima, N.; Fujino, K.; Hosoi, E.; Kobayashi, H.; Somekawa, S.; Niki, Y.; Yamashiro, Y.; Yoshida, H. Exercise and Nutritional Supplementation on Community-Dwelling Elderly Japanese Women With Sarcopenic Obesity: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2016, 17, 1011–1019. [Google Scholar] [CrossRef]
- Flor-Rufino, C.; Barrachina-Igual, J.; Pérez-Ros, P.; Pablos-Monzó, A.; Sanz-Requena, R.; Martínez-Arnau, F.M. Fat infiltration and muscle hydration improve after high-intensity resistance training in women with sarcopenia. A randomized clinical trial. Maturitas 2023, 168, 29–36. [Google Scholar] [CrossRef]
- Babic, A.; Pijuk, A.; Brázdilová, L.; Georgieva, Y.; Raposo Pereira, M.A.; Poklepovic Pericic, T.; Puljak, L. The judgement of biases included in the category “other bias” in Cochrane systematic reviews of interventions: A systematic survey. BMC Med. Res. Methodol. 2019, 19, 77. [Google Scholar] [CrossRef] [Green Version]
- Bao, W.; Sun, Y.; Zhang, T.; Zou, L.; Wu, X.; Wang, D.; Chen, Z. Exercise Programs for Muscle Mass, Muscle Strength and Physical Performance in Older Adults with Sarcopenia: A Systematic Review and Meta-Analysis. Aging Dis. 2020, 11, 863–873. [Google Scholar] [CrossRef]
- Hanach, N.I.; McCullough, F.; Avery, A. The Impact of Dairy Protein Intake on Muscle Mass, Muscle Strength, and Physical Performance in Middle-Aged to Older Adults with or without Existing Sarcopenia: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 59–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, L.; Mao, L.; Feng, Y.; Ainsworth, B.E.; Liu, Y.; Chen, N. Effects of different exercise training modes on muscle strength and physical performance in older people with sarcopenia: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 708. [Google Scholar] [CrossRef] [PubMed]
- Vlietstra, L.; Hendrickx, W.; Waters, D.L. Exercise interventions in healthy older adults with sarcopenia: A systematic review and meta-analysis. Australas. J. Ageing 2018, 37, 169–183. [Google Scholar] [CrossRef]
- Churchward-Venne, T.A.; Tieland, M.; Verdijk, L.B.; Leenders, M.; Dirks, M.L.; de Groot, L.C.; van Loon, L.J. There Are No Nonresponders to Resistance-Type Exercise Training in Older Men and Women. J. Am. Med. Dir. Assoc. 2015, 16, 400–411. [Google Scholar] [CrossRef]
- Akune, T.; Muraki, S.; Oka, H.; Tanaka, S.; Kawaguchi, H.; Nakamura, K.; Yoshimura, N. Exercise habits during middle age are associated with lower prevalence of sarcopenia: The ROAD study. Osteoporos. Int. 2014, 25, 1081–1088. [Google Scholar] [CrossRef]
- Wu, P.Y.; Huang, K.S.; Chen, K.M.; Chou, C.P.; Tu, Y.K. Exercise, Nutrition, and Combined Exercise and Nutrition in Older Adults with Sarcopenia: A Systematic Review and Network Meta-analysis. Maturitas 2021, 145, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, W.K.; Williams, J.; Atherton, P.; Larvin, M.; Lund, J.; Narici, M. Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Front. Physiol. 2012, 3, 260. [Google Scholar] [CrossRef] [Green Version]
- Delmonico, M.J.; Harris, T.B.; Visser, M.; Park, S.W.; Conroy, M.B.; Velasquez-Mieyer, P.; Boudreau, R.; Manini, T.M.; Nevitt, M.; Newman, A.B.; et al. Longitudinal study of muscle strength, quality, and adipose tissue infiltration. Am. J. Clin. Nutr. 2009, 90, 1579–1585. [Google Scholar] [CrossRef] [Green Version]
- Clark, B.C.; Manini, T.M. Functional consequences of sarcopenia and dynapenia in the elderly. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 271–276. [Google Scholar] [CrossRef] [Green Version]
- Chow, Z.S.; Moreland, A.T.; Macpherson, H.; Teo, W.P. The Central Mechanisms of Resistance Training and Its Effects on Cognitive Function. Sports Med. 2021, 51, 2483–2506. [Google Scholar] [CrossRef] [PubMed]
- Herda, T.J. Resistance exercise training and the motor unit. Eur. J. Appl. Physiol. 2022, 122, 2019–2035. [Google Scholar] [CrossRef] [PubMed]
- Škarabot, J.; Brownstein, C.G.; Casolo, A.; Del Vecchio, A.; Ansdell, P. The knowns and unknowns of neural adaptations to resistance training. Eur. J. Appl. Physiol. 2021, 121, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, D.A.; Kamen, G.; Frost, G. Neural adaptations to resistive exercise: Mechanisms and recommendations for training practices. Sport. Med. 2006, 36, 133–149. [Google Scholar] [CrossRef]
- Adams, L.M.; Turk, D.C. Central sensitization and the biopsychosocial approach to understanding pain. J. Appl. Biobehav. Res. 2018, 23, e12125. [Google Scholar] [CrossRef]
- Dhillon, R.J.; Hasni, S. Pathogenesis and Management of Sarcopenia. Clin. Geriatr. Med. 2017, 33, 17–26. [Google Scholar] [CrossRef] [Green Version]
- Shu, X.; Lin, T.; Wang, H.; Zhao, Y.; Jiang, T.; Peng, X.; Yue, J. Diagnosis, prevalence, and mortality of sarcopenia in dialysis patients: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 145–158. [Google Scholar] [CrossRef]
- Xu, J.; Wan, C.S.; Ktoris, K.; Reijnierse, E.M.; Maier, A.B. Sarcopenia Is Associated with Mortality in Adults: A Systematic Review and Meta-Analysis. Gerontology 2022, 68, 361–376. [Google Scholar] [CrossRef]
- Zhang, X.M.; Wu, X. Comment on ‘Prevalence of depression in patients with sarcopenia and correlation between the two diseases: Systematic review and meta-analysis’. J. Cachexia Sarcopenia Muscle 2022, 13, 2257–2258. [Google Scholar] [CrossRef]
- Li, Z.; Tong, X.; Ma, Y.; Bao, T.; Yue, J. Prevalence of depression in patients with sarcopenia and correlation between the two diseases: Systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 128–144. [Google Scholar] [CrossRef]
- Delibaş, D.H.; Eşkut, N.; İlhan, B.; Erdoğan, E.; Top Kartı, D.; Yılmaz Küsbeci, Ö.; Bahat, G. Clarifying the relationship between sarcopenia and depression in geriatric outpatients. Aging Male 2021, 24, 29–36. [Google Scholar] [CrossRef]
- Nipp, R.D.; Fuchs, G.; El-Jawahri, A.; Mario, J.; Troschel, F.M.; Greer, J.A.; Gallagher, E.R.; Jackson, V.A.; Kambadakone, A.; Hong, T.S.; et al. Sarcopenia Is Associated with Quality of Life and Depression in Patients with Advanced Cancer. Oncologist 2018, 23, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dragašević-Mišković, N.T.; Bobić, V.; Kostić, M.; Stanković, I.; Radovanović, S.; Dimitrijević, K.; Svetel, M.; Petrović, I.; Đurić-Jovičić, M. Impact of depression on gait variability in Parkinson’s disease. Clin. Neurol. Neurosurg. 2021, 200, 106324. [Google Scholar] [CrossRef]
- Naharci, M.I.; Katipoglu, B.; Veizi, B.; Tasci, I. Gait Speed is independently associated with Depression Symptoms in Mild Cognitive Impairment. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2022, 29, 637–650. [Google Scholar] [CrossRef]
- Park, S.-H.; Rho, Y. Which intervention is more effective in improving sarcopenia in older adults? a systematic review with meta-analysis of randomized controlled trials. Mech. Ageing Dev. 2022, 210, 111773. [Google Scholar] [CrossRef]
- Zhao, H.; Cheng, R.; Song, G.; Teng, J.; Shen, S.; Fu, X.; Yan, Y.; Liu, C. The Effect of Resistance Training on the Rehabilitation of Elderly Patients with Sarcopenia: A Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 15491. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants | Outcomes | Study Design |
|---|---|---|
| Elderly OR older adults OR aged | Gait speed OR walking speed OR locomotion OR muscle activity OR muscle strength OR lower extremity strength | Randomized controlled trial |
| Sarcopenia |
| Study | Age, Sample Size | Time Points of Measurement | Intervention Therapeutic Intensity | Outcomes: Unit |
|---|---|---|---|---|
| Chang et al., 2021 [15] | 74.3 ± 5.8, EG = 29; 75.7 ± 5.9, CG = 28 | 12 weeks | Exercise and nutritional intervention: exercise twice a week, nutritional interventions provided daily (two sticks of branched-chain amino acids daily and two tablets of calcium and vitamin D3 supplement daily). Control = Home exercise program. | Muscle mass: g |
| Flor-Rufino et al., 2023 [21] | 79.9 ± 7.2, EG = 20; 79.6 ± 7.7, CG = 18 | 6 months | High-intensity resistance training: 6 exercise programs of 65 min per session twice a week for a total of 6 months. Control = Telephone follow-up to assess general health. | Muscle mass: kg/m2 LE strength: kg Gait speed: m/s |
| Kim et al., 2016 [20] | 80.9 ± 4.2, EG 1 = 36; 81.4 ± 4.3, EG 2 = 34; 81.1 ± 5.1, CG = 34 | 3 months | EG 1 = Exercise plus nutrition EG 2 = Physical comprehensive training program; each exercise was conducted for 60 min twice a week for a total of 3 months. Control = Health education. | Muscle mass: kg LE strength: N Gait speed: m/s |
| Liao et al., 2017 [18] | 66.4 ± 4.5, EG = 25; 68.4 ± 5.9, CG = 21 | 12 weeks | Elastic resistance exercises performed three times a week for a total of 12 weeks; each workout session included a 10 min general warm-up, resistance training (35–40 min), and finally a cool-down routine. Control = No exercise intervention provided. | LE strength: N Gait speed: m/s |
| Lu et al., 2019 [12] | 69.8 ± 4.3, EG = 33; 71.0 ± 6.7, CG = 33 | 3 months 6 months | Complex intervention: physical exercise, nutritional enhancement, cognitive training, and integrative interventions or standard care for 6 months Control = Standard care. | Muscle mass: kg/m2 LE strength: kg Gait speed: s |
| Morawin et al., 2021 [14] | Mean range: 69.8 to 73.6, EG = 27 CG = 36 | 4 months 6 months | Tai-Chi training: exercises were performed twice a week, and 2–4 exercises were added monthly. Control = Health education. | Gait speed: m/s |
| Seo et al., 2021 [16] | 70.3 ± 5.38, EG = 12; 72.9 ± 4.75, CG = 10 | 16 weeks | Resistance training: a total of 48 sessions were provided three times per week. Each training session included a 5 min warm-up, 50 min resistance exercise, and a 5 min cool-down. Control = No exercise intervention provided. | Muscle mass: kg Gait speed: m/s |
| Vasconcelos et al., 2016 [17] | 72 ± 4.6, EG = 14; 72 ± 3.6, CG = 14 | 10 weeks | Resistance exercise: 10-week resistance exercise program for 1 h twice per week (designed to improve lower extremity strength, power, and endurance through open and closed kinetic chain exercises) Control = Monitored by therapists once per week by phone for a 10-week period. | Gait speed: m/s |
| Yuenyongchaiwat and Akekawatchai, 2022 [13] | 69.23 ± 6.71, EG = 28; 71.93 ± 5.19, CG = 29 | 12 weeks | Walking-based home program: the intervention program increased PA by encouraging walking, ≥7500 steps daily, for 5 days/week for a total of 12 weeks. Control = Routine daily activities. | Muscle mass: kg/m2 Gait speed: m/s |
| Zhu et al., 2019 [19] | 74.5 ± 7.1, EG 1 = 40; 74.8 ± 6.9, EG 2 = 36; 72.2 ± 6.6, CG = 37 | 12 weeks | EG 1 = Exercise: group exercise and one home exercise twice a week for 12 weeks. EG 2 = Combined exercise program plus nutrition supplement: the nutrition supplement consisted of two sachets of Ensure NutriVigor daily from baseline to 12 weeks. Control = Waitlist. | Muscle mass: kg/m2 LE strength: kg Gait speed: m/s |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, S.; Kim, G.; Kim, H. A Systematic Review and Meta-Analysis of Exercise Beneficial for Locomotion in Community-Dwelling Elderly People with Sarcopenia. J. Funct. Morphol. Kinesiol. 2023, 8, 92. https://doi.org/10.3390/jfmk8030092
Song S, Kim G, Kim H. A Systematic Review and Meta-Analysis of Exercise Beneficial for Locomotion in Community-Dwelling Elderly People with Sarcopenia. Journal of Functional Morphology and Kinesiology. 2023; 8(3):92. https://doi.org/10.3390/jfmk8030092
Chicago/Turabian StyleSong, Seunghyeok, Gushik Kim, and Hyunjoong Kim. 2023. "A Systematic Review and Meta-Analysis of Exercise Beneficial for Locomotion in Community-Dwelling Elderly People with Sarcopenia" Journal of Functional Morphology and Kinesiology 8, no. 3: 92. https://doi.org/10.3390/jfmk8030092
APA StyleSong, S., Kim, G., & Kim, H. (2023). A Systematic Review and Meta-Analysis of Exercise Beneficial for Locomotion in Community-Dwelling Elderly People with Sarcopenia. Journal of Functional Morphology and Kinesiology, 8(3), 92. https://doi.org/10.3390/jfmk8030092