1. Introduction
Following outbreaks of measles epidemics in recent years, especially the incident connected with Disneyland in early 2015, and widespread outbreaks in Ohio in 2014 [
1], the arguments over children’s vaccination have become a serious problem in public health [
1,
2].
Measles is a highly contagious infectious disease caused by the (red) measles virus. Symptoms usually develop 10–12 days after exposure, during which time the virus multiplies in the upper respiratory tract, and lasts 7–10 days. Initial symptoms typically include fever, cough, runny nose, and inflamed eyes. A rash typically begins 2–4 days after the start of symptoms, spreads from the head downwards (neck, arms, legs), and disappears in the same order [
1]. According to the World Health Organization (WHO) [
2], most measles-related deaths are linked to complications that develop during the disease. Serious complications are more common among children under the age of 5 or adults over 30, and may include blindness, encephalitis, severe diarrhea and dehydration, ear infections, severe respiratory infections, mainly among patients with a vitamin A deficiency or a repressed immune system (such as AIDS patients).
The treatment of measles is non-specific, except palliative treatment of symptoms, and it takes time until the immune system overcomes the virus. WHO recommends vitamin A to treat measles, consisting of two doses of 50,000 IU for infants under the age of six months, and 100,000 IU for infants up to a year old, and 200,000 IU for children over one year old. Vitamin A additives are considered effective in reducing measles-related mortality from various causes including diarrhea [
3]. Measles is highly contagious, so that if one is sick, nine out of ten people in their close vicinity will probably be infected if they are not protected [
1,
2,
3,
4].
The US Centers for Disease Control and Prevention (CDC) reported 1249 new cases of measles in the US between January and September 2019—the highest annual number since 1992. According to WHO, 112,163 children and adults were infected in Europe in 2019, and in 2018, 28,124 cases of measles were reported [
4], in contrast to 2017, when 23,927 cases were reported. According to the Epidemiology Division of the Ministry of Health in Israel, the annual number of measles cases in 2019 was 1427, in contrast with 2018, when there were 2872 reported cases. WHO considers measles to still be one of the main causes of child mortality throughout the world, despite the existence of a vaccine that actually prevents it [
5].
1.1. The Measles Vaccine
The vaccine against measles consists of an attenuated live virus administered via a subcutaneous injection, and is a trivalent vaccine that acts against Measles, Mumps and Rubella (MMR). In some countries, the vaccine acts against four diseases: Measles, Mumps, Rubella and Varicella (MMRV) [
6]. The vaccination is administered in two doses. The effectivity of the vaccine is 95% after the first dose and 99% after the second dose. Serological and immunological tests have shown that protection following the vaccination is long term, probably for life.
A single vaccine—only against measles—has been administered in 44 African countries and 24 more around the world. The MMR vaccine is common in more than 90 countries, primarily in Europe and North America. From a public health perspective, measles is considered the most important of the three (or four), because of its high contagiousness and fatality rates. In fact, the availability of an effective vaccine affords control over the disease, and even its prevention and eradication, which should be the main goal.
The measles vaccination is one of the first and most effective in the vaccine pool, and is responsible for a dramatic and significant decrease in infant mortality. During the years 1990–2008, 23% of children’s deaths were prevented following measles vaccinations. Without the vaccine, over ten million children would have died worldwide in the last decade because of measles [
7]. This is the most effective means available to prevent measles morbidity. With an average of 99% effectivity, for individuals vaccinated with two doses who nevertheless contract the disease (3%), the disease is expected to be milder [
8].
In Europe, as of 2017, the measles vaccination rate was 90%. In the USA, the rate for 2016 was 96% [
2]. In Israel, a 96% measles vaccination rate was reported for 2018 [
8,
9].
The Measles Vaccination Program in Israel
The National Health Insurance system in Israel legally went into effect in 1995. Public health services are provided by the Ministry of Health, including routine free-of-charge vaccinations during childhood. The measles vaccine is part of the routine vaccinations, and is administered in two doses—at the ages of 12 months and 6 years [
9]. The vaccine is a combination serum that acts against four diseases: Measles, Mumps, Rubella and Varicella (MMRV) or a combined serum against Measles, Mumps and Rubella (MMR), and has been administered in Israel since 1987 [
7,
8,
9].
It is not possible to get vaccinated solely against the measles virus in Israel [
8]. If the routine vaccination is not possible, for example among immunosuppressed individuals or infants younger than one year old, and if there was exposure to the measles virus, an active vaccine can be administered within 72 h, or composed of immunoglobulins can be administered within six days (for people with counter-indications for the active virus) [
10].
1.2. The Health Belief Model (HBM)
The theoretical model upon which this study is based is the Health Belief Model (HBM) [
11], which was developed by Rosenstock in 1974 [
12]. This is a social-psychological health behavior change model developed to explain and predict health-related behaviors, particularly in regard to the individual’s uptake of health services. Previous studies among various groups have shown that this model can explain and predict health-related behaviors [
13,
14,
15,
16,
17]. The basic premise of HBM is that an individual must be in a state of psychological willingness to make a health behavior change, i.e., to take action to prevent a disease. Vaccine decision-making can be explained by the HBM, which conceives vaccination behaviors as an output of an individual’s perceptions of both a disease and its related vaccine [
16,
17]. Studies of compliance with other routine vaccinations investigated the model’s elements in relation to predicting vaccination, and some have been found to affect the decision to receive vaccines. Previous studies have also indicated that by means of understanding the model’s elements, health-related behaviors could be explained, for instance in the field of vaccinations [
13,
14,
16,
17,
18,
19,
20,
21,
22].
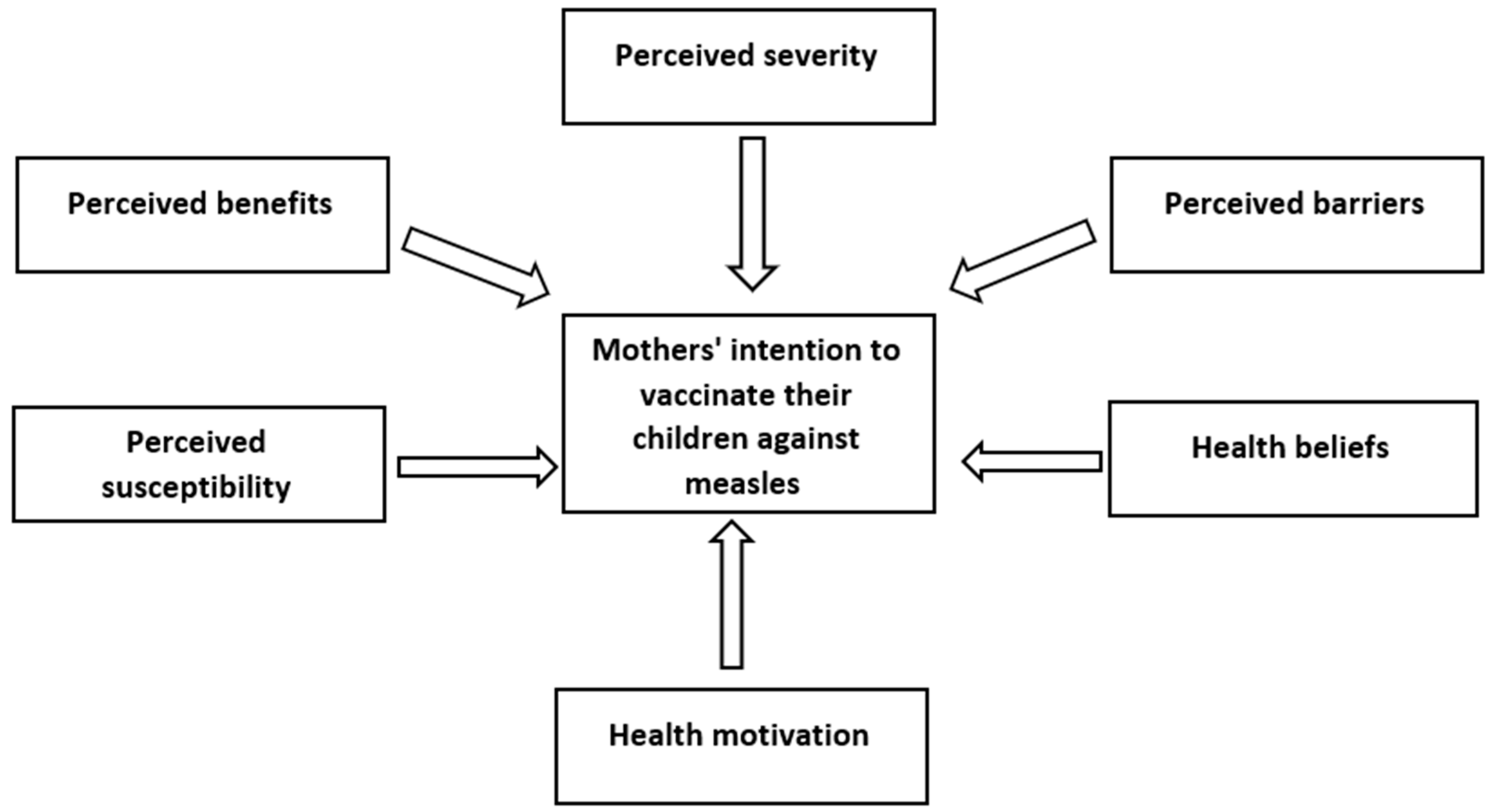
The HBM includes several categories: perceived severity of the medical problem, perceived susceptibility to illness, perceived benefits of health-related behavior, perceived barriers and downsides of health-related behavior, and health motivation.
Perceived severity of the disease relates to the degree of the disease’s gravity and its potential consequences as perceived by the individual. This category reflects the individual’s beliefs about the problems the disease could cause such as pain, discomfort, or financial burden.
Perceived susceptibility refers to the individual’s subjective perception of his/her risk of becoming ill.
Perceived benefits mean the individual’s understanding of the advantages of a recommended health-related behavior to prevent disease or reduce its effects. For example, belief that receiving a vaccine would help to prevent the illness for the individual and keep those around him/her safe.
Perceived barriers of health-related behavior relate to the negative aspects of such behavior, or aspects that serve as barriers to action and/or motivation to avoid action. For example, fear of pain and side effects of being vaccinated.
Health motivation reflects the individual’s motivation to remain healthy; i.e., does s/he maintain a healthy lifestyle, and how his/her lifestyle affects the decision whether or not to receive a vaccine.
We must understand the issue of maternal response to measles vaccinations in depth, and thus develop programs to increase the vaccination rates in the population. Understanding the reasons and motivations that underlie the attitudes of mothers who refuse measles vaccination could facilitate appropriate planning to cope with the problem, and devote the necessary resources to eradicate the phenomenon for the greater good.
The aims of the current study were to examine (1) the factors that influence mothers to vaccinate their children with this routine vaccination, and (2) whether the Health Belief Model can predict maternal response to measles vaccinations.
1.3. Research Hypotheses
Hypothesis 1 (H1). A correlation will be found between mothers’ perceived severity of measles and their intention to vaccinate their children, so that the higher the perceived severity of the disease—the more they will be willing to administer the vaccine.
Hypothesis 2 (H2). A correlation will be found between mothers’ perceived susceptibility of their children to measles and their intention to vaccinate their children, so that the higher the perceived susceptibility—the more they will administer the vaccine.
Hypothesis 3 (H3). A correlation will be found between mothers’ perceived benefits of the measles vaccine and their intention to vaccinate their children, so that the higher the perceived benefits—the more they will be willing to administer the vaccine.
Hypothesis 4 (H4). A correlation will be found between mothers’ perceived barriers of the measles vaccine and their intention to vaccinate their children, so that the higher the perceived barriers—the less they will be willing to administer the vaccine.
Hypothesis 5 (H5). A correlation will be found between mothers’ health motivation and their intention to vaccinate their children, so that the higher the motivation—the more they will be willing to administer the vaccine.
Hypothesis 6 (H6). A correlation will be found between mothers’ average score of health beliefs and their intention to vaccinate their children, so that the more pro-vaccination beliefs they hold—the more they will be willing to administer the vaccine.
3. Results
A total of 181 randomly picked mothers participated in the study. Their age range was 22–60 (M = 35.68; SD = 7.86). Among them, 83.4% (n = 151) of the mothers were married, 13.3% (n = 24) were divorced, 1.1% (n = 2) widows, and 2.2% (n = 4) other. The age range of their children was 1–7 (M = 2.41; SD = 1.17). About 42% (n = 77) of the respondents were born in Israel.
Regarding religiosity, 63% (n = 114) described themselves as secular, 29.3% (n = 53) as traditional, 6.1% (n = 11) as religious, and 1.7% (n = 3) other. Education: 32.6% (n = 59) had high school/tertiary education, 59.7% (n = 108) had an undergraduate degree, and 7.2% (n = 13) had a graduate degree. 95% (n = 172) of the mothers reported being employed at the time they filled out the questionnaire. 32.6% (n = 59) reported a below-average salary, 42% (n = 76) an average salary, and 25.4% (n = 46) an above-average salary.
92.8% of the respondents had vaccinated their children against measles. About 79% (n = 143) had administered both doses of the vaccine.
The means and standard deviations of the research variables are presented in
Table 1.
3.1. Intention to Vaccinate
The mean of the intention to vaccinate variable was very high (5.41 out of 6). Most respondents (74.6%; n = 135) agreed very much that they would vaccinate their children against measles, as opposed to 5% (n = 9) who reported that they had no intention to do so. Additionally, 71.3% (n = 129) of the mothers agreed very much that they would also vaccinate their children in the distant future, as opposed to 5.5% (n = 10) who reported that they had no intention whatsoever to do so. Furthermore, 73.5% (n = 133) agreed very much that they would give their children both doses of the vaccine, whereas 5% (n = 9) reported that they had no intention to do so in the future.
3.2. Perceived Susceptibility
The mean of the respondents’ perception of their children’s risk to catch measles was 2.73 (SD = 1.41). 29.8% (n = 54) completely disagreed with the argument that their children were at low risk to catch measles, as opposed to 8.3% (n = 15) who agreed very much with this argument. Additionallyy, 34.3% (n = 62) completely disagreed with the statement that their children’s health was too good for them to catch measles, versus 3.3% (n = 6) who agreed completely with this statement.
3.3. Perceived Severity
The mean of the perceived severity of measles was very high (5.41; SD = 0.97). Most respondents (79.6%; n = 144) agreed completely that measles was highly contagious and led to complications, as opposed to 1.1% (n = 2) who reported that they completely disagreed with this statement. Additionally, 80.1% (n = 145) of the mothers agreed very much that measles was dangerous, as opposed to 2.8% (n = 5) who reported that they did not agree at all that measles was dangerous. Additionally, 71.8% (n = 130) of the respondents agreed very much with the statement that measles was deadly, versus 2.2% (n = 4) who disagreed completely with this statement.
3.4. Perceived Barriers
The mean of the perceived barriers that affect the mother’s decision to vaccinate her children against measles was relatively low (M = 3.92; SD = 0.25). Most respondents (80.7%; n = 146) disagreed completely with the statement that they would not vaccinate their children because of the risk of autism, as opposed to 4.4% (n = 8) who reported that they completely agreed with this statement. Only 2.2% (n = 4) of the mothers agreed very much with the statement that they would not vaccinate their children against measles because the vaccine caused the disease, as opposed to 85.6% (n = 155) who completely disagreed with this statement. In addition, the majority of mothers (81.8%; n = 148) completely disagreed that the disadvantages of the measles vaccine surpassed its advantages, as opposed to 6.1% (n = 11) who agreed very much with this statement. Additionally, most respondents (89.5%; n = 162) disagreed completely with the statement that they did not intend to vaccinate their children because one child had been oversensitive to the vaccine, as opposed to 0.6% (n = 1) who reported that she completely agreed with this statement. Finally, most respondents (82.3%; n = 149) disagreed completely with the statement that they did not intend to vaccinate their children because the vaccine included dangerous substances such as mercury, whereas 2.2% (n = 4) reported complete agreement with this statement.
3.5. Perceived Benefits
The mean of the perceived benefits of the measles vaccine was very high (5.41; SD = 1.12). The majority of mothers (74%; n = 134) agreed very much that they would vaccinate their children because the measles vaccine saved lives. 71.8% (n = 130) agreed very much that the measles vaccine reduces morbidity in Israel, as opposed to 2.2% (n = 4) who completely disagreed with this statement. Additionally, 71.3% (n = 128) agreed that the measles vaccine reduced their child’s risk of catching the disease.
3.6. Health Motivation
The mean of the respondents’ health motivation was very high (M = 5.19; SD = 1.08). 53.6% (n = 97) of the mothers made sure that their children engaged in sports on a regular basis to stay healthy, as opposed to 1.7% (n = 3) who reported that they did not encourage their children to engage in sports. Additionally, 53.6% (n = 123) reported that they made sure their children got all of the routine vaccines.
3.7. Health Beliefs
In general, the mothers’ health beliefs tended to be positive (M = 4.21; SD = 0.35). Only 5.5% (n = 10) of the mothers agreed that they did not believe in vaccinations. A total of 88.4% (n = 160) disagreed with the statement that they did not believe in Western medicine, whereas 5% (n = 9) reported that they would not vaccinate their children because they did not believe in Western medicine.
3.8. Hypotheses Analysis Results
The first hypothesis, that a positive correlation would be found between mothers’ perceived severity of measles and their intention to vaccinate their children, was corroborated (r = 0.673; p < 0.01). A significant, positive and strong correlation was found between the degree of the mother’s perceived severity of measles and her intention to vaccinate her child.
The second hypothesis assumed that a correlation would be found between mothers’ perceived susceptibility of their children to measles and their intention to vaccinate their children, so that the higher the perceived susceptibility, the more they would administer the vaccine, which was corroborated (r = 0.205; p < 0.01); i.e., the higher their perceived susceptibility, the more they indicated willingness to administer the vaccine.
The third hypothesis, that a correlation would be found between mothers’ perceived benefits of the measles vaccine and their intention to vaccinate their children, was corroborated. A strong positive correlation was found (r = 0.853; p < 0.01); i.e., the higher their perceived benefits, the more they indicated willingness to administer the vaccine.
The fourth hypothesis assumed that a correlation would be found between mothers’ perceived barriers of the measles vaccine and their intention to vaccinate their children. This hypothesis was corroborated (r = 0.393, p < 0.01). A correlation was found, i.e., the lower the perceived barriers, the more they were willing to administer the vaccine.
The fifth hypothesis, that the higher the mother’s health motivation, the more she would be willing to vaccinate her child, was substantiated (r = 0.527, p < 0.01). A significant positive correlation was found, so that the higher the mother’s health motivation was, the more inclined she was to vaccinate her child.
The sixth hypothesis was also corroborated (r = 0.583, p < 0.01). A significant positive correlation was found, indicating that the higher the average score of the mothers’ health beliefs, the more they supported administering the measles vaccine.
Table 2 sums up the correlation between the HBM categories and the intention to accept the measles vaccine.
The research model is depicted in
Figure 1. Multiple linear regression was performed to determine whether the regression model was a good fit. The results were statistically significant (F(679.71) = 5.001 sig < 0.01). The entire model was able to predict 1% of the variance of the intention to accept the vaccine. The variable ‘perceived benefits’ was significant (B = 0.831, sig < 0.01).
4. Discussion
The present study examined whether the Health Beliefs Model (HBM) could predict parents’ acquiescence to measles vaccines for their children, and to which degree. The study’s main research question was largely validated. It was found that the HBM variables predicted mothers’ consent to vaccinate their children against measles, thus supporting previous findings [
23], which indicated a correlation between parents’ various perceptions about vaccination and the decision to vaccinate their children. The difference between parents who vaccinate their children routinely, parents who are uncertain, and parents who outright refuse vaccinations can be interpreted by their different perceptions of susceptibility, benefits, and risks and barriers. Bond [
23] also found that parents who routinely vaccinate their children fear the outbreak of diseases, and parents who postpone or refuse vaccinations are primarily concerned about the safety of the vaccine and long-term side-effects.
This finding in the present study contradicts the findings of other studies [
24,
25,
26,
27], which emphasized that the HBM variables overly depended on psychological factors rather than focusing on cultural values, myths, misconceptions and prejudices, which typically predict human behavior [
28].
This study found that mothers’ disease severity perceptions, namely that measles was an infectious, contagious disease that could be deadly, were found to correspond with their willingness to vaccinate their children. Similar findings were reported by Sun and colleagues [
29]. The severity of the disease—particularly possible long-term damage—was the most powerful factor that affected parents’ vaccine decision-making. When parents perceived the disease as light, they seemed to prefer ‘natural immunization’. This is in contradiction to a meta-analysis [
30], which found a weak link between perceived severity and intention to vaccinate. It is possible that in Israel, where there had been a measles outbreak not long before this research was conducted, and which had been heavily reported by the media, parents’ decision-making tended to be affected. During 2018–2019, 4000 new cases of measles (mainly among children younger than 9 years old) and three deaths were reported. Whereas the very high vaccination coverage in other countries could have reduced the perceived severity of the disease, in Israel the outcome of the recent outbreak seems to have exacerbated it.
We found that the higher the mothers’ perceived susceptibility of their children to measles, the more they would administer the vaccine. The literature on this issue also revealed a strong positive correlation. For example, Smith and colleagues [
30] found that about 70% of the parents who delayed or refused to vaccinate their children believed that their children might catch measles if not vaccinated, as opposed to 90% of parents who routinely vaccinated their children. Furthermore, Hayden [
31] argued that it is reasonable that when people believe they are at risk, they do more to prevent it. Our findings reveal that although mothers perceived measles as a severe disease, if they did not believe their children were at risk to catch it, they would not vaccinate them.
It was also found that the higher the mothers’ perceived benefits, the more they indicated willingness to administer the measles vaccine. In this study, the perceived benefits variable is ranked second in its positive effect on the decision-making process. This supports Smith and colleagues’ [
30] findings, which showed that parents who delayed or refused the vaccine perceived less benefits and more detriments of the vaccine than parents who routinely vaccinated their children.
The next hypothesis related to perceived barriers to the measles vaccine. Mann [
32] described the barriers that affected the decision to administer the measles vaccine; the most powerful one being fear of autism. In this study, mothers were asked about their perception of a link between the vaccine and autism. 80% of the respondents stated that their refusal to vaccinate their children was related to fear of autism, but 20% disagreed that this was the reason. It seems that the lower the mother’s perceived barriers, the more they are willing to vaccinate their children against measles. This finding is related to the perception of the vaccine’s safety. The periodic national vaccine research in the US [
33] asked parents about their perception of the safety of the measles vaccine, and 93% stated that they thought the vaccine was completely safe. Meanwhile, 3.1% stated that the vaccine was completely unsafe. Multivariate regression analysis found that the likelihood a child would be vaccinated fully by the age of two was 9.2 times higher if the parents believed that the vaccines were safe, as opposed to parents who believed they were unsafe. Indeed, among parents who thought the vaccines were unsafe, full vaccination coverage by the age of two was 47%, in comparison to 90% among parents who perceived the vaccines as safe.
A CDC report [
1] on the measles vaccine concluded that the presence of Thimerosal in vaccines did not cause autism; autism rates continued to rise even after Thimerosal was removed from almost all childhood vaccinations. Parents are scared because the first signs of autism are often detected around age two, which is shortly after the first MMR vaccine.
Hayden [
31] maintained that perceived barriers were the most significant factor that affected one’s intention to vaccinate. Although it is natural for parents to have some concerns about the safety of the vaccine, it seems that in Israel this element is a significant factor in the decision to vaccinate, albeit not the most powerful one. A possible explanation is that at the time of the 2018 outbreak of measles, there was an increase in anti-vaccinationist voices, which used the media massively to advocate avoidance of the vaccine because of its link to autism. Among young parents, it was found that their exposure to the media and various health forums on social media, and their constant search for online information, reduces the intention to vaccinate. They are more hesitant, because they are more aware of the downside of vaccination alongside its benefits [
34]. A single study conducted in Israel [
35] among new mothers in maternity hospitals found that the rate of mothers who refused to have their infant vaccinated against hepatitis B, which is administered in the hospital, was less than 1%. The study found that the majority of mothers had made an informed decision following in-depth investigation before they gave birth. Most mothers who refused the vaccine also declared that they would continue to refuse to vaccinate their child with the other recommended routine vaccines.
The fifth hypothesis examined the correlation between the mothers’ health motivation and intention to vaccinate. The higher the mother’s health motivation was, the more she intended to vaccinate her children, which is also important to herd immunity. When highly health-motivated mothers, who take care of their own and their children’s health, search for reliable information and understand the significance and advantages of the vaccine, they vaccinate their children. Furthermore, and no less important, they disseminate the information to other mothers, emphasize the importance of vaccination, and encourage them to do the same [
36].
Finally, this study found that the higher the average score of the mothers’ health beliefs was, the more they supported administering the measles vaccine. The literature has shown that parental vaccine-hesitancy based on personal beliefs includes parents who rely on herd immunization, arguing that they chose not to vaccinate because their children are safe anyway [
37]. The hypothesis is that a negative attitude to vaccination is rooted in non-scientific evidence, and could lead people to adopt unconventional or alternative medicine. Others mistrust vaccination because it supposedly contradicts god’s will [
38]. Jewish rabbinical law (halacha) includes prohibitions regarding the ingestion of non-kosher items, and the measles vaccine contains animal products [
39,
40]. This combination leads to lower vaccination rates and more measles outbreaks among orthodox Jewish communities compared to the general population. Indeed, during the recent measles outbreak in Israel, over 50% of the patients were from ultra-orthodox communities in Jerusalem.
In summary, the present study has shown that the HBM can be used to explain what motivates mothers to vaccinate their children with the MMR vaccine. The perceived severity of the disease has the biggest impact on the decision-making process, alongside the perceived benefits and perceived barriers.
The herd immunity threshold is somewhat fragile, because the majority of the population (96–99%) must be vaccinated in order to provide maximal protection [
41]. When the threshold drops even slightly, the population is vulnerable.
Possibly, reassurance by the medical staff and promotion by the health system, providing a rational explanation of the vaccine’s importance, would increase parents’ intention to vaccinate and raise the rate of vaccinated population. Some parents may, in fact, feel strongly about denying vaccination, but it is likely that many of them are simply in need for reassurance and guidance about making this decision for their children. This is where public health advocates and health care professionals can make the biggest impact.
In Israel, the most significant predictors among the HBM variables are perceived severity of the disease and perceived benefits of the vaccine. Since young parents are highly influenced by social media and their peer group, social media could be the next step for public health education regarding vaccine recommendations and safety. Instead of using a top-down approach, where providers present information to parents and patients, it has been suggested that advocates of vaccines use a side-to-side approach where parents can advocate to their peers [
42]. Social media presents a channel through which information is easily passed; however, it could either prove helpful for health advocates, or detrimental, which is also possible if the wrong ideas are shared.





{kind=link}