1. Introduction
Special pathogens are classified as highly infectious and easily transmissible microorganisms capable of causing life-threatening illnesses in humans and posing a major threat to the general public and in the healthcare setting [
1]. They are associated with high morbidity and/or mortality, have a high likelihood of secondary cases (person-to-person spread), may lack an effective vaccine, prophylaxis, or treatment, and might prompt the use of a biocontainment unit due to clinical or public health concerns [
2]. Examples of special pathogens include viral hemorrhagic fevers, such as Ebola and Lassa Fever, as well as severe respiratory special pathogens, such as Middle East respiratory syndrome and severe acute respiratory syndrome.
The World Health Organization (WHO) has reported that infectious diseases are growing faster than ever before, which is unsurprising given how technological investments have made travel nearly universally accessible among other contributing factors [
3]. There have been numerous outbreaks of special pathogens around the world requiring prompt healthcare response for identification, isolation, and treatment [
4]. This includes at least five outbreaks of Ebola virus disease since 2014 in West Africa, ongoing and sporadic cases of Middle East respiratory syndrome (MERS) reported in 12 countries in the Eastern Mediterranean Region since April 2012, and ongoing and sporadic cases of Crimean-Congo Hemorrhagic fever (CCHF) in countries within Asia, Africa, and Europe [
5,
6].
While many of these special pathogen outbreaks disproportionately affect lower-resource countries with inadequate public health systems, high-income countries are also not spared. There is often a paradox of low patient count but high resource demand. This was seen in the 2014 Ebola outbreak. In March of 2014, the WHO reported Ebola cases in rural Guinea. The next 2 years represented the largest Ebola epidemic in history, including numerous cases in Liberia, Sierra Leone, Mali, Nigeria, Senegal, Spain, the United Kingdom, and the United States. During the outbreak, many public health experts and academics expressed concerns about the United States’ ability to properly manage patients with suspected and confirmed Ebola or other special pathogens [
7]. These concerns became a reality in September 2014 when a Liberian national visiting the United States was admitted to Texas Heath Presbyterian Hospital in Dallas, Texas, where he was diagnosed with Ebola virus disease (EVD) shortly after. During his time as a patient, two nurses were exposed to the virus and both were diagnosed with EVD in October 2014. Within the same month, a healthcare worker who was working overseas in West Africa for Ebola response returned to the United States and was diagnosed with EVD in New York and treated in NYC H+H’s Bellevue Hospital. In April of 2015, the CDC contacted 55 Ebola treatment centers (ETCs) in the US and determined that only three had adequate preexisting biocontainment units and the other 52 needed to undertake extensive changes, including “development of plans, recruitment of facility leadership, recruitment and training of a multidisciplinary team of volunteers, and purchase of specialized supplies and equipment” [
8]. These developments cost the ETCs nearly 54 million USD.
Following the outbreak, numerous evaluations of public health policies and hospital preparedness highlighted the need for increased training and education among healthcare workers. A 2014–2015 national survey of internists concluded that practitioners had widely different understandings of the risk of Ebola and required better risk communication [
9]. Lack of preparedness education was not limited to the United States. Incorrect information about the risks and treatment of Ebola spread within West Africa at the beginning of the outbreak, making effective containment of the disease more difficult [
10]. Internationally, many hospitals were unable to quickly implement procedures for diagnosing and caring for Ebola patients, putting healthcare workers also at risk [
11,
12]. The outbreak also highlighted the importance of training other members of hospital staff in special pathogen preparedness, as waste removal and patient transportation put numerous employees at risk [
13,
14].
All told, the 2014–2016 Ebola outbreak exposed the numerous cracks that exist in the United States preparedness toward special pathogens. As we know all too well, “special pathogens pose a significant risk to healthcare personnel and require specific healthcare facility processes to ensure early identification and isolation of infected patients and the use of effective infection control practices to prevent disease transmission while the patient is further evaluated” [
2].
NYC H+H is the largest public healthcare system in the United States, with one of its acute care facilities, NYC Health + Hospitals/Bellevue, designated as one of 10 regional treatment centers in the country capable of treating Ebola patients and the remaining 10 acute facilities as frontline hospitals tasked with identification, isolation, and transferring suspected patients with Ebola or other special pathogens to the treatment center [
15]. With 24 large facilities, NYC H+H is an important first line of defense for any outbreak in the city and, as such, the development of the Region 2 Frontline Facility Special Pathogens Course was started.
As a hub for both national and international travel, New York City plays a vital role in protecting the United States against transmission of special pathogens [
16]. However, from a sample of 73 administrators, physicians, and nurses in Region 2 which includes NY, NJ, PR, and VI, 85.4% rated their facility as somewhat prepared or unprepared to combat an outbreak of a special pathogen in 2018 [
17]. This highlights the need to provide ongoing training and education for special pathogen events including appropriate processes and procedures within healthcare systems.
Primary healthcare providers in HHS Region 2 expressed concern with the seemingly too narrowed focus on identification. When it comes to the goal in special pathogen preparation to “Identify, Isolate, Inform”, one physician commented, “We’re good at identifying, but if we are strong in just one area, we will fail.” Staff rarely work in the level of PPE that would be required for special pathogens. An outbreak would also place staff in an environment of much higher stress and less preparation than they are accustomed. Training in these unusual conditions is necessary to prepare for the real-life conditions of a special pathogen case [
18]. The Frontline Facility Special Pathogens Training Course, created by the hospital systems’ Systemwide Special Pathogens Program, was an 8 h course offered throughout 2018–2019 to healthcare workers throughout the NYC H + H healthcare delivery system and Health and Human Services Region 2. The course mixed presentations, simulations, and discussions in an attempt to better prepare healthcare employees for an unexpected special pathogen case. The goal was to equip administrators and healthcare providers with centralized skills in order to effectively identify, isolate, preliminary manage, and inform appropriate stakeholders in the event of a special pathogen case and transfer of the patient to a treatment facility.
2. Materials and Methods
The 8 h course, offered in NYC between 2018 and 2019 as 20 courses, included three modules and culminated in group analysis of the participants’ performance and discussion of special considerations, such as pediatric, geriatric, and behavioral health. It did so through presenting decision support tools and resources, discussing best practices and basic infection control strategies, and providing immersive live scenarios. The course covered the practice of donning/doffing PPE and other clinical stations, including Middle East respiratory syndrome (MERS-CoV) workup on a mid-fidelity mannequin, immediate spill remediation of a bodily fluid spill, removal of contaminated PPE, and how to properly transfer and transport patients while wearing the high-level PPE attire. Module 1 covered “Identify, Isolate, Inform”, module 2 covered working in Level 1 PPE, and module 3 covered working in Level 2 PPE.
The course was open to all healthcare professionals but targeted frontline healthcare workers. Participants of this course included healthcare workers such as physicians, nurses, infection preventionists, and physician assistants who would be directly involved with the identification, assessment, or preliminary treatment of patients with suspected special pathogen disease (e.g., Ebola, MERS). Other allied healthcare professionals also participated in the course including patient care technicians, emergency management coordinators, hospital police, administration staff, triage staff, respiratory therapists, social workers, and others. According to a post-course follow up survey of participants who took the training, (
Table A1,
Appendix A), the majority of the respondents worked in a hospital, while the others either worked in healthcare management, such as a government agency, or in a non-hospital healthcare facility, such as a nursing home. Their employment included healthcare practitioners (46%), public servants (21%), and other nontraditional healthcare vocations, including educators (9%), sanitation workers (4%), and hospital administrators (20%). The instructors of the course included an infectious disease epidemiologist, infection preventionist, emergency management coordinator, and emergency medical services commanding officer.
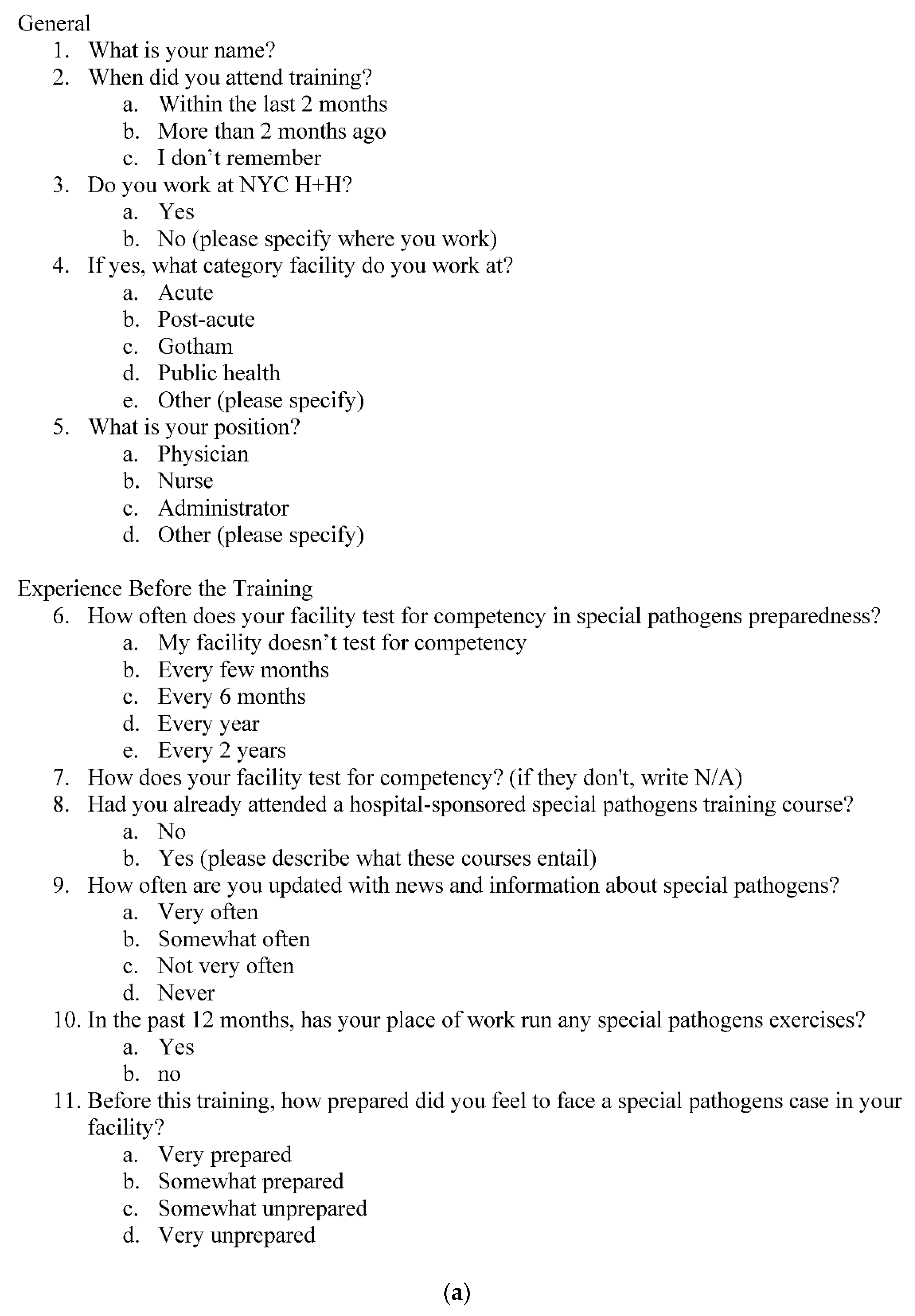
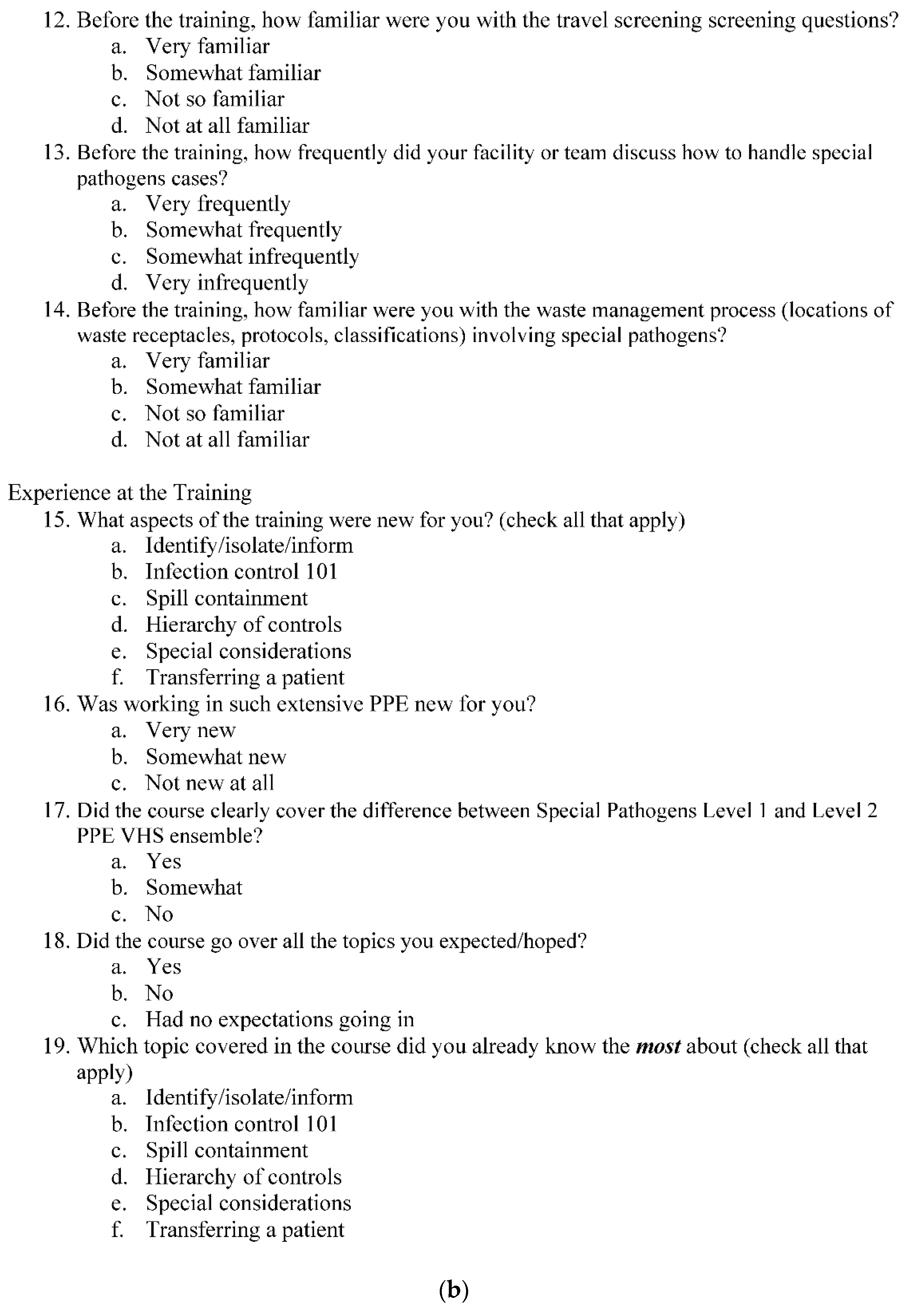
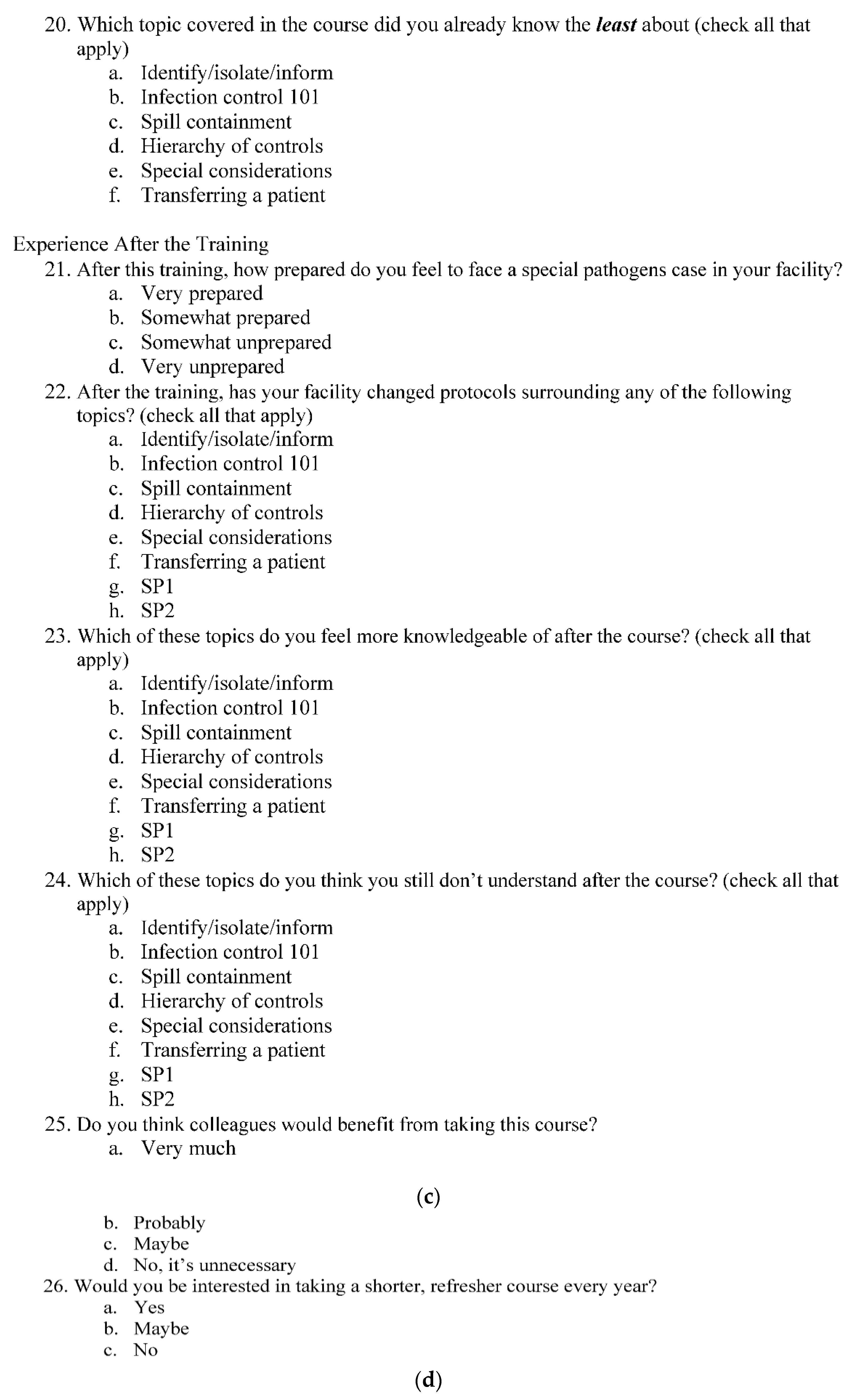
The success and impact of the course were evaluated by a subsequent cohort analysis, involving pre- and post-course examinations the day of the training, a course evaluation survey, post-course interviews of select course participants (
Figure A1a–d,
Appendix A), and a post-course survey. The post-course survey, distributed electronically no less than 2 weeks after completion of the course, evaluated participants’ prior preparation for and awareness of special pathogen cases, the course’s ability to meet expectations, and how the course changed their knowledge and or practices. Questions were written primarily in a multiple-choice format, with optional write-ins. The selected questions focused on the participants’ experience with special pathogen preparedness before the training, asking about both subjective feelings of preparedness and accounts of previous trainings at the hospital.
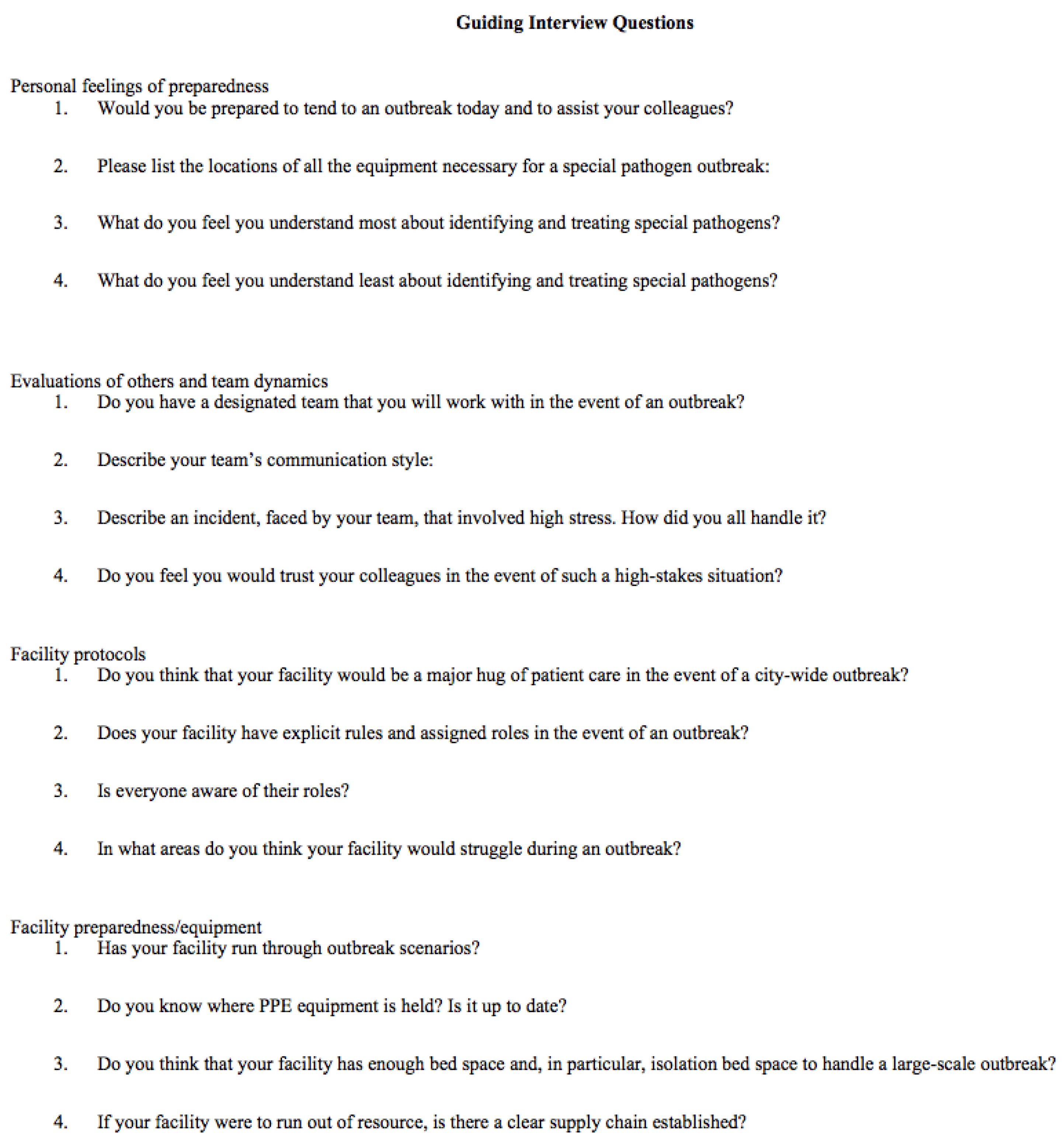
In addition to a written, survey-based approach, in-depth interviews were conducted with 10 participants 1–2 weeks after completion of the survey, centered around the following topics: personal feelings of preparedness, evaluations of others and team dynamics, facility protocols, and facility preparedness/equipment (
Figure A2,
Appendix A).
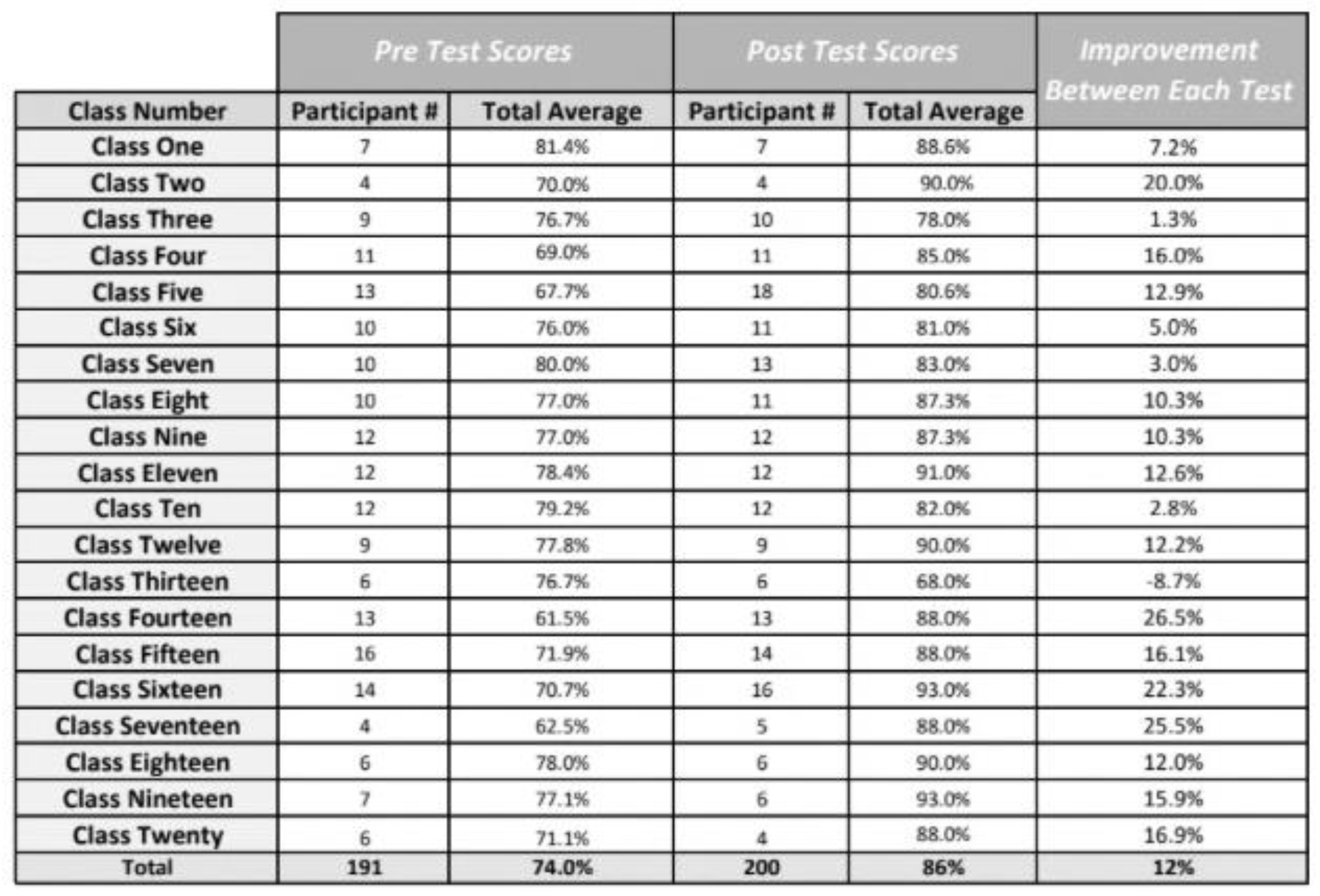
Lastly, multiple-choice quizzes covering knowledge of special pathogen preparedness were given on the day of training immediately before and after the course. They were completed by 200 participants, scored out of 20 questions, and evaluated for quantitative improvement in knowledge. The questions were based on the following core competencies covered in the course:
Healthcare worker safety when caring for a highly infectious disease patient,
PPE donning and doffing technique,
Rapid identification and isolation of high-risk patient through triage,
Importance of early recognition and isolation,
Safe patient care and management simulations,
Enhanced infection control precautions,
Drawing of routine (basic) labs on a suspected high-risk patient,
Bodily fluid clean up and containment simulation,
Special consideration for behavioral support,
Special consideration for pediatric patient,
Special consideration for geriatric patient,
Appropriate internal and external contacts,
Patient transport and transfer technique.
The end result of these surveys and interviews was a mixed-methods report, combining quantitative analysis of the participants’ changes in knowledge and their reported (survey-based) preparedness levels, as well as a qualitative discussion based on interviews.
4. Discussion
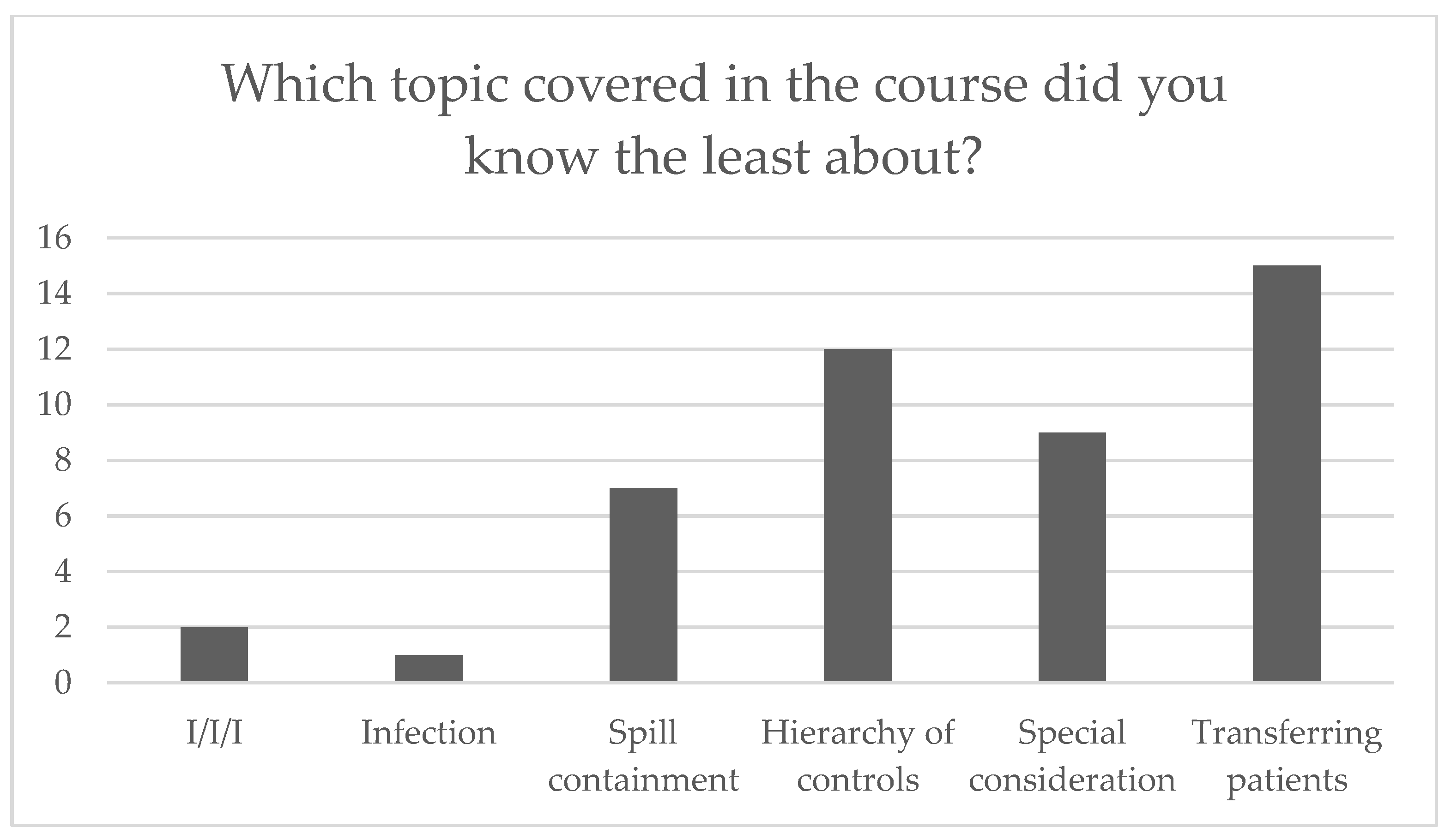
Survey participants reported not only general satisfaction with the course, but also an increased level of preparation for a special pathogen case. Specifically, greatest improvements in preparation were made in the areas of special considerations and special pathogen-specific PPE. Interview responses elaborated on the course’s ability to increase participants’ confidence and the course’s ability to affect change in facility protocol. Together, these results suggest that this interactive, mixed-method training increased special pathogen preparedness across different healthcare sectors.
The demographic data collected from the survey indicate that many of those that self-selected the course were hospital workers, but not necessarily nurses and physicians. Follow-up interviews with administrators and managers revealed that many of these professionals felt excluded from normal hospital preparedness trainings and were worried about their role in the event of a special pathogens outbreak. Environmental service employees found it especially important to take this course as they would also be expected to work in the relevant PPE and patient care environment.
Questions about prior preparedness interventions indicated that both hospital workers and the hospital administrators were already taking active steps to be prepared. Most facilities were testing regularly for competency and the employees themselves self-reported staying up to date with relevant news and information; however, most reported never previously attending a hospital-sponsored special pathogens training course, indicating that facilities may be testing for preparedness without offering the necessary education beforehand.
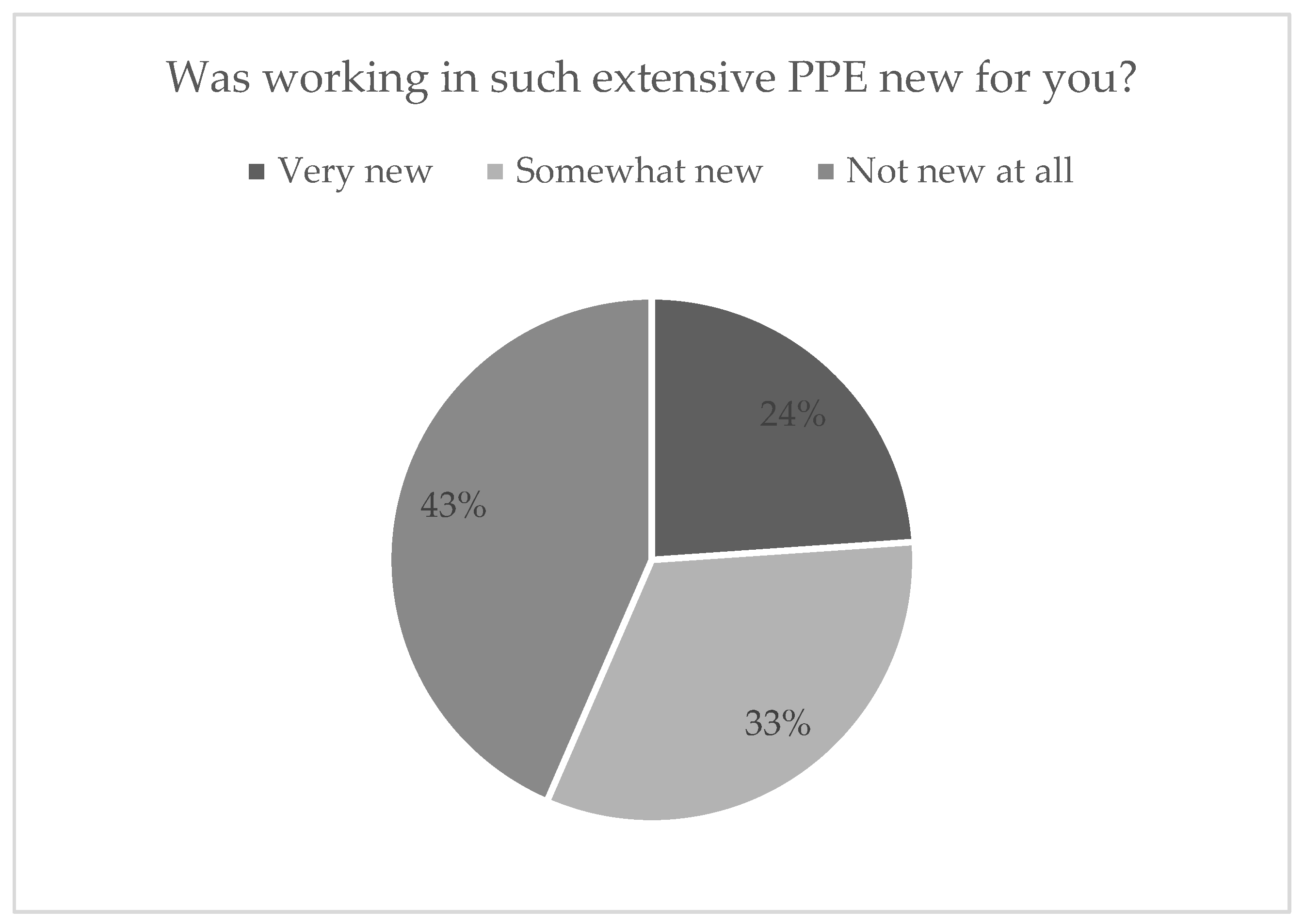
Respondent reports of inexperience working in PPE and patient transfer reinforced the need for this course, as the second and third module focused heavily on moving the patient and performing procedures in the restrictive special pathogen PPE.
4.1. Effectiveness of the Training Course
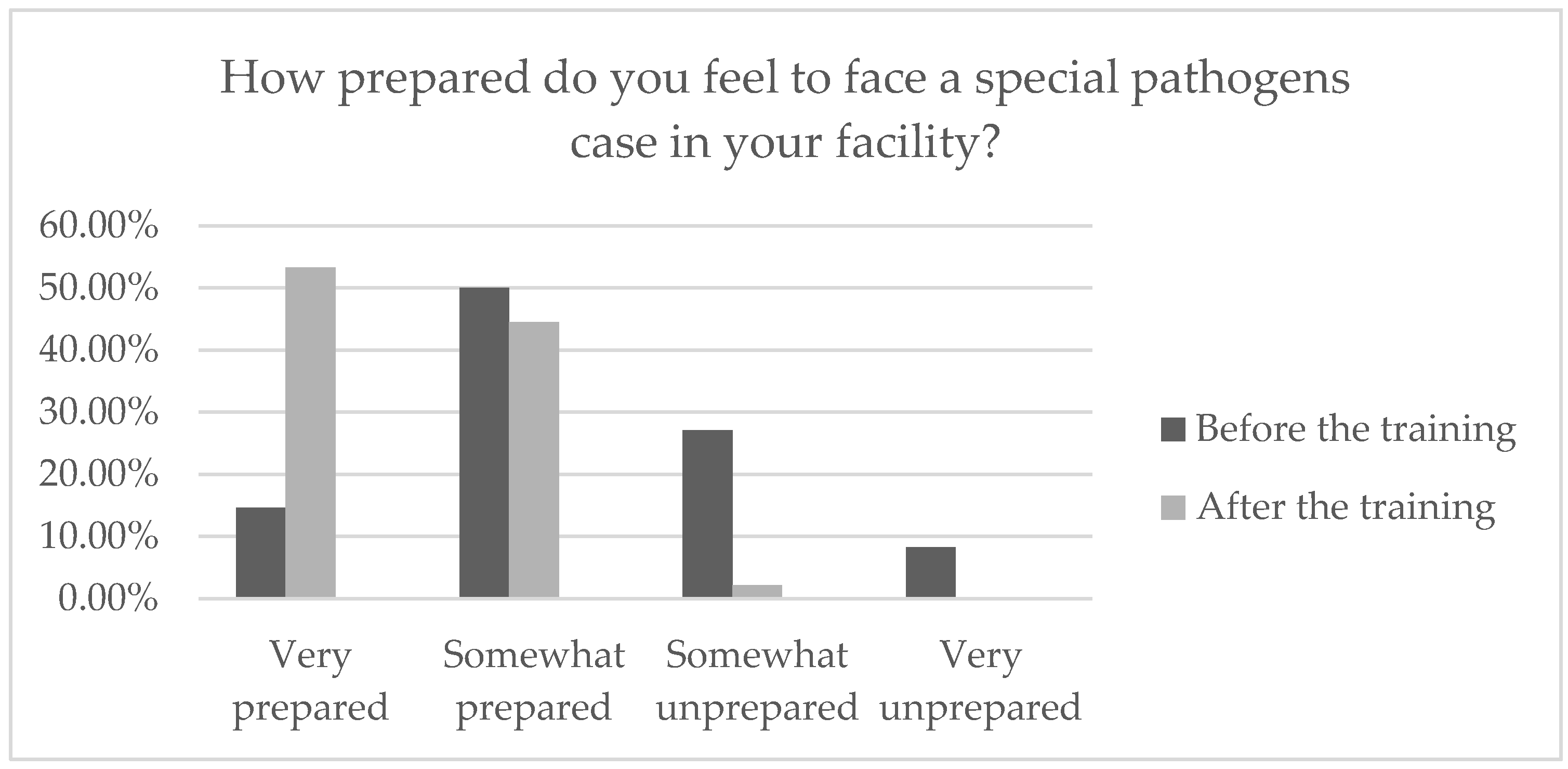
Self-assessments of preparedness before and after the training suggested a dramatic shift from the majority of participants feeling somewhat prepared and somewhat unprepared before the training to almost the entirety of the respondents indicating feelings of preparedness, with the majority feeling “very prepared”. Although this result was self-reported, we find it to be incredibly promising because it indicates that the workers left the training feeling more confident in their abilities, which would help them work better as a team member in the case of a special pathogens emergency. Only one participant noted a feeling of “somewhat unprepared” after the course; however, reported feeling “very unprepared” before the course; hence, this finding still shows improvement.
Results from the pre and post examinations also indicate that there was objective improvement in knowledge surrounding special pathogen preparedness. It is important to note, however, that the rates varied greatly between each class and that definitive conclusions cannot be made about any improvement in knowledge until more data are gathered.
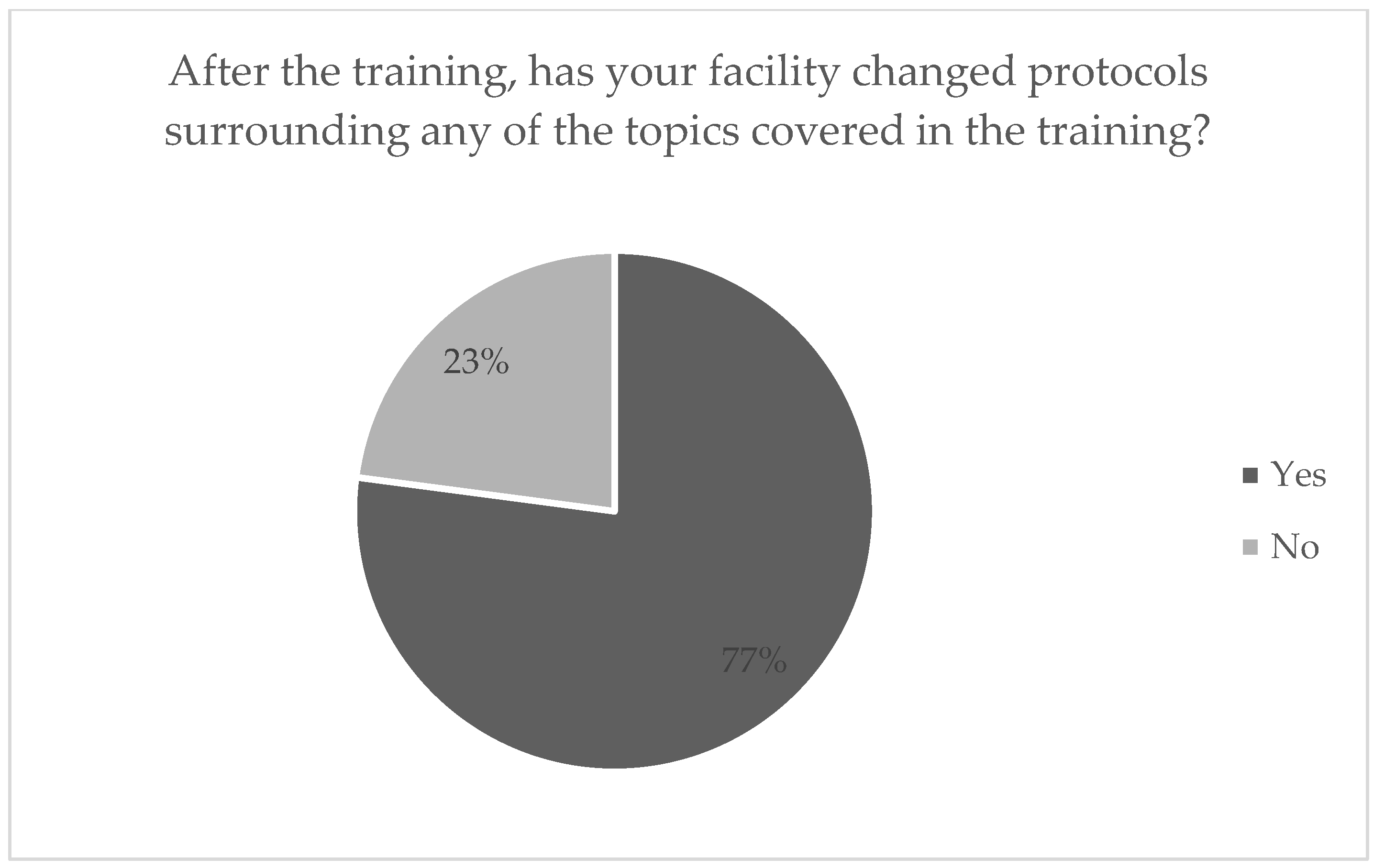
Some of the most unexpected but most promising results from this survey were the questions involving changes in facility protocol. The majority of respondents indicated that their facility changed their special pathogen protocol, most often those involving special consideration and special pathogen-specific PPE after they had taken this training. This suggests that there may be a ripple effect due to increased training, i.e., the idea that those who are trained will train others and inspire change in their facilities.
Follow-up interviews with physicians and administrators from multiple hospitals were conducted to more deeply evaluate how hospitals instated changes in protocol after their employees attended the class. Most hospital staff reported that the largest protocol change was in PPE training and equipment availability. Although all interviews reported having prior training with PPE, all reported that these preparations consisted of online training courses and demonstrations; one described the state of PPE protocol as “woefully underdeveloped”. Reported changes after the Frontline course included more accessibility to the equipment detailed in the training course and instituting active donning and doffing training drills, rather than relying on online modules.
4.2. Satisfaction with the Training Course
The majority of 200 respondents indicated that the course was what they expected, that it would benefit their colleagues, and that they would be interested in taking a yearly refresher course. This finding is significant given the need to maintain a state of readiness on an ongoing basis. Preparedness is not a state; rather, it is an active process that requires continuous training and education in the form of refreshers.
Follow-up interviews reported no dissatisfaction with the course. When prompted for recommendations for alternations, only one interviewee spoke up, noting the importance of including a degree of “applicable honesty”, a discussion of what is realistic for clinicians, and making sure not to undermine the existing knowledge and experience they already have about the subject.
4.3. Limitations
One limitation of the paper was the inability to evaluate actual preparedness without the occurrence of an actual special pathogen case. Simulating a special pathogen case or outbreak is difficult. We hope that incorporating a wide variety of questions surrounding factual knowledge, situational decision-making, simulation, and subjective experience of preparedness can help to qualify the complex subject of preparedness. The Frontline course itself is one of the best indicators for preparedness, as it most realistically mimics a high-risk case; therefore, the Special Pathogens team hopes to initiate an additional yearly refresher course to test competency.
Self-selection bias was a concern as it is possible that those who chose to attend the course were those who believed they were not prepared. Although this factor is important to consider, it should not affect the question to be addressed, i.e., that this course promoted a positive change in preparedness. Starting at a lower level of preparedness would not have altered our ability to study change.
All 200 course participants completed the pre and post assessments. The interviews and follow-up survey were completed by a smaller number but offered to all. Given the busy schedules of healthcare workers and competing priorities, not all participants were able to devote additional time for post-training evaluation.
5. Conclusions and Future Directions
As infectious diseases continue to proliferate with many factors responsible for the rise and spread of diseases including human ecological and environmental changes, agricultural development, travel and commerce, human demographic changes and behavior, microbial adaptation, and breakdown and poor public health infrastructure, it is increasingly important for all healthcare workers to prepare for the nearly inevitable next outbreak. The Frontline Facility Special Pathogens Training Course creates a hands-on way for hospital staff to engage with the pressing reality of a special pathogens case or potential outbreak. The need to offer ongoing training and education to staff including having established protocols and processes is essential for preparedness and eventual response.
As a preventative measure, these trainings may be limited in their effectiveness due to technical, social, and financial constraints. The implementation of such a program within hospitals will rely on available funds, the willingness of administration to make the training mandatory, and the eagerness of employees to participate if voluntary. Funds will be necessary to both provide the training and allocate a day off for employees to participate. This may not be possible for all hospitals and highlights another larger issue in changing the way healthcare and public health infectious disease prevention and readiness is funded at the local, state, and national level.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




