1. Introduction
Cardiovascular diseases are estimated to be the most common cause of death and of disability-adjusted life years (DALYs) worldwide, where ischemic heart disease, stroke, and hypertension are the major diseases within this group [
1,
2]. Likewise, in Germany, where this study was conducted, ischemic heart disease is the leading cause of death and loss of healthy years of life [
3]. According to the estimates of the Global Burden of Disease (GBD) study 2010, hypertension has—after unhealthy nutrition—the second highest impact on the disease burden in Germany [
3].
Lower respiratory diseases as a group show a retrogressive trend in DALYs but are still the second leading cause for disability worldwide [
2]. In Germany, the burden of lower and chronic respiratory diseases is the seventh most important cause of DALYs [
3]. Among children, bronchitis is one of the most common acute diseases diagnosed, and asthma the most common chronic disease diagnosed [
4,
5,
6].
Environmental noise, especially road traffic and aircraft noise in urban settings is considered to be relevant risk factors for adverse health effects, and several biological and epidemiological studies have shown the link between noise and different cardiovascular health outcomes [
7,
8,
9,
10,
11]. Results from the KORA study (Cooperative health research in the Region of Augsburg) for instance showed a higher prevalence for hypertension with an increase in noise (odds ratio (OR) for a 10-dB(A) increase = 1.16 (95% CI: 1.00; 1.35) [
7].
However, studies investigating and showing the relationship between noise, noise annoyance, and respiratory diseases such as asthma in children are rare, and their underlying mechanisms need to be further identified [
12,
13,
14,
15].
Additionally, it is suggested that health access as well as social services might influence specific health outcomes and that social and health services are more available in urban than they are in rural areas [
16,
17,
18]. In a study conducted in three French regions, significant differences were found among geographic areas with greater access to primary care in Paris, along with income disparities in health access [
17]. Moreover, individual sociodemographic and socioeconomic factors such as gender, age, educational and occupational background or income are suggested to be important risk factors for cardiovascular and respiratory diseases [
7,
19,
20]. However, the use of single and highly correlated indicators for the economic and demographic situation reduces the available information and may imperfectly set the focus point on selected parameters.
Other studies focused on borough or metropolitan socioeconomic status, and showed associations between deprived areas and cardiovascular or respiratory health outcomes, such as hypertension or asthma [
21,
22,
23]. Researchers from the Heinz Nixdorf Recall (HNR) Study used unemployment rates as area-level markers of socioeconomic status. Results showed that smoking, obesity, and low physical activity, used as response variables for cardiovascular risk factors were more common in deprived boroughs in Germany, even after adjusting for personal characteristics such as age, sex, or individual education [
21].
Recently, a conceptual model emphasizing the importance of individual, societal, and environmental factors and their interactions, which are potentially associated with urban health was published by the authors [
24].
The objective of this paper, being part of this interdisciplinary collaboration, was to investigate in a first step association between road traffic noise, physician density, socioeconomic and demographic risk factors, classified by a number of indicators as a Principal Component Analysis (PCA)-based score, and cardiovascular and respiratory disease on borough level in the city of Hamburg. Specifically, we used statistical modeling to assess the associations between road traffic noise > 65 decibel A (dB(A)), social deprivation, and physician density used as a surrogate parameter for health access on the age-adjusted prevalence rates of heart failure and hypertension. Additionally, the effect of potential associations between road traffic noise > 65 dB(A), social deprivation, and physician density on the prevalence rates of acute bronchitis and asthma in children aged 14 or younger was analyzed.
2. Materials and Methods
2.1. Study Area
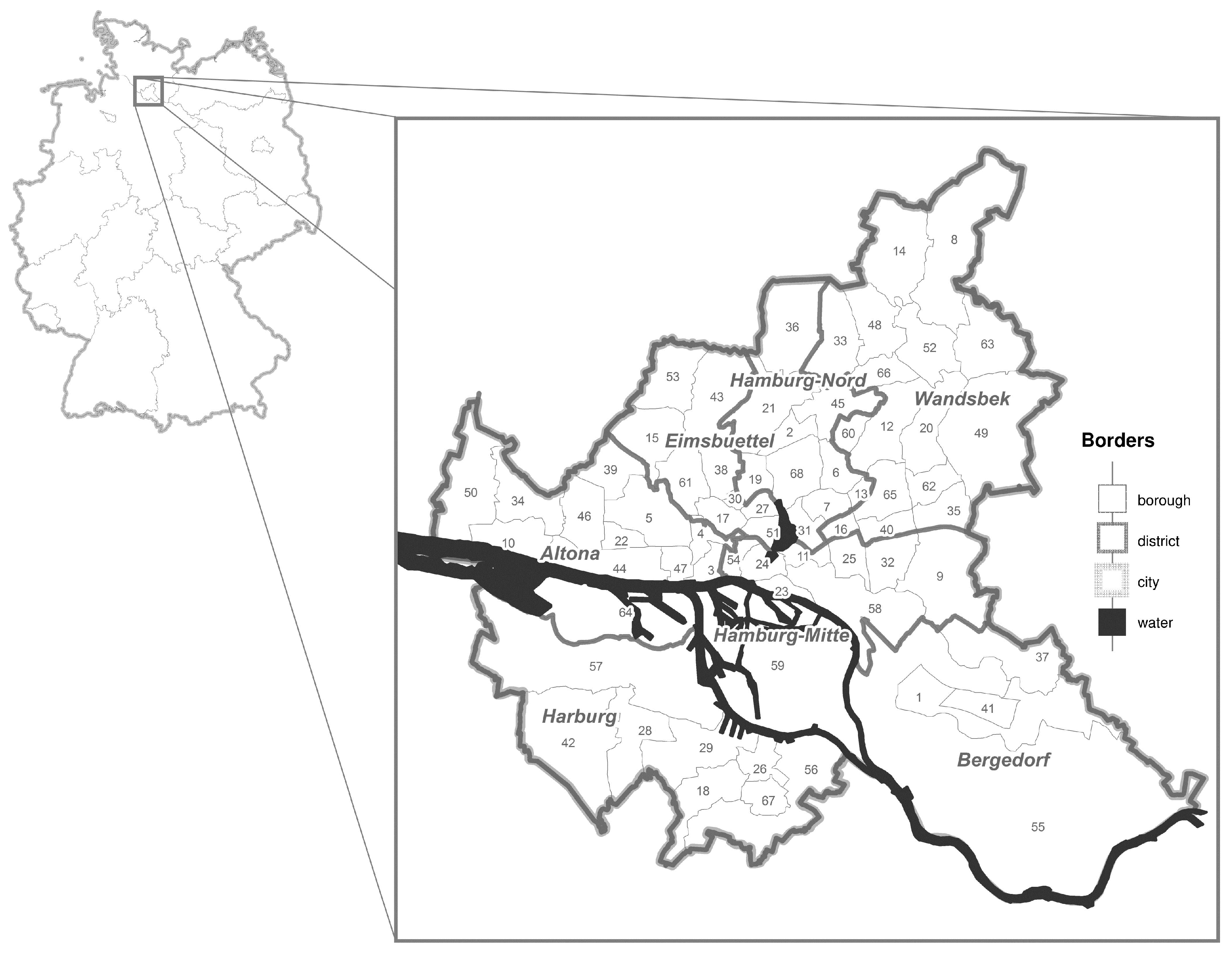
This study was conducted in the city state of Hamburg, in northern Germany. Hamburg consists of 104 boroughs and seven districts, and is the second biggest city in Germany with approximately 1.8 Million inhabitants [
25].
The socioeconomic background shows a heterogeneous pattern and varies greatly among the boroughs, where boroughs with a better social structure and hence, for instance more income and lower unemployment rate can mostly be found in the district of Altona, or in the outer parts of Wandsbek. Contrarily, boroughs with a poorer social structure and hence, for instance lower income and higher unemployment rate are mostly located in the district of Hamburg-Mitte [
25]. Due to a low prevalence of disease in some of the 104 boroughs in Hamburg and hence, low power, some of the adjacent boroughs with comparable socioeconomic and sociodemographic factors were aggregated to a total of 67, and used for all analyses (see
Figure 1 below and
Table A1 in the
Appendix A). No data were available for the borough “Hafencity” [
26].
2.2. Prevalence Rates of Cardiovascular and Respiratory Diseases
All of the disease prevalence rates (year 2011) were obtained from the Ministry for Health and Consumer Protection of the Free and Hanseatic City of Hamburg, and refer to the territory of the city state of Hamburg. Prevalence rates were computed by considering the care claims data from the public health care system of all statutory health insured patients, with at least one contact to a contract physician working in the ambulatory sector, as the population (
N = 442.336) [
26].
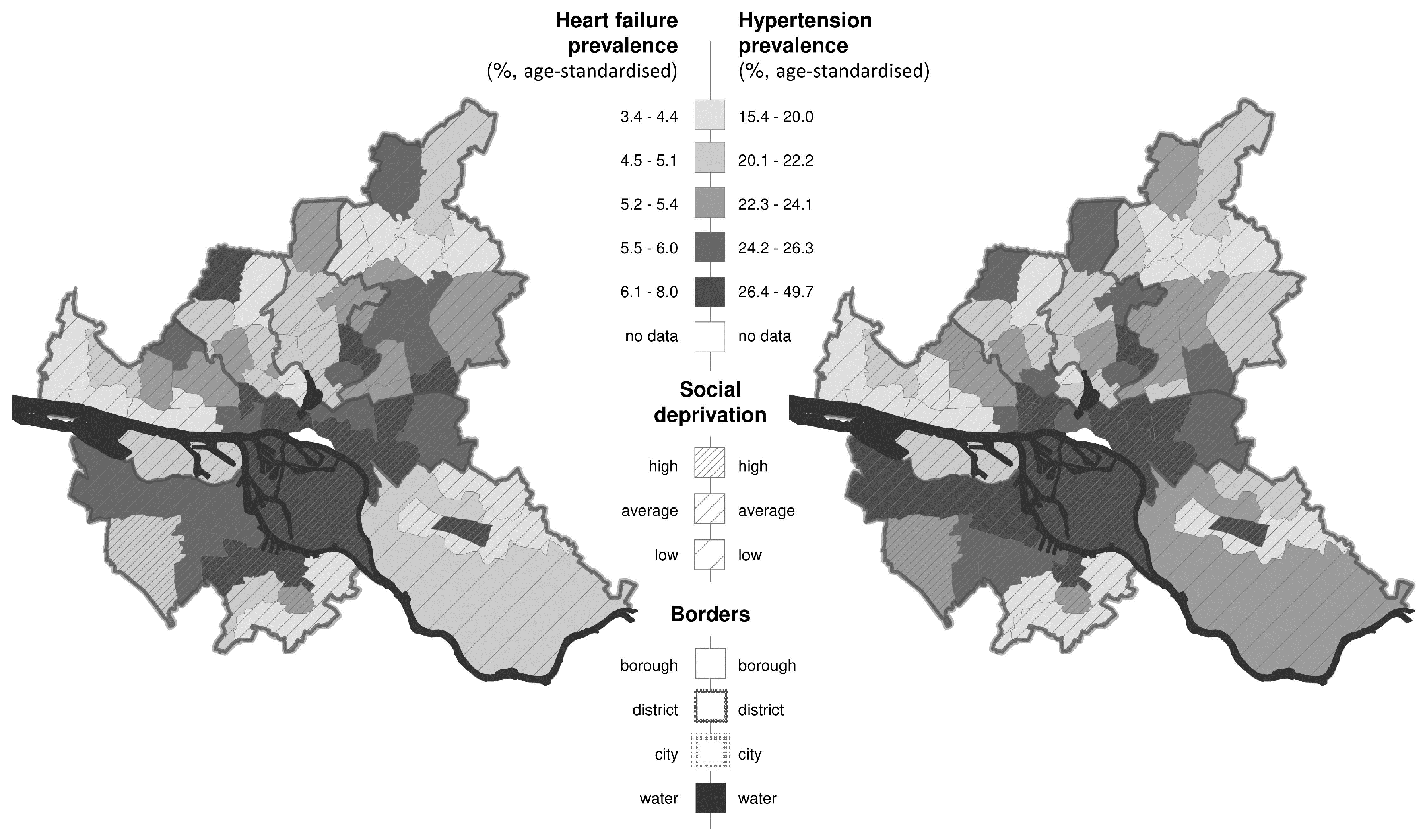
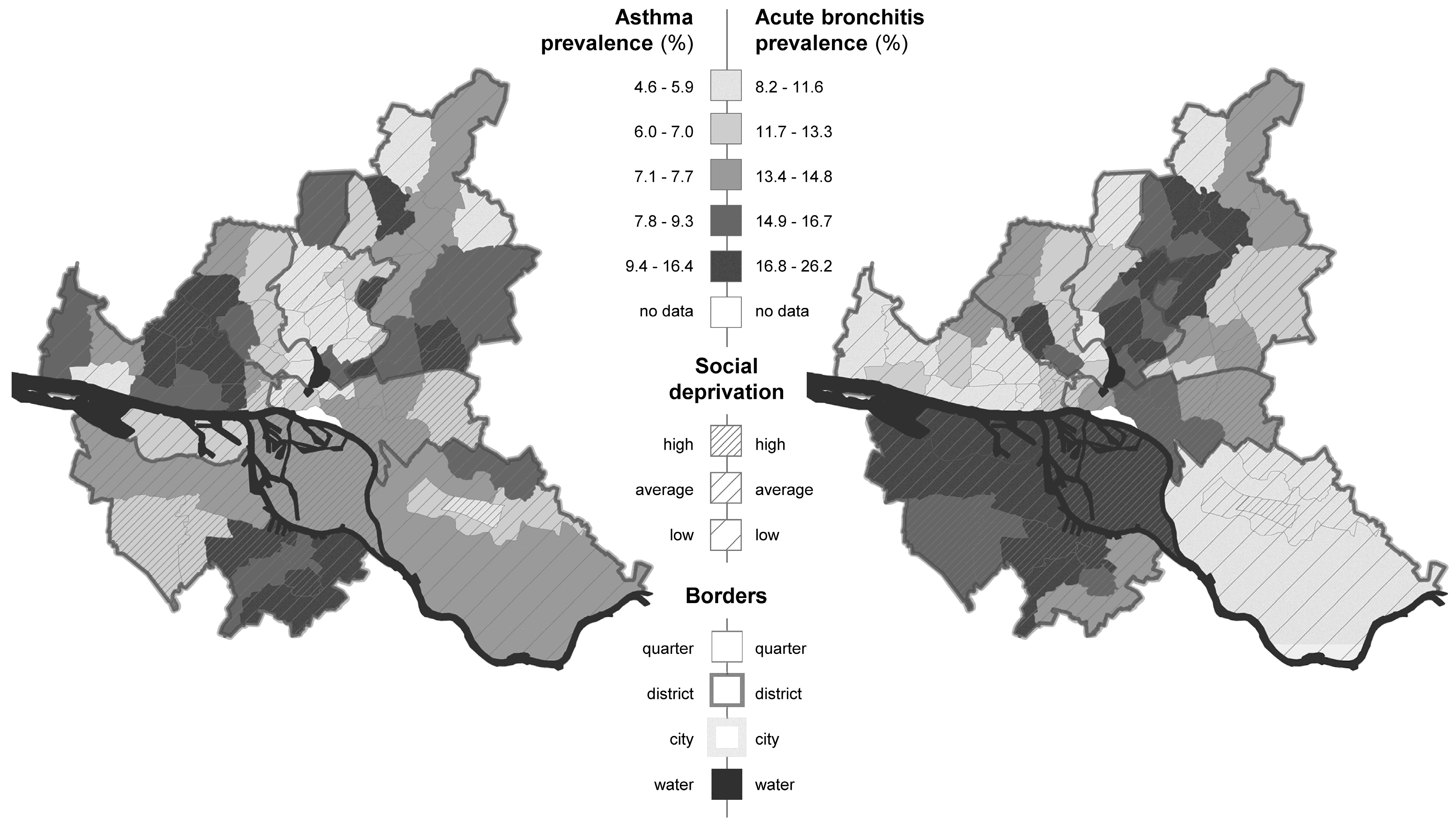
Prevalence was divided by borough and sex, respectively. Prevalence rates for heart failure (N = 73.230) and hypertension (N = 326.733) were available for the total population, the prevalence rates for acute bronchitis (N = 27.643) and asthma (N = 14.730) were obtained only for children up to 14 years of age.
The following ICD-10-codes (International Classification of Diseases) were used for the respective health outcome (
Table 1) [
26].
To account for potential geographical differences in age-distribution, we additionally calculated the age-standardized prevalence for heart failure and hypertension for each borough by using a weighting factor for every borough. This weighting factor was calculated by dividing the standard (average) population aged 65 and older for all Hamburg boroughs (standard population >65 years of age = 19.0% (micro census 2014)) divided by the population data >65 years of age for each borough, respectively [
25].
2.3. Road Traffic Noise
Road traffic noise mapping was performed by the State Ministry for Urban Development and the Environment according to the guideline 34, BImSchV and the Directive 2002/49/EC in 2007 using the software LimA [
27,
28]. The grid width was 10 m × 10 m and the immission height was 4 m above ground level. The resulting areas with a road traffic noise level of L
den (day, evening, and night) > 65 dB(A) as a threshold for high exposure to noise [
11] were the basis for our exposure analysis.
To determine the potentially affected population on the building block level, the road traffic noise map was overlayed with a population map, using the Geographical Information System ArcGIS 10.3.1 (Environmental System Research Institute (ESRI), Redlands, CA, USA). Population census data for 2013 on borough levels were obtained from the Statistical Office for Hamburg and Schleswig-Holstein [
25]. As typically not all houses of one building block are located in the same distance to the road (as the main sound source) or do not even face the same road, not the entire building block is affected by L
den > 65 dB(A). For this reason, we calculated the percentage of each building block that is affected by L
den > 65 dB(A). The resulting fractions were subsequently transferred to the number of potentially affected residents per building block by multiplying the percentage that is effected by L
den > 65 dB(A) with the total amount of inhabitants.
Afterwards, the population data and the number of potentially affected residents by Lden > 65 dB(A) were aggregated to the 67 boroughs. The percentage of the affected residents per borough was then used for further analysis.
2.4. Socioeconomic and Sociodemographic Borough Characteristics
Information on social indicators on borough level were obtained from the Statistical Office for Hamburg and Schleswig-Holstein [
25]. To classify a borough’s socioeconomic and sociodemographic situation and for the sake of the multivariable analysis, we used the variable “social deprivation”, which was obtained from a previously conducted PCA [
26]. This variable was then used as a proxy measure for a borough´s socioeconomic and sociodemographic situation. The following data (data from 2012) indicating the socioeconomic and demographic borough characteristics were considered in the PCA (
Table 2):
The factor of the PCA with the highest eigenvalue was used as the variable, which might sufficiently describe the social deprivation of a borough. The respective factor scores were categorized in subgroups where the lowest 25 percent of a borough according to the social deprivation were classified as low social deprivation, with the upper 25 percent as high social deprivation, and the rest as average social deprivation.
Additionally, data per borough describing the physician density per 1000 inhabitants used as a proxy measure for health access were obtained from the Statistical Office for Hamburg and Schleswig-Holstein [
25], and used for the statistical analyses as a potential co-factor.
2.5. Statistical Modeling
Due to the expected sex-specific differences, all analyses were conducted for both sexes, separately. Additionally, and to account for the age dependency of the two health outcomes “heart failure” and “hypertension” we used in the age-adjusted overall prevalence rates for computations.
Afterwards, we modeled associations between the potential risk factors and the prevalence of heart failure, hypertension, acute bronchitis, and asthma by multivariate regression (ANCOVA) analyses (Analysis of Covariance), using the IBM SPSS Statistics 23 program. To account for both, categorical and continuous variables in one model, the ANCOVA model was chosen. The independent variables “proportion of borough area affected by noise > 65 dB(A)” and “physician density” were considered continuous and were scaled by units per 5 percent increase in borough area and per unit step of social deprivation (three groups: low, average, and high). The covariates in the ANCOVA model were examined for interactions, but none could be confirmed.
The criterion for inclusion of a determinant in the final model was set to a significance level of p ≤ 0.05. For a measure of association between a determinant and the respective prevalence, the regression coefficient (B) was calculated by using the respective estimated standardized regression parameter of the ANCOVA model, and, therefore, adjusted for all other determinants was included in the model. All estimates of the regression coefficients were complemented by a 95% confidence interval (CI) and a p-value. The adjusted R-squared (R2) was provided as a measure of overall goodness-of-fit of the statistical model.
4. Discussion
Cardiovascular and respiratory diseases induce a great amount of disease burden in most countries [
1,
2]. It is reported that such morbidity and mortality is associated with social and environmental factors [
7,
8,
9,
10,
11]. This study was conducted to get the first possible insight in such an association based on large-scale, population-based urban data, which differentiates different spatial areas. The analysis conducted in the city of Hamburg indicated a strong association between the socioeconomic and sociodemographic background of a borough, classified by a PCA with the spatial prevalence of heart failure, hypertension, acute bronchitis, and asthma. Significantly higher prevalence rates for both age-standardized cardiovascular endpoints could be detected for boroughs classified as high social deprivation. For the respiratory health outcomes, the results were less strong but the trend showing higher prevalence among children in deprived boroughs remained. This is in agreement with previous reports on factors describing the social environment, such as deprived borough and cardiovascular and respiratory health outcomes, even after controlling for individual cofactors [
21,
22,
23,
30,
31,
32].
A PCA is a useful tool that reduces the complexity of correlated data, which can be easily collected and obtained as single indicator variables. On the contrary, the process of generalization leads to a loss of information, the criteria for the selection of variables for a PCA are not specified well, and the number of selected components is arbitrary. Whether a single principal component can sufficiently identify the socioeconomic and sociodemographic background is entirely dependent on the data, and the correlation matrix of the considered and included variables, their validity, and reliability [
33]. However, the data which entered the PCA and was used in our study can assumed to be credible [
25] and hence, should approximately reflect a borough´s socioeconomic and demographic background.
Besides the socioeconomic and sociodemographic borough background, > 65 years of age is suggested to be associated with rising cardiovascular prevalence rates [
34].
We regarded the crude prevalence rates of heart failure and hypertension together with the age distribution > 65 years of age and the variable “social deprivation” (data not shown). Prevalence rates of heart failure and hypertension were higher the more people aged 65 or older lived in a borough, additionally accompanied by boroughs classified as low social deprived areas, and vice versa. Contrarily, by using the age-standardized prevalence rates for the two cardiovascular endpoints, we found a pattern showing high age-standardized prevalence rates together with high social deprived areas, and vice versa, emphasizing on one hand the importance of age among these diseases, and on the other side the potential association between the socioeconomic and sociodemographic borough background and specific health outcomes.
The variable “physician density” used as a surrogate parameter for health access revealed no significant associations on any of the health outcomes, and even contrary results could be observed. The fact that only data on a borough level were available might have limited our analyses and hence the interpretation of our results. However, even though it can be assumed that the physician density should be evenly distributed in a metropolis such as Hamburg, we found great differences among boroughs (ranging from 0.2 to 10.4 per 1000 inhabitants and borough) (
Table 3). Nevertheless, it has to be noted that people do not always seek medical care close to their home address. Instead, they seek help at a specialist in another borough or go directly to the hospital. Additionally, diseases might be underdiagnosed in some certain groups of the population due to differences in seeking health care behavior. Hence, our results might be biased. In this context it should be noticed, that we only obtained data from statutory health insurance patients with at least one contact, to a contract physician working in the ambulatory sector. No data regarding the proportion and distribution of privately insured individuals or data from private practice were available, and the data considered in our study only capture a fraction of the estimated prevalence. However, it is suggested that approximately 10 to 20 percent of all individuals in Hamburg are privately insured [
26] (additionally, please see
Table A1 depicting the amount of the statutory health insured patients per borough). Therefore, our data should cover the largest amount of prevalence rates. Nevertheless, due to the high costs of the private insurance, mostly people above a certain income level can afford this status. Therefore, the results might be biased in areas with low social deprivation due to the lack of data from the privately insured population.
Contrary to many other studies [
12,
13,
14,
35,
36,
37], noise did not show any significant association with any cardiovascular or respiratory disease. Road traffic noise was transferred to the number of potentially affected residents per building block, and scaled in percent per borough. Certainly this does not reflect the real environment, or covers the real circumstances of noise exposure. Additionally, it was not possible to differentiate between residential buildings and non-residential buildings; therefore, a non-differential misclassification bias might have occurred and affected our results. Furthermore, individual factors describing the housing conditions, location of rooms, subjective noise annoyance, hearing problems, or length of residence are known to potentially influence cardio-respiratory disease [
35,
38,
39]. Additionally, aircraft or industrial noise [
10,
40] is suggested to affect cardiovascular and respiratory disease and was, due to missing data, not considered in our study. Nevertheless, exposure to noise also occurs in many workplaces, and was associated with a number of cardiovascular diseases [
41,
42,
43].
Exposure to gaseous (carbon monoxide, sulphur dioxide, nitrogen dioxide, ozone) and particulate (PM
2.5 or PM
10) air pollutants, which is higher in cities than in non-urban areas, has been associated with cardiovascular and respiratory disease morbidity and mortality. Several studies investigated short-term effects and found the strongest associations on the day of exposure, or one to three days after exposure [
44,
45]. Other studies investigated chronic and long-term exposure of air pollution and found a higher risk for all causes and cardiovascular and respiratory mortality [
19,
46,
47]. In the KORA study, significant associations were found between PM
2.5 and hypertension using noise as a covariate [
7]. However, for this first investigation, no data on air pollution in the city of Hamburg were available.
It is hypothesized that asthma is less common in children or families where older siblings are present [
48]. We therefore, conducted an analysis including the variable “number of family members”, which, additionally was identified as a second component from the PCA. This factor described the household size and number of children per family. However, inclusion of this variable in the ANCOVA model did not change the significance and magnitude of the associations of included variables with the respective prevalence (data not shown).
Furthermore, besides genetic disposition, family history, and previous atopic disease [
49,
50], individual behavioral factors such as smoking status including passive smoking, alcohol intake, or physical activity, awareness for diseases such as hypertension and factors describing the daily routine are discussed to be associated with the occurrence of different cardiovascular and respiratory health outcomes [
7,
23,
35,
36,
37,
51,
52,
53,
54,
55].
Another limitation of our study is the temporality: due to the fact that prevalence, not incidence data was examined, it cannot be determined if traffic noise exposure or social depravity preceded the diseases. While it is not discernible that the children afflicted with acute bronchitis or asthma may have moved due to their disease, poor health could also result in a loss of income and cause someone to move to more affordable housing, e.g., to areas with increased social deprivation or increased road traffic noise. Contrarily, families with a better socioeconomic situation might have moved to areas with less noise and less deprivation.
Our ecological study design has the advantage that a large number of large-scale, population-based aggregated data for the city of Hamburg could easily be obtained and analyzed, and the first potential associations could be found and discussed. So far, our first results coincide with other studies showing the potential importance of the socioeconomic and sociodemographic background of a borough, even though our ecological study design makes the results of this study difficult to interpret and potentially misleading.
To account for the above-discussed limitation of this first study;, we will conduct in a second step a case-control study, with the example of hypertensive patients as cases aimed at elucidating the potential individual risk factors together with environmental living and working conditions. Our control group will be obtained from the Hamburg City Health Study (HCHS), the largest local follow-up health study worldwide with an estimated number of 45,000 participants. This study just started in spring 2016, and will run for the coming 12 years. Additionally, noise data (traffic noise, aircraft noise, and industrial noise) as well as data about air pollution shall be selectively collected in the near living environment of participants, and considered in the upcoming studies to better analyze potential environmental covariates.

 ,
, 
{kind=link}
{kind=link}
{kind=link}


