
Virtual Reality Assessment of Attention Deficits in Traumatic Brain Injury: Effectiveness and Ecological Validity

 ,
,  and
and
Abstract
:1. Introduction
1.1. Motivation
1.2. VR Technology
1.3. The Use of VR for Neuropsychological Assessment
1.4. Problem Statement
2. Materials and Methods
2.1. Research Context and Participants
2.2. Apparatus
2.3. Materials
2.3.1. Computerized Battery for the Assessment of Attention Disorders
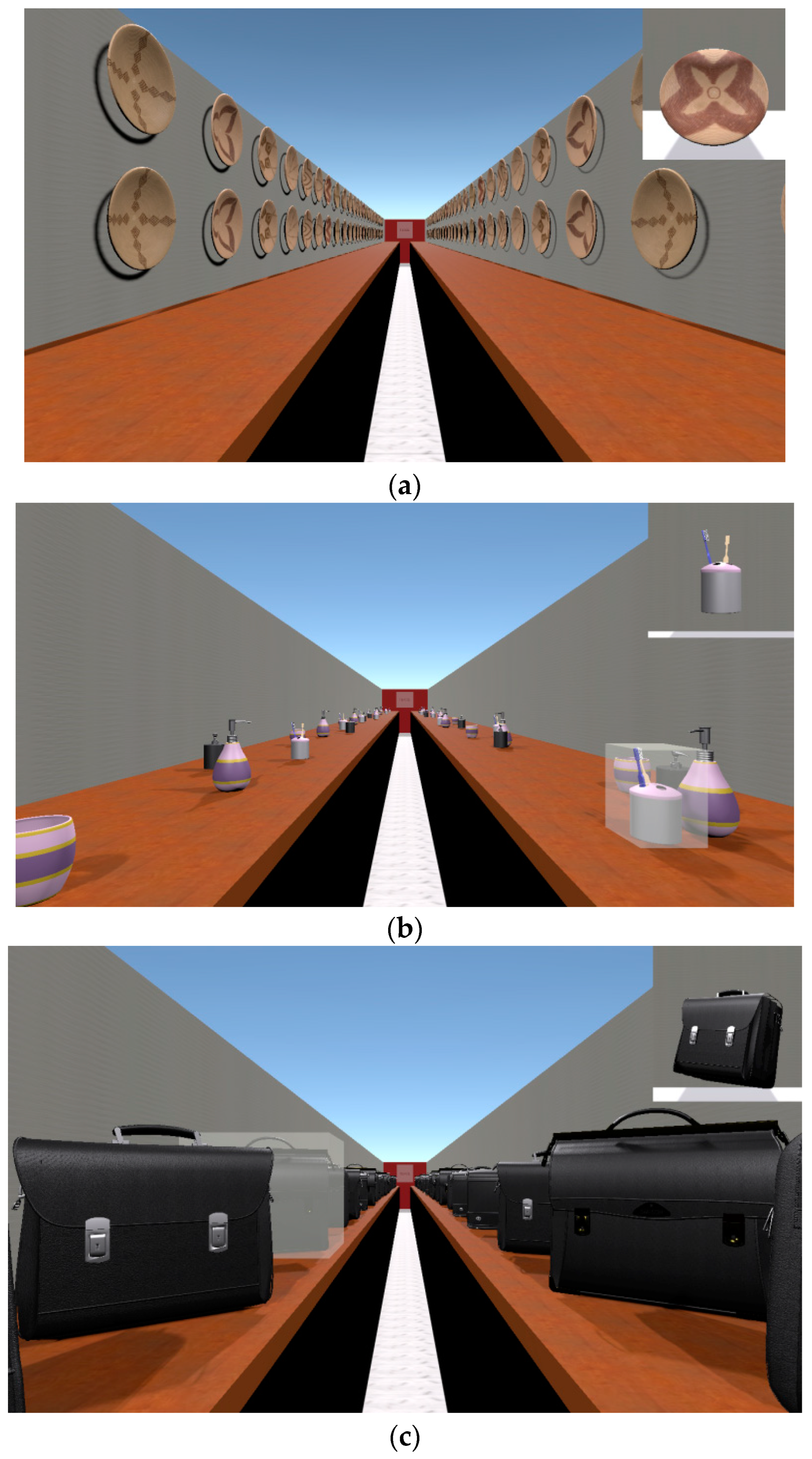
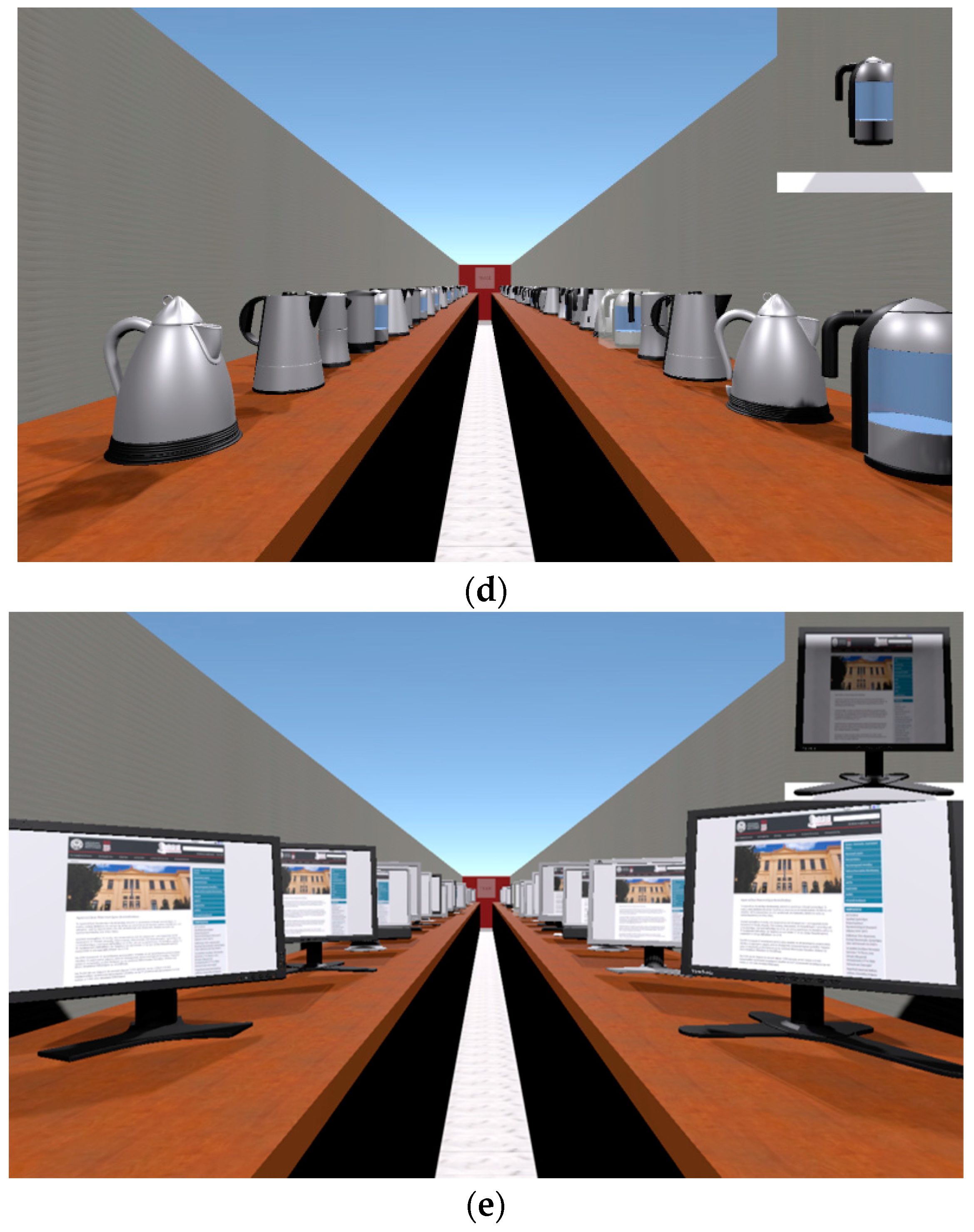
- The Supermarket-selective attention subtest was performed in a 3D scene resembling a real visit to a supermarket. The examinee moved (either in a forward or backward direction) through a corridor by scrolling the mouse wheel. The task required the examinee to scan the scene visually and select (mouse click) all objects/products that match a predefined target (i.e., all the kettles with a certain pattern) as quickly as possible. The subtest consisted of six levels with different objects for each level (plates, toothbrushes, kettles, briefcases, and televisions; see Figure 1a–e) and the examinee proceeded to the next level when he/she thought that he/she had found all the level’s objects. The number of all selectable objects was 351, while the targets were 83. The total duration of the entire subtest depended on the examinee’s reaction speed and usually did not take more than 10 min to complete. Performance indices were calculated separately for each level and the total performance for all levels.
- 2.
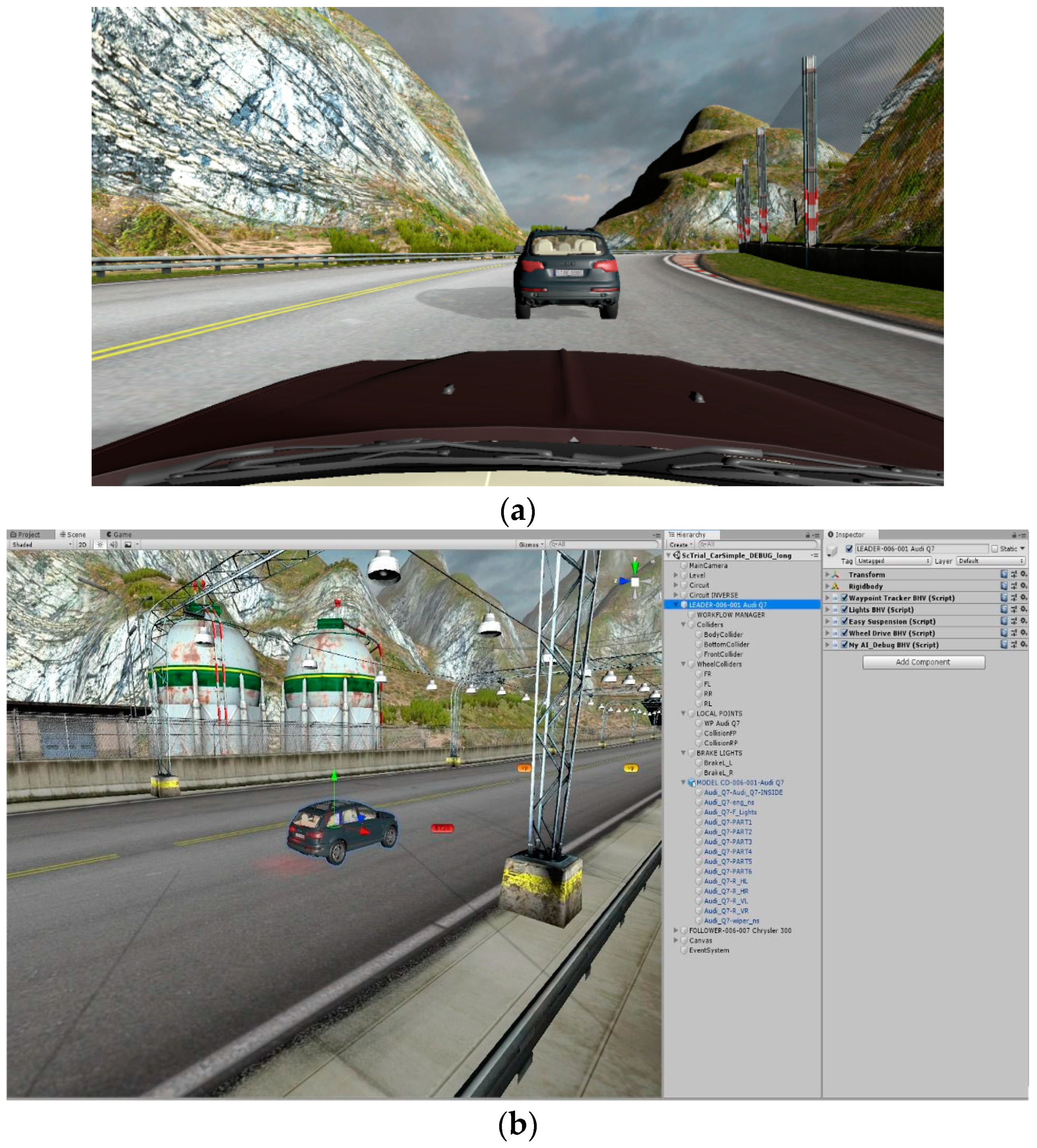
- The Car driving-sustained attention subtest involves the examinee participating in a monotonous driving task, where they follow another car (lead car) on a highway (Figure 2). The lead car was automated using a script component, relieving the examinee of navigation responsibilities. Notably, this task extensively employed the physics engine of Unity, integrated with CBAAD script components that applied forces to both the leader and follower cars, effectively controlling their movements and wheel colliders. This incorporation of a physics engine ensures a more realistic driving experience. Throughout the task, the lead car driver intermittently applies brakes at certain positions on the highway, signaled by the activation of red brake lights. The examinee’s objective was to promptly press the brake button (Spacebar) upon observing the brake lights, thereby avoiding a collision with the lead car. The response time, indicating the speed of reaction, was recorded when the brake button was pressed within a minimum time frame of 5 s. Failure to press the brake button within this interval resulted in a recorded error, signifying a crash. Irrespective of whether a crash occurred or not, the driving task continued until the subsequent breakpoint. Any inadvertent pressing of the brake button outside the brake phase was categorized as a false alarm error. The entire duration of this task was set at 3 min.
- 3.
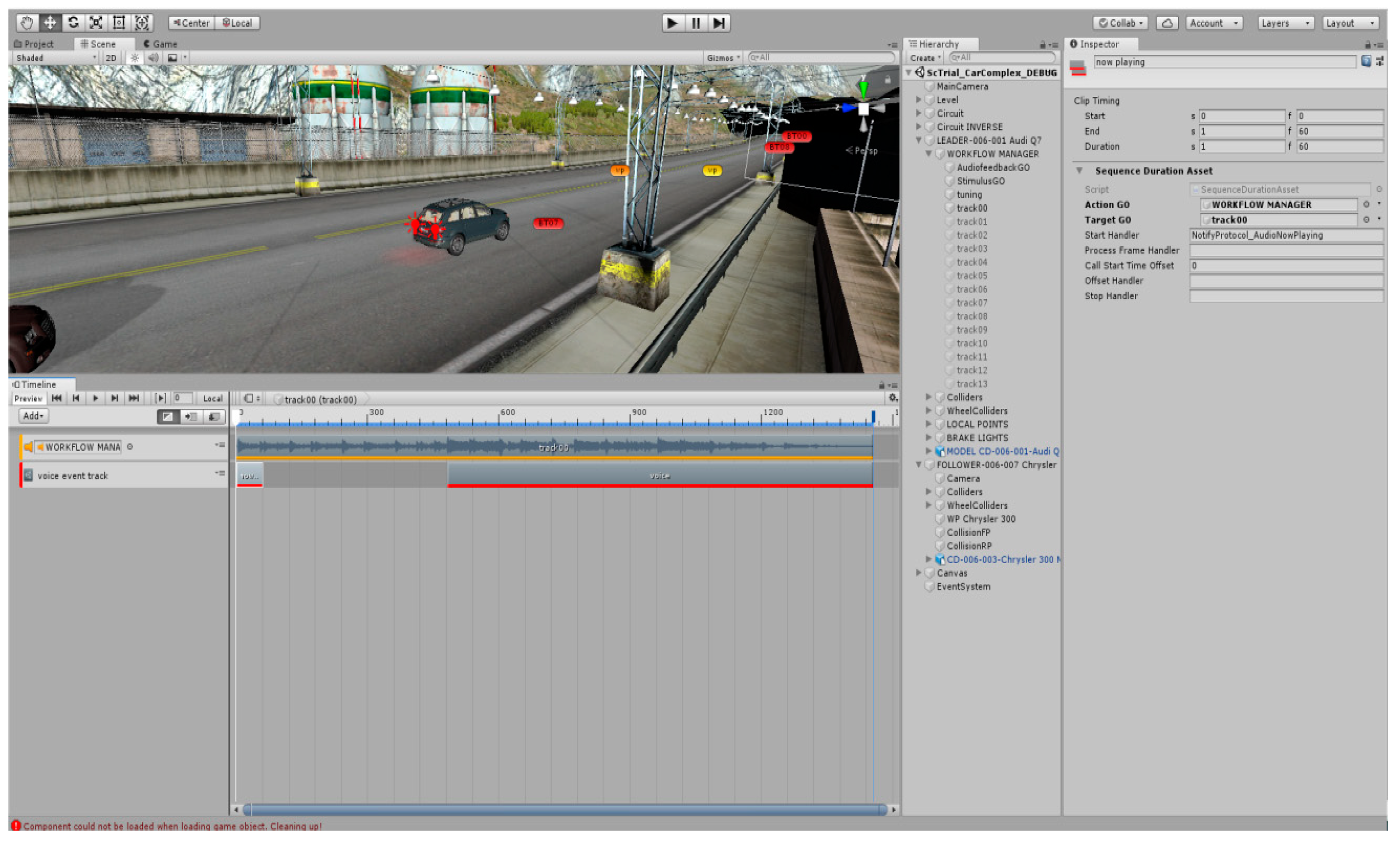
- The Car driving while listening to music-divided attention subtest is a dual task consisting of a visual component (which is based on the Car driving subtest) and an audio component, which resembles the everyday habit of listening to music. More specifically, the latter uses the Unity timeline component (see Figure 3) and involves listening to different song clips. The composition, orchestration, and production of the song clips playing in the subtest were delegated to a music professional. In between songs, he/she hears the tuner searching for the next song. The examinee was asked to press a “buzzer key” as quickly as possible (response time) only for songs including a female voice, which represented the correct response to the task. For songs with a male voice or instrumental pieces, the examinee had to withhold his/her response by avoiding pressing the button; in case he/she hit the button, this event was recorded as a false alarm error. Moreover, if he/she forgot to press the button to indicate hearing a female-voiced song, an omission error was recorded. The second (audio) task was independent of the driving task since the need for a response to a female-voiced song could occur either during driving or a brake phase. The whole test duration was approximately 10 min.
- 4.
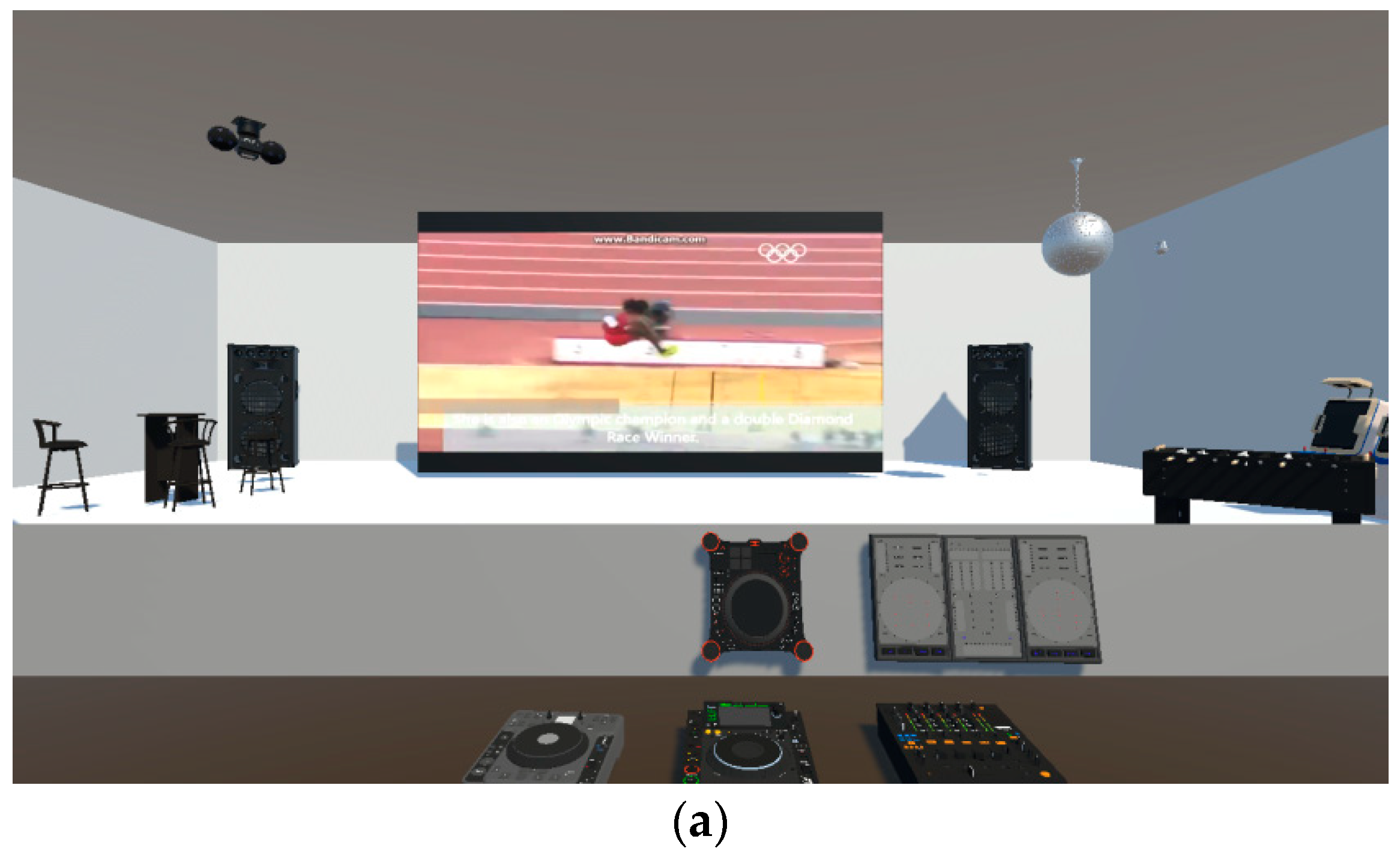
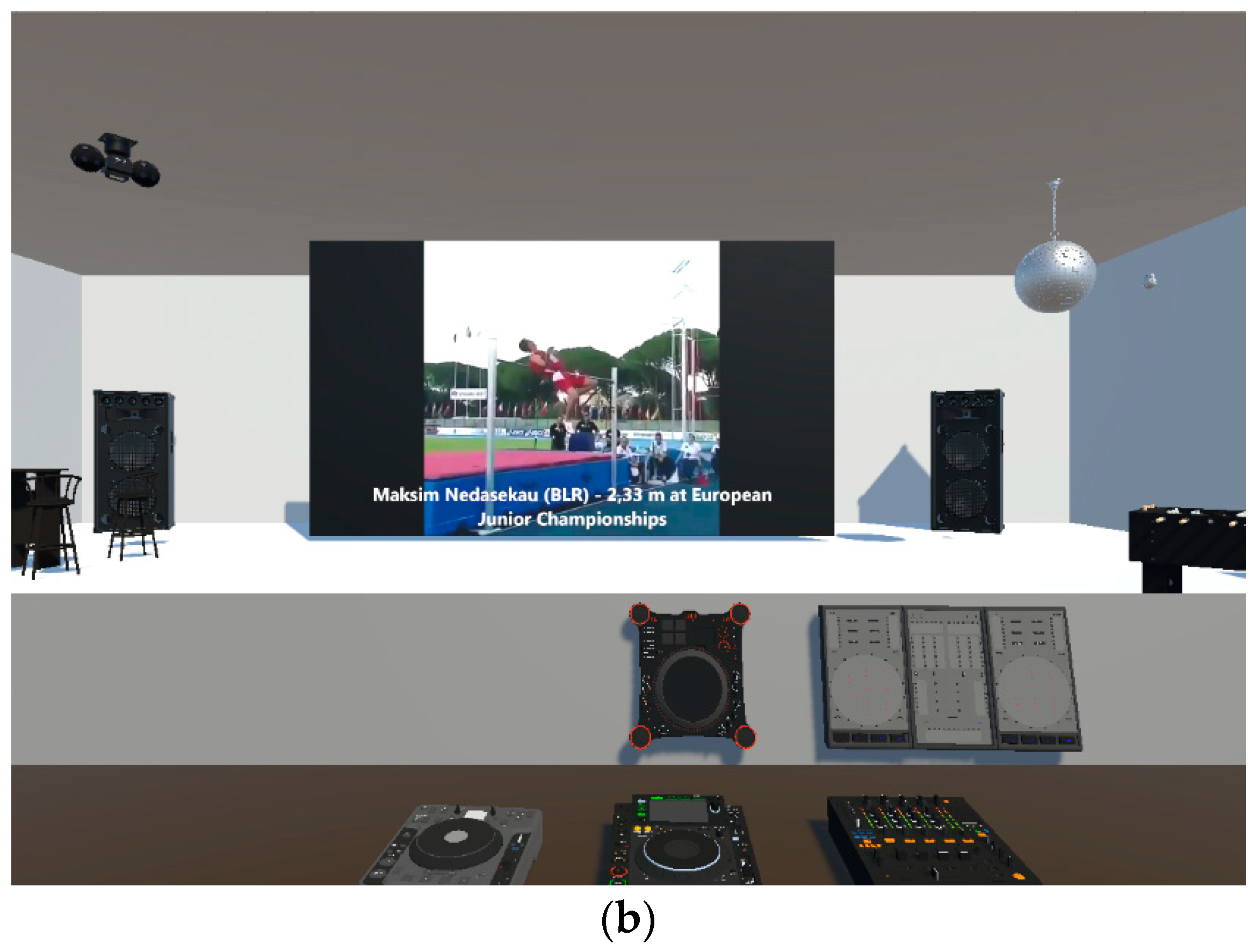
- The TV sports watching–switching attention subtest is a task designed to measure one’s ability to alternate his/her attention between two same modality tasks (visual). The 3D environment here was very similar to a real café and the examinee sat in front of a monitor panel watching track and field sports (Figure 4a,b). In particular, he/she watched athletes perform high and long jumps. The player showed clips from two video sources (high and long jumps) without splitting the video sources via the VideoClipInfo-type, which were references and denoted the start and end of the clips, and also the start and end of the jump. Many VideoClipInfo objects were used to form a sequence of clips, which represented the clip sequence for the examinee responding to the jumps. For each type of jump, the examinee had to press as quickly as possible (response time) the correct jump-type button (there were two buttons), as the athlete was airborne (correct response). If either of the buttons was pressed when the athlete was grounded, the response was recorded as an error. If the wrong jump-type button is pressed for the jump (key error), the response was recorded as a false alarm error. In case someone forgot to press any key as the athlete was airborne, this constituted an omission error. The whole test duration lasted no more than 5 min.
2.3.2. Attention Related Cognitive Errors Scale
2.4. Procedure
2.5. Data Analysis
3. Results
4. Discussion
4.1. The CBAAD’s Ability to Differentiate TBI Patients from Healthy Controls
4.2. The CBAAD’s Predictive Ability concerning Errors in Daily Life Activities
5. Conclusions
6. Theoretical and Practical Implications
- Advancement in assessment tools: the study highlights the potential for innovative neuropsychological assessment tools, using VR to enhance ecological validity and sensitivity for measuring cognitive impairments.
- Understanding attentional deficits in TBI patients: the research deepens our theoretical understanding of attentional impairments in TBI patients, examining specific components of attention through the CBAAD.
- Linking cognitive performance to everyday functioning: establishing a connection between performance on the CBAAD and real-life attentional errors in TBI patients bridges the gap between cognitive assessments in controlled settings and practical implications for patients’ daily lives.
- Potential for individualized rehabilitation: the study suggests that the CBAAD’s effectiveness in predicting attentional errors opens avenues for personalized rehabilitation planning, addressing specific challenges faced by each patient.
- Early detection and intervention: the CBAAD offers a practical tool for the early detection of attentional impairments in TBI patients, enabling timely intervention strategies and facilitating interactions through well-presented visual elements in VR applications.
- Enhanced rehabilitation planning: implementing the CBAAD in clinical settings aids in formulating effective rehabilitation plans by identifying specific attentional domains of difficulties, with VR applications enhancing the participants’ comprehension of real-life scenarios.
- Objective measurement of progress: the CBAAD provides a standardized way to objectively measure the progress of TBI patients during rehabilitation, allowing clinicians to track their improvements over time and adjust treatment plans accordingly.
- Facilitating therapeutic feedback: the CBAAD’s ability to identify attentional strengths and weaknesses facilitates the therapeutic feedback, helping patients gain insights into their difficulties and motivating their engagement in rehabilitation efforts, with VR-supported assessments offering multisensory exploratory contexts.
- Supporting long-term functional outcomes: addressing attentional deficits early on with the CBAAD has the potential to improve long-term functional outcomes for TBI patients, positively impacting various aspects of their lives.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aulisio, M.C.; Han, D.Y.; Glueck, A.C. Virtual reality gaming as a neurorehabilitation tool for brain injuries in adults: A systematic review. Brain Inj. 2020, 34, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu-Bonneau, B.; Fortier-Brochu, C.; Ivers, H.; Morin, C. Attention following traumatic brain injury: Neuropsychological and driving simulator data, and association with sleep, sleepiness, and fatigue. Neuropsychol. Rehabil. 2017, 27, 216–238. [Google Scholar] [CrossRef] [PubMed]
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2018, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.K. Diffusion MRI: Theory, Methods, and Applications; Oxford University Press: Oxford, UK, 2010. [Google Scholar] [CrossRef]
- Choi, J.Y.; Yi, S.H.; Ao, L.; Tang, X.; Xu, X.; Shim, D.; Yoo, B.; Park, E.S.; Rha, D. Virtual reality rehabilitation in children with brain injury: A randomized controlled trial. Dev. Med. Child Neurol. 2021, 63, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Temkin, N.R.; Corrigan, J.D.; Dikmen, S.S.; Machamer, J. Social functioning after traumatic brain injury. J. Head Trauma Rehabil. 2009, 24, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Morales-Rodríguez, M.; Pavard, B. Design of an emotional and social interaction paradigm for the animation of 3D characters: The case of a therapy for brain injured people (the mirror neuron paradigm). Virtual Real. 2007, 2, 175–184. [Google Scholar] [CrossRef]
- Malegiannaki, A.C.; Metallidou, P. Development of attentional functions in school-age: Evidence from both traditional and computerized tasks. J. Educ. Dev. Psychol. 2017, 7, 42–51. [Google Scholar] [CrossRef]
- Van Zomeren, A.H.; Brouwer, W.H. Clinical Neuropsychology of Attention; Oxford University Press: Oxford, UK, 1994; Available online: https://psycnet.apa.org/record/1994-98150-000 (accessed on 12 August 2023).
- Kelly, T.P. The clinical neuropsychology of attention in school-aged children. Child Neuropsychol. 2000, 6, 24–36. [Google Scholar] [CrossRef]
- Belmont, A.; Agar, N.; Azouvi, P. Subjective fatigue, mental effort, and attention deficits after severe traumatic brain injury. Neurorehabilit. Neural Repair 2009, 23, 939–944. [Google Scholar] [CrossRef]
- Mathias, J.L.; Wheaton, P. Changes in attention and information-processing speed following severe traumatic brain injury: A meta-analytic review. Neuropsychology 2007, 21, 212–223. [Google Scholar] [CrossRef]
- Sinclair, K.L.; Ponsford, J.L.; Rajaratnam, S.M.; Anderson, C. Sustained attention following traumatic brain injury: Use of the Psychomotor Vigilance Task. J. Clin. Exp. Neuropsychol. 2013, 35, 210–224. [Google Scholar] [CrossRef] [PubMed]
- Michael, G.A.; Masson, M.; Robert, E.; Bacon, E.; Desert, J.-F.; Rhein, F.; Offerlin-Meyer, I.; Colliot, P. Disturbances of selective attention in traumatic brain injury and schizophrenia: What is common and what is different? Psychol. Française 2015, 60, 387–402. [Google Scholar] [CrossRef]
- Leclercq, M.; Azouvi, P. Attention after traumatic brain injury. In Applied Neuropsychology of Attention: Theory, Diagnosis, and Rehabilitation; Leclerq, M., van Zomeren, A.H., Eds.; Oxford University Press: Oxford, UK, 2002; pp. 257–279. [Google Scholar] [CrossRef]
- Neguț, A.; Jurma, A.M.; David, D. Virtual-reality-based attention assessment of ADHD: ClinicaVR: Classroom-CPT versus a traditional continuous performance test. Child Neuropsychol. 2017, 23, 692–712. [Google Scholar] [CrossRef] [PubMed]
- Malegiannaki, A.C.; Metallidou, P. Assessment of sustained attention: Psychometric properties of the computerized SART. Hellenic J. Psychol. 2012, 9, 162–183. [Google Scholar]
- Moser, M.B.; Rowland, D.C.; Moser, E.I. Place cells, grid cells, and memory. Cold Spring Harb. Perspect. Biol. 2015, 7, a021808. [Google Scholar] [CrossRef] [PubMed]
- Parsons, N. Ecological validity in virtual reality-based neuropsychological assessment. In Encyclopedia of Information Science and Technology; Khosrow-Pour, M., Ed.; IGI Global: Hershey, PA, USA, 2016; pp. 214–223. [Google Scholar] [CrossRef]
- Gates, N.J.; Kochan, N.A. Computerized and on-line neuropsychological testing for late-life cognition and neurocognitive disorders: Are we there yet? Curr. Opin. Psychiatry 2015, 28, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Hogan, C.; Cornwell, P.; Fleming, J.; Man, D.W.; Shum, D.H. Assessment of prospective memory after stroke utilizing virtual reality. Virtual Real. 2021, 27, 333–346. [Google Scholar] [CrossRef]
- Simmons, C.; Conley, M.I.; Gee, D.G.; Baskin-Sommers, A.; Barch, D.M.; Hoffman, E.A.; Huber, R.S.; Iacono, W.G.; Nagel, B.J.; Palmer, C.E.; et al. Responsible use of open-access developmental data: The adolescent brain cognitive development (ABCD) study. Psychol. Sci. 2021, 32, 866–870. [Google Scholar] [CrossRef]
- Kourtesis, P.; Collina, S.; Doumas, L.A.A.; MacPherson, E. Validation of the Virtual Reality Everyday Assessment Lab (VR-EAL): An immersive virtual reality neuropsychological battery with enhanced ecological validity. Int. J. Neuropsychol. Soc. 2021, 27, 181–196. [Google Scholar] [CrossRef]
- Spreij, L.; Visser-Meily, M.S.; Sibbel, J.; Gosselt, I.; Nijboer, T. Feasibility and user-experience of virtual reality in neuropsychological assessment following stroke. Neuropsychol. Rehabil. 2020, 32, 499–519. [Google Scholar] [CrossRef]
- Bashiri, A.; Ghazisaeedi, M.; Shahmoradi, L. The opportunities of virtual reality in the rehabilitation of children with attention deficit hyperactivity disorder: A literature review. Korean J. Pediatr. 2017, 60, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Pellas, N.; Dengel, A.; Christopoulos, A. A scoping review of immersive Virtual Reality in STEM education. IEEE Trans. Learn. Technol. 2020, 13, 748–761. [Google Scholar] [CrossRef]
- Pellas, N.; Mystakidis, S.; Kazanidis, I. Immersive virtual reality in K-12 and higher education: A systematic review of last decade scientific literature. Virtual Real. 2021, 25, 835–861. [Google Scholar] [CrossRef]
- Câmara, J.; Ferreira, R.; Teixeira, L.; Nóbrega, J.; Romeira, C.; Bermúdez i Badia, S.; Faria, A.L. Efficacy of adaptive cognitive training through desktop virtual reality and paper-and-pencil in the treatment of mental and behavioral disorders. Virtual Real. 2023, 27, 291–306. [Google Scholar] [CrossRef]
- Kourtesis, P.; Korre, D.; Collina, S.; Doumas, L.A.; MacPherson, S.E. Guidelines for the development of immersive virtual reality software for cognitive neuroscience and neuropsychology: The development of virtual reality everyday assessment lab (VR-EAL), a neuropsychological test battery in immersive virtual reality. Front. Comput. Sci. 2020, 1, 12. [Google Scholar] [CrossRef]
- Corti, C.; Oprandi, M.C.; Chevignard, M.; Jansari, A.; Oldrati, V.; Ferrari, E.; Martignoni, M.; Romaniello, R.; Strazzer, S.; Bardoni, A. Virtual-reality performance-based assessment of cognitive functions in adult patients with acquired brain injury: A scoping review. Neuropsychol. Rev. 2022, 32, 352–399. [Google Scholar] [CrossRef] [PubMed]
- Pieri, L.; Serino, S.; Cipresso, P.; Mancuso, V.; Riva, G.; Pedroli, E. The ObReco-360°: A new ecological tool to memory assessment using 360° immersive technology. Virtual Real. 2021, 26, 639–648. [Google Scholar] [CrossRef]
- Lesk, V.E.; Shamsuddin, S.N.W.; Elizabeth, R.; Walters, E.R.; Ugail, H. Using a virtual environment to assess cognition in the elderly. Virtual Real. 2014, 18, 271–279. [Google Scholar] [CrossRef]
- Calvillo, M.; Irimia, A. Neuroimaging and psychometric assessment of mild cognitive impairment after traumatic brain injury. Front. Psychol. 2020, 11, 14–23. [Google Scholar] [CrossRef]
- Krawczyk, D.C.; Han, K.; Martinez, D.; Rakic, J.; Kmiecik, M.J.; Chang, Z.; Nguyen, L.; Lundie, M.; Cole, R.C.; Nagele, M.; et al. Executive function training in chronic traumatic brain injury patients: Study protocol. Trials 2019, 20, 435. [Google Scholar] [CrossRef]
- Park, M. Driving scene-based driving errors in brain injury patients and their relevance to cognitive perceptual function and functional activity level: A cross-sectional study. Medicine 2019, 98, e16315. [Google Scholar] [CrossRef] [PubMed]
- Bock, O.; Drescher, U.; Van Winsum, W.; Kesnerus, T.F.; Voelcker-Rehage, C. A virtual-reality approach for the assessment and rehabilitation of multitasking deficits. Int. J. Virtual Augment. Real. 2018, 2, 48–58. [Google Scholar] [CrossRef]
- Voinescu, A.; Petrini, K.; Stanton Fraser, D.; Lazarovicz, R.A.; Papavă, I.; Fodor, L.A.; David, D. The effectiveness of a virtual reality attention task to predict depression and anxiety in comparison with current clinical measures. Virtual Real. 2021, 27, 119–140. [Google Scholar] [CrossRef]
- Abich, J.; Parker, J.; Murphy, J.S.; Eudy, M. A review of the evidence for training effectiveness with virtual reality technology. Virtual Real. 2021, 25, 919–933. [Google Scholar] [CrossRef]
- Romero-Ayuso, D.; Toledano-González, A.; Rodríguez-Martínez, M.D.; Arroyo-Castillo, P.; Triviño-Juárez, J.M.; González, P.; Ariza-Vega, P.; González, A.D.P.; Segura-Fragoso, A. Effectiveness of virtual reality-based interventions for children and adolescents with ADHD: A systematic review and meta-analysis. Children 2021, 8, 70. [Google Scholar] [CrossRef] [PubMed]
- Lorentz, L.; Simone, M.; Zimmermann, M.; Studer, B.; Suchan, B.; Althausen, A.; Estocinova, J.; Müller, K.; Lendt, M. Evaluation of a VR prototype for neuropsychological rehabilitation of attentional functions. Virtual Real. 2021, 27, 187–199. [Google Scholar] [CrossRef]
- Malegiannaki, A.C.; Malegiannakis, A.; Garefalaki, E.; Kosmidis, M.H. Assessing attention in a 3D environment: Preliminary evidence from a pilot study using the Computerized Battery for the Assessment of Attention Disorders (CBAAD). Dialogues Clin. Neurosci. Ment. Health 2019, 4, 185–192. [Google Scholar]
- Cheyne, J.; Carriere, J.; Smilek, D. Absent-mindedness: Lapses of conscious awareness and everyday cognitive failures. Conscious. Cogn. 2006, 15, 578–592. [Google Scholar] [CrossRef]
- White, M.G. Why human subjects research protection is important. Ochsner J. 2020, 20, 16–33. [Google Scholar] [CrossRef]
- Malegiannaki, A.C.; Garefalaki, E.; Nestoraki, D.; Malegiannakis, A.; Kosmidis, M.H. Can the Trail Making Test be substituted by a 3D computerized visit to a supermarket? Clinical implications. Dialogues Clin. Neurosci. Ment. Health 2021, 4, 71–80. [Google Scholar]
- Jaschinski-Kruza, W. Visual strain during VDU work: The effect of viewing distance and dark focus. Ergonomics 1988, 31, 1449–1465. [Google Scholar] [CrossRef] [PubMed]
- Caeyenberghs, K.; Leemans, A.; Leunissen, I.; Gooijers, J.; Michiels, K.; Synaert, S.; Swinnen, S.P. Altered structural networks and executive deficits in traumatic brain injury patients. Brain Struct. Funct. 2014, 219, 193–209. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.L.; Worthington, A. Neurobehavioral abnormalities associated with executive dysfunction after traumatic brain injury. Front. Behav. Neurosci. 2017, 11, 195. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Bai, G.; Wang, S.; Yang, X.; Gan, S.; Jia, X.; Yin, B.; Yan, Z. Strategic white matter injury associated with long-term information processing speed deficits in mild traumatic brain injury. Hum. Brain Mapp. 2020, 41, 4431–4441. [Google Scholar] [CrossRef]
- Ponsford, A.O.; Velikonja, D.; Janzen, S.; Harnett, A.; McIntyre, A.; Wiseman-Hakes, C.; Togher, L.; Teasell, R.; Kua, A.; Patsakos, E.; et al. Guidelines for cognitive rehabilitation following traumatic brain injury, Part II: Attention and information processing speed. J. Head Trauma Rehabil. 2023, 38, 38–51. [Google Scholar] [CrossRef]
- Bivona, U.; D’Ippolito, M.; Giustini, M.E.; Vignally, P.; Longo, E.; Taggi, F.; Formisano, R. Return to driving after severe traumatic brain injury: Increased risk of traffic accidents and personal responsibility. J. Head Trauma Rehabil. 2012, 27, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Cullen, N.; Krakowski, A.; Taggart, C. Early neuropsychological tests as correlates of return to driving after traumatic brain injury. Brain Inj. 2014, 28, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Tamietto, M.; Torrini, G.; Adenzato, M.; Pietrapiana, P.; Rago, P.; Perino, C. To drive or not to drive (after TBI)? A review of the literature and its implications for rehabilitation and future research. NeuroRehabilitation 2006, 21, 81–92. Available online: https://pubmed.ncbi.nlm.nih.gov/16720941/ (accessed on 12 August 2023). [CrossRef]
- Gaudet, C.E.; Konin, J.; Faust, D. Immediate post-concussion and cognitive testing: Ceiling effects, reliability, and implications for interpretation. Arch. Clin. Neuropsychol. 2021, 36, 561–569. [Google Scholar] [CrossRef]
- Malegiannaki, A.C.; Metallidou, P.; Kiosseoglou, G. Psychometric properties of the Test of Everyday Attention for Children in Greek-speaking school children. Eur. J. Dev. Psychol. 2015, 12, 234–242. [Google Scholar] [CrossRef]
- Guilmette, T.J.; Sweet, J.J.; Hebben, N.; Koltai, D.; Mark Mahone, E.; Spiegler, B.J.; Stucky, K.; Westerveld, M.; Conference Participants. American Academy of Clinical Neuropsychology consensus conference statement on uniform labeling of performance test scores. Clin. Neuropsychol. 2020, 34, 437–453. [Google Scholar] [CrossRef] [PubMed]
- Manly, T.; Anderson, V.; Nimmo-Smith, I.; Turner, A.; Watson, P.; Robertson, I.H. The differential assessment of children’s attention: The Test of Everyday Attention for Children (TEA-Ch), normative sample and ADHD performance. J. Child Psychol. Psychiatry 2001, 42, 1065–1081. [Google Scholar] [CrossRef] [PubMed]
- Van Solkema, M.; McCann, C.; Barker-Collo, S.; Foster, A. Attention and communication following TBI: Making the connection through a meta-narrative systematic review. Neuropsychol. Rev. 2020, 30, 345–361. [Google Scholar] [CrossRef] [PubMed]
- Pinnow, D.; Causey-Upton, R.; Meulenbroek, P. Navigating the impact of workplace distractions for persons with TBI: A qualitative descriptive study. Sci. Rep. 2022, 12, 15881. [Google Scholar] [CrossRef]
- Donker-Cools, B.H.P.M.; Daams, J.G.; Wind, H.; Frings-Dresen, M.H.W. Effective return-to-work interventions after acquired brain injury: A systematic review. Brain Inj. 2016, 30, 113–131. [Google Scholar] [CrossRef]
- Hart, T.; Ketchum, J.M.; O’Neil-Pirozzi, T.M.; Novack, T.A.; Johnson-Greene, D.; Dams-O’Connor, K. Neurocognitive status and return to work after moderate to severe traumatic brain injury. Rehabil. Psychol. 2019, 64, 435–444. [Google Scholar] [CrossRef]
- Libeson, L.; Downing, M.; Ross, P.; Ponsford, J. The experience of return to work in individuals with traumatic brain injury (TBI): A qualitative study. Neuropsychol. Rehabil. 2020, 30, 412–429. [Google Scholar] [CrossRef]
- Aliaga, A.; Bracho, M.J.; Romero, M.; Saldías, M.J.; Jofré, X.; Salas, C. The contribution of executive functions to the process of return to work after brain injury: A systematic review. Neuropsychol. Rehabil. 2023; 1–30, online ahead of print. [Google Scholar] [CrossRef]
- Tombu, M.; Jolicœur, P. A central capacity sharing model of dual-task performance. J. Exp. Psychol. Hum. Percept. Perform. 2003, 29, 3–18. [Google Scholar] [CrossRef]
- Buckley, R.; Helton, W.S.; Innes, C.R.S.; Dalrymple-Alford, J.C.; Jones, R.D. Attention lapses and behavioral microsleeps during tracking, psychomotor vigilance, and dual tasks. Conscious. Cogn. 2016, 45, 174–183. [Google Scholar] [CrossRef]
- Dockree, P.; Tarleton, Y.; Carton, S.; FitzGerald, M. Connecting Self-Awareness and error-awareness in patients with traumatic brain injury. J. Int. Neuropsychol. Soc. 2015, 21, 473–482. [Google Scholar] [CrossRef]
- Huygelier, H.; Schraepen, B.; Lafosse, C.; Vaes, N.; Schillebeeckx, F.; Michiels, K.; Note, E.; Abeele, V.V.; van Ee, R.; Gillebert, C.R. An immersive virtual reality game to train spatial attention orientation after stroke: A feasibility study. Appl. Neuropsychol. Adult 2020, 29, 915–935. [Google Scholar] [CrossRef] [PubMed]
- Doebel, S. Rethinking executive function and its development. Perspect. Psychol. Sci. 2020, 15, 942–956. [Google Scholar] [CrossRef] [PubMed]
- Besnard, J.; Richard, P.; Banville, F.; Nolin, P.; Aubin, G.; Le Gall, D.; Richard, I.; Allain, P. Virtual reality and neuropsychological assessment: The reliability of a virtual kitchen to assess daily-life activities in victims of traumatic brain injury. Appl. Neuropsychol. Adult 2016, 23, 223–235. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TBI | Control | ||||||
|---|---|---|---|---|---|---|---|
| (n = 20) | (n = 20) | ||||||
| Variable | M | SD | M | SD | t | df | p |
| Age (years) | 42.20 | 1.90 | 42.40 | 14.90 | −0.053 | 38 | 0.958 |
| Education (years) | 13.50 | 4.47 | 14.90 | 4.13 | −1.03 | 38 | 0.310 |
| Time since injury (years) | 11.50 | 7.25 | - | - | |||
| Days of hospitalization (days) | 99.60 | 95.77 |
| TBI | Control | ||||||
|---|---|---|---|---|---|---|---|
| (n = 20) | (n = 20) | ||||||
| CBAAD Subtests | M | SD | M | SD | t | df | p |
| Supermarket-selective attention subtest | |||||||
| Corrects | 67.90 | 19.11 | 79.30 | 9.10 | −2.41 | 27.19 | 0.023 |
| Errors | 8.00 | 8.35 | 3.45 | 7.58 | 1.81 | 38.00 | 0.079 |
| Omissions | 9.05 | 12.15 | 2.25 | 3.04 | 2.41 | 21.37 | 0.024 |
| Total duration (sec) | 503.51 | 334.66 | 267.31 | 99.58 | 3.03 | 22.34 | 0.006 |
| Mean level duration (sec) | 83.92 | 55.78 | 44.55 | 16.60 | 3.03 | 22.34 | 0.006 |
| Median level duration (sec) | 78.14 | 52.58 | 43.02 | 16.02 | 2.86 | 22.50 | 0.009 |
| SD level duration (sec) | 28.10 | 32.87 | 11.08 | 7.09 | 2.26 | 20.76 | 0.034 |
| Car driving-sustained attention subtest | |||||||
| Corrects | 4.85 | 1.23 | 5.70 | 1.34 | −2.09 | 38.00 | 0.430 |
| Errors | 0.65 | 0.67 | 0.00 | 0.000 | 4.33 | 19.00 | 0.000 |
| Omissions | 0.50 | 0.61 | 0.00 | 0.000 | 3.68 | 19.00 | 0.002 |
| Mean RT (msec) | 855.24 | 300.37 | 602.27 | 182.70 | 3.216 | 31.37 | 0.003 |
| Median RT (msec) | 776.35 | 319.04 | 534.70 | 153.81 | 3.051 | 27.38 | 0.005 |
| SD RT (msec) | 0.27 | 0.20 | 0.21 | 0.15 | 1.128 | 38.00 | 0.266 |
| Car driving while listening to music-divided attention subtest | |||||||
| Audio corrects | 6.50 | 1.638 | 8.55 | 5.10 | −5.34 | 38.00 | 0.000 |
| Audio errors | 1.00 | 1.214 | 0.30 | 0.47 | 2.41 | 24.58 | 0.024 |
| Audio omissions | 1.40 | 1.00 | 0.15 | 0.37 | 5.47 | 24.02 | 0.000 |
| Audio mean RT (msec) | 3685.90 | 2323.45 | 1747.65 | 1028.99 | 3.41 | 26.18 | 0.002 |
| Audio median RT (msec) | 2615.58 | 2237.11 | 1324.70 | 723.45 | 2.46 | 22.18 | 0.002 |
| Audio SD RT (msec) | 3.23 | 3.38 | 1.27 | 1.37 | 2.40 | 25.07 | 0.024 |
| Visual corrects | 11.65 | 2.72 | 14.25 | 1.02 | −4.00 | 24.24 | 0.001 |
| Visual errors | 0.95 | 1.00 | 0.35 | 0.59 | 2.32 | 30.73 | 0.027 |
| Visual omissions | 2.35 | 2.52 | 0.35 | 0.93 | 3.33 | 24.12 | 0.003 |
| Visual mean RT (msec) | 790.40 | 211.53 | 588.88 | 123.46 | 3.68 | 30.60 | 0.001 |
| Visual median RT (msec) | 746.53 | 228.79 | 568.05 | 126.31 | 3.05 | 29.60 | 0.005 |
| Visual SD RT (msec) | 0.21 | 0.10 | 0.13 | 0.06 | 3.07 | 38.00 | 0.004 |
| Sports watching-switching attention subtest | |||||||
| Corrects | 25.15 | 3.63 | 29.20 | 0.89 | −4.84 | 21.30 | 0.000 |
| Errors | 2.80 | 2.35 | 0.55 | 0.76 | 4.07 | 22.91 | 0.000 |
| False alarms | 1.35 | 1.76 | 0.25 | 0.55 | 2.67 | 22.70 | 0.014 |
| Omissions | 0.75 | 1.59 | 0.00 | 0.00 | 2.12 | 19.00 | 0.048 |
| Mean RT (msec) | 1686.46 | 2339.39 | 1668.35 | 2297.61 | 0.03 | 38.00 | 0.980 |
| Median RT (msec) | 1592.75 | 2337.90 | 1071.43 | 18.79 | 1.00 | 19.00 | 0.331 |
| SD RT (msec) | 0.28 | 0.02 | 0.27 | 0.01 | 2.06 | 21.52 | 0.052 |
| CBAAD | ||||||||||||
| Supermarket-selective attention subtest | Car driving-sustained attention subtest | |||||||||||
| ARCES | COR | ERR | OM | MTD | MdLD | SDLD | COR | ERR | OM | MRT | MdRT | SDRT |
| Errors of attention distraction | −0.570 * | - | 0.584 * | - | 0.448 * | - | - | - | - | 0.477 * | 0.464 * | - |
| Errors of automated action | −0.466 * | 0.487 * | - | 0.521 * | 0.457 * | 0.477 * | - | - | - | 0.446 * | - | - |
| Total errors | −0.625 * | 0.557 * | 0.587 ** | 0.584 * | 0.557 * | - | - | - | - | 0.564 * | 0.548 * | - |
| CBAAD | ||||||||||||
| Car driving while listening to music-divided attention subtest | ||||||||||||
| Audio | Visual | |||||||||||
| ARCES | COR | ERR | OM | MRT | MdRT | SDRT | COR | ERR | OM | MRT | MdRT | SDRT |
| Errors of attention distraction | −0.520 * | - | 0.447 * | 0.565 * | 0.556 * | 0.456 * | −0.565 * | - | 0.657 * | 0.621 * | 0.606 * | - |
| Errors of automated action | - | - | - | - | - | - | - | - | - | - | - | - |
| Total errors | - | - | - | 0.580 * | 0.458 * | - | −0.502 * | - | 0.552 * | 0.593 * | 0.551 * | - |
| ARCES Scores (Dependent Variables) | CBAAD Subtests (Independent Variables) | Beta | t | p | R2 | F | df | p |
|---|---|---|---|---|---|---|---|---|
| ARCES errors of attention distraction | Supermarket-selective attention subtest | |||||||
| Omissions | 0.584 | 3.053 | 0.007 | 0.341 | 9.322 | 1.18 | 0.007 | |
| Car driving-sustained attention subtest | ||||||||
| Mean RT (msec) | 0.477 | 2.301 | 0.034 | 0.227 | 5.293 | 1.18 | 0.034 | |
| Car driving while listening to music-divided attention subtest | ||||||||
| Visual correct responses | −0.639 | −4.873 | 0.000 | 0.736 | 23.724 | 2.17 | 0.000 | |
| Visual mean RT (msec) | 0.408 | 3.113 | 0.006 | |||||
| Sports watching-switching attention subtest | ||||||||
| False alarms | 0.501 | 2.459 | 0.024 | 0.251 | 6.048 | 1.18 | 0.024 | |
| ARCES errors of automated action | Supermarket:-selective attention subtest | |||||||
| Mean total duration (sec) | 0.521 | 2.586 | 0.019 | 0.271 | 6.690 | 1.18 | 0.019 | |
| Car driving-sustained attention subtest | ||||||||
| Mean RT (msec) | 0.446 | 2.113 | 0.049 | 0.199 | 4.466 | 1.18 | 0.049 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malegiannaki, A.-C.; Garefalaki, E.; Pellas, N.; Kosmidis, M.H. Virtual Reality Assessment of Attention Deficits in Traumatic Brain Injury: Effectiveness and Ecological Validity. Multimodal Technol. Interact. 2024, 8, 3. https://doi.org/10.3390/mti8010003
Malegiannaki A-C, Garefalaki E, Pellas N, Kosmidis MH. Virtual Reality Assessment of Attention Deficits in Traumatic Brain Injury: Effectiveness and Ecological Validity. Multimodal Technologies and Interaction. 2024; 8(1):3. https://doi.org/10.3390/mti8010003
Chicago/Turabian StyleMalegiannaki, Amaryllis-Chryssi, Evangelia Garefalaki, Nikolaos Pellas, and Mary H. Kosmidis. 2024. "Virtual Reality Assessment of Attention Deficits in Traumatic Brain Injury: Effectiveness and Ecological Validity" Multimodal Technologies and Interaction 8, no. 1: 3. https://doi.org/10.3390/mti8010003
APA StyleMalegiannaki, A. -C., Garefalaki, E., Pellas, N., & Kosmidis, M. H. (2024). Virtual Reality Assessment of Attention Deficits in Traumatic Brain Injury: Effectiveness and Ecological Validity. Multimodal Technologies and Interaction, 8(1), 3. https://doi.org/10.3390/mti8010003