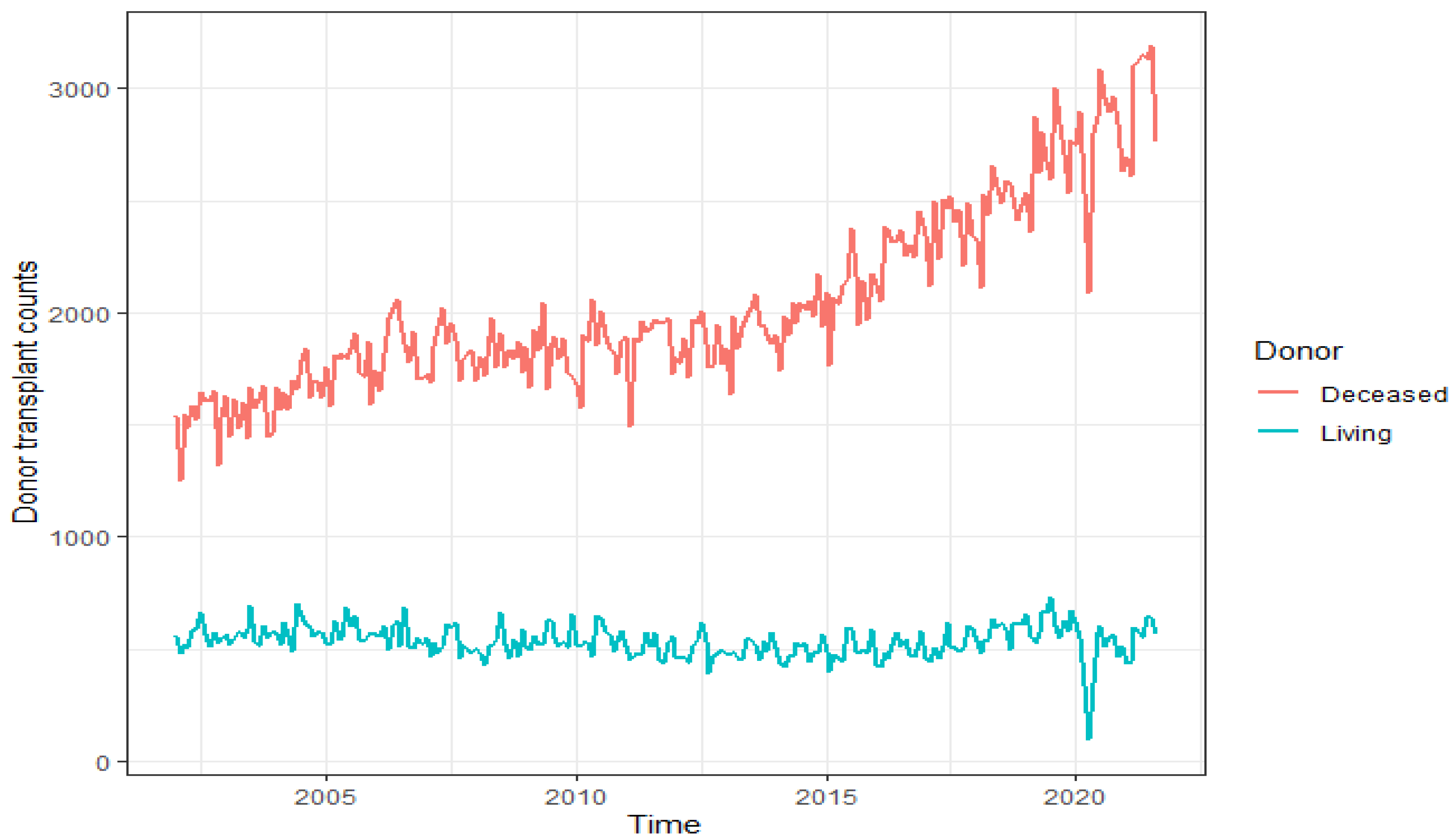
Figure 1.
Donor transplant counts in the US by donor type, based on OPTN data as of November 2021.
Figure 1.
Donor transplant counts in the US by donor type, based on OPTN data as of November 2021.
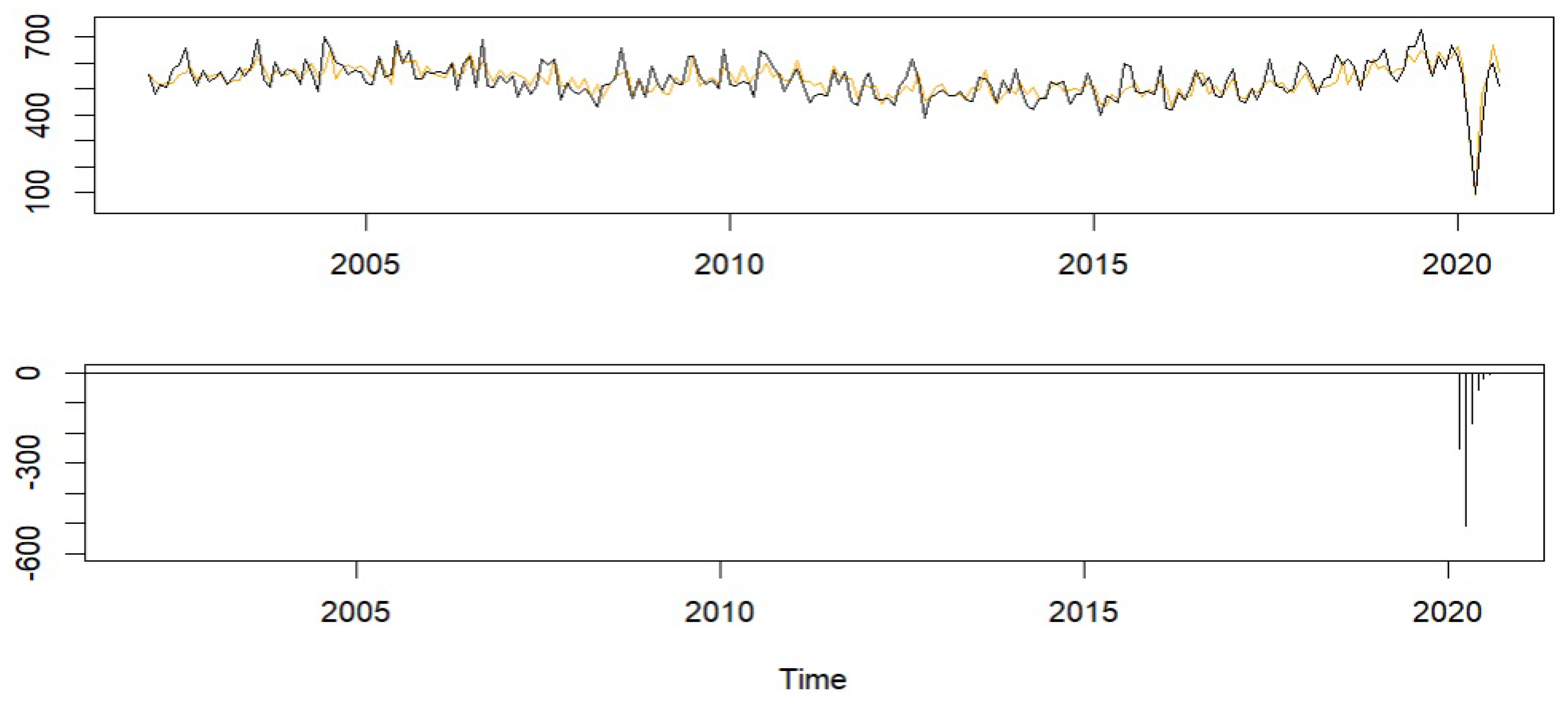
Figure 2.
Living donor transplant counts with the model fit (top) and the estimated COVID-19 effects (bottom).
Figure 2.
Living donor transplant counts with the model fit (top) and the estimated COVID-19 effects (bottom).
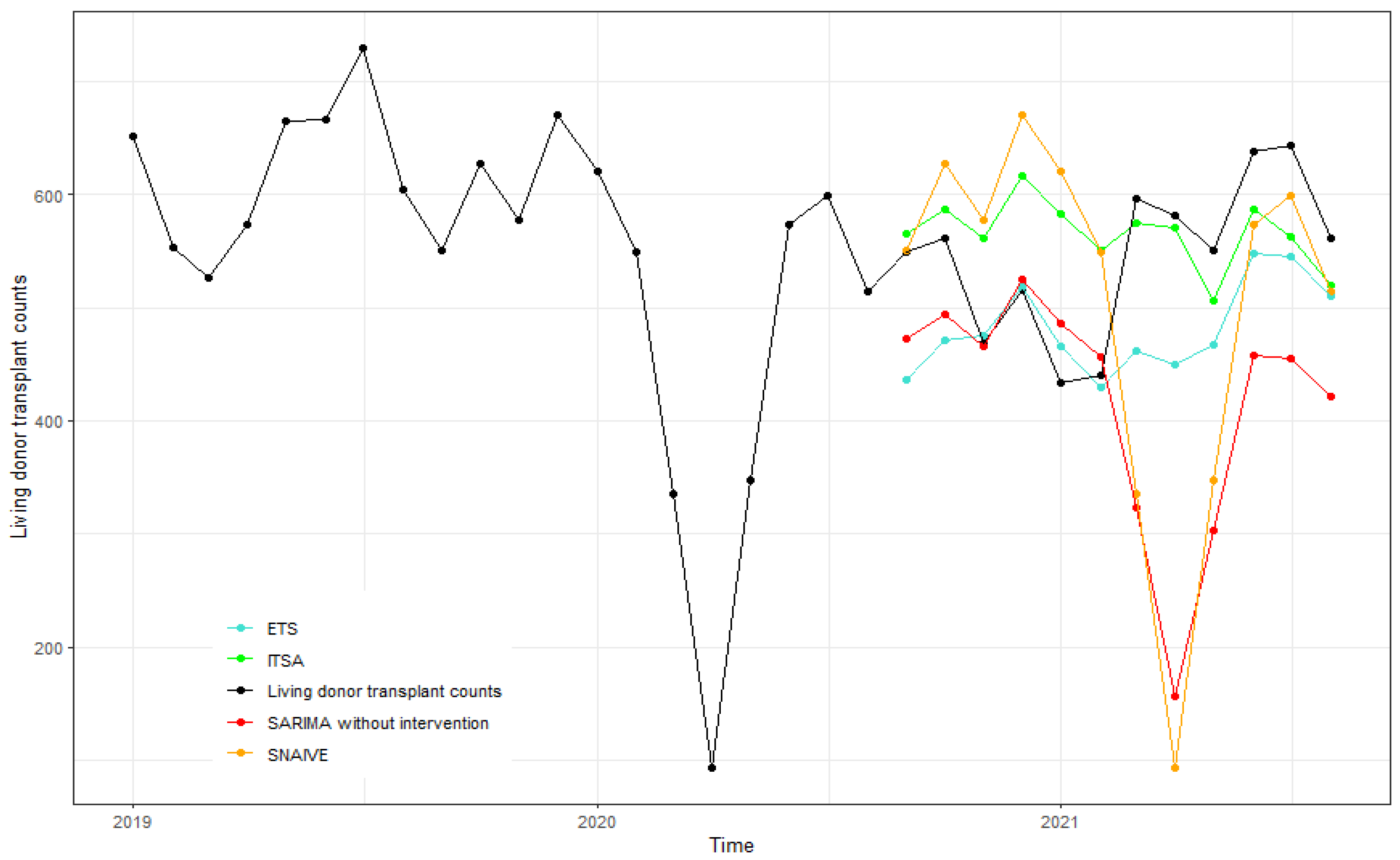
Figure 3.
Forecasts of living donor transplant counts from September 2020 to August 2021 using ITSA, SARIMA without intervention, ETS, and SNAIVE.
Figure 3.
Forecasts of living donor transplant counts from September 2020 to August 2021 using ITSA, SARIMA without intervention, ETS, and SNAIVE.
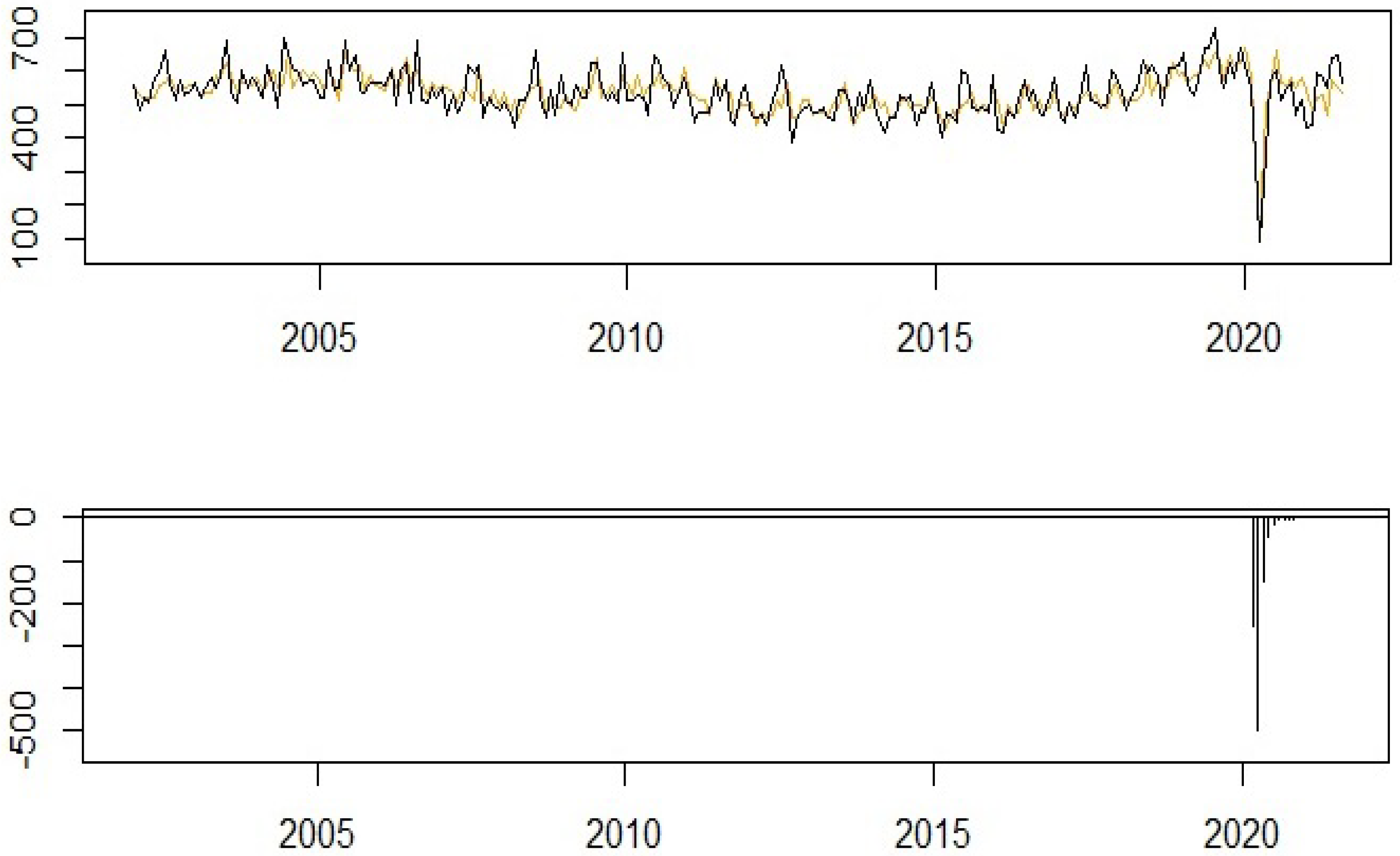
Figure 4.
Living donor transplant counts (January 2002 to August 2021) with the model fit (top) and the estimated COVID-19 effects (bottom).
Figure 4.
Living donor transplant counts (January 2002 to August 2021) with the model fit (top) and the estimated COVID-19 effects (bottom).
Figure 5.
Forecasts of living donors from September 2021 to March 2022.
Figure 5.
Forecasts of living donors from September 2021 to March 2022.
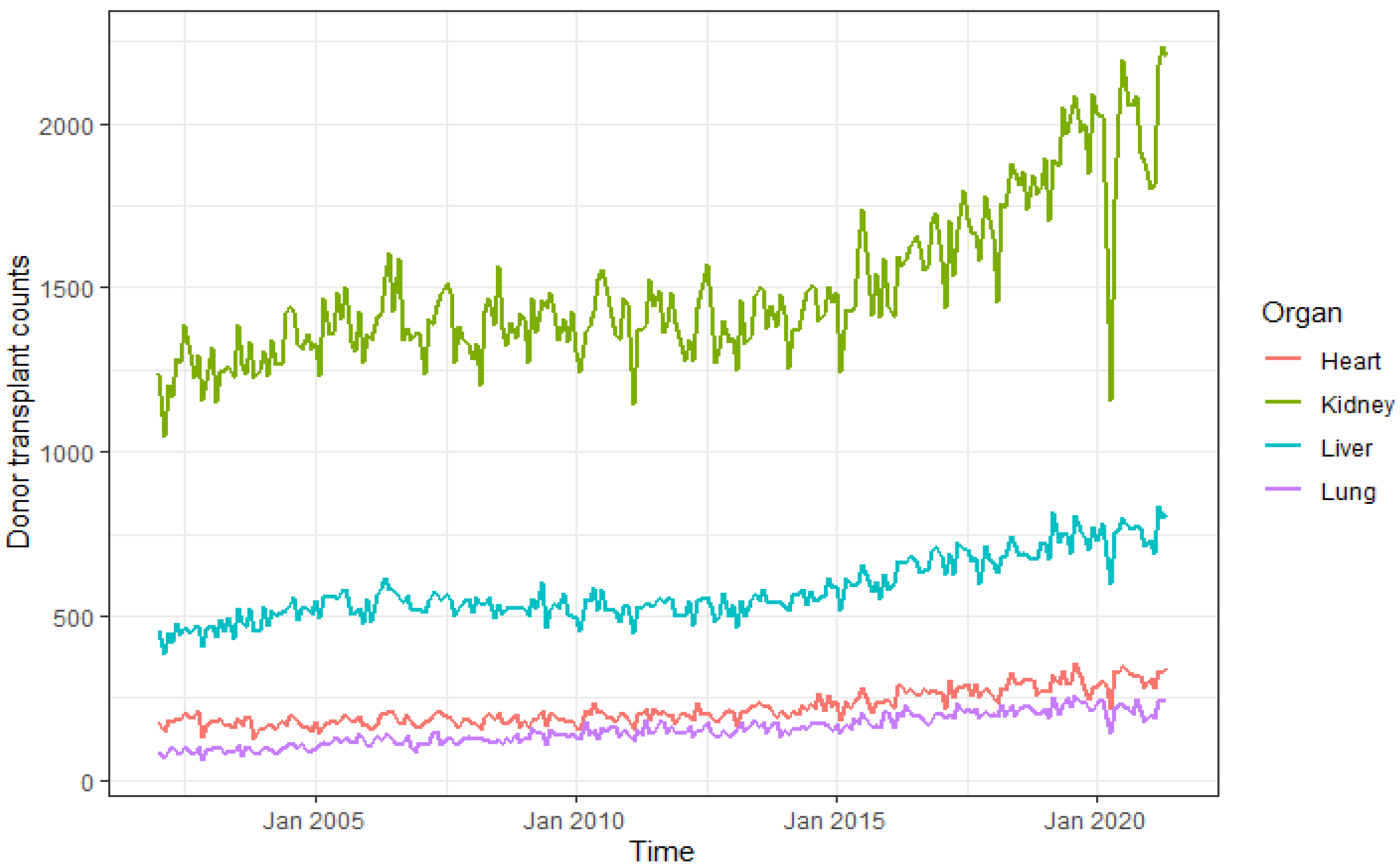
Figure 6.
Donor transplant counts in the US by organ, based on OPTN data as of November 2021.
Figure 6.
Donor transplant counts in the US by organ, based on OPTN data as of November 2021.
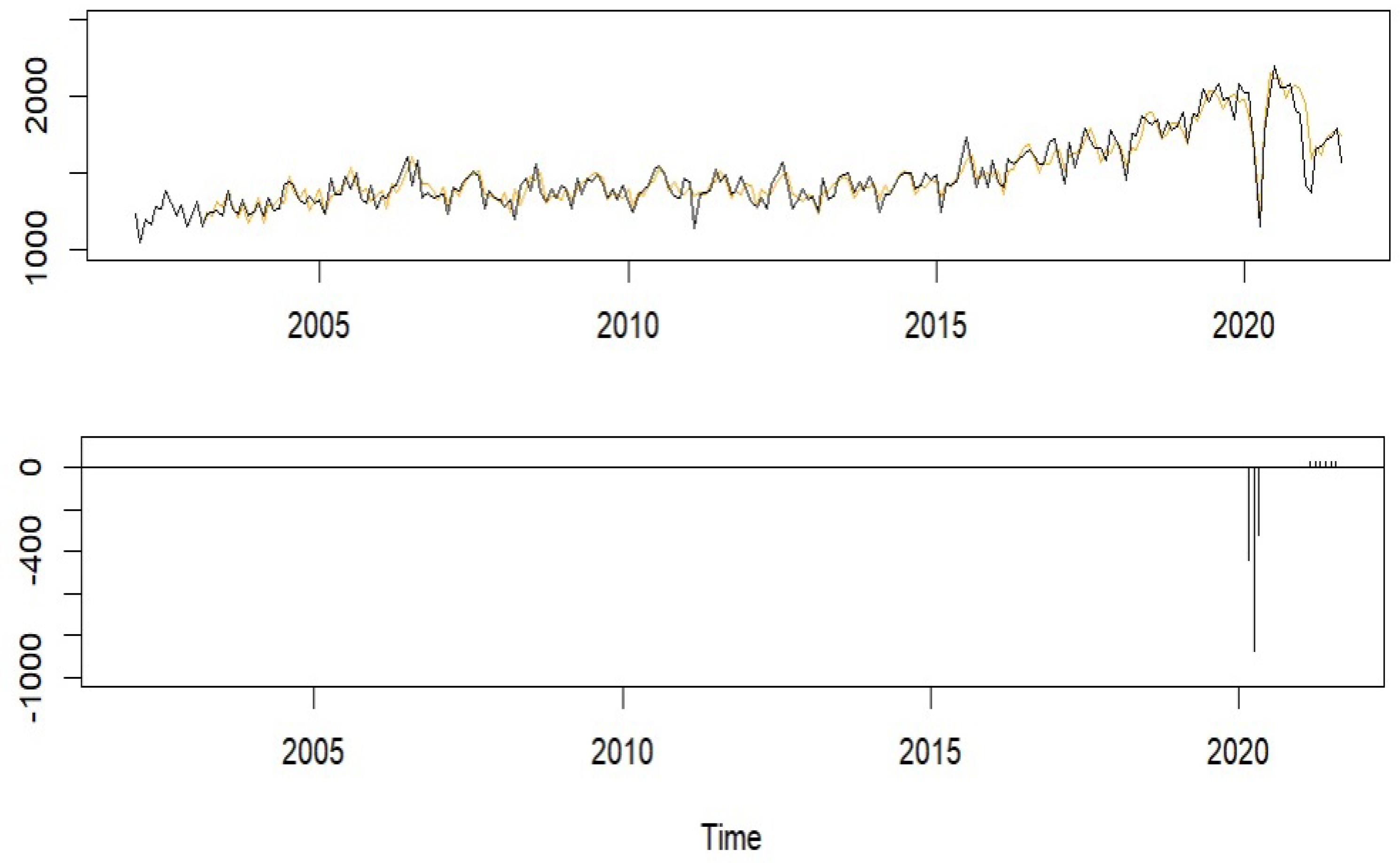
Figure 7.
Kidney donor transplant counts with the model fit (top) and the estimated COVID-19 effects (bottom).
Figure 7.
Kidney donor transplant counts with the model fit (top) and the estimated COVID-19 effects (bottom).
Figure 8.
Forecasts of kidney donor transplant counts from September 2021 to April 2022 using ITSA, SARIMA without intervention, ETS, and SNAIVE.
Figure 8.
Forecasts of kidney donor transplant counts from September 2021 to April 2022 using ITSA, SARIMA without intervention, ETS, and SNAIVE.
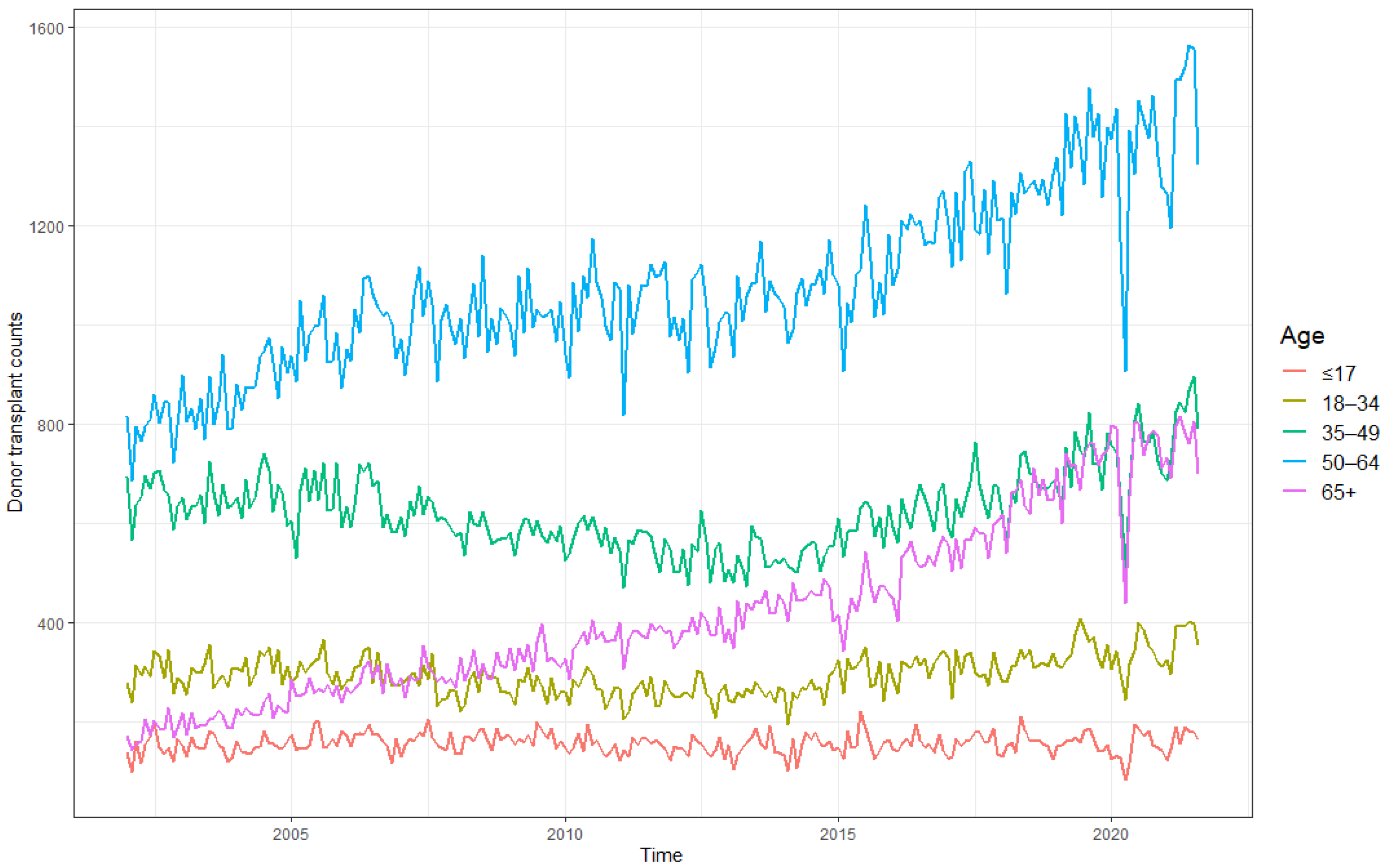
Figure 9.
All donor transplant counts in the US across different age groups, based on OPTN data as of November 2021.
Figure 9.
All donor transplant counts in the US across different age groups, based on OPTN data as of November 2021.
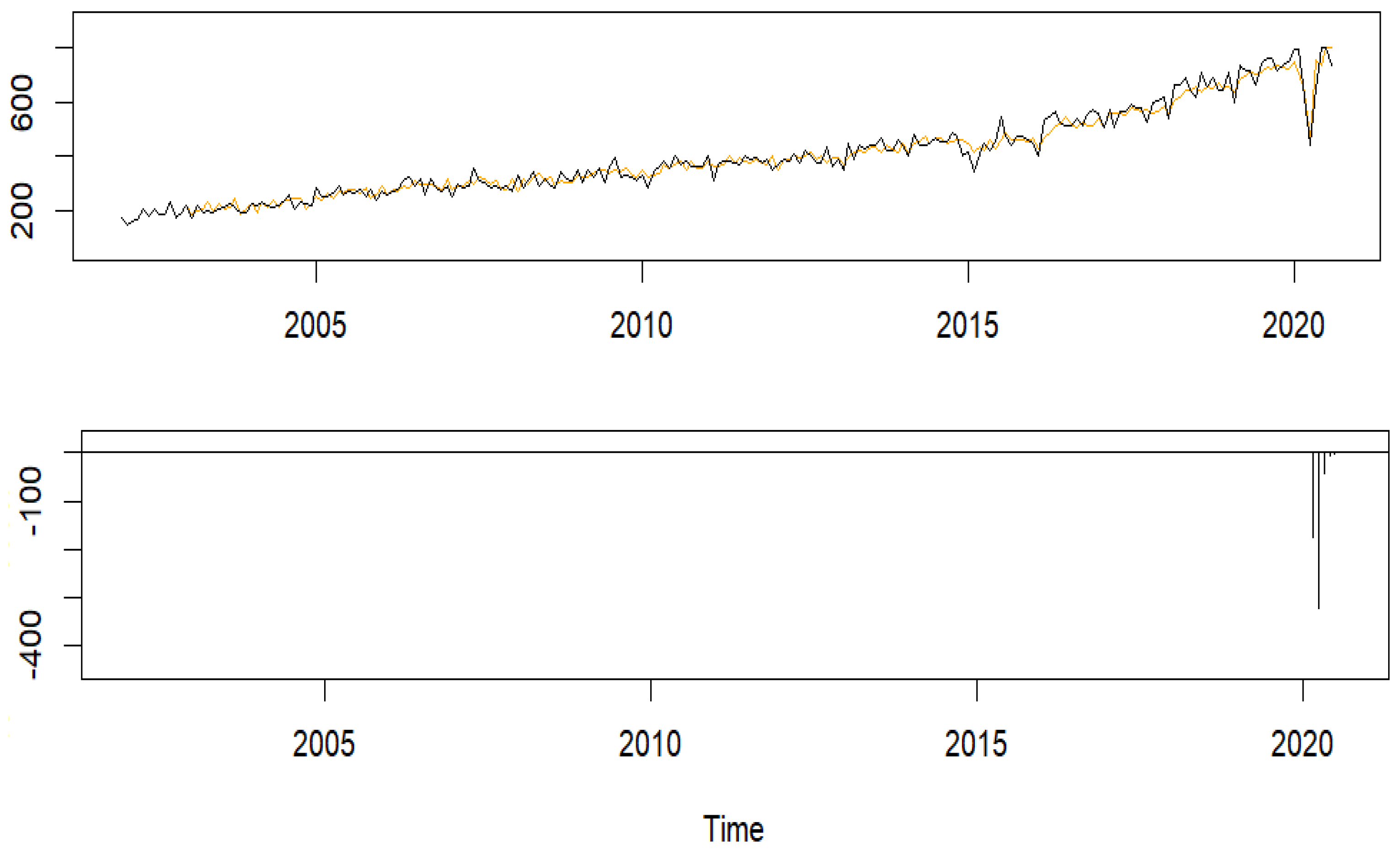
Figure 10.
Donor transplant counts for the 65+-year-old group with the model fit (top) and the estimated COVID-19 effects (bottom).
Figure 10.
Donor transplant counts for the 65+-year-old group with the model fit (top) and the estimated COVID-19 effects (bottom).
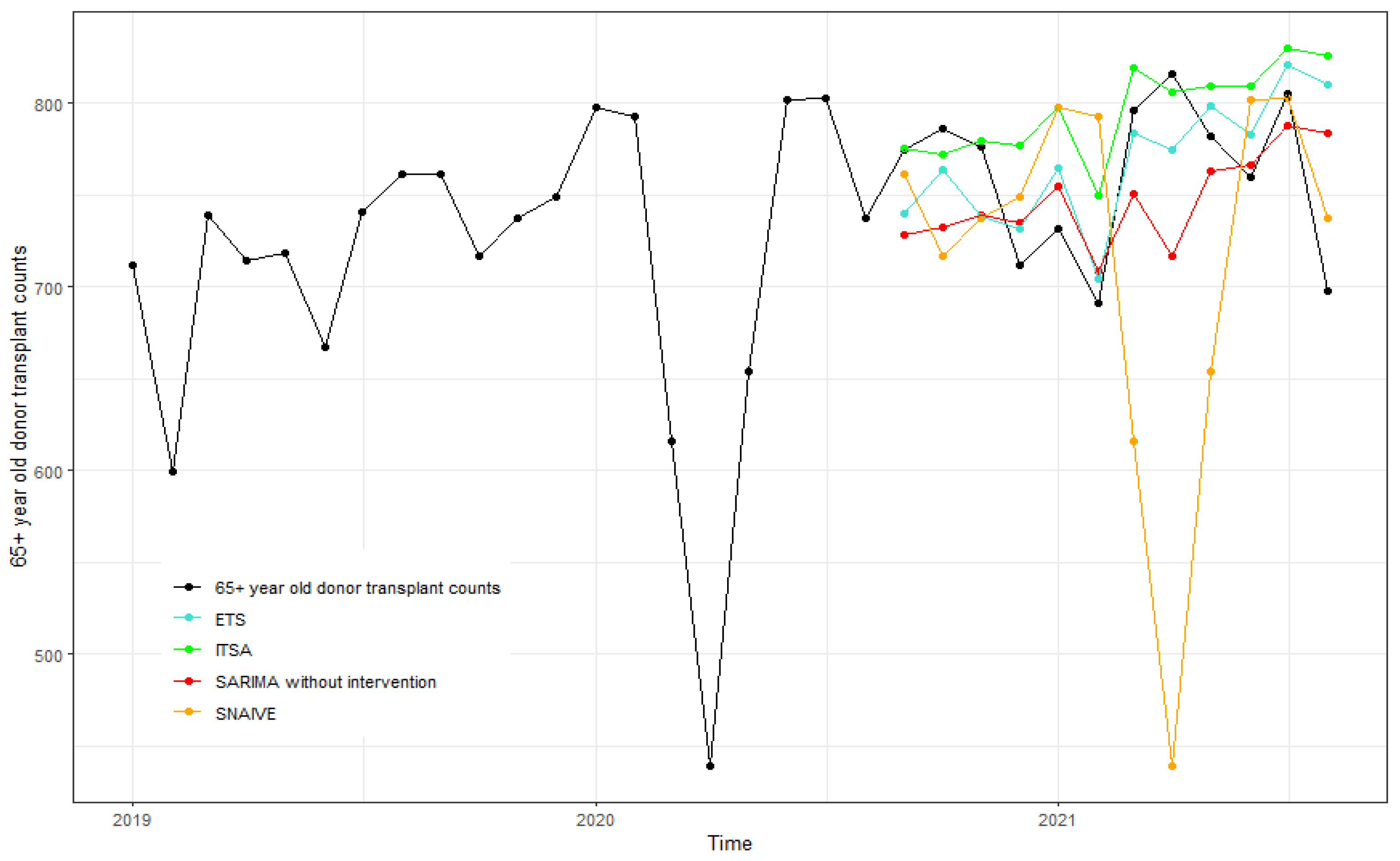
Figure 11.
Forecasts of all donor transplant counts for the 65+-year-old from September 2020 to August 2021 using ITSA, SARIMA without intervention, ETS, and SNAIVE.
Figure 11.
Forecasts of all donor transplant counts for the 65+-year-old from September 2020 to August 2021 using ITSA, SARIMA without intervention, ETS, and SNAIVE.
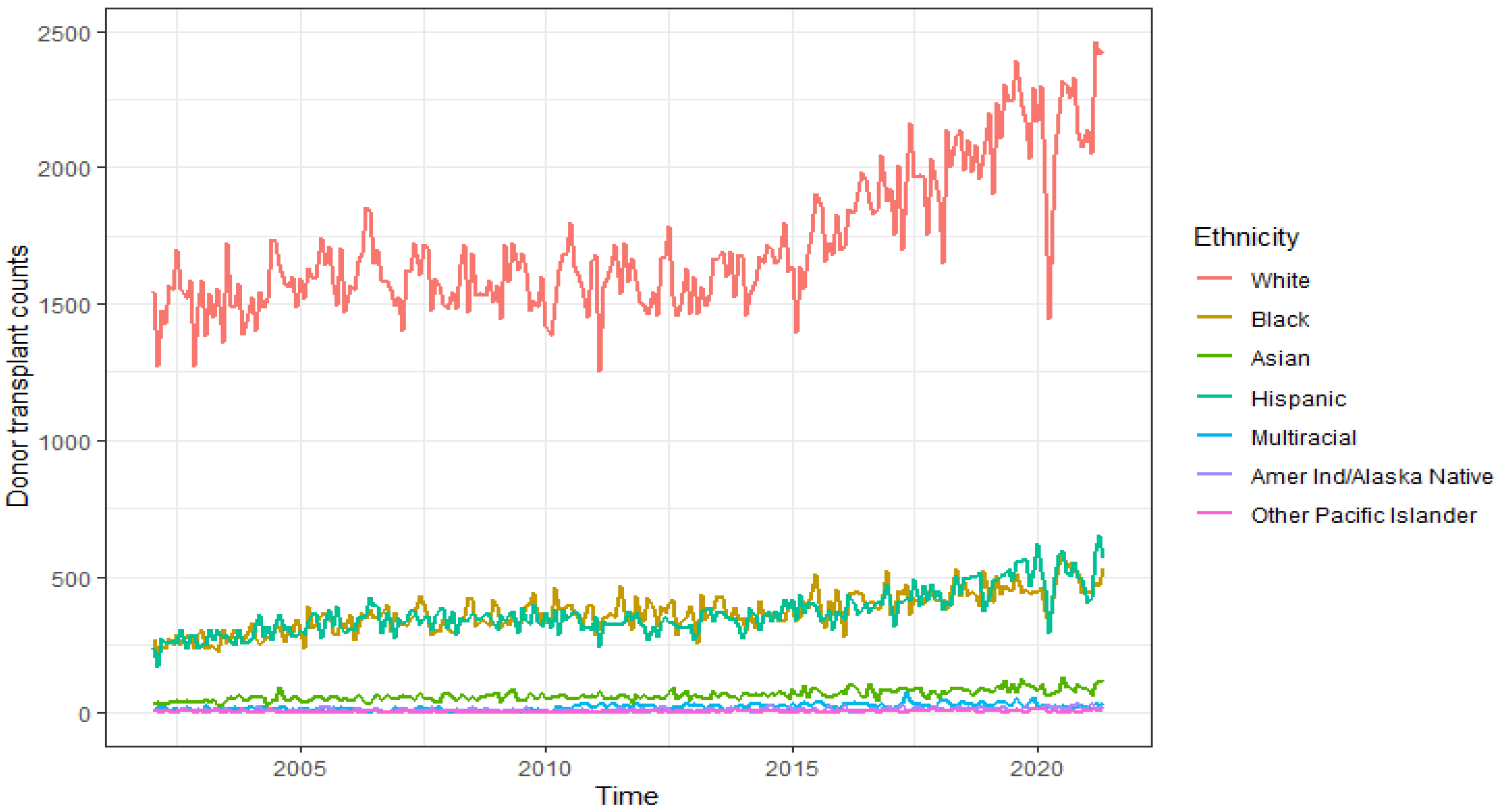
Figure 12.
Donor transplant counts in the US across ethnicity, based on OPTN data as of November 2021.
Figure 12.
Donor transplant counts in the US across ethnicity, based on OPTN data as of November 2021.
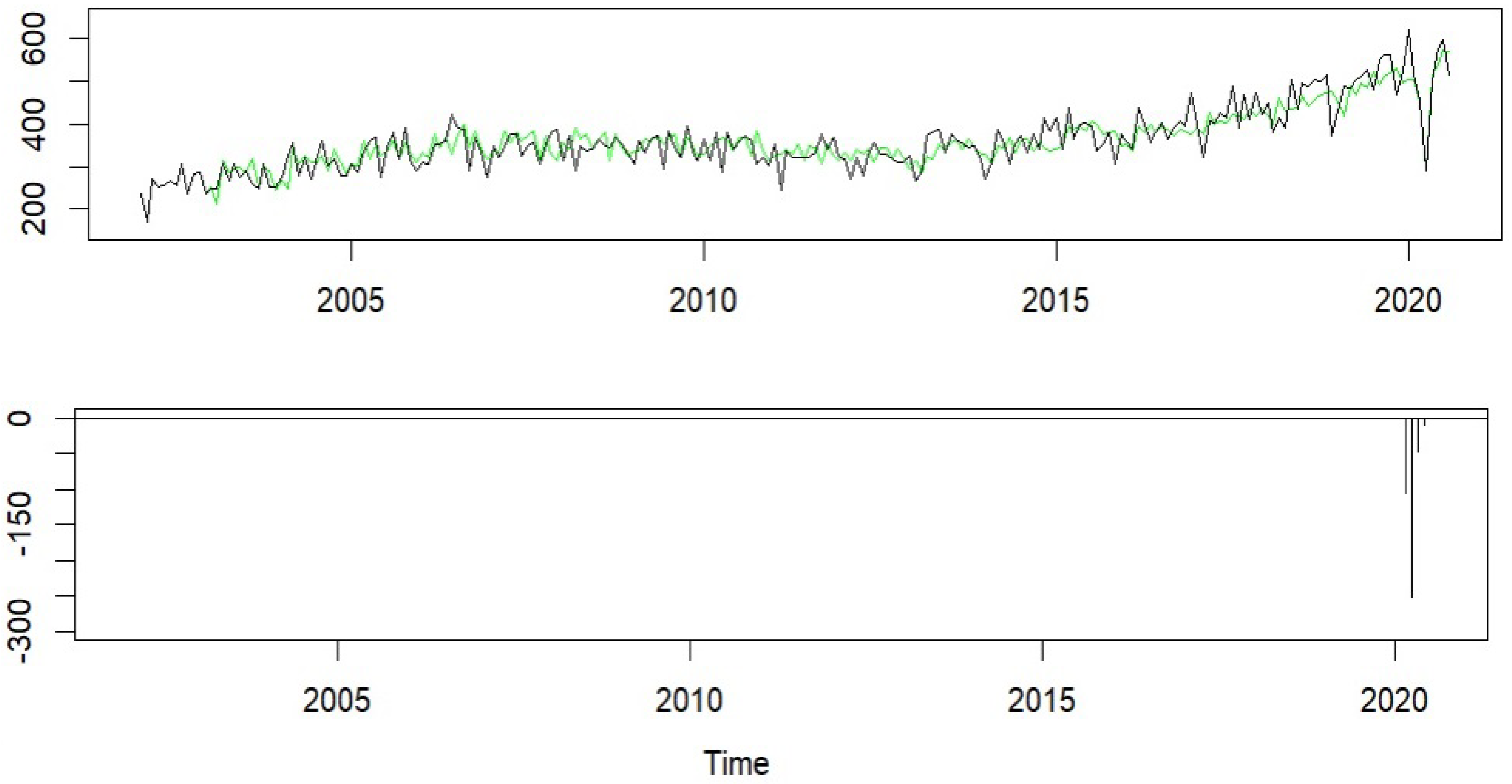
Figure 13.
Hispanic donor transplant counts with the model fit (top) and the estimated COVID-19 effects (bottom).
Figure 13.
Hispanic donor transplant counts with the model fit (top) and the estimated COVID-19 effects (bottom).
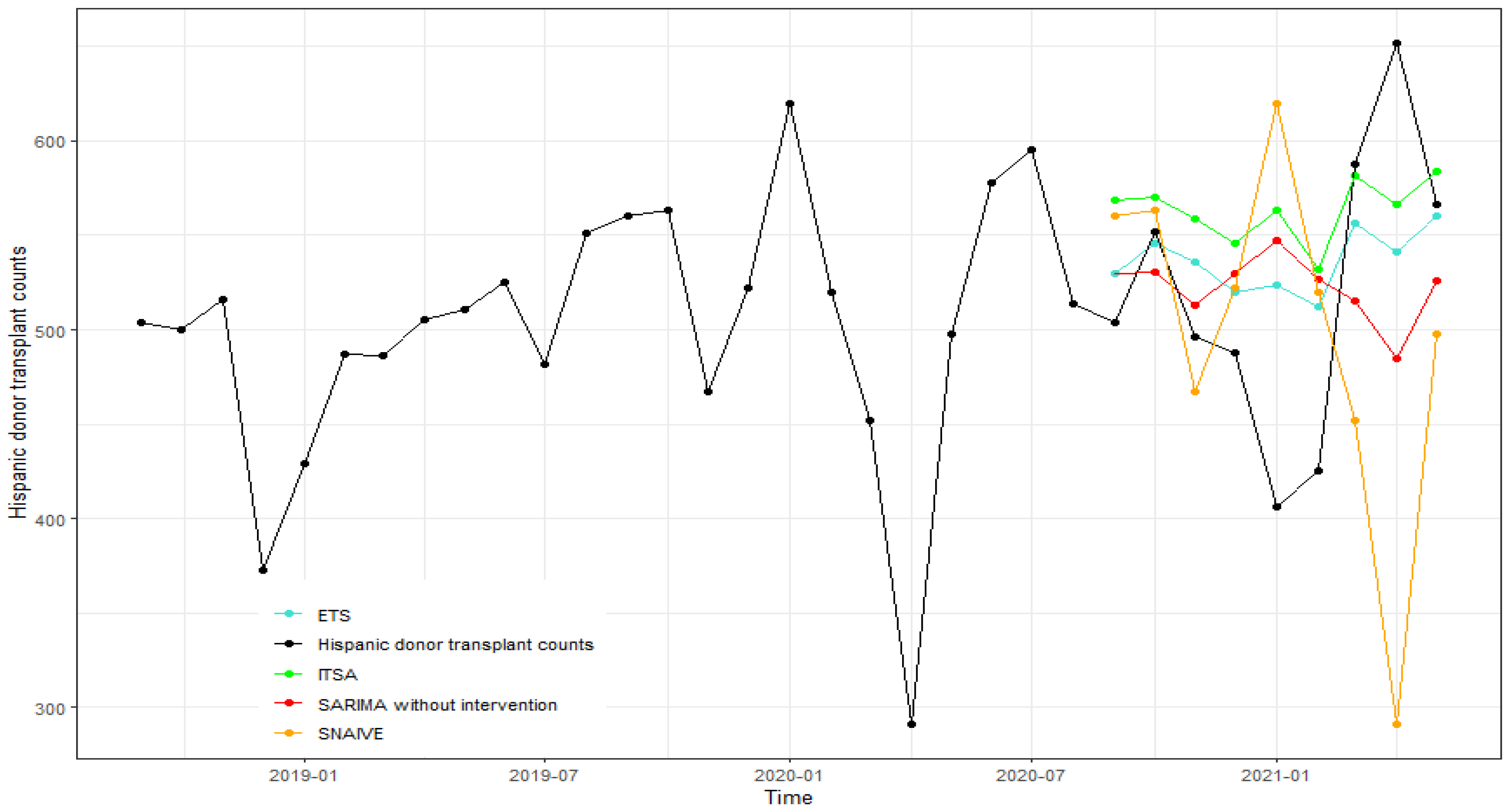
Figure 14.
Forecasts of the Hispanic donor transplants from September 2020 to May 2021 using ITSA, SARIMA without intervention, ETS, and SNAIVE.
Figure 14.
Forecasts of the Hispanic donor transplants from September 2020 to May 2021 using ITSA, SARIMA without intervention, ETS, and SNAIVE.
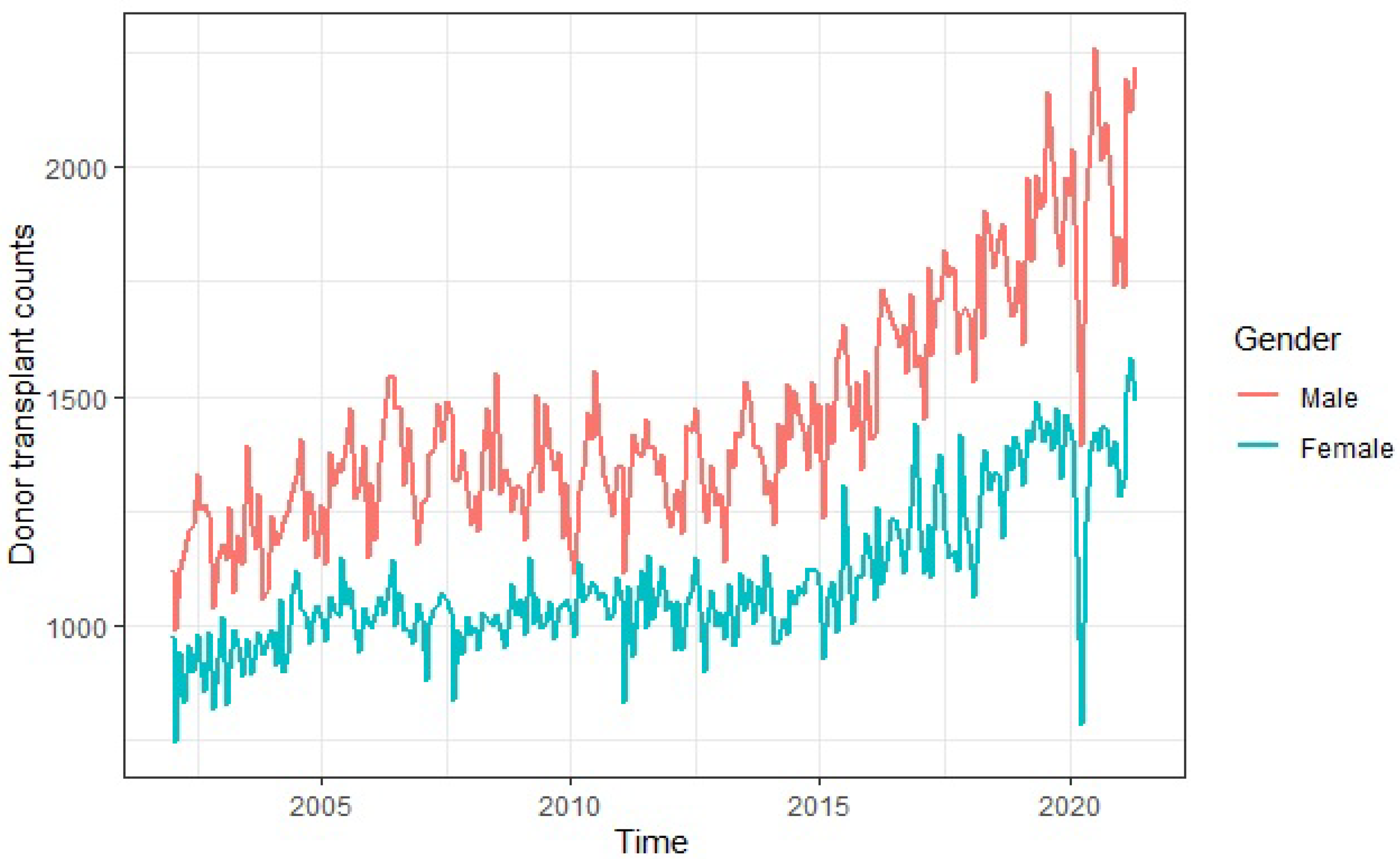
Figure 15.
Donor transplant counts in the US across gender, based on OPTN data as of November 2021.
Figure 15.
Donor transplant counts in the US across gender, based on OPTN data as of November 2021.
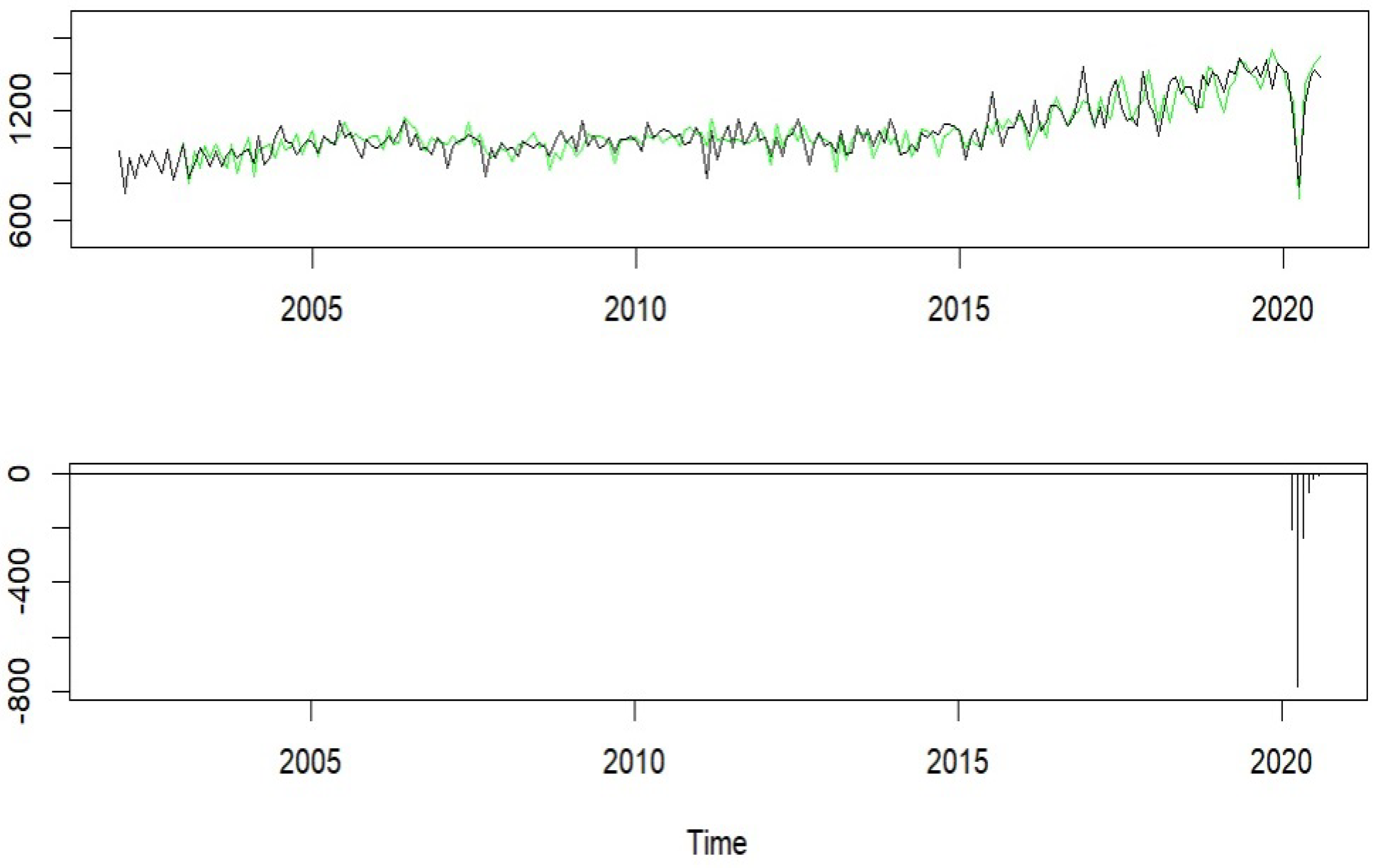
Figure 16.
Female donor transplant counts with the model fit (top) and the estimated COVID-19 effects (bottom).
Figure 16.
Female donor transplant counts with the model fit (top) and the estimated COVID-19 effects (bottom).
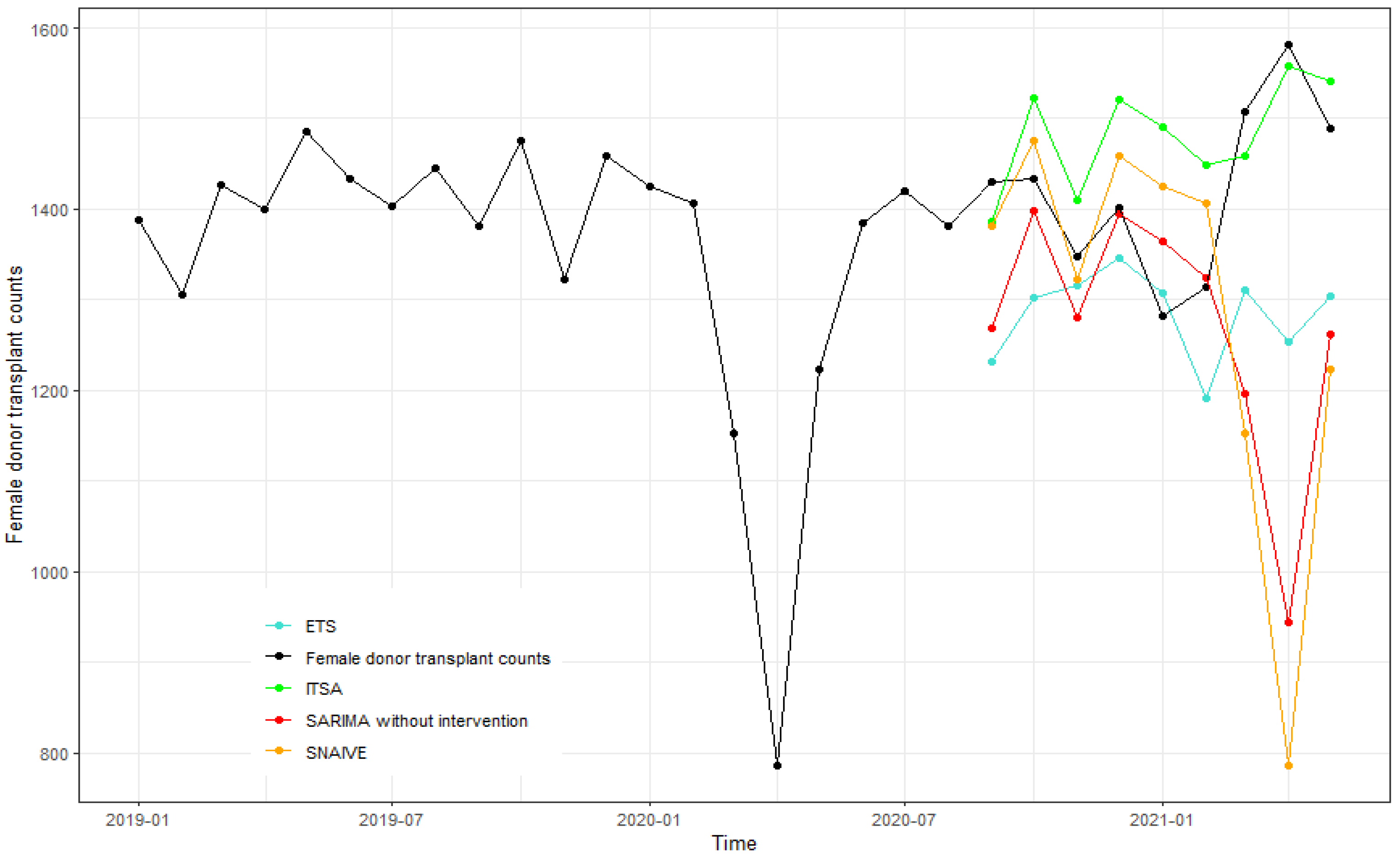
Figure 17.
Forecasts of female donor transplants from September 2020 to May 2021 using ITSA, SARIMA without intervention, ETS, and SNAIVE.
Figure 17.
Forecasts of female donor transplants from September 2020 to May 2021 using ITSA, SARIMA without intervention, ETS, and SNAIVE.
Table 1.
Forecast accuracy measures by donor type at various forecast horizons.
Table 1.
Forecast accuracy measures by donor type at various forecast horizons.
| | h | MAPE (%) | RMSE |
|---|
| | Living | Deceased | Living | Deceased |
|---|
| ITSA | 1 | 12.16 | 5.46 | 72.78 | 191.79 |
| 2 | 16.76 | 6.08 | 93.09 | 210.46 |
| 4 | 18.95 | 7.64 | 104.88 | 232.60 |
| 8 | 9.58 | 3.97 | 65.78 | 183.95 |
| SARIMA | 1 | 13.49 | 6.27 | 113.19 | 235.95 |
| 2 | 21.53 | 7.45 | 171.14 | 262.09 |
| 4 | 26.73 | 8.22 | 195.57 | 274.17 |
| 8 | 37.20 | 8.08 | 244.44 | 303.53 |
| ETS | 1 | 10.28 | 4.94 | 68.39 | 178.38 |
| 2 | 10.57 | 6.09 | 69.86 | 204.10 |
| 4 | 10.48 | 6.60 | 71.19 | 217.95 |
| 8 | 11.45 | 7.39 | 76.62 | 240.55 |
| SNAIVE | 1 | 26.94 | 10.06 | 192.28 | 398.95 |
| 2 | 29.35 | 10.81 | 200.83 | 416.41 |
| 4 | 32.01 | 11.03 | 217.98 | 440.09 |
| 8 | 29.25 | 12.63 | 240.27 | 513.26 |
Table 2.
Results of the modified Diebold–Mariano test comparing ITSA to ETS, SARIMA without intervention, and SNAIVE by donor type.
Table 2.
Results of the modified Diebold–Mariano test comparing ITSA to ETS, SARIMA without intervention, and SNAIVE by donor type.
| Donor Type | h | ETS | SARIMA | SNAIVE |
|---|
| Living | 1 | 0.32 | −1.11 | −1.66 |
| | 4 | 3.52 | −1.47 | −2.25 |
| Deceased | 1 | 0.46 | −1.12 | 1.40 |
| | 4 | 0.14 | −0.86 | −1.19 |
Table 3.
Forecast accuracy measures by organ type at various forecast horizons.
Table 3.
Forecast accuracy measures by organ type at various forecast horizons.
| | h | MAPE (%) | RMSE |
|---|
| | Heart | Liver | Lung | Kidney | Heart | Liver | Lung | Kidney |
|---|
| ITSA | 1 | 3.69 | 5.50 | 11.68 | 9.97 | 13.94 | 55.40 | 27.19 | 181.45 |
| 2 | 3.45 | 6.37 | 12.13 | 9.73 | 13.64 | 64.03 | 28.57 | 178.25 |
| 4 | 3.63 | 7.67 | 14.16 | 11.23 | 14.23 | 79.37 | 31.07 | 182.16 |
| 8 | 3.13 | 9.36 | 7.23 | - | 11.27 | 88.98 | 16.97 | - |
| SARIMA | 1 | 4.64 | 6.11 | 11.73 | 9.46 | 18.06 | 60.76 | 30.39 | 166.30 |
| 2 | 4.92 | 7.28 | 13.03 | 10.28 | 19.03 | 71.05 | 33.79 | 170.12 |
| 4 | 4.94 | 8.79 | 15.33 | 12.37 | 19.50 | 89.14 | 35.92 | 194.96 |
| 8 | 5.36 | 11.77 | 11.92 | - | 23.02 | 110.43 | 31.76 | - |
| ETS | 1 | 4.59 | 5.83 | 8.78 | 9.26 | 16.72 | 57.05 | 24.22 | 165.18 |
| 2 | 5.09 | 6.95 | 10.30 | 9.06 | 18.60 | 67.71 | 26.64 | 164.43 |
| 4 | 5.58 | 8.84 | 10.78 | 11.35 | 21.00 | 91.24 | 26.25 | 180.73 |
| 8 | 6.99 | 13.26 | 9.52 | - | 25.47 | 122.95 | 24.38 | - |
| SNAIVE | 1 | 9.33 | 11.62 | 15.47 | 20.36 | 45.48 | 128.04 | 43.15 | 352.98 |
| 2 | 10.06 | 12.66 | 15.32 | 17.84 | 47.48 | 133.73 | 43.88 | 310.89 |
| 4 | 0.08 | 13.99 | 18.02 | 15.35 | 45.23 | 145.76 | 48.37 | 269.19 |
| 8 | 9.26 | 16.63 | 14.66 | - | 52.95 | 162.84 | 49.30 | - |
Table 4.
Results of the modified Diebold–Mariano test comparing ITSA to ETS, SARIMA without intervention, and SNAIVE by organ type.
Table 4.
Results of the modified Diebold–Mariano test comparing ITSA to ETS, SARIMA without intervention, and SNAIVE by organ type.
| Organ | h | ETS | SARIMA | SNAIVE |
|---|
| Heart | 1 | −0.82 | −1.18 | −1.63 |
| | 4 | −0.83 | −0.79 | −1.47 |
| Liver | 1 | −0.36 | −1.61 | −2.21 |
| | 4 | −1.08 | -1.27 | −2.21 |
| Lung | 1 | 1.04 | −0.94 | −1.38 |
| | 4 | 0.79 | −0.84 | −1.41 |
| Kidney | 1 | 0.88 | 0.90 | −2.17 |
| | 4 | 0.08 | -0.26 | −1.44 |
Table 5.
Forecast accuracy measures by age group at various forecast horizons.
Table 5.
Forecast accuracy measures by age group at various forecast horizons.
| | h | MAPE (%) | RMSE |
|---|
| | 65+ | 50–64 | 35–49 | 18–34 | ≤17 | 65+ | 50–64 | 35–49 | 18–34 | ≤17 |
|---|
| ITSA | 1 | 4.12 | 6.81 | 5.69 | 6.71 | 6.91 | 41.27 | 104.08 | 56.11 | 29.30 | 16.88 |
| 2 | 4.74 | 8.00 | 6.49 | 7.45 | 7.06 | 46.62 | 116.91 | 60.94 | 31.64 | 16.98 |
| 4 | 5.69 | 8.77 | 7.42 | 8.41 | 7.91 | 52.99 | 126.29 | 64.49 | 34.03 | 18.11 |
| 8 | 6.17 | 6.50 | 3.83 | 3.55 | 5.18 | 58.04 | 98.80 | 36.31 | 15.52 | 15.76 |
| SARIMA | 1 | 4.88 | 7.19 | 7.49 | 7.91 | 8.41 | 45.59 | 112.28 | 59.09 | 36.88 | 20.14 |
| 2 | 5.51 | 8.07 | 9.22 | 8.91 | 9.33 | 50.98 | 125.23 | 96.80 | 41.30 | 22.07 |
| 4 | 5.11 | 8.77 | 10.71 | 10.42 | 10.99 | 50.88 | 132.05 | 104.98 | 45.86 | 24.30 |
| 8 | 5.96 | 9.01 | 10.85 | 4.89 | 10.48 | 52.15 | 141.89 | 122.05 | 17.28 | 24.21 |
| ETS | 1 | 5.22 | 6.88 | 6.52 | 6.33 | 8.14 | 45.92 | 109.60 | 56.17 | 28.95 | 18.66 |
| 2 | 5.55 | 8.17 | 7.02 | 7.05 | 7.50 | 49.15 | 128.15 | 63.40 | 32.14 | 16.59 |
| 4 | 4.97 | 8.73 | 7.79 | 8.85 | 8.42 | 46.86 | 138.20 | 73.26 | 37.63 | 18.64 |
| 8 | 5.73 | 9.11 | 9.62 | 8.79 | 6.04 | 54.53 | 146.68 | 89.77 | 39.18 | 14.87 |
| SNAIVE | 1 | 11.76 | 12.22 | 11.68 | 12.85 | 0.07 | 134.41 | 232.17 | 127.27 | 62.29 | 35.69 |
| 2 | 12.66 | 13.34 | 12.22 | 13.53 | 15.35 | 140.32 | 242.49 | 132.27 | 64.80 | 37.07 |
| 4 | 13.94 | 15.34 | 13.18 | 15.61 | 0.07 | 152.87 | 266.35 | 143.51 | 71.32 | 11.61 |
| 8 | 14.78 | 15.58 | 14.85 | 16.29 | 20.42 | 179.89 | 298.91 | 170.29 | 80.71 | 46.56 |
Table 6.
Results of the modified Diebold–Mariano test comparing ITSA to ETS, SARIMA without intervention, and SNAIVE by age group.
Table 6.
Results of the modified Diebold–Mariano test comparing ITSA to ETS, SARIMA without intervention, and SNAIVE by age group.
| Age Group | h | ETS | SARIMA | SNAIVE |
|---|
| 65+ | 1 | −0.67 | −0.78 | −1.40 |
| | 4 | −0.37 | −0.31 | −1.87 |
| 50−64 | 1 | −0.63 | −1.05 | −1.59 |
| | 4 | −0.37 | −0.31 | −1.87 |
| 35−49 | 1 | 0.00 | −1.12 | −1.46 |
| | 4 | −0.26 | −1.73 | −1.79 |
| 18−34 | 1 | 0.07 | −1.04 | −1.70 |
| | 4 | −0.20 | −0.90 | −1.58 |
| ≤17 | 1 | −0.64 | −1.70 | 1.82 |
| | 4 | −0.35 | −2.06 | −2.10 |
Table 7.
Forecast accuracy measures by ethnicity at various forecast horizons.
Table 7.
Forecast accuracy measures by ethnicity at various forecast horizons.
| | h | MAPE (%) | RMSE |
|---|
| | Hispanic | White | African
American | Asian | Hispanic | White | African
American | Asian |
|---|
| ITSA | 1 | 12.05 | 4.86 | 6.82 | 7.02 | 74.91 | 130.51 | 43.53 | 40.39 |
| 2 | 14.11 | 6.02 | 9.33 | 7.34 | 84.40 | 151.80 | 53.46 | 39.54 |
| 4 | 16.41 | 6.47 | 15.24 | 8.51 | 89.45 | 151.35 | 76.45 | 41.60 |
| 8 | 6.96 | 5.19 | 14.05 | 3.07 | 122.36 | 135.65 | 69.42 | 17.23 |
| SARIMA | 1 | 13.69 | 5.08 | 7.73 | 7.64 | 87.82 | 171.76 | 48.80 | 43.04 |
| 2 | 16.01 | 6.50 | 10.20 | 7.35 | 100.48 | 196.25 | 59.48 | 38.34 |
| 4 | 19.56 | 6.72 | 16.18 | 5.54 | 109.03 | 203.83 | 80.63 | 31.65 |
| 8 | 16.69 | 12.21 | 14.87 | 5.37 | 122.36 | 314.61 | 74.62 | 31.27 |
| ETS | 1 | 9.67 | 5.29 | 7.22 | 7.22 | 70.14 | 158.23 | 46.69 | 46.69 |
| 2 | 12.10 | 5.78 | 6.72 | 6.72 | 80.78 | 179.67 | 40.45 | 40.45 |
| 4 | 13.66 | 5.66 | 5.46 | 5.46 | 84.57 | 188.96 | 30.03 | 30.03 |
| 8 | 14.65 | 11.49 | 2.85 | 2.85 | 106.19 | 285.78 | 20.09 | 20.09 |
| SNAIVE | 1 | 21.27 | 12.74 | 12.92 | 12.92 | 154.02 | 413.60 | 79.90 | 79.90 |
| 2 | 22.54 | 14.19 | 12.02 | 12.02 | 162.16 | 438.60 | 75.12 | 75.12 |
| 4 | 28.75 | 17.05 | 11.22 | 11.22 | 186.80 | 500.79 | 75.23 | 75.23 |
| 8 | 33.69 | 27.99 | 20.51 | 20.51 | 259.75 | 738.082 | 106.04 | 106.04 |
Table 8.
Results of the modified Diebold–Mariano test comparing ITSA to ETS, SARIMA without intervention, and SNAIVE by ethnicity.
Table 8.
Results of the modified Diebold–Mariano test comparing ITSA to ETS, SARIMA without intervention, and SNAIVE by ethnicity.
| Ethnicity | h | ETS | SARIMA | SNAIVE |
|---|
| Hispanic | 1 | 0.60 | −1.49 | −1.49 |
| | 4 | 0.18 | −0.88 | −1.07 |
| White | 1 | −1.12 | −1.41 | −1.56 |
| | 4 | -0.46 | -0.56 | -1.26 |
| African American | 1 | −0.29 | −1.26 | −1.58 |
| | 4 | 1.13 | −1.64 | 0.02 |
| Asian | 1 | −0.83 | −0.63 | −1.97 |
| | 4 | 1.30 | 0.94 | −0.84 |
Table 9.
Forecast accuracy measures by gender at various forecast horizons.
Table 9.
Forecast accuracy measures by gender at various forecast horizons.
| | h | MAPE (%) | RMSE |
|---|
| | Male | Female | Male | Female |
|---|
| ITSA | 1 | 6.97 | 6.00 | 151.43 | 96.07 |
| 2 | 7.57 | 7.20 | 163.41 | 110.79 |
| 4 | 8.46 | 7.16 | 220.10 | 177.23 |
| 8 | 2.41 | 2.77 | 53.03 | 45.15 |
| SARIMA | 1 | 6.67 | 9.31 | 158.27 | 217.90 |
| 2 | 8.59 | 9.31 | 184.78 | 217.90 |
| 4 | 9.25 | 13.91 | 189.85 | 289.89 |
| 8 | 9.84 | 26.74 | 227.79 | 472.06 |
| ETS | 1 | 5.81 | 6.53 | 137.09 | 119.81 |
| 2 | 7.29 | 6.49 | 160.64 | 127.23 |
| 4 | 7.18 | 8.10 | 153.22 | 142.24 |
| 8 | 8.57 | 14.41 | 185.94 | 237.84 |
| SNAIVE | 1 | 13.91 | 13.58 | 347.11 | 310.31 |
| 2 | 15.64 | 14.84 | 368.17 | 328.66 |
| 4 | 17.46 | 18.98 | 407.49 | 378.96 |
| 8 | 23.72 | 34.09 | 554.77 | 593.45 |
Table 10.
Results of the modified Diebold–Mariano test comparing ITSA to ETS, SARIMA without intervention, and SNAIVE by gender.
Table 10.
Results of the modified Diebold–Mariano test comparing ITSA to ETS, SARIMA without intervention, and SNAIVE by gender.
| Gender | h | ETS | SARIMA | SNAIVE |
|---|
| Female | 1 | −0.72 | −1.20 | −1.27 |
| | 4 | −0.26 | −0.85 | −0.98 |
| Male | 1 | 0.53 | −0.30 | −1.73 |
| | 4 | 0.22 | −0.15 | −1.15 |



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
















