
Investigating the Cytotoxicity of Dual-Cure Bulk-Fill Resin Materials on L929 Cells

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Culture
2.2. Preparation of the Specimens
2.2.1. Experimental Groups
2.2.2. Control Groups
- The Medium Control Group (MC): The medium of L929 cells was not removed. No light was applied to the cells;
- The Medium-Free Control Group (MFC): The purpose of this control group was to investigate to what extent the 40 s waiting time (which is the longest polymerization time of the materials) would affect the viability of the cells when preparing the samples in an outside environment. While preparing this group, the medium of L929 cells was removed. No light was applied to the cells. After waiting for 40 s, the medium was readded;
- The Physical Control Group (PC): The purpose of this control group was to mimic the weight of the test material with a cotton pellet, a sterile neutral material, to examine whether any cell death would occur on the cell group they were applied to. After removing the medium, plastic rings with only cotton pellets were placed directly on the cells and the medium was readded;
- The Light Applied Control Group (LAC): The purpose of this control group was to investigate whether there would be any cell death when light was applied for 40 s (which is the longest polymerization applied to the tested materials), and then the medium was readded.
2.3. Evaluation of Cell Morphology and Assessment of Cell Viability Using WST-1 Assay
2.4. Statistical Analyzes
3. Results
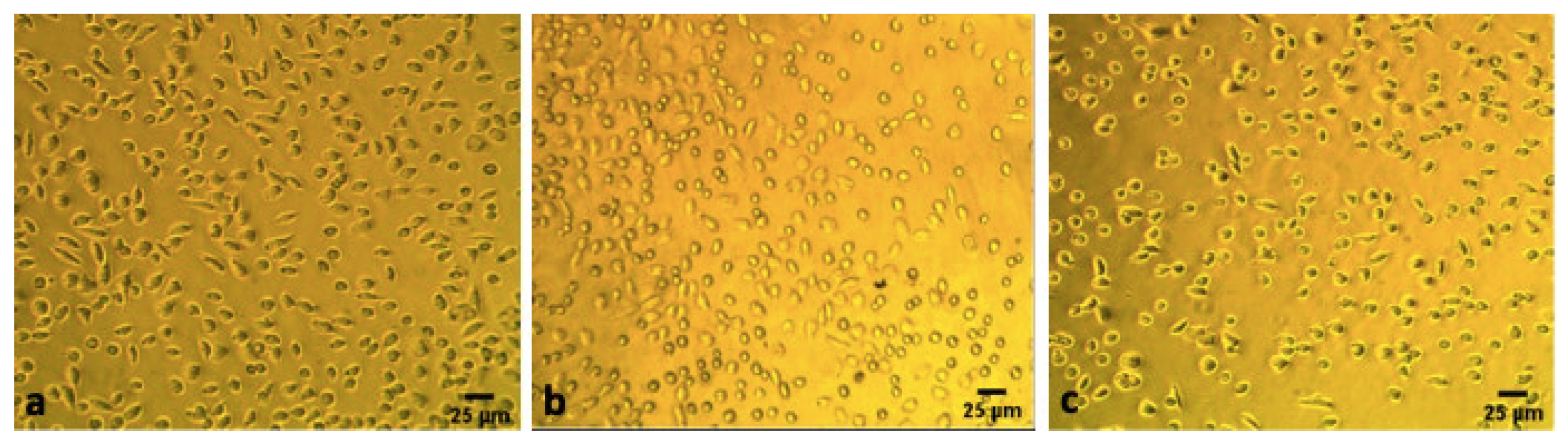
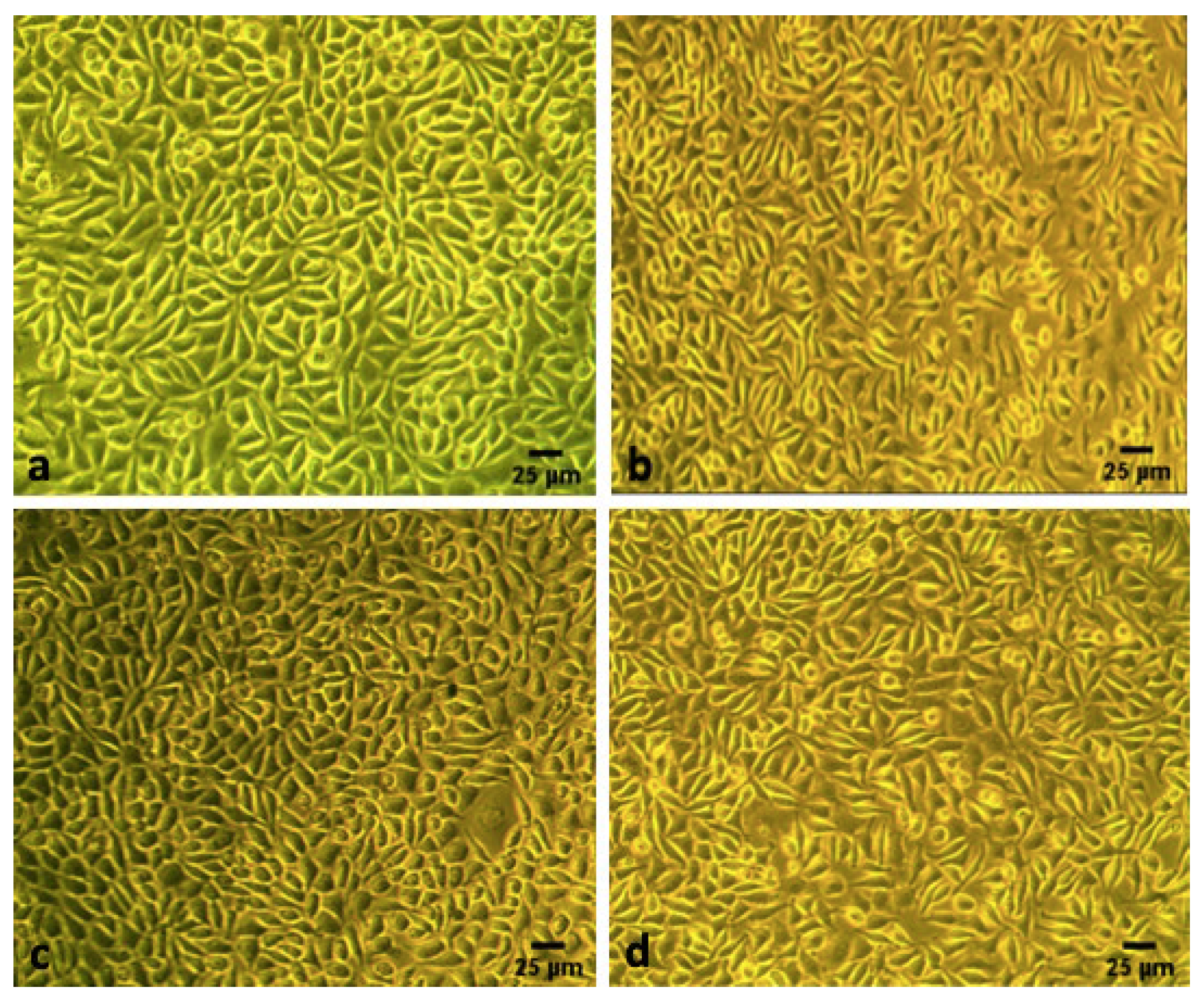
3.1. Alteration in the Morphology of Cells
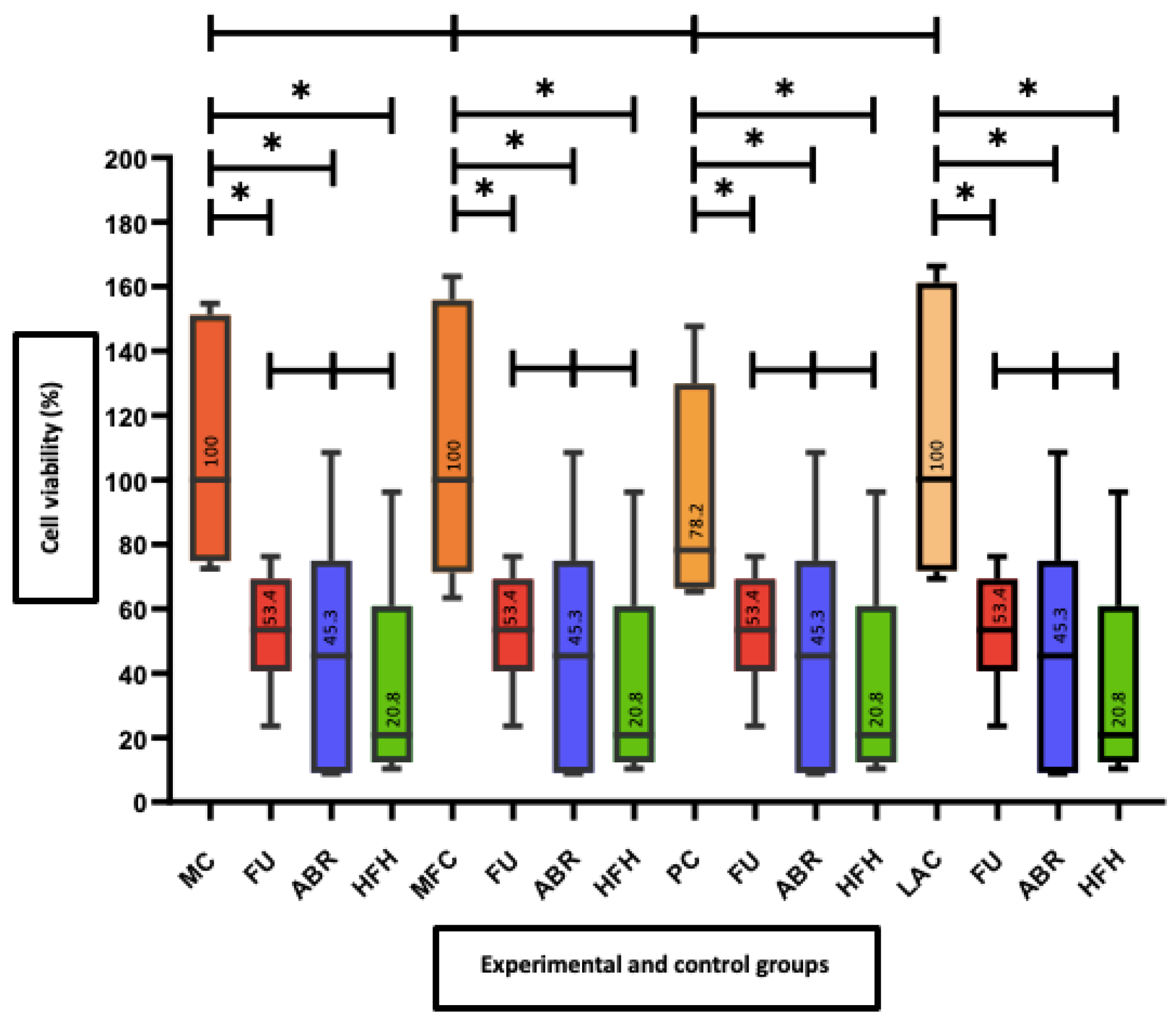
3.2. Viability of the Cells (WST-1 Test)
4. Discussion
5. Conclusions
- The cytotoxic effects of the materials on cell viability have been shown to parallel with the cell morphology;
- It can be suggested that clinicians should pay attention, while applying dual-cure bulk-fill materials in deep cavities or should use a liner material under these materials.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leprince, J.G.; Palin, W.M.; Hadis, M.A.; Devaux, J.; Leloup, G. Progress in dimethacrylate-based dental composite technology and curing efficiency. Dent. Mater. 2013, 29, 139–156. [Google Scholar] [CrossRef] [PubMed]
- Uzel, Y.; Kuru, R.; Eden, E. The effect of different application procedures on microleakage and microhardness of a bulk-fill composite material. J. Ege Univ. Faculty Dent. 2017, 38, 48–53. [Google Scholar] [CrossRef]
- Ilie, N.; Bucuta, S.; Draenert, M. Bulk-fill resin-based composites: An in vitro assessment of their mechanical performance. Oper. Dent. 2013, 38, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Kwon, T.Y.; Bagheri, R.; Kim, Y.K.; Kim, K.H.; Burrow, M.F. Cure mechanisms in materials for use in esthetic dentistry. J. Investig. Clin. Dent. 2012, 3, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Taubock, T.T.; Bortolotto, T.; Buchalla, W.; Attin, T.; Krejci, I. Influence of light-curing protocols on polymerization shrinkage and shrinkage force of a dual-cured core build-up resin composite. Eur. J. Oral Sci. 2010, 118, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Vandewalker, J.P.; Casey, J.A.; Lincoln, T.A.; Vandewalle, K.S. Properties of dual-cure, bulk-fill composite resin restorative materials. Gen. Dent. 2016, 64, 68–73. [Google Scholar]
- Wataha, J.C. Predicting clinical biological responses to dental materials. Dent. Mater. 2012, 28, 23–40. [Google Scholar] [CrossRef]
- Murray, P.E.; García Godoy, C.; García Godoy, F. How is the biocompatibilty of dental biomaterials evaluated? Med. Oral Patol. Oral Cir. Bucal. 2007, 12, 258–266. [Google Scholar]
- Gencoglu, N.; Kelasioglu, F. Investigation of cytotoxicity of some root canal sealers. J. Istanbul Univ. Fac. Dent. 1994, 28, 109–112. [Google Scholar]
- ElReash, A.A.; Hamama, H.; Abdo, W.; Wu, Q.; El-Din, A.Z.; Xiaoli, X. Biocompatibility of new bioactive resin composite versus calcium silicate cements: An animal study. BMC Oral Health 2019, 19, 194. [Google Scholar] [CrossRef]
- Kazak, M.; Donmez, N.; Bahadori, F.; Yenigun, V.B.; Kocyigit, A. A preliminary research study on the cytotoxicity of expired and non-expired composite resins: In vitro study. Odovtos 2020, 22, 123–134. [Google Scholar]
- Mosmann, T. Rapid colorimetric assay for cellular growth and survival: Application to proliferation and cytotoxicity assays. J. Immunol. Methods 1983, 65, 55–63. [Google Scholar] [CrossRef]
- ISO 10993-5; 2009-Biological Evaluation of Medical Devices-Part 5: Tests for In Vitro Cytotoxicity. International Organization for Standardization: Geneve, Switzerland, 2009.
- Toz, T.; Kiremitci, A.; Cakmak, A.S.; Tan, O.U.; Palaska, E.; Gumusderelioglu, M.; Ozcan, M. A comparative study on monomer elution and cytotoxicity of different adhesive restoration materials. J. Adhes. Sci. Technol. 2017, 31, 414–429. [Google Scholar] [CrossRef]
- Monterubbianesi, R.; Orsini, G.; Tosi, G.; Conti, C.; Librando, V.; Procaccini, M.; Putignano, A. Spectroscopic and mechanical properties of a new generation of bulk fill composites. Front. Physiol. 2016, 7, 652. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.E.; Smith, A.J. Saving pulps—A biological basis. An overview. Prim. Dent. Care 2002, 9, 21–26. [Google Scholar] [CrossRef]
- Geurtsen, W. Biocompatibility of resin-modified filling materials. Crit. Rev. Oral Biol. Med. 2000, 11, 333–355. [Google Scholar] [CrossRef]
- Schedle, A.; Franz, A.; Rausch-Fan, X.; Spittler, A.; Lucas, T.; Samorapoompichit, P.; Sperr, W.; Boltz-Nitulescu, G. Cytotoxic effects of dental composites, adhesive substances, compomers and cements. Dent. Mater. 1998, 14, 429–440. [Google Scholar] [CrossRef]
- Selimović-Dragaš, M.; Huseinbegović, A.; Kobašlija, S.; Hatibović-Kogfman, S. A comparison of the in vitro cytotoxicity of conventional and resin modified glass ionomer cements. Bosn. J. Basic Med. Sci. 2012, 12, 273–278. [Google Scholar] [CrossRef]
- Ulker, H.E.; Sengun, A. Cytotoxicity evaluation of self adhesive composite resin cements by dentin barrier test on 3D pulp cells. Eur. J. Dent. 2009, 3, 120–126. [Google Scholar] [CrossRef]
- Cao, T.; Saw, T.Y.; Heng, B.C.; Liu, H.; Yap, A.U.J.; Ng, M.L. Comparison of different test models for the assessment of cytotoxicity of composite resins. J. Appl. Toxicol. 2005, 25, 101–108. [Google Scholar] [CrossRef]
- Taira, M.; Nakao, H.; Matsumoto, T.; Takahashi, J. Cytotoxic effect of methyl methacrylate on 4 cultured fibroblasts. Int. J. Prosthodont. 2000, 13, 311–315. [Google Scholar] [PubMed]
- Saw, T.Y.; Cao, T.; Yap, A.U.J.; Ng, M.M.L. Tooth slice organ culture and established cell line culture models for cytotoxicity assessment of dental materials. Toxicol. In Vitro 2005, 19, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Thonemann, B.; Schmalz, G.; Hiller, K.A.; Schweikl, H. Responses of L929 mouse fibroblasts, primary and immortalized bovine dental papilla-derived cell lines to dental resin components. Dent. Mater. 2002, 18, 318–323. [Google Scholar] [CrossRef]
- Skin, H.-P.A. Mucosal reactions associated with dental materials. Eur. J. Oral Sci. 1998, 106, 707–712. [Google Scholar]
- Wataha, J.C.; Lockwood, P.E.; Bouillaguet, S.; Noda, M. In vitro biological response to core and flowable dental restorative materials. Dent. Mater. 2003, 19, 25–31. [Google Scholar] [CrossRef]
- Kazak, M.; Donmez, N.; Bahadori, F.; Yenigun, V.B.; Kocyigit, A. Investigation of in vitro cytotoxic effects of different content bulk-fill materials polymerized with a new generation light curing unit and determination of cytotoxicity origins by LC-MS/MS method. In Proceedings of the Turkish Society of Restorative Dentistry, 23rd International Scientific Congress, Antalya, Turkey, 6–8 December 2019; Abstract Book. pp. 114–115. [Google Scholar]
- López-García, S.; Pecci-Lloret, M.P.; Pecci-Lloret, M.R.; Oñate-Sánchez, R.E.; García-Bernal, D.; Castelo-Baz, P.; Rodríguez-Lozano, F.J.; Guerrero-Gironés, J. In vitro evaluation of the biological effects of ACTIVA Kids BioACTIVE restorative, Ionolux, and Riva Light Cure on human dental pulp stem cells. Materials 2019, 12, 3694. [Google Scholar] [CrossRef]
- Karabulut, B.; Donmez, N.; Goret, C.C.; Atas, C.; Kuzu, O. Reactions of subcutaneous connective tissue to mineral trioxide aggregate, Biodentine®, and a newly developed BioACTIVE Base/Liner. Scanning 2020, 2020, 6570159. [Google Scholar] [CrossRef]
- Eckhardt, A.; Harorli, T.; Limtanyakul, J.; Hiller, K.A.; Bosl, C.; Bolay, C.; Reichl, F.X.; Schmalz, G.; Schweikl, H. Inhibition of cytokine and surface antigen expression in LPS-stimulated murine macrophages by triethylene glycol dimethacrylate. Biomaterials 2009, 30, 1665–1674. [Google Scholar] [CrossRef]
- Ferracane, J. Elution of leachable components from composites. J. Oral Rehabil. 1994, 21, 441–452. [Google Scholar] [CrossRef]
- Kanjevac, T.; Milovanovic, M.; Volarevic, V.; Lukic, M.L.; Arsenijevic, N.; Markovic, D.; Zdravkovic, N.; Tesic, Z.; Lukic, A. Cytotoxic effects of glass ionomer cements on human dental pulp stem cells correlate with fluoride release. Med. Chem. 2012, 8, 40–45. [Google Scholar] [CrossRef]
- Demirel, G.; Gur, G.; Demirsoy, F.F.; Altuntas, E.G.; Yener-Ilce, B.; Kilicarslan, M.A. Cytotoxic effects of contemporary bulk-fill dental composites: A real-time cell analysis. Dent. Mater. J. 2020, 39, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Toh, W.; Yap, A.; Lim, S. In vitro biocompatibility of contemporary bulk-fill composites. Oper. Dent. 2015, 40, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Yoruc, A.B.H.; Kızılbey, K.A.; Karaul, A.; Cakmakcioglu, O. Effects of curing systems and light units on cytotoxicity of dental composites. IJOER 2016, 2, 117–126. [Google Scholar]
- Goncalves, F.; Campos, L.M.P.; Rodrigues-Júnior, E.C.; Costa, F.V.; Marques, P.A.; Francci, C.E.; Braga, R.R.; Boaro, L.C.C. A comparative study of bulk-fill composites: Degree of conversion, post-gel shrinkage and cytotoxicity. Braz. Oral Res. 2018, 32, e17. [Google Scholar] [CrossRef]
- Attik, N.; Hallay, F.; Bois, L.; Brioude, A.; Grosgogeat, B.; Colon, P. Mesoporous silica fillers and resin composition effect on dental composites cytocompatibility. Dent. Mater. 2017, 33, 166–174. [Google Scholar] [CrossRef]
- de Souza Costa, C.A.; Hebling, J.; Garcia-Godoy, F.; Hanks, C.T. In vitro cytotoxicity of five glass-ionomer cements. Biomaterials 2003, 24, 3853–3858. [Google Scholar] [CrossRef]
- Imazato, S.; Horikawa, D.; Takeda, K.; Kiba, W.; Izutani, N.; Yoshikawa, R.; Hayashi, M.; Ebisu, S.; Nakano, T. Proliferation and differentiation potential of pluripotent mesenchymal precursor C2C12 cells on resin-based restorative materials. Dent. Mater. J. 2010, 29, 341–346. [Google Scholar] [CrossRef]
- Soderholm, K.J.M. Filler leachability during water storage of six composite materials. Scand. J. Dent. Res. 1990, 98, 82–88. [Google Scholar] [CrossRef]
- Soderholm, K.J.M.; Mukherjee, R.; Longmate, J. Filler leachability of composites stored in distilled water or artificial saliva. J. Dent. Res. 1996, 75, 1692–1699. [Google Scholar] [CrossRef]
- Soderholm, K.J.M.; Yang, M.C.; Garcea, I. Filler particle leachability of experimental dental composites. Eur. J. Oral Sci. 2000, 108, 555–560. [Google Scholar] [CrossRef]
- Bouschlicher, M.R.; Rueggeberg, F.A.; Wilson, B.M. Correlation of bottom-to-top surface microhardness and conversion ratios for a variety of resin composite compositions. Oper. Dent. 2004, 29, 698–704. [Google Scholar] [PubMed]
- Leprince, J.G.; Leveque, P.; Nysten, B.; Gallez, B.; Devaux, J.; Leloup, G. New insight into the “depth of cure” of dimethacrylate-based dental composites. Dent. Mater. 2012, 28, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.; Park, S.; Hwang, I. Polymerization shrinkage and depth of cure of bulk-fill resin composites and highly filled flowable resin. Oper. Dent. 2015, 40, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, N.; Jain, A.; Gupta, H.; Abrol, A.; Singh, C.; Rapgay, T. The comparative evaluation of depth of cure of bulk-fill composites—An in vitro study. J. Conserv. Dent. 2019, 22, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Schmalz, G. Use of cell cultures for toxicity testing of dental materials-advantages and limitations. J. Dent. 1994, 22, S6–S11. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Material | Material | Composition | Polymerization Reaction | Inorganic Filler Content | Color | LOT Number | Manufacturer |
|---|---|---|---|---|---|---|---|
| Flowable bulk-fill material | Fill-Up!™ | TMPTMA, UDMA, BisGMA, TEGDMA, dental glass, amorphous silica, zinc oxide | Dual-cure | 65% (weight) 49% (volume) | Universal | 192896 | Coltene, Whaledent, Switzerland |
| Bioactive material | ACTIVA™ BioACTIVE-RESTORATIVE™ | Blend of diurethane and other methacrylates with modified polyacrylic acid, sodium fluoride, amorphous silica, bioactive glass | Dual-cure + Acid-Base reaction (glass ionomer reaction) | 56% (weight) | A2 | 190110 | Pulpdent Corporation, Watertown, USA |
| Dual-cure bulk-fill composite material | HyperFIL® HAp | BisEMA, TEGDMA, TMDPO, UDMA, TMPTA, HEMA, BPO, camphoroquinone, barium glass, silica, nano-hydroxyapatite | Dual-cure | 74% (weight) | Universal | 1901019010 | Parkell, USA |
| Fill-Up!™ + VALO™ Cordless (10 s) (n = 3) | ACTIVA™ BioACTIVE-RESTORATIVE™ + VALO™ Cordless (20 s) (n = 3) |
|---|---|
| HyperFIL® HAp + VALO™ Cordless (40 s) (n = 3) | The Medium Control Group (n = 3) |
| The Medium-Free Control Group (n = 3) | The Physical Control Group (n = 3) |
| The Light Applied Control Group (n = 3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koymen, S.S.; Donmez, N.; Yenigun, V.B.; Bahadori, F.; Kocyigit, A. Investigating the Cytotoxicity of Dual-Cure Bulk-Fill Resin Materials on L929 Cells. Prosthesis 2022, 4, 447-457. https://doi.org/10.3390/prosthesis4030036
Koymen SS, Donmez N, Yenigun VB, Bahadori F, Kocyigit A. Investigating the Cytotoxicity of Dual-Cure Bulk-Fill Resin Materials on L929 Cells. Prosthesis. 2022; 4(3):447-457. https://doi.org/10.3390/prosthesis4030036
Chicago/Turabian StyleKoymen, Safiye Selin, Nazmiye Donmez, Vildan Betul Yenigun, Fatemeh Bahadori, and Abdurrahim Kocyigit. 2022. "Investigating the Cytotoxicity of Dual-Cure Bulk-Fill Resin Materials on L929 Cells" Prosthesis 4, no. 3: 447-457. https://doi.org/10.3390/prosthesis4030036
APA StyleKoymen, S. S., Donmez, N., Yenigun, V. B., Bahadori, F., & Kocyigit, A. (2022). Investigating the Cytotoxicity of Dual-Cure Bulk-Fill Resin Materials on L929 Cells. Prosthesis, 4(3), 447-457. https://doi.org/10.3390/prosthesis4030036