


Pregnancy and Type 2 Diabetes: Unmet Goals



Abstract
:1. Introduction
2. Epidemiology
3. Pregnancy Outcomes
4. Metabolic Control during Pregnancy
5. Factors Affecting Pregnancy Outcomes in Women with Type 2 Diabetes
6. Physiopathology: New Trends
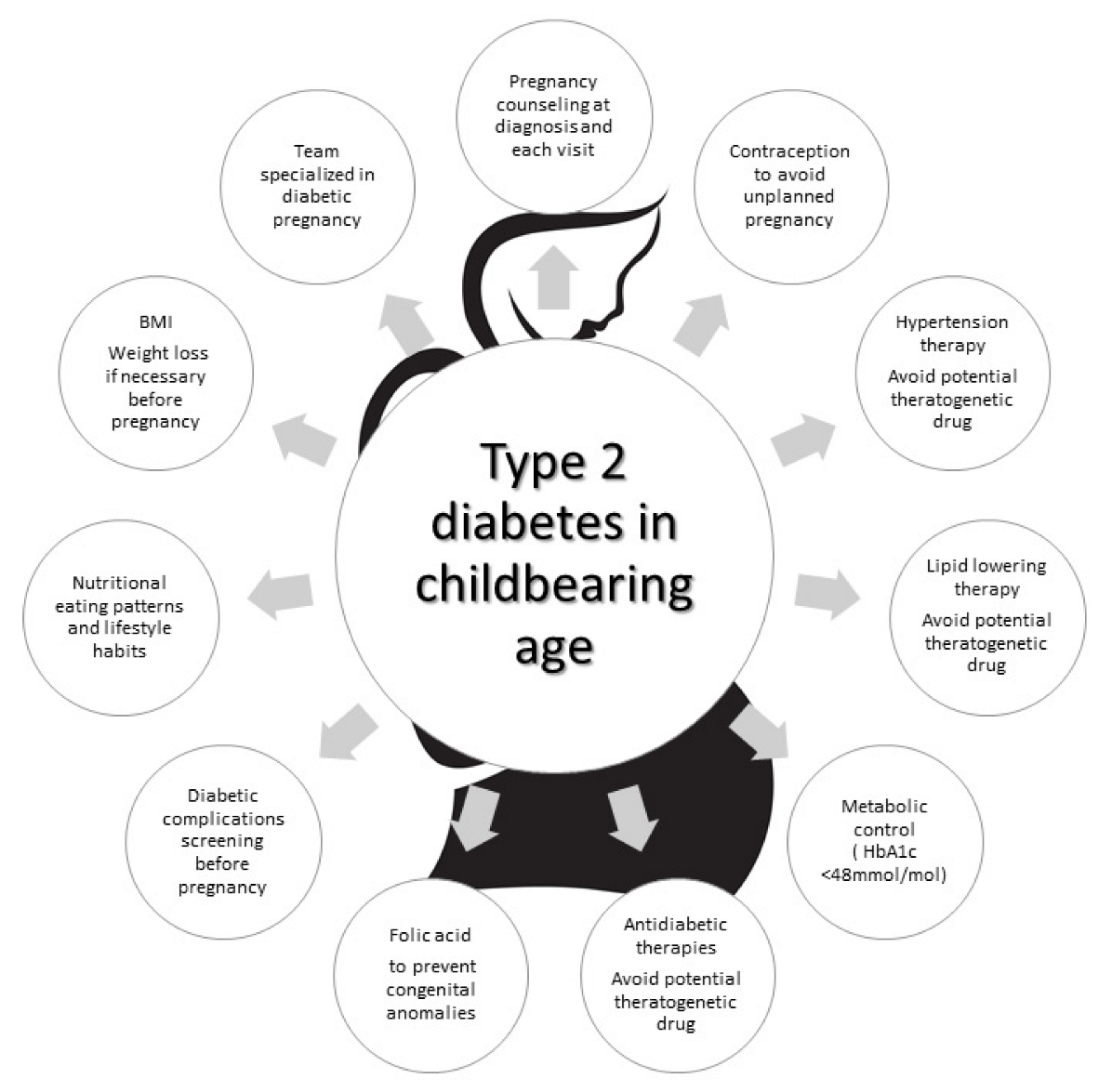
7. Strategies to Improve Pregnancy Outcomes in Women with TD2
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sugrue, R.; Zera, C. Pregestational Diabetes in Pregnancy. Obstet. Gynecol. Clin. N. Am. 2018, 45, 315–331. [Google Scholar] [CrossRef] [PubMed]
- Chivese, T.; Hoegfeldt, C.A.; Werfalli, M.; Yuen, L.; Sun, H.; Karuranga, S.; Li, N.; Gupta, A.; Immanuel, J.; Divakar, H.; et al. IDF Diabetes Atlas: The prevalence of pre-existing diabetes in pregnancy—A systematic reviewand meta-analysis of studies published during 2010–2020. Diabetes Res. Clin. Pract. 2022, 183, 109049. [Google Scholar] [CrossRef] [PubMed]
- Engelgau, M.M.; Herman, W.H.; Smith, P.J.; German, R.R.; Aubert, R.E. The epidemiology of diabetes and pregnancy in the U.S., 1988. Diabetes Care 1995, 18, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, S.S.; Kuklina, E.V.; Bansil, P.; Jamieson, D.J.; Whiteman, M.K.; Kourtis, A.P.; Posner, S.F.; Callaghan, W.M. Diabetes trends among delivery hospitalizations in the U.S., 1994–2004. Diabetes Care 2010, 33, 768–773. [Google Scholar] [CrossRef]
- Fadl, H.E.; Simmons, D. Trends in diabetes in pregnancy in Sweden 1998–2012. BMJ Open Diabetes Res. Care 2016, 4, e000221. [Google Scholar] [CrossRef]
- Mackin, S.T.; Nelson, S.M.; Kerssens, J.J.; Wood, R.; Wild, S.; Colhoun, H.M.; Leese, G.P.; Philip, S.; Lindsay, R.S. on behalf of the SDRN Epidemiology Group. Diabetes and pregnancy: National trends over a 15 year period. Diabetologia 2018, 61, 1081–1088. [Google Scholar]
- Coton, S.J.; Nazareth, I.; Petersen, I. A cohort study of trends in the prevalence of pregestational diabetes in pregnancy recorded in UK general practice between 1995 and 2012. BMJ Open 2016, 6, e009494. [Google Scholar] [CrossRef]
- López-de-Andrés, A.; Perez-Farinos, N.; Hernández-Barrera, V.; Palomar-Gallego, M.A.; Carabantes-Alarcón, D.; Zamorano-León, J.J.; de Miguel-Diez, J.; Jimenez-Garcia, R. A Population-Based Study of Diabetes During Pregnancy in Spain (2009–2015): Trends in Incidence, Obstetric Interventions, and Pregnancy Outcomes. J. Clin. Med. 2020, 9, 582. [Google Scholar] [CrossRef]
- National Pregnancy in Diabetes Audit Report (NPID) 2020–2021. Available online: https://www.hqip.org.uk/resource/national-pregnancy-in-diabetes-audit-report-2020/ (accessed on 11 May 2023).
- Weindling, A.M. The confidential enquiry into maternal and child health (CEMACH). Arch. Dis. Child. 2003, 88, 1034–1037. [Google Scholar] [CrossRef]
- Macintosh, M.C.; Fleming, K.M.; Bailey, J.A.; Doyle, P.; Modder, J.; Acolet, D.; Golightly, S.; Miller, A. Perinatal mortality and congenital anomalies in babies of women with type 1 or type 2 diabetes in England, Wales, and Northern Ireland: Population based study. BMJ 2006, 333, 177. [Google Scholar] [CrossRef]
- Balsells, M.; García-Patterson, A.; Gich, I.; Corcoy, R. Maternal and fetal outcome in women with type 2 versus type 1 diabetes mellitus: A systematic review and metaanalysis. J. Clin. Endocrinol. Metab. 2009, 94, 4284–4291. [Google Scholar] [CrossRef] [PubMed]
- Lapolla, A.; Dalfrà, M.G.; Di Cianni, G.; Bonomo, M.; Parretti, E.; Mello, G.; Scientific Committee of the GISOGD Group. A multicenter Italian study on pregnancy outcome in women with diabetes. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Owens, L.A.; Sedar, J.; Carmody, L.; Dunne, F. Comparing type 1 and type 2 diabetes in pregnancy- similar conditions or is a separate approach required? BMC Pregnancy Childbirth 2015, 15, 69. [Google Scholar] [CrossRef] [PubMed]
- Murphy, H.R.; Bell, R.; Cartwright, C.; Curnow, P.; Maresh, M.; Morgan, M.; Sylvester, C.; Young, B.; Lewis-Barned, N. Improved pregnancy outcomes in women with type 1 and type 2 diabetes but substantial clinic-to-clinic variations: A prospective nationwide study. Diabetologia 2017, 60, 1668–1677. [Google Scholar] [CrossRef] [PubMed]
- Mirabelli, M.; Tocci, V.; Donnici, A.; Giuliano, S.; Sarnelli, P.; Salatino, A.; Greco, M.; Puccio, L.; Chiefari, E.; Foti, D.P.; et al. Maternal Preconception Body Mass Index Overtakes Age as a Risk Factor for Gestational Diabetes Mellitus. J. Clin. Med. 2023, 12, 2830. [Google Scholar] [CrossRef]
- Maple-Brown, L.; Lee, I.L.; Longmore, D.; Barzi, F.; Connors, C.; Boyle, J.A.; Moore, E.; Whitbread, C. PANDORA Study research team. Pregnancy And Neonatal Diabetes Outcomes in Remote Australia: The PANDORA study-an observational birth cohort. Int. J. Epidemiol. 2019, 48, 307–318. [Google Scholar] [CrossRef]
- Ali, D.S.; Davern, R.; Rutter, E.; Coveney, C.; Devine, H.; Walsh, J.M.; Higgins, M.; Hatunic, M. Pre-Gestational Diabetes and Pregnancy Outcomes. Diabetes Ther. 2020, 11, 2873–2885. [Google Scholar] [CrossRef]
- Murphy, H.R.; Howgate, C.; O’Keefe, J.; Myers, J.; Morgan, M.; Coleman, M.A.; Jolly, M.; Valabhji, J.; Scott, E.M.; Knighton, P.; et al. National Pregnancy in Diabetes (NPID) advisory group. Characteristics and outcomes of pregnant women with type 1 or type 2 diabetes: A 5-year national population-based cohort study. Lancet Diabetes Endocrinol. 2021, 9, 153–164. [Google Scholar] [CrossRef]
- Guarnotta, V.; Mineo, M.I.; Giacchetto, E.; Imbergamo, M.P.; Giordano, C. Maternal-foetal complications in pregnancy: A retrospective comparison between type 1 and type 2 diabetes mellitus. BMC Pregnancy Childbirth 2021, 21, 243. [Google Scholar] [CrossRef]
- Gualdani, E.; Di Cianni, G.; Seghieri, M.; Francesconi, P.; Seghieri, G. Pregnancy outcomes and maternal characteristics in women with pregestational and gestational diabetes: A retrospective study on 206,917 singleton live births. Acta Diabetol. 2021, 58, 1169–1176. [Google Scholar] [CrossRef]
- Newman, C.; Egan, A.M.; Ahern, T.; Al-Kiyumi, M.; Balan, G.; Brassill, M.J.; Brosnan, E.; Carmody, L.; Clarke, H.; Kelly, C.C.; et al. Diabetes care and pregnancy outcomes for women with pregestational diabetes in Ireland. Diabetes Res. Clin. Pract. 2021, 173, 108685. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.; Egan, A.M.; Ahern, T.; Al-Kiyumi, M.; Bacon, S.; Bahaeldein, E.; Balan, G.; Brassill, M.J.; Breslin, E.; Brosnan, E.; et al. Retrospective national cohort study of pregnancy outcomes for women with type 1 and type 2 diabetes mellitus in Republic of Ireland. Diabetes Res. Clin. Pract. 2022, 189, 109947. [Google Scholar] [CrossRef] [PubMed]
- TODAY Study Group. Pregnancy Outcomes in Young Women With Youth-Onset Type 2 Diabetes Followed in the TODAY Study. Diabetes Care 2022, 45, 1038–1045. [Google Scholar] [CrossRef] [PubMed]
- Pylypjuk, C.; Sellers, E.; Wicklow, B. Perinatal Outcomes in a Longitudinal Birth Cohort of First Nations Mothers With Pregestational Type 2 Diabetes and Their Offspring: The Next Generation Study. Can. J. Diabetes 2021, 45, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Booth, G.L.; Ray, J.G.; Ling, V.; Feig, D.S. Undiagnosed type 2 diabetes during pregnancy is associated with increased perinatal mortality: A large population-based cohort study in Ontario, Canada. Diabet. Med. 2020, 37, 1696–1704. [Google Scholar] [CrossRef] [PubMed]
- Murphy, H.R.; Rayman, G.; Duffield, K.; Lewis, K.S.; Kelly, S.; Johal, B.; Fowler, D.; Temple, R.C. Changes in the glycemic profiles of women with type 1 and type 2 diabetes during pregnancy. Diabetes Care 2007, 30, 2785–2791. [Google Scholar] [CrossRef] [PubMed]
- Murphy, H.R.; Moses, R.G. Pregnancy Outcomes of Young Women with Type 2 Diabetes: Poor Care and Inadequate Attention to Glycemia. Diabetes Care 2022, 45, 1046–1048. [Google Scholar] [CrossRef]
- Lapolla, A.; Dalfrà, M.G.; Fedele, D. Pregnancy complicated by diabetes: What is the best level of HbA1c for conception? Acta Diabetol. 2010, 47, 187–192. [Google Scholar] [CrossRef]
- Catalano, P.M.; Tyzbir, E.D.; Roman, N.M.; Amini, S.B.; Sims, E.A. Longitudinal changes in insulin release and insulin resistance in nonobese pregnant women. Am. J. Obstet. Gynecol. 1991, 165, 1667–1672. [Google Scholar] [CrossRef]
- Catalano, P.M.; Huston, L.; Amini, S.B.; Kalhan, S.C. Longitudinal changes in glucose metabolism during pregnancy in obese women with normal glucose tolerance and gestational diabetes mellitus. Am. J. Obstet. Gynecol. 1999, 180, 903–916. [Google Scholar] [CrossRef]
- Nadeau, H.C.G.; Maxted, M.E.; Madhavan, D.; Pierce, S.L.; Feghali, M.; Scifres, C. Insulin Dosing, Glycemic Control, and Perinatal Outcomes in Pregnancies Complicated by Type-2 Diabetes. Am. J. Perinatol. 2021, 38, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Wernimont, S.A.; Sheng, J.S.; Tymkowicz, A.; Fleener, D.K.; Summers, K.M.; Syrop, C.H.; Andrews, J.I. Adherence to self-glucose monitoring recommendations and perinatal outcomes in pregnancies complicated by diabetes mellitus. Am. J. Obstet. Gynecol. MFM 2019, 1, 100031. [Google Scholar] [CrossRef] [PubMed]
- Gaudio, M.; Dozio, N.; Feher, M.; Scavini, M.; Caretto, A.; Joy, M.; Van Vlymer, M.; Hinton, W.; de Lusignan, S. Trends in Factors Affecting Pregnancy Outcomes Among Women with Type 1 or Type 2 Diabetes of Childbearing Age (2004–2017). Front. Endocrinol. 2021, 11, 596633. [Google Scholar] [CrossRef] [PubMed]
- Allen, A.J.; Snowden, J.M.; Lau, B.; Cheng, Y.; Caughey, A.B. Type-2 diabetes mellitus: Does prenatal care affect outcomes? J. Matern. Fetal Neonatal Med. 2018, 31, 93–97. [Google Scholar] [CrossRef]
- Creanga, A.A.; Catalano, P.M.; Bateman, B.T. Obesity in Pregnancy. N. Engl. J. Med. 2022, 387, 248–259. [Google Scholar] [CrossRef]
- Lapolla, A.; Dalfrà, M.G.; Fedele, D. Pregnancy complicated by type 2 diabetes: An emerging problem. Diabetes Res. Clin. Pract. 2008, 80, 2–7. [Google Scholar] [CrossRef]
- McIntire, H.D.; Barrett, H.L. Obesity in pregnancy: Epidemiology, mechanisms, nutritional and metabolic management. In Gestational Diabetes a Decade after the HAPO Study; Front, D., Lapolla, A., Metzeg, B.E., Eds.; Karger: Basel, Switzerland, 2020; Volume 28, p. 2134. [Google Scholar]
- Feig, D.S.; Donovan, L.E.; Zinman, B.; Sanchez, J.J.; Asztalos, E.; Ryan, E.A.; Fantus, I.G.; Hutton, E.; Armson, A.B.; Lipscombe, L.L.; et al. MiTy Collaborative Group. Metformin in women with type 2 diabetes in pregnancy (MiTy): A multicentre, international, randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2020, 8, 834–844. [Google Scholar] [CrossRef]
- Lapolla, A.; Burlina, S.; Dalfrà, M.G. Comment: Characteristics and outcomes of pregnant women with type 1 or type 2 diabetes-a 5-year national population-based cohort study. J. Endocrinol. Investig. 2022, 45, 221–224. [Google Scholar] [CrossRef]
- Khurana, R.; Meneilly, G.S.; Lim, K.; Thompson, D. The effect of hyperinsulinemia and hyperglycemia on endothelial function in pregnant patients with type-2 diabetes. Diabetes Res. Clin. Pract. 2014, 103, e11–e13. [Google Scholar] [CrossRef]
- Sultan, S. The effect of maternal type 2 diabetes on fetal endothelial gene expression and function. Acta Diabetol. 2019, 56, 73–85. [Google Scholar] [CrossRef]
- Dalfrà, M.G.; Burlina, S.; Del Vescovo, G.G.; Lapolla, A. Genetics and Epigenetics: New Insight on Gestational Diabetes Mellitus. Front. Endocrinol. 2020, 11, 602477. [Google Scholar] [CrossRef] [PubMed]
- Moreli, J.B.; Santos, J.H.; Lorenzon-Ojea, A.R.; Corrêa-Silva, S.; Fortunato, R.S.; Rocha, C.R.; Rudge, M.V.; Damasceno, D.C.; Bevilacqua, E.; Calderon, I.M. Hyperglycemia Differentially Affects Maternal and Fetal DNA Integrity and DNA Damage Response. Int. J. Biol. Sci. 2016, 12, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Michalczyk, A.A.; Janus, E.D.; Judge, A.; Ebeling, P.R.; Best, J.D.; Ackland, M.J.; Asproloupos, D.; Dunbar, J.A.; Ackland, M.L. Transient epigenomic changes during pregnancy and early postpartum in women with and without type 2 diabetes. Epigenomics 2018, 10, 419–431. [Google Scholar] [CrossRef]
- Gupta, J.; Tikoo, K. Involvement of insulin-induced reversible chromatin remodeling in altering the expression of oxidative stress-responsive genes under hyperglycemia in 3T3-L1 preadipocytes. Gene 2012, 504, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Klose, R.J.; Zhang, Y. Regulation of histone methylation by demethylimination and demethylation. Nat. Rev. Mol. Cell Biol. 2007, 8, 307–318. [Google Scholar] [CrossRef] [PubMed]
- Schaefer-Graf, U.; Napoli, A.; Nolan, C.J. Diabetic Pregnancy Study Group. Diabetes in pregnancy: A new decade of challenges ahead. Diabetologia 2018, 61, 1012–1021. [Google Scholar] [PubMed]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 15. Management of Diabetes in Pregnancy: Standards of Care in Diabetes-2023. Diabetes Care 2023, 46, S254–S266. [Google Scholar] [CrossRef]
- The Saint Vincent Declaration on diabetes care and research in Europe. Acta Diabetol. 1989, 10, 143–144.


{kind=link}
| Author (References) | N° | T2D Duration Years | AGE Years | HbA1c% 1st Trim. | BMI or % Obesity (O) (>30 kg/m2) | Caucasian | PPC | Folic Acid | Pregnancy Outcomes | Country |
|---|---|---|---|---|---|---|---|---|---|---|
| Macintosh 2006 [11] | 652 | 3(2–6) | 33.5(30–37) | 7.0(6.1–7.1) | O = 62% | 50.8% | 24.8% | 29.4% | CA 4.3% SB 29.2‰ PND 32.3‰ ND 9.5‰ LGA 13.9% | UK CEMACH |
| Lapolla 2008 [12] | 164 | 5.7(5.9) | 33.2 (4.8) | 6.6(1.7) | 28.1(6.4) | NA | 29.1% | NA | Miscarriage 10.7% ND 1.9% SB 1.9% CA 2.0% Macrosomia 11.8% | Italy |
| Owens 2015 [13] | 108 | 4.3(3.8) | 33.7(4.8) | 6.9(1.7) | 34.9(6.7) | 70% | 34% | 55% | Miscarriage 8.3% SB 1.9% CA 2.8% LGA 20% SGA 5.6% | Ireland ATLANTIC DIP |
| Murphy 2017 [14] | 1386 | 4.8(4.3) | 33.6(5.2) | 6.8 | 33.3(7.3) | 46% | NA | 22.5% | CA 34.6‰ ND 11.4‰ SB 10.5‰ PTD 21.7% LGA 23.9% | UK |
| Maple-Brown 2019 [15] | 175 (NI 23 I 152) | NA | NI = 33.6(5.6) I = 31.1(5.6) | NI = 6.9(1.8) I = 7.8(2.0) | NI = 30.3(7.6)I = 31.3(5.7) | NA | NA | NA | CA NI = 4.2 vs. I = 4.6% LGA NI = 27.3 vs. I = 39.5% SGA NI = 18.2 vs. I = 6.9% | Australia PANDORA |
| Ali 2020 [16] | 50 | 5.49(4.4) | 35.5(3.8) | NA | 32.6(8.1) | 59% | 46% | 64% | Intrauterine fetal death 8.1% CA 2.7% Miscarriage 18.3% Macrosomia ≥ 4000 g 30% | Ireland |
| Lopez de Andres 2020 [8] | 4391 | NA | 34.17(5.42) | NA | 10.79% | NA | NA | NA | PTD 15.03% | Spain |
| Nadeau 2020 [17] | 160 | NA | IR 29.1(6.4) Non IR 30.6(5.5) | IR 8.4(2.0) Non IR 7.3(1.9) | IR 38.6(9.2) Non IR 36.6(8.2) | IR 28% Non IR19% | NA | NA | PTD IR 23% NON-IR 25% SB IR 1% NON-IR 2% CA IR 6% NON-IR 6% LGA IR 20% NON-IR 32% SGA IR 3% NON-IR 4% | USA 2 groups according to insulin resistance |
| Murphy 2021 [18] | 8685 | 3(0–10) | 34 (22–37) | 6.9 | 32.5 (24.8–43.0) ≥30 = 65% | 43.2% | NA | 22.3% | PTD 23.4% SB 13.5‰ ND11.2‰ CA 40.5‰ LGA 26.2% SGA 14.1% | UK |
| Guarnotta 2021 [19] | 62 | 4.11(3.1) | 33.7(6.1) | NA | 31.4(6.7) | NA | NA | NA | PTD 19.1% Miscarriage 12.9% LGA 25.8% | Italy |
| Gualdani 2021 [20] | 606 | NA | 33.8(4.9) | NA | 28.1(6.3) | 78.3% | NA | NA | LGA 12.5% CA 0.9% PTD 25.6% | Italy |
| Newman 2021 [21] | 244 | 6.8(6.3) | 34.3(5.7) | 6.7(3.5) | 32.5(6.9) | 61.1% | 29.5% | 49.6% | SB 0.4% PTD 22.4% CA 3.9% | Ireland |
| Newman 2022 [22] | 374 | 5.6(3.2) | 34.4(5.8) | 6.7(3.5) | 33.4 (7.6) | 63.6% | 25.9% | 36.1% | SB 0.8% Miscarriage 15.6% PTD 20.7% CA 5.1% | Ireland |
| Pylypjuk C 2021 [23] | 112 | NA | 22 (19–25.5) | 9.3 (7.8–10.9) | 27.5 (26.9–28.6) O = 39.6% | NA | NA | NA | Miscarriage 27.7% SB 11.6% NND 3.6% Shoulder distocia 13.1% CS 41% LGA 55.4% CA 19.6% | Canada |
| Today study 2022 [24] | 141 (260 pregnancies) | 8.1(3.2) | 21.5(3.16) | 8.7(2.78) | 35.6 (7.16) | 15% | 20% | NA | Miscarriage 25.3% PTD 23.8% Fetal death 3.7% CA 10% | USA |
| Identify type 2 diabetes as soon as possible in high risk women |
| Inform all type 2 diabetic women of childbearing age about the risk of an unplanned pregnancy at diagnosis and at each visit |
| Inform all type 2 diabetic women of childbearing age about the recommended HbA1c at conception in order to reduce congenital anomalies |
| Inform all type 2 diabetic women of childbearing age about the risks during pregnancy related to overweight and obesity |
| Screen diabetes complications before pregnancy |
| Modify diabetic therapy before conception |
| Stop statin if used |
| Modify antihypertensive therapy if used |
| Loss of 5–10% body weight if overweight or obese before pregnancy |
| Nutrition education |
| SBGM monitoring education |
| Considering starting FGM or CGM |
| Agree with the women on the timing of conception |
| Start folic acid at least one month before conception |
| Use safe contraception until the best clinical-metabolic conditions for conception are achieved |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalfrà, M.G.; Burlina, S.; Lapolla, A. Pregnancy and Type 2 Diabetes: Unmet Goals. Endocrines 2023, 4, 366-377. https://doi.org/10.3390/endocrines4020028
Dalfrà MG, Burlina S, Lapolla A. Pregnancy and Type 2 Diabetes: Unmet Goals. Endocrines. 2023; 4(2):366-377. https://doi.org/10.3390/endocrines4020028
Chicago/Turabian StyleDalfrà, Maria Grazia, Silvia Burlina, and Annunziata Lapolla. 2023. "Pregnancy and Type 2 Diabetes: Unmet Goals" Endocrines 4, no. 2: 366-377. https://doi.org/10.3390/endocrines4020028
APA StyleDalfrà, M. G., Burlina, S., & Lapolla, A. (2023). Pregnancy and Type 2 Diabetes: Unmet Goals. Endocrines, 4(2), 366-377. https://doi.org/10.3390/endocrines4020028