
Extremely Rare Pathologies of the Craniovertebral Junction Region: A Case Series and Review of the Literature

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
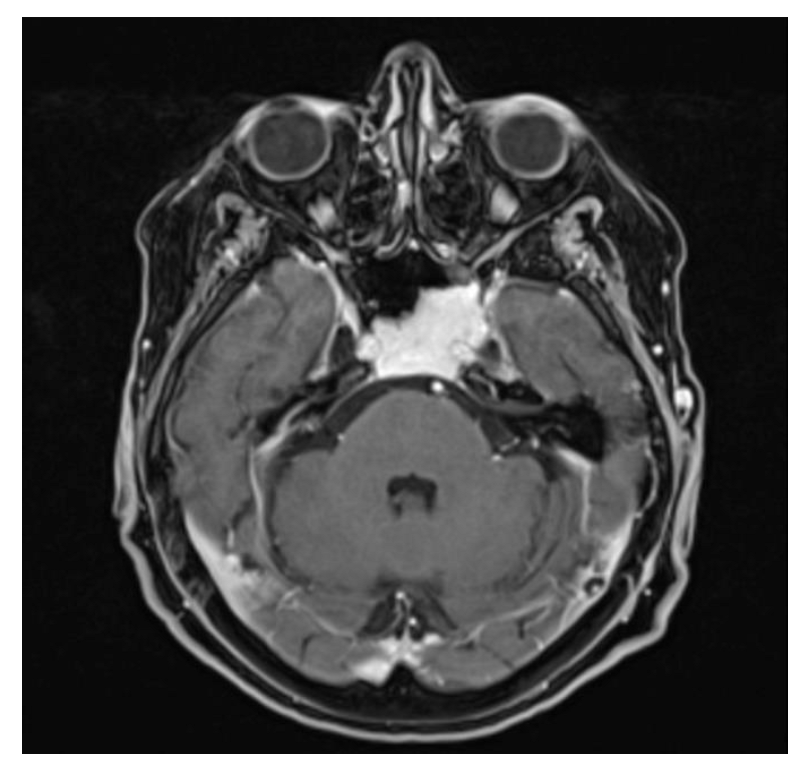
3.1. Case 1—Clival Osteoradionecrosis
3.2. Case 2—Ecchordosis Physaliphora
3.3. Case 3—Hepatocellular Carcinoma Metastasis
3.4. Case 4—Capillary Hemangioma
3.5. Case 5—Embryonal Rhabdomyosarcoma
3.6. Case 6—Cholesterol Granuloma
3.7. Case 7—Extradural Meningioma
3.8. Case 8—Ganglion Cyst
3.9. Case 9—Histiocytic Sarcoma
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kimura, F.; Kim, K.S.; Friedman, H.; Russell, E.J.; Breit, R.; Kimura, K.S.K.F.; Chaljub, G.; Van Fleet, R.; Guinto, F.C.; Crow, W.N.; et al. MR imaging of the normal and abnormal clivus. Am. J. Roentgenol. 1990, 155, 1285–1291. [Google Scholar] [CrossRef]
- Goel, A.; Cacciola, F. The Craniovertebral Junction, Diagnosis, Pathology, Surgical Techniques, 1st ed.; Thieme Medical Publishers, Inc.: Leipzig, Germany, 2011. [Google Scholar]
- Menezes, A.H. Decision Making for Management of Craniovertebral Junction Pathology. Oper. Tech. Neurosurg. 2005, 8, 125–130. [Google Scholar] [CrossRef]
- Tang, R.; Mao, S.; Li, D.; Ye, H.; Zhang, W. Treatment and Outcomes of Iatrogenic Cerebrospinal Fluid Leak Caused by Different Surgical Procedures. World Neurosurg. 2020, 143, e667–e675. [Google Scholar] [CrossRef]
- Lee, J.J.; Kim, H.Y.; Dhong, H.-J.; Chung, S.-K.; Kong, D.-S.; Nam, D.-H.; So, Y.K.; Hong, S.D. Delayed Cerebrospinal Fluid Leakage After Treatment of Skull Base Tumors: Case Series of 9 Patients. World Neurosurg. 2019, 132, e591–e598. [Google Scholar] [CrossRef]
- Ogawa, Y.; Tominaga, T. Delayed Cerebrospinal Fluid Leakage 10 Years after Transsphenoidal Surgery and Gamma Knife Surgery. Neurol. Med.-Chir. 2007, 47, 483–485. [Google Scholar] [CrossRef]
- Adel, M.; Chang, K.-P. Using a nasoseptal flap for the reconstruction of osteoradionecrosis in nasopharyngeal carcinoma: A case report. J. Otolaryngol.-Head Neck Surg. 2016, 45, 27. [Google Scholar] [CrossRef]
- Korchi, A.M.; Garibotto, V.; Lovblad, K.-O.; Haller, S.; Weber, D.C. Radiologic Patterns of Necrosis After Proton Therapy of Skull Base Tumors. Can. J. Neurol. Sci./J. Can. Sci. Neurol. 2013, 40, 800–806. [Google Scholar] [CrossRef]
- Hongmei, Y.; Zhe, W.; Jing, W.; Daokui, W.; Peicheng, C.; Yongjie, L. Delayed cerebrospinal fluid rhinorrhea after gamma knife surgery in a patient with a growth hormone-secreting adenoma. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2012, 19, 900–902. [Google Scholar] [CrossRef]
- Risso, A.; Zoia, C.; Gianformaggio, C.; Pagella, F.; Pusateri, A.; Benazzo, M.; Gaetani, P. Tension pneumocephalus secondary to osteoradionecrosis of the clivus. Rep. Pract. Oncol. Radiother. J. Greatpoland Cancer Cent. Pozn. Pol. Soc. Radiat. Oncol. 2016, 21, 71–75. [Google Scholar] [CrossRef]
- Marx, R.E. Osteoradionecrosis: A new concept of its pathophysiology. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 1983, 41, 283–288. [Google Scholar] [CrossRef]
- Wood, J.; Halen, J.V.; Samant, S.; Florendo, N. Radiation-induced sarcoma masquerading as osteoradionecrosis: Case report and literature review. J. Laryngol. Otol. 2015, 129, 279–282. [Google Scholar] [CrossRef]
- Veiceschi, P.; Arosio, A.D.; Agosti, E.; Bignami, M.; Pistochini, A.; Cerati, M.; Castelnuovo, P.; Locatelli, D. Symptomatic ecchordosis physaliphora of the upper clivus: An exceedingly rare entity. Acta Neurochir. 2021, 163, 2475–2486. [Google Scholar] [CrossRef]
- Vilela, M.D.; Pedrosa, H.A.; Filho, M.A.D. A Hemorrhagic Clival Chordoma with a Long Progression-Free Survival. World Neurosurg. 2017, 105, 1042.e1–1042.e4. [Google Scholar] [CrossRef]
- Ahn, S.S.; Han, J. Ecchordosis physaliphora presenting with abducens nerve palsy. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2016, 20, 266–268. [Google Scholar] [CrossRef]
- Ghimire, P.; Shapey, J.; Bodi, I.; Connor, S.; Thomas, N.; Barkas, K. Spontaneous tension pneumocephalus and pneumoventricle in ecchordosis physaliphora: Case report of a rare presentation and review of the literature. Br. J. Neurosurg. 2019, 34, 537–542. [Google Scholar] [CrossRef]
- Derakhshani, A.; Livingston, S.; William, C.; Lieberman, S.; Young, M.; Pacione, D.; Dehkharghani, S. Spontaneous, Intrasphenoidal Rupture of Ecchordosis Physaliphora with Pneumocephalus Captured During Serial Imaging and Clinical Follow-Up: Pathoanatomic Features and Management. World Neurosurg. 2020, 141, 85–90. [Google Scholar] [CrossRef]
- Sun, R.; Ajam, Y.; Campbell, G.; Masel, T. A Rare Case of Ecchordosis Physaliphora Presenting With Headache, Abducens Nerve Palsy, and Intracranial Hypertension. Cureus 2020, 12, e8843. [Google Scholar] [CrossRef]
- Otsuka, N.; Fukunaga, M.; Morita, K.; Ono, S.; Nagai, K.; Tomomitsu, T.; Yanagimoto, S.; Mimura, H.; Yamamoto, S.; Hirano, Y. Accumulation of99mTc-HM-PAO in photon deficient areas in bone scan of bone metastasis from hepatocellular carcinoma. Ann. Nucl. Med. 1992, 6, 215–220. [Google Scholar] [CrossRef]
- Aung, T.H.; Po, Y.C.; Wong, W.K. Hepatocellular carcinoma with metastasis to the skull base, pituitary gland, sphenoid sinus, and cavernous sinus. Hong Kong Med. J. Xianggang Yi Xue Za Zhi 2002, 8, 48. [Google Scholar]
- Escarda, A.; Vaquer, P.; Bonet, L.; Miralbés, S.; Gómez, C.; Obrador, A. Clivus metastasis from hepatocarcinoma associated with transarterial hepatic chemoembolization]. Gastroenterol. Y Hepatol. 2006, 29, 401–404. [Google Scholar] [CrossRef]
- Kim, S.R.; Kanda, F.; Kobessho, H.; Sugimoto, K.; Matsuoka, T.; Kudo, M.; Hayashi, Y. Hepatocellular carcinoma metastasizing to the skull base involving multiple cranial nerves. World J. Gastroenterol. 2006, 12, 6727–6729. [Google Scholar] [CrossRef]
- Kim, S.J.; Kim, H.J.; Lee, H.W.; Choi, C.H.; Kim, J.U.; Do, J.H.; Kim, J.K.; Chang, S.K. Hepatocellular carcinoma with metastasis to the cavernous sinus of skull base causing pto-sis. Korean J. Gastroenterol. = Taehan Sohwagi Hakhoe Chi 2008, 52, 389–393. [Google Scholar] [PubMed]
- Isaka, T.; Nakagawa, H.; Suzuki, T.; Yamada, J.; Wada, K.; Kadota, T. Successful Removal of a Giant Skull Base Metastasis from Hepatocellular Carcinoma after Direct Ethanol Injection: Case Report. J. Neurol. Surg. Part B Skull Base 2000, 10, 081–086. [Google Scholar] [CrossRef]
- Pallini, R.; Sabatino, G.; Doglietto, F.; Lauretti, L.; Fernandez, E.; Maira, G. Clivus metastases: Report of seven patients and literature review. Acta Neurochir. 2009, 151, 291–296. [Google Scholar] [CrossRef]
- Trivedi, P.; Gupta, A.; Pasricha, S.; Agrawal, G.; Shah, M. Isolated Skull Base Metastasis as the First Manifestation of Hepatocellular Carcinoma—A Rare Case Report with Review of Literature. J. Gastrointest. Cancer 2009, 40, 10–14. [Google Scholar] [CrossRef]
- Tamura, T.; Kawamura, Y.; Ikeda, K.; Seko, Y.; Fukushima, T.; Kumada, H.; Yamada, S.; Matumaru, Y. Hepatocellular carcinoma metastasis to the brain mimicking primary pituitary tumor around the sella turcica. Clin. J. Gastroenterol. 2013, 6, 319–325. [Google Scholar] [CrossRef]
- Cathel, A.; Khan, Y.R.; Blais, D.; Mahato, B.; Mahato, D. Metastatic Disease to Clivus: Biopsy or Not? Cureus 2019, 11, e5658. [Google Scholar] [CrossRef]
- Carey, R.A.B.; Nathaniel, S.; Das, S.; Sudhakar, S. Cavernous sinus syndrome due to skull base metastasis: A rare presentation of hepatocellular carcinoma. Neurol. India 2015, 63, 437. [Google Scholar] [CrossRef]
- Ram, A.; Paul, R.; Viswam, V.; Aravind, B. A Trigeminal Neuropathy From an Inactive Hepatocellular Carcinoma. Cureus 2021, 13, e20340. [Google Scholar] [CrossRef]
- Höpfel-Kreiner, I. Histogenesis of Hemangiomas—An Ultrastructural Study on Capillary and Cavernous Hemangiomas of the Skin. Pathol.-Res. Pract. 1980, 170, 70–90. [Google Scholar] [CrossRef]
- Smoller, B.R.; Apfelberg, D.B. Infantile (juvenile) capillary hemangioma: A tumor of heterogeneous cellular elements. J. Cutan. Pathol. 1993, 20, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.I.; Mural, M.; Rubino, F.; Lopez, E.S.; Cervio, A.; Olvi, L. Clivus Hemangioma in a Pediatric Patient: Case Report. World Neurosurg. 2019, 130, 512–515. [Google Scholar] [CrossRef]
- Moravan, M.; Petraglia, A.L.; Almast, J.; Yeaney, G.A.; Miller, M.C.; Vates, G.E. Intraosseous hemangioma of the clivus: A case report and review of the literature. J. Neurosurg. Sci. 2012, 56, 255–259. [Google Scholar] [PubMed]
- Grosu, A.L.; Nieder, C. Stereotactic Fractionated Radiotherapy for Recurrent Capillary Hemangioma of the Cavernous Sinus. Strahlenther. Onkol. Organ Der Dtsch. Rontgenges. 2006, 182, 179–182. [Google Scholar] [CrossRef]
- Tsao, M.N.; Schwartz, M.L.; Bernstein, M.; Halliday, W.C.; Lightstone, A.W.; Hamilton, M.G.; Jaywant, S.; Laperriere, N.; Almaghrabi, N.A.; Almaghrabi, A.; et al. Capillary hemangioma of the cavernous sinus. J. Neurosurg. 2003, 98, 169–174. [Google Scholar] [CrossRef]
- Morace, R.; Marongiu, A.; Vangelista, T.; Galasso, V.; Colonnese, C.; Giangaspero, F.; Innocenzi, G.; Esposito, V.; Cantore, G. Intracranial Capillary Hemangioma: A Description of Four Cases. World Neurosurg. 2012, 78, 191.e15–191.e21. [Google Scholar] [CrossRef]
- Jawad, N.; McHugh, K. The clinical and radiologic features of paediatric rhabdomyosarcoma. Pediatr. Radiol. 2019, 49, 1516–1523. [Google Scholar] [CrossRef]
- Unsal, A.A.; Chung, S.Y.; Unsal, A.B.; Baredes, S.; Eloy, J.A. A Population-Based Analysis of Survival for Sinonasal Rhabdomyosarcoma. Otolaryngol.-Head Neck Surg. 2017, 157, 142–149. [Google Scholar] [CrossRef]
- Larson, J.H.B.; Rutledge, R.P.-C.; Hunnell, L.P.-C.; Choi, D.K.; Kellogg, R.G.; Naran, S. Nasal Embryonal Rhabdomyosarcoma in the Pediatric Population: Literature Review and Report of Midline Presentation. Plast. Reconstr. Surg.-Glob. Open 2021, 9, e3534. [Google Scholar] [CrossRef]
- Li, X.; Peng, J.; Liu, Z.; Cui, Z.; Zhang, P.; Jin, H. Clinical analysis of 35 cases of adult rhabdomyosarcoma of nasal cavity and sinuses. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi = J. Clin. Otorhinolaryngol. Head Neck Surg. 2020, 34, 223–226. [Google Scholar] [CrossRef]
- Zhang, X.; Ma, K.; Wang, J.; Wu, W.; Ma, L.; Huang, D. A Prospective Evaluation of the Combined Helical Tomotherapy and Chemotherapy in Pediatric Patients with Unresectable Rhabdomyosarcoma of the Temporal Bone. Cell Biochem. Biophys. 2014, 70, 103–108. [Google Scholar] [CrossRef]
- Talenti, G.; Picariello, S.; Robson, C.; Mertiri, L.; Russo, C.; Slater, O.; Bisdas, S.; Abate, M.E.; Perrotta, S.; Hewitt, R.; et al. Magnetic resonance features and cranial nerve involvement in pediatric head and neck rhabdomyosarcomas. Neuroradiology 2021, 63, 1925–1934. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Baek, H.J.; Yoon, T.M.; Lee, J.K.; Lim, S.C. Endoscopic transpterygoid approach to a mass in a child. Int. J. Pediatr. Otorhinolaryngol. 2018, 105, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Shrirao, N.; Mukherjee, B.; Krishnakumar, S.; Biswas, J. Cholesterol granuloma: A case series & review of literature. Graefe’s Arch. Clin. Exp. Ophthalmol. Albrecht Von Graefes Arch. Klin. Exp. Ophthalmol. 2015, 254, 185–188. [Google Scholar] [CrossRef]
- Isaacson, B. Cholesterol Granuloma and Other Petrous Apex Lesions. Otolaryngol. Clin. N. Am. 2015, 48, 361–373. [Google Scholar] [CrossRef] [PubMed]
- Emanuelli, E.; Ciorba, A.; Bianchini, C.; Bossolesi, P.; Stomeo, F.; Pelucchi, S. Transnasal endoscopic management of petrous apex and clivus selected lesions. Eur. Arch. Oto-Rhino-Laryngol. 2012, 270, 1747–1750. [Google Scholar] [CrossRef]
- Sade, B.; Batra, P.S.; Scharpf, J.; Citardi, M.J.; Lee, J.H. Minimally Invasive Endoscopic Endonasal Management of Skull Base Cholesterol Granulomas. World Neurosurg. 2012, 78, 683–688. [Google Scholar] [CrossRef]
- Hernández-Estrada, R.A.; Kshettry, V.R.; Vogel, A.N.; Curtis, M.T.; Evans, J.J. Cholesterol granulomas presenting as sellar masses: A similar, but clinically distinct entity from craniopharyngioma and Rathke’s cleft cyst. Pituitary 2016, 20, 325–332. [Google Scholar] [CrossRef]
- Lai, C.Y.A.L.; Salkade, P.R.; Chuah, K.L.; Sitoh, Y.Y. Extradural cervical spinal meningioma mimicking malignancy. J. Radiol. Case Rep. 2018, 12, 1–10. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, H.; Shao, H.; Wang, C. Primary extradural meningiomas in head: A report of 19 cases and review of literature. Int. J. Clin. Exp. Pathol. 2015, 8, 5624–5632. [Google Scholar] [PubMed]
- Bruder, M.; Cattani, A.; Gessler, F.; Droste, C.; Setzer, M.; Seifert, V.; Marquardt, G. Synovial cysts of the spine: Long-term follow-up after surgical treatment of 141 cases in a single-center series and comprehensive literature review of 2900 degenerative spinal cysts. J. Neurosurg. Spine 2017, 27, 256–267. [Google Scholar] [CrossRef]
- Miyazawa, R.; Miyawaki, S.; Yamada, K.; Amemiya, S.; Ikemura, M.; Hinata, M.; Uchikawa, H.; Shiode, T.; Kin, T.; Takai, K.; et al. Retro-odontoid Pseudotumor: Two Cases of Intradural Ganglion Cysts Arising from the Odontoid Process with Syringobulbia. World Neurosurg. 2020, 144, 148–153. [Google Scholar] [CrossRef]
- Theodotou, C.B.; Urakov, T.M.; Vanni, S. Atlantoaxial Synovial Cyst: Case Report and Literature Review. World Neurosurg. 2016, 92, 588.e7–588.e15. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, E.; Nakamura, S. Histiocytic Sarcoma: An Updated Literature Review Based on the 2008 WHO Classification. J. Clin. Exp. Hematop. 2013, 53, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hornick, J.L.; Jaffe, E.S.; Fletcher, C.D.M. Extranodal Histiocytic Sarcoma: Clinicopathologic analysis of 14 cases of a rare epithelioid malignancy. Am. J. Surg. Pathol. 2004, 28, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Perez, I.; Gokden, M.; Day, J.D.; Yaziji, H.; Pina-Oviedo, S. Primary histiocytic sarcoma of the clivus with focal extension into central nervous system and neurologic manifestations: First description at an unusual site with an overwhelming and rapid progression. Clin. Neuropathol. 2021, 41, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Liu, Y.; Wang, W.; Xu, F.-L. Histiocytic sarcoma of the neck: A case report. Mol. Clin. Oncol. 2018, 9, 54–57. [Google Scholar] [CrossRef]
- Lopez, A.J.; Scheer, J.K.; Leibl, K.E.; Smith, Z.A.; Dlouhy, B.J.; Dahdaleh, N.S. Anatomy and biomechanics of the craniovertebral junction. Neurosurg. Focus 2015, 38, E2. [Google Scholar] [CrossRef] [PubMed]
- Visocchi, M.; Signorelli, F.; Parrilla, C.; Paludetti, G.; Rigante, M. Multidisciplinary approach to the craniovertebral junction. Historical insights, current and future perspectives in the neurosurgical and otorhinolaryngological alliance. Acta Otorhinolaryngol. Ital. Organo Uff. Della Soc. Ital. Di Otorinolaringol. E Chir. Cervico-Facciale 2021, 41 (Suppl. S1), S51–S58. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | Sex | Symptoms | Technique | Type of Surgery | Histological Diagnosis | Complications | Neo/Adjuvant Therapy | Follw-Up | Status |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 36 | M | Drowsiness, cephalea, fever and aqueous rhinorrhea | EEA | Biopsy and CSF leak repair | Osteoradionecrosis | None | Yes | 36 months | Dead |
| 2 | 69 | F | Cephalea, aqueous rhinorrhea | EEA | Resection and CSF leak repair | Ecchordosis physaliphora | None | None | 24 months | Alive without disease |
| 3 | 78 | M | VI cranial nerve (cn) palsy | EEA | Biopsy and debulking | Localization of a hepatocarcinoma | None | Yes | 3 months | Dead |
| 4 | 78 | F | None—occasional finding at RMN | EEA | Biopsy | Capillary hemangioma | None | None | 60 months | Alive symptoms free |
| 5 | 7 | M | VI cn palsy, VII cn palsy | EEA | Biopsy | Embryonal rhabdomyosarcoma | None | Yes | 18 months | Alive, no progression |
| # 6 | 46 | M | Headache, photophobia | EEA | Resection | Cholesterol granuloma | None | None | 20 months | Alive without disease |
| # 7 | 36 | F | Cervical pain | EEA FLA | Biopsy Resection | Extradural meningioma | Temporary left hypoglossal nerve palsy and rhinolalia | None | 5 years | Alive without disease |
| # 8 | 75 | M | Right upper limb weakness | C1 hemilaminectomy | Resection | Ganglion cyst | None | None | 3 years | Alive without disease |
| # 9 | 47 | F | Neck pain | FLA | Resection and CVJ stabilization | Histiocytic sarcoma | None | Yes | 9 months | Alive |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maiorano, E.; Spena, G.; Sovardi, F.; Dehgani-Mobaraki, P.; Pagella, F.; Montalbetti, A.; Peppucci, E.; Grasso, C.; Zoia, C. Extremely Rare Pathologies of the Craniovertebral Junction Region: A Case Series and Review of the Literature. Surgeries 2023, 4, 420-433. https://doi.org/10.3390/surgeries4030042
Maiorano E, Spena G, Sovardi F, Dehgani-Mobaraki P, Pagella F, Montalbetti A, Peppucci E, Grasso C, Zoia C. Extremely Rare Pathologies of the Craniovertebral Junction Region: A Case Series and Review of the Literature. Surgeries. 2023; 4(3):420-433. https://doi.org/10.3390/surgeries4030042
Chicago/Turabian StyleMaiorano, Eugenia, Giannantonio Spena, Fabio Sovardi, Puya Dehgani-Mobaraki, Fabio Pagella, Andrea Montalbetti, Elisabetta Peppucci, Christian Grasso, and Cesare Zoia. 2023. "Extremely Rare Pathologies of the Craniovertebral Junction Region: A Case Series and Review of the Literature" Surgeries 4, no. 3: 420-433. https://doi.org/10.3390/surgeries4030042
APA StyleMaiorano, E., Spena, G., Sovardi, F., Dehgani-Mobaraki, P., Pagella, F., Montalbetti, A., Peppucci, E., Grasso, C., & Zoia, C. (2023). Extremely Rare Pathologies of the Craniovertebral Junction Region: A Case Series and Review of the Literature. Surgeries, 4(3), 420-433. https://doi.org/10.3390/surgeries4030042