
Advances in Simple and Chiral-HPLC Methods for Antiallergic Drugs and Chiral Recognition Mechanism

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. World Scenario
2.1. Asia
2.2. Europe
2.3. Australia
2.4. America
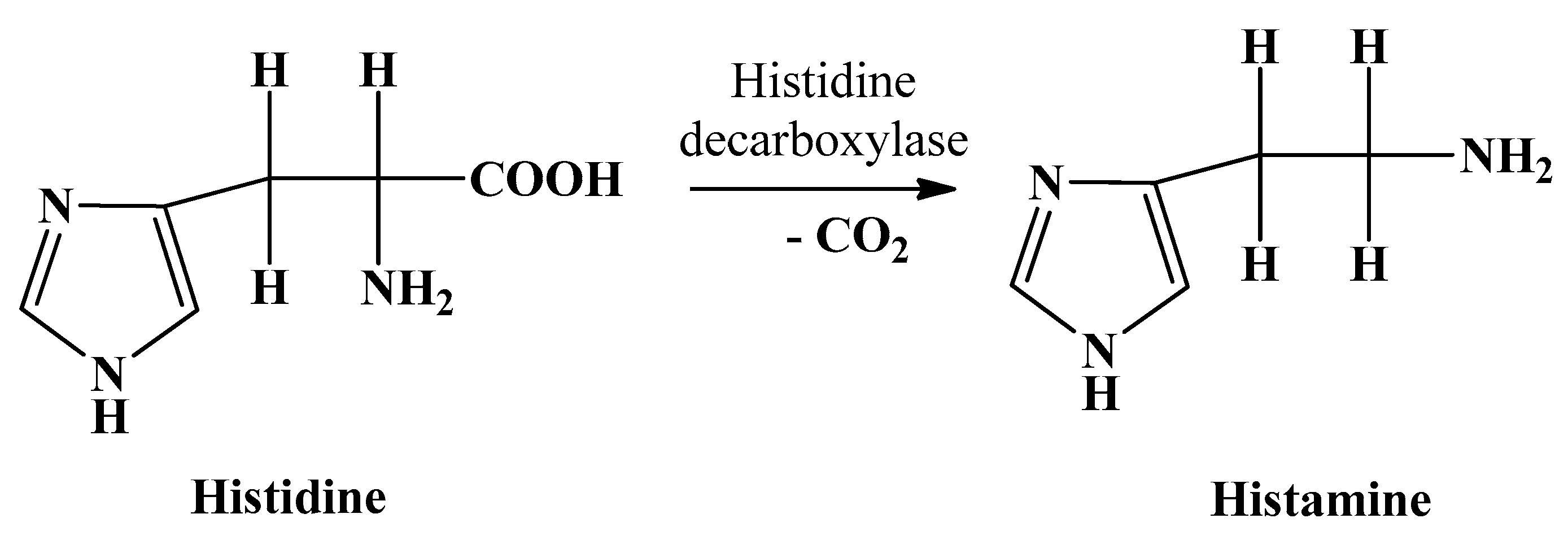
3. Causes of Allergy
4. Effect of Allergy on Economy
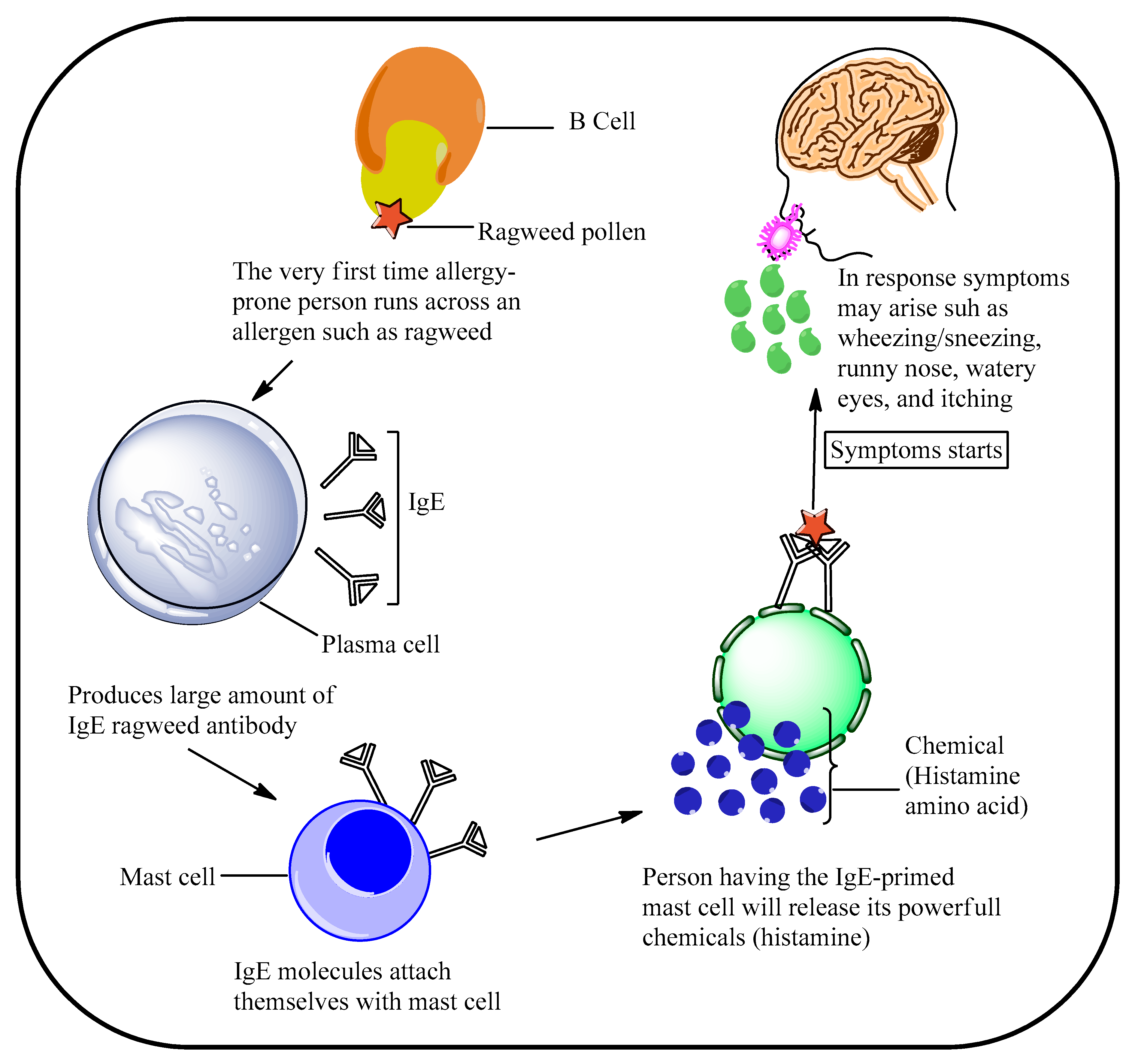
5. Mechanism of Allergy in Humans
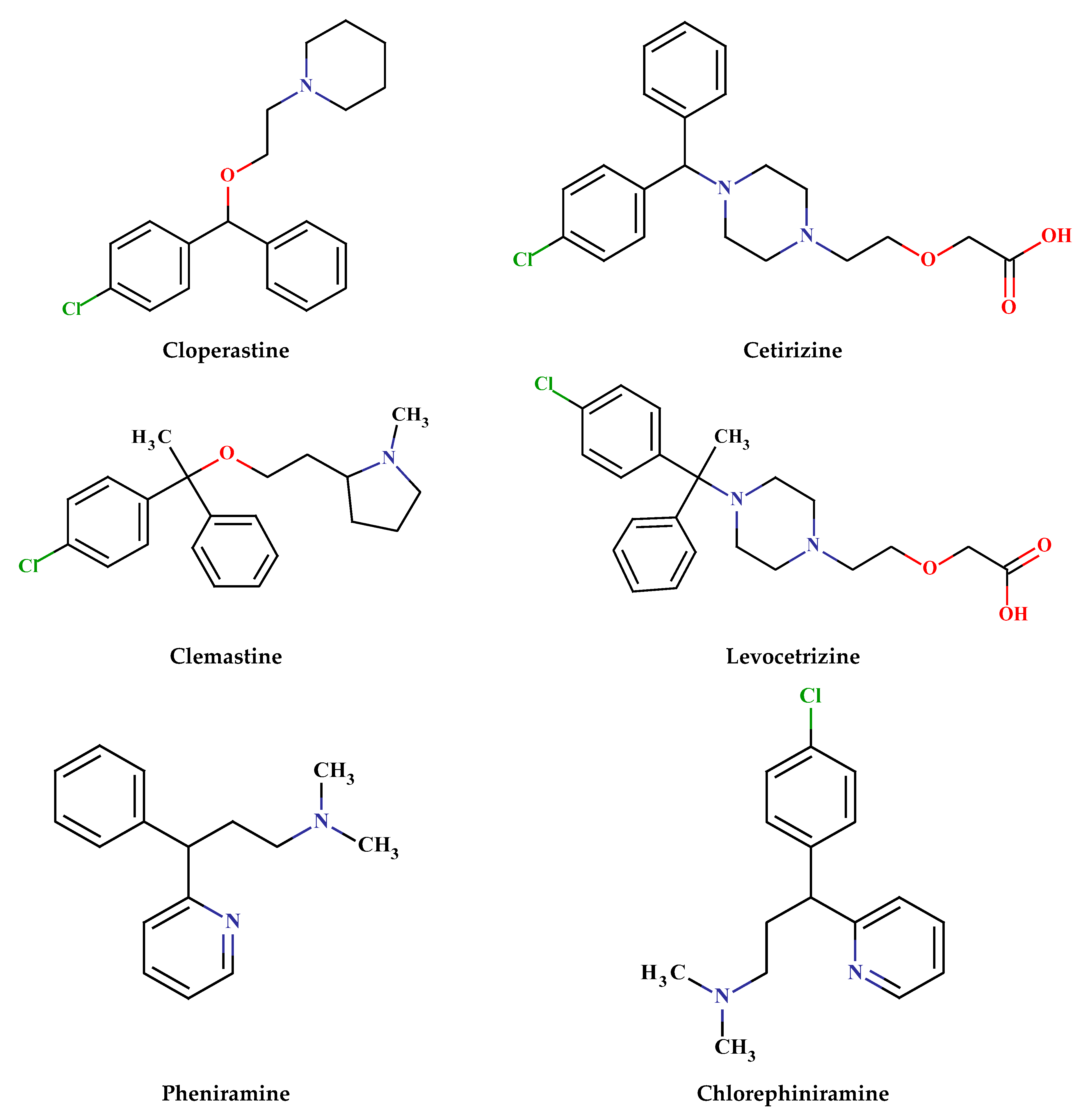
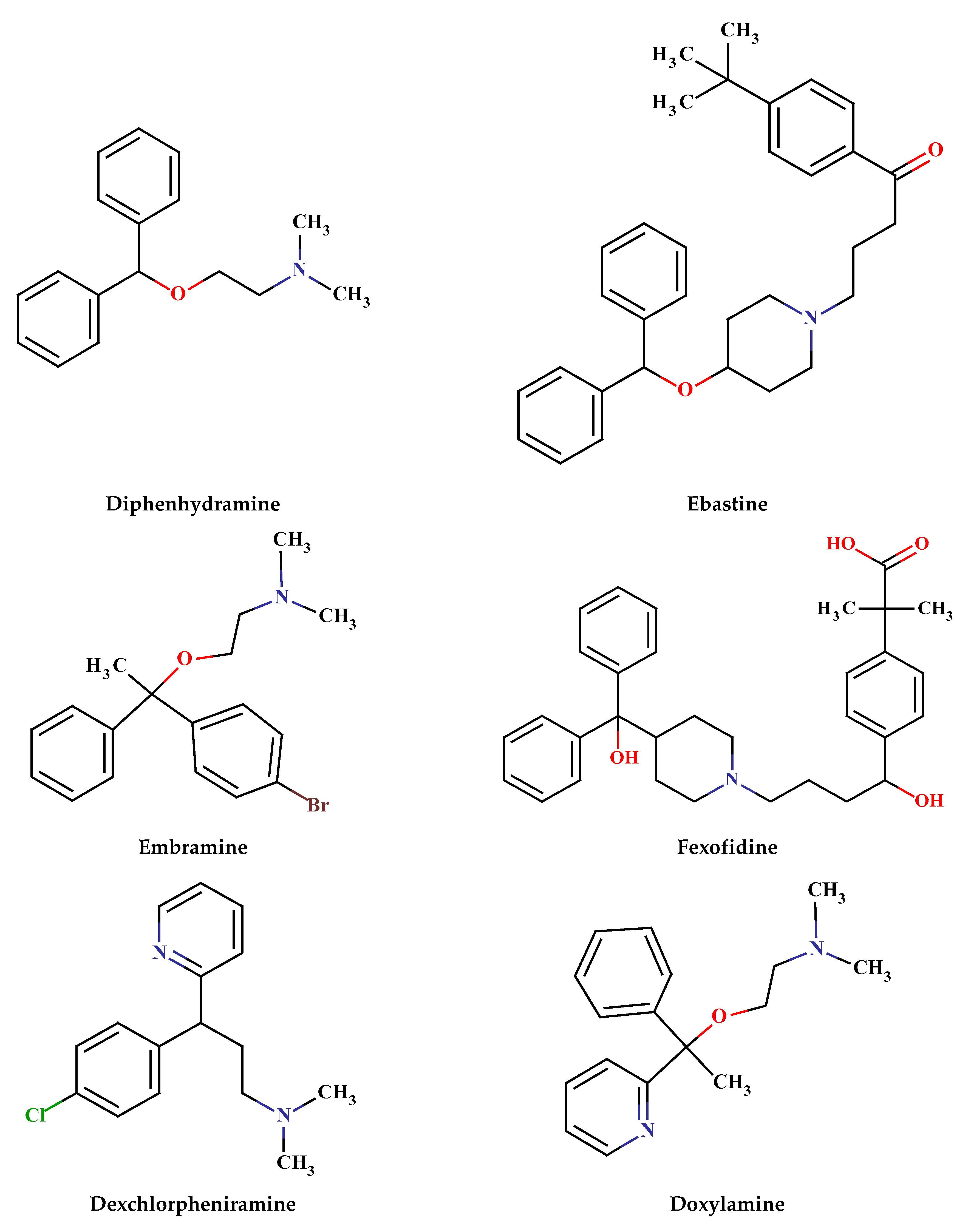
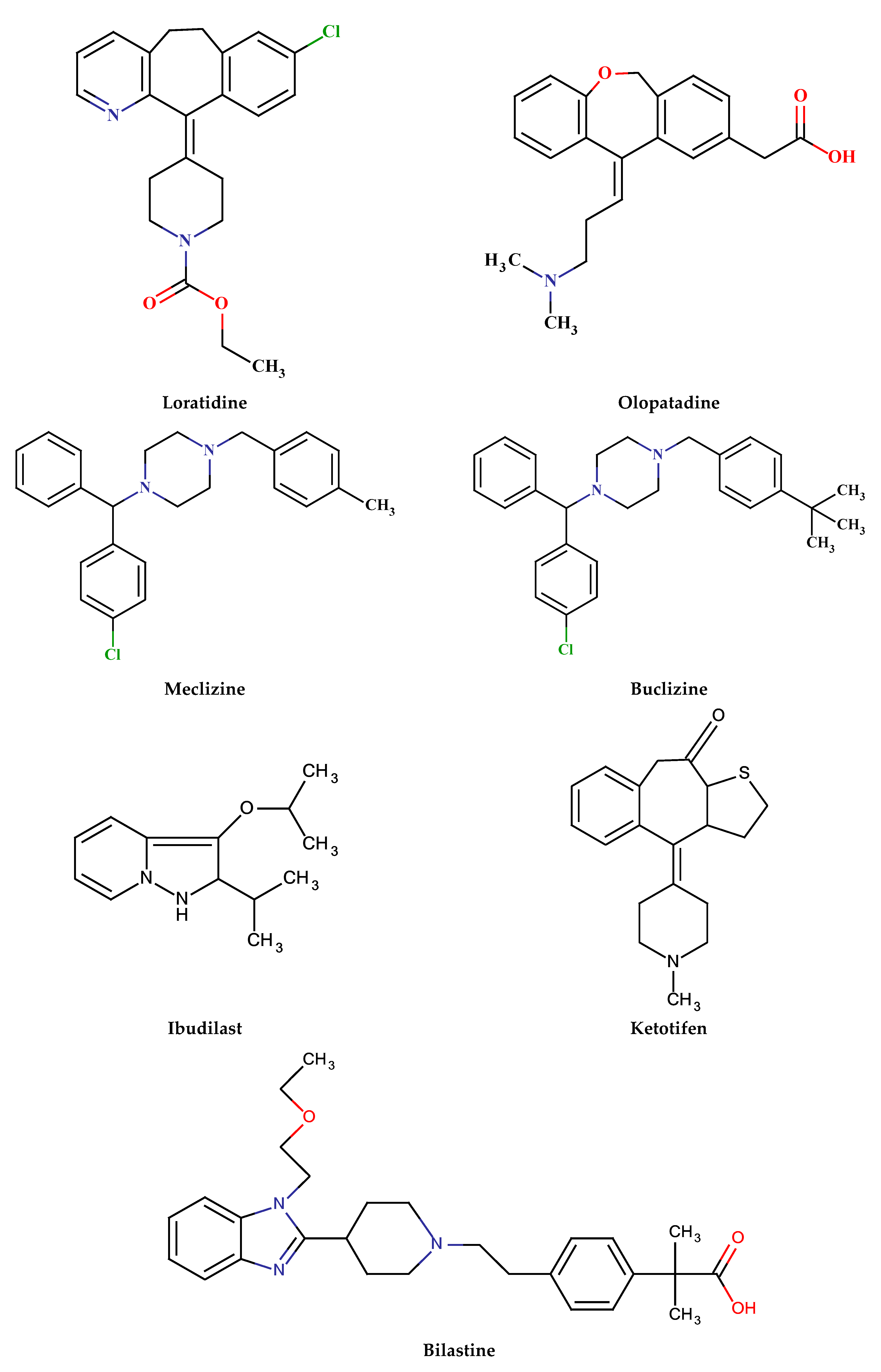
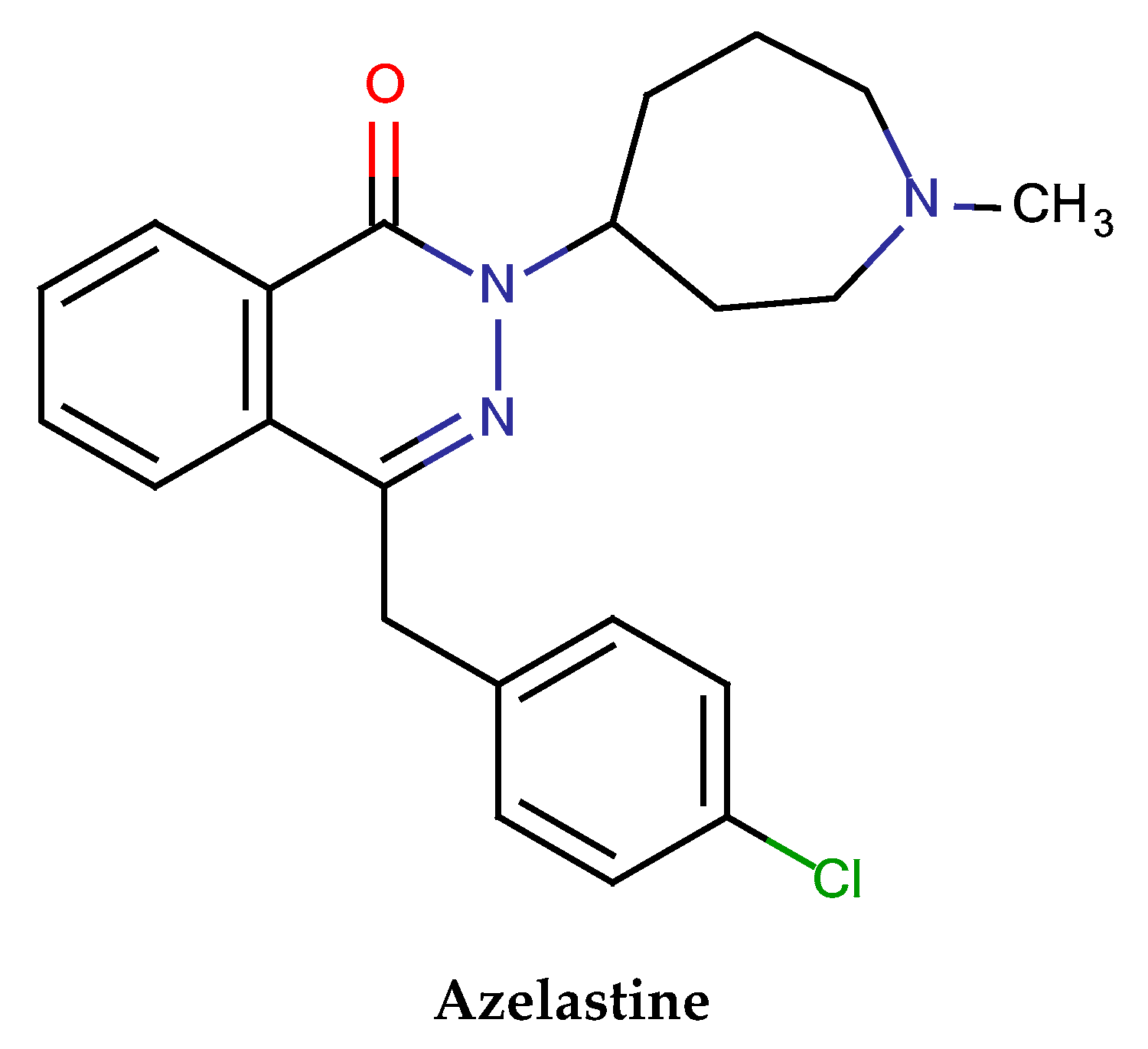
6. Classes of Antiallergic Drugs
6.1. Simple Drugs
6.2. Chiral Drugs
7. Analyses of Antiallergic Drugs by HPLC
7.1. Sample Preparation
7.2. Separation and Identification
7.2.1. Simple
7.2.2. Chiral
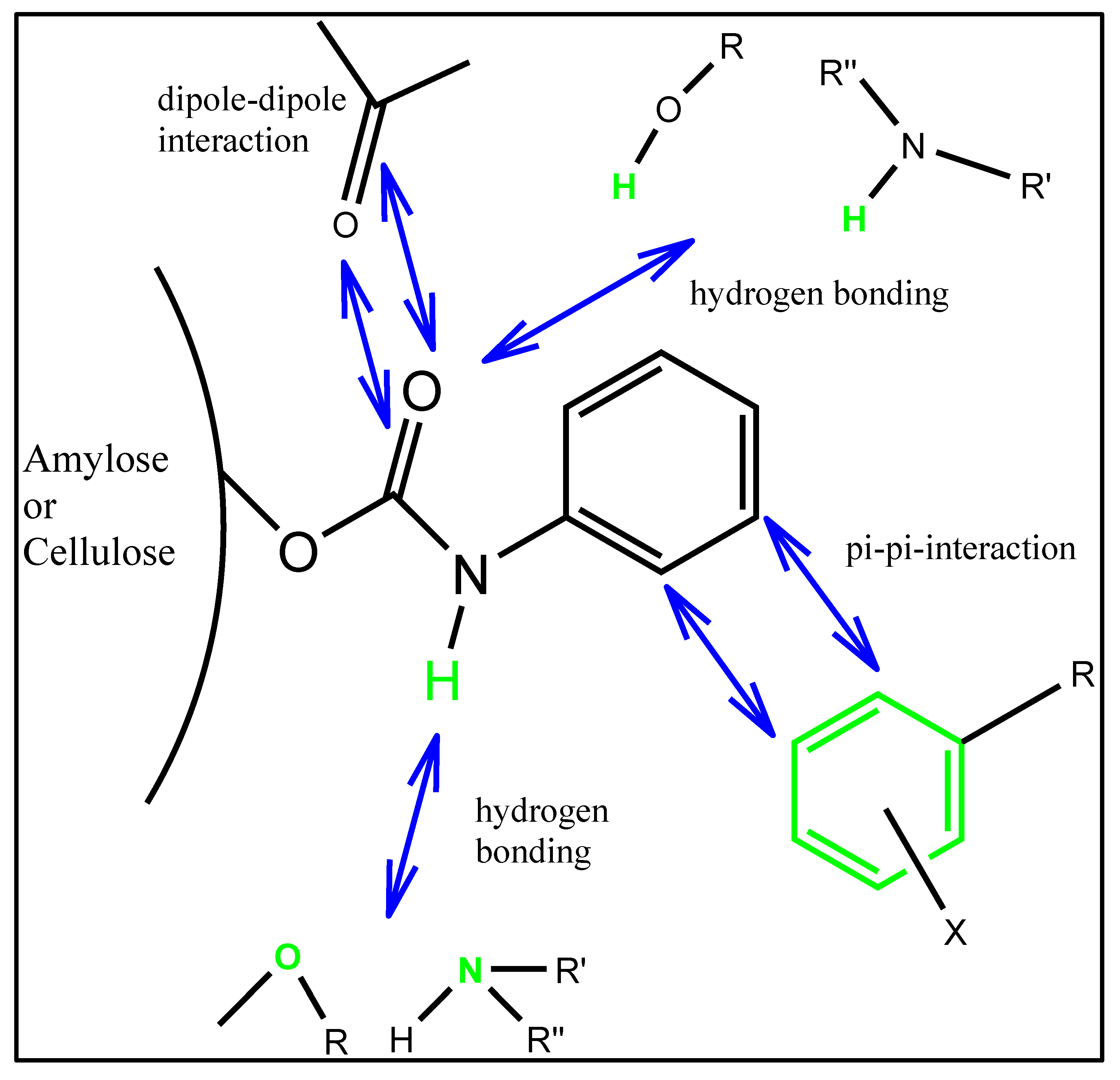
8. Chiral Recognition Mechanism
9. Future Perspectives
10. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Bielory, L. Ocular allergy overview. Immunol. Allergy Clin. N. Am. 2008, 28, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Bielory, L.; Meltzer, E.O.; Nichols, K.K.; Melton, R.; Thomas, R.K.; Bartlett, J.D. An algorithm for the management of allergic conjunctivitis. In Allergy and Asthma Proceedings; Oceanside Publications Inc.: East Providence, Rhode Island, 2013; Volume 34, pp. 408–420. [Google Scholar]
- Rogers, C.A.; Wayne, P.M.; Macklin, E.A. Interaction of the onset of spring and elevated atmospheric CO2 on ragweed (Ambrosia artemisiifolia L.) pollen production. Environ. Health Perspect. 2006, 114, 865–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, D. What Is an Allergic Reaction. Newsletter Healthline. 2017. Available online: http://www.healthline.com/health/allergies/allergic-reaction#Prevention7 (accessed on 20 January 2023).
- Liu, A.H. Hygiene theory and allergy and asthma prevention. Paediatr. Périnat. Epidemiol. 2007, 21, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Bielory, L.; Lyons, K.; Goldberg, R. Climate change and allergic disease. Curr. Allergy Asthma Rep. 2012, 12, 485–494. [Google Scholar] [CrossRef]
- Blando, J.; Bielory, L.; Nguyen, V.; Diaz, R.; Jeng, H.A. Anthropogenic Climate Change and Allergic Diseases. Atmosphere 2012, 3, 200–212. [Google Scholar] [CrossRef] [Green Version]
- Rosario, N.; Bielory, L. Epidemiology of allergic conjunctivitis. Curr. Opin. Allergy Clin. Immunol. 2011, 11, 471–476. [Google Scholar] [CrossRef]
- Pitt, A.D.; Smith, A.F.; Lindsell, L. Economic and quality-of-life impact of seasonal allergic conjunctivitis in Oxford shire. Ophthalmic Epidemiol. 2004, 11, 17–33. [Google Scholar] [CrossRef]
- Jacobson, M.Z. Enhancement of Local Air Pollution by Urban CO2 Domes. Environ. Sci. Technol. 2010, in press. [Google Scholar] [CrossRef]
- Ziska, L.H.; Epstein, P.R.; Rogers, C.A. Climate change, aerobiology and public health in the Northeast United States. Mitig. Adapt. Strateg. Glob. Chang. 2008, 13, 607–613. [Google Scholar] [CrossRef]
- Food Allergy: American College of Allergy, Asthma & Immunology. Available online: http://acaai.org/allergies/types/food-allergies (accessed on 20 January 2023).
- American Lung Association. Trends in Asthma Morbidity and Mortality. 2011. Available online: http://www.lung.org/finding-cures/our-research/epidemiology-and-statistics-rpts.html (accessed on 20 January 2023).
- Lee, A.J.; Thalayasingam, M.; Lee, B.W. Food allergy in Asia: How does it compare? Asia Pac. Allergy 2013, 3, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Nwaru, B.I.; Hickstein, L.; Panesar, S.S.; Roberts, G.; Muraro, A.; Sheikh, A. Prevalence of common food allergies in Europe: A systematic review and meta-analysis, on behalf of the EAACI Food Allergy and Anaphylaxis Guidelines Group. Allergy 2014, 69, 992–1007. [Google Scholar] [CrossRef]
- Mullins, R.J.; Clark, S.; Wiley, V.; Eyles, D.; Camargo, C.A., Jr. The Economic Impact of Allergic Disease in Australia: Not to Be Sneezed at; ASCIA/Access Economics Report; Access Economics: Sydney, Australia, 2007. [Google Scholar]
- Mullins, R.J.; Dear, K.; Tang, M.L. Characteristics of childhood peanut allergy in the Australian Capital Territory 1995–2007. J. Allergy Clin. Immunol. 2009, 123, 689–693. [Google Scholar] [CrossRef]
- Liew, W.K.; Williamson, E.; Tang, M.L. Anaphylaxis fatalities and admissions in Australia. J. Allergy Clin. Immunol. 2009, 123, 434–442. [Google Scholar] [CrossRef]
- Osborne, N.J.; Koplin, J.J.; Martin, P.E.; Gurrin, L.C.; Lowe, A.J.; Matheson, M.C.; Ponsonby, A.L.; Wake, M.; Tang, M.L.; Dharmage, S.C.; et al. Health Nuts Investigators. Prevalence of challenge-proven IgE-mediated food allergy using population-based sampling and predetermined challenge criteria in infants. J. Allergy Clin. Immunol. 2011, 127, 668–676. [Google Scholar] [CrossRef]
- Swarte, D.R. Drug allergy—Problems and strategies. J. Allergy Clin. Immunol. 1984, 74, 209–221. [Google Scholar]
- ASCIA Allergy in Australia A Submission for Allergic Diseases to be Recognized as a National Health Priority Area; ASCIA: Brookvale, NSW, Australia, 2014; pp. 1–15.
- Centers for Disease Control and Prevention. Fast Stats A to Z; CDC, National Center for Health Statistics: Hyattsville, MD, USA, 2009.
- Soni, A. Allergic rhinitis: Trends in use and expenditures, 2000 to 2005. In Statistical Brief #204; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- AAFA, Allergy Facts and Figures. Asthma and Allergy Foundation of America. The Oldest Asthma and Allergy Patient Group in the World. Available online: http://www.aafa.org/display.cfm?id=9&sub=30 (accessed on 6 July 2020).
- Staudt, A.; Glick, P.; Mizejewski, D.; Inkley, D. Extreme Allergies and Global Warming; National Wild Life Federation: Reston, VA, USA; Asthma and Allergy Foundation of America: Landover, MD, USA, 2010. [Google Scholar]
- Moscato, G.; Vandenplas, O.; Wijk, R.G.V.; Malo, J.; Perfetti, L.; Quirce, S.; Walusiak, J.; Castano, R.; Pala, G.; Gautrin, D.; et al. EAACI position paper on occupational rhinitis. Respir. Res. 2009, 10, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Galli, S.J.; Mindy, T.; Piliponsky, A.M. The development of allergic inflammation. Nature 2008, 454, 445–454. [Google Scholar] [CrossRef] [Green Version]
- Karasuyama, H.; Mukai, K.; Tsujimura, Y.; Obata-Ninomiya, K. Newly discovered roles for basophils: A neglected minority gains new respect. Nat. Rev. Immunol. 2009, 9, 9–13. [Google Scholar] [CrossRef]
- Sullivan, B.M.; Locksley, R.M. Basophils: A non redundant contributor to host immunity. Immunity 2009, 30, 12–20. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Pawliszyn, J. Headspace Solid-Phase Microextraction. J. Anal. Chem. 1993, 65, 1843–1852. [Google Scholar] [CrossRef]
- Zhang, Z.; Yang, M.J.; Pawliszyn, J. Solid-phase micro-extraction. A Solvent-Free Alternative for Sample Preparation. J. Anal. Chem. 1994, 66, 844A–853A. [Google Scholar] [CrossRef]
- Sabik, H.; Cooper, S.; Lafrance, P.; Fournier, J. Determination of atrazine, its degradation products and metolachlor in runoff water and sediments using solid-phase extraction. Talanta 1995, 42, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Chiron, S.; Dupas, S.; Scribe, P.; Barcelo, D. Application of on-line solid-phase extraction followed by liquid chromatogaraphy- thermospray mass spectrometry to the determination of pesticides in environmental waters. J. Chromatogr. A 1994, 665, 295–305. [Google Scholar] [CrossRef]
- Kealey, D.; Haines, P.J. Instant notes Analytical Chemistry. In BIOS Instant Notes in Analytical; BIOS Scientific Publishers Ltd.: Milton Park, UK, 2002. [Google Scholar]
- Hawthorne, S.B.; Miller, D.J.; Krieger, M.S. Coupled SFE-GC: A Rapid and Simple Technique for Extracting, Identifying, and Quantitating Organic Analytes from Solids and Sorbent Resins. J. Chromatogr. Sci. 1989, 27, 347–354. [Google Scholar] [CrossRef]
- Aboul-Enein, H.Y.; Ali, I. A comparison of chiral resolution of econazole, miconazole and sulconazole by HPLC using normal phase amylose CSPs. Fres. J. Anal. Chem. 2001, 370, 951–955. [Google Scholar] [CrossRef] [PubMed]
- Aboul-Enein, H.Y.; Ali, I.; Simons, C.; Gubitz, G. Enantiomeric resolution of the novel aromatase inhibitors by HPLC on cellulose and amylose based reversed and chiral stationary phases. Chirality 2000, 12, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Dewani, A.P.; Shelke, P.G.; Bakal, R.L.; Jaybhaye, S.S.; Chandewar, A.V.; Patra, S. Gradient HPLC-DAD Determination of Paracetamol Phenylephrine Hydrochloride, Cetirizine in Tablet Formulation. Drug Res. 2014, 64, 251–256. [Google Scholar] [CrossRef]
- Sher, N.; Siddiqui, F.A.; Hasan, N.; Shafi, N.; Zubair, A.; Mirza, A.Z. Simultaneous determination of antihistamine antiallergic drugs, cetirizine, domperidone, chlorphenamine maleate, loratadine, meclizine and buclizine in pharmaceutical formulations, human serum and pharmacokinetics application. Anal. Methods 2014, 6, 2704–2714. [Google Scholar] [CrossRef]
- Borges, P.F.; Lozano, P.P.; Montoya, E.G.; Miñarro, M.; Ticó, J.R.; Jo, E.; Negre JM, S. Determination of stress-induced degradation products of cetirizine dihydrochloride by a stability-indicating RP-HPLC method. DARU J. Pharm. Sci. 2014, 22, 82. [Google Scholar] [CrossRef]
- Souri, E.; Hatami, A.; Ravari, N.S.; Alvandifar, F.; Tehrani, M.B. Validating a Stability Indicating HPLC Method for Kinetic Study of Cetirizine Degradation in Acidic and Oxidative Conditions. Iran. J. Pharm. Res. 2013, 12, 287–294. [Google Scholar]
- Kumar, A.; Sharma, R.; Nair, A.; Saini, G. Development and Validation of RP-HPLC Method for Simultaneous Estimation of Nimesulide, Phenylephrine Hydrochloride, Chlorpheniramine Maleate and Caffeine anhydrous in Pharmaceutical dosage form. Acta. Pol. Pharm. Drug Res. 2012, 69, 1017–1022. [Google Scholar]
- Sujana, K.; Sankar, D.G.; Abbulu, K.; Souri, O.B. New validated RP-HPLC method for the determination of fexofenadine in bulk and dosage form. Der Pharm. Lett. 2012, 4, 1005–1009. [Google Scholar]
- Trivedi, R.K.; Patel, M.C.; Jadhav, S.B. A Rapid, Stability Indicating RP-UPLC Method for Simultaneous Determination of Ambroxol Hydrochloride, Cetirizine Hydrochloride and Antimicrobial Preservatives in Liquid Pharmaceutical Formulation. Sci. Pharm. 2011, 79, 525–543. [Google Scholar] [CrossRef] [Green Version]
- Sivasubramanian, L.; Lakshmi, K.S. Reverse phase-high performance liquid chromatographic method for the analysis of paracetamol, cetirizine and pseudoephedrine from tablets. Der Pharm. Chem. 2009, 1, 37–46. [Google Scholar]
- Karakus, S.; Kucukguzel, I.; Kucukguzel, S.G. Development and validation of a rapid RP-HPLC method for the determination of cetirizine or fexofenadine with pseudoephedrine in binary pharmaceutical dosage forms. J. Pharm. Biomed. Anal. 2008, 46, 295–302. [Google Scholar] [CrossRef]
- El-Sherbiny, D.T.; El-Enany, N.; Belal, F.; Hansen, S.H. Simultaneous determination of loratadine and desloratadine in pharmaceutical preparations using liquid chromatography with a micro emulsion as eluent. J. Pharm. Biomed. Anal. 2007, 43, 1236–1242. [Google Scholar] [CrossRef]
- Fujimaki, K.; Xiao-Pen, L.; Kumazawa, T.; Sato, J.; Sato, K. Determination of some antiallergic drugs in human plasma by direct-injection high-performance liquid chromatography-tandem mass spectrometry. Forensic Toxicol. 2006, 24, 8–16. [Google Scholar] [CrossRef]
- Songa, Q.; Junga, H.; Tang, Y.; Li, A.C.; Addison, T.; McCort-Tipton, M.; Beato, B.; Naidong, W. Automated 96-well solid phase extraction and hydrophilic interaction liquid chromatography-tandem mass spectrometric method for the analysis of cetirizine (ZYRTEC®) in human plasma-with emphasis on method ruggedness. J. Chromatogr. B 2005, 814, 105–114. [Google Scholar] [CrossRef]
- Qia, M.; Wang, P.; Geng, Y. Determination of desloratadine in drug substance and pharmaceutical preparations by liquid chromatography. J. Pharm. Biomed. Anal. 2005, 38, 355–359. [Google Scholar] [CrossRef]
- Liu, L.; Qi, M.; Wang, P.; Li, H. High-performance liquid chromatographic method for the bioequivalence evaluation of desloratadine fumarate tablets in dogs. J. Pharm. Biomed. Anal. 2004, 34, 1013–1019. [Google Scholar] [CrossRef]
- Jaber, A.M.Y.; Al-Sherife, H.A.; Al-Omari, M.M.; Badwan, A.A. Determination of cetirizine dihydrochloride, related impurities and preservatives in oral solution and tablet dosage forms using HPLC. J. Pharm. Biomed. Anal. 2004, 36, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Kunicki, P.K. Determination of loratadine in human plasma by high-performance liquid chromatographic method with ultraviolet detection. J. Chromatogr. B 2001, 755, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Prathyusha, P.; Sundararajan, R.; Bhanu, P.; Mukthinuthalapati, M.A. A new stability indicating RP-HPLC method for determination of Bilastine in bulk and pharmaceutical formulation. Res. J. Pharm. Technol. 2020, 13, 2849. [Google Scholar] [CrossRef]
- Patel, S.H.I.T.A.L.; Pasha, T.Y. Stability-Indicating High-Performance Liquid Chromatography method for determination of antihistamine drug azelastine. Asian J. Pharm. Clin. Res. 2018, 11, 248–251. [Google Scholar] [CrossRef]
- Alali, F.Q.; Tashtoush, B.M.; Najib, N.M. Determination of ketotifen in human plasma by LC-MS. J. Pharm. Biomed. Anal. 2004, 34, 87–94. [Google Scholar] [CrossRef]
- Li, A.C.; Junga, H.; Shou, W.Z.; Bryant, M.S.; Jiang, X.; Naidong, W. Direct injection of solid-phase extraction eluents onto silica columns for the analysis of polar compounds isoniazid and cetirizine in plasma using hydrophilic interaction chromatography with tandem mass spectrometry. Rapid Commun. Mass Spectrom. 2004, 18, 2343–2350. [Google Scholar] [CrossRef]
- Chen, X.; Zhong, D.; Liu, D.; Wang, Y.; Han, Y.; Gu, J. Determination of ketotifen and its conjugated metabolite in human plasma by liquid chromatography/tandem mass spectrometry: Application to a pharmacokinetic study. Rapid Commun. Mass Spectrom. 2003, 17, 2459–2463. [Google Scholar] [CrossRef]
- Fujita, K.; Magara, H.; Kobayashi, H. Determination of olopatadine, a new antiallergic agent, and its metabolites in human plasma by high-performance liquid chromatography with electrospray ionization tandem mass spectrometry. J. Chromatogr. B 1999, 731, 345–352. [Google Scholar] [CrossRef]
- Zeid, A.A.; Alwarthan, A.; Ali, I. Advances in enantiomeric resolution on chiral monolithic phases in liquid chromatography and electrochromatography. J. Sep. Sci. 2014, 37, 1033–1057. [Google Scholar]
- Ali, I.; Singh, P.; Aboul-Enein, H.Y.; Sharma, B. Chiral analysis of ibuprofen residues in water and sediment. Anal. Lett. 2009, 42, 1747–1760. [Google Scholar] [CrossRef]
- Ali, I.; Alothman, Z.; Nagae, N.; Gaitonde, V.D.; Dutta, K.K. Recent trends in ultrafast HPLC: New generation of superficially porous silica columns. J. Sep. Sci. 2013, 35, 3235–3249. [Google Scholar] [CrossRef]
- Ryu, J.K.; Yoo, S.D. Simultaneous Determination of Levocetirizine and Pseudoephedrine in Dog Plasma by Liquid Chromatography-Mass Spectrometry in the Presence of Dextrocetirizine. J. Pharm. Pharmaceut. Sci. 2012, 15, 519–527. [Google Scholar] [CrossRef] [Green Version]
- Rustichelli, C.; Gamberini, M.C.; Ferioli, V.; Gamberini, G. Enantioselective Analyses of Antihistaminic Drugs by High-Performance Liquid Chromatography. Chromatographia 2004, 60, 99–103. [Google Scholar] [CrossRef]
- Ali, I.; Al-Othman, Z.A.; Al-Warthan, A.; Alam, S.D.; Farooqi, J.A. Enantiomeric Separation and Simulation Studies of Pheniramine, Oxybutynin, Cetirizine and Brinzolamide Chiral Drugs on Amylose Based Columns. Chirality 2014, 26, 136–143. [Google Scholar] [CrossRef]
- Gokulakrishnanm, K.; Balamurugan, K. Validated HPLC method for the determination of enantiomeric impurity of d-pseudoephedrine sulfate. Int. J. Appl. Chem. 2009, 5, 85–91. [Google Scholar]
- Ozkırımlı, S.; Aboul-Enein, H.Y.; Nesrin, C. Enantioselective Quantification of Doxylamine in Human Plasma by HPLC. J. Liq. Chromatogr. Relat. Technol. 2011, 34, 671–678. [Google Scholar] [CrossRef]
- Paris, S.; Blaschke, G.; Locher, M.; Borbe, H.O.; Engel, J. Investigation antiasthmatic/antiallergic liquid chromatography of the stereoselective in vitro metabolism of the chiral drug flezelastine by high-performance and capillary zone electrophoresis. J. Chromatogr. B 1997, 691, 463–471. [Google Scholar] [CrossRef]
- Zhou, J.; Luo, P.; Chen, S.; Meng, L.; Sun, C.; Du, Q.; Sun, F. Enantioseparation of Six Antihistamines with Immobilized Cellulose Chiral Stationary Phase by HPLC. J. Chromatogr. Sci. 2016, 54, 531–535. [Google Scholar] [CrossRef] [Green Version]
- Yanru, L.; Bolin, Z.; Mengyao, X.; Zhen, J.; Xingjie, G. Studies on the chiral separation of pheniramine and its enantioselective pharmacokinetics in rat plasma by HPLC-MS/MS. Microchem. J. 2020, 156, 104989. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S.N. | Name of Drugs | Mobile Phase | Column | Other Conditions | Ref |
|---|---|---|---|---|---|
| 1 | Phenylephrine hydrochloride, paracetamol, and cetirizine hydrochloride | 10 mM phosphate buffer (pH 3.3) and acetonitrile | Phenomenex Kinetex-C18 | 1 mL/min at 230 nm; recoveries from 101 to 102.40% | [38] |
| 2 | Chlorphenamine maleate, loratadine, Cetirizine HCl, domperidone, buclizine, and meclizine | Heptane sulphonic acid salt buffer in water and MeCN | symmetry C18 | 1 mL/min at 230 nm; LOD from 0.52 ng/mL to 5.16 ng/mL | [39] |
| 3 | Cetirizine dihydrochloride | 0.2 M K2HPO4 (pH 7) and ACN (65:35, v/v) | Eclipse XDB C8 | 1 mL/min at 230 nm; LOD and LOQ were 0.25 and 0.056 μg/mL | [40] |
| 4 | Cetirizine dihydrochloride | 50 mM KH2PO4 and ACN (60:40, v/v) | Symmetry C18 | 1 mL/min at 230 nm; LOQ was 1 µg/mL. LOD) was 0.2 µg/mL with recovery of 99% | [41] |
| 5 | Nimesulide, phenylephrine hydrochloride, caffeine anhydrous, and chlorpheniramine maleate | Methanol and buffer (55:45, v/v, pH 5.5) | RP-Hypersil phenyl (4.6 mm × 25 cm) | 1 mL/min at 214 nm; LOD from 0.45 to 9.34 µg/mL; recovery from 99.03 to 100.30% | [42] |
| 6 | Fexofenadine | Buffer and Methanol (30:70, v/v) | Symmetry-C18 (150 × 4.6 mm), 5 μm | at 254 nm; LOD = 9.92 ng mL | [43] |
| 7 | Ambroxol hydrochloride, cetirizine hydrochloride, methylparaben, and propylparaben | 0.01 M phosphate buffer and 0.1% triethylamine as a solvent-A and ACN as a solvent-B (mixture of both) | Agilent Eclipse plus C18 (50 × 2.1 mm), 1.8 μm) | at 237 nm; LOQ from 0.12 to 0.18 µg/mL); recovery of more than 99% | [44] |
| 8 | Pseudoephedrine, Paracetamol, and Cetirizine | 25 mM Na2HPO4 (pH 5.0)-MeOH-ACN (30:60:10, v/v) | Hypersil C18 | 1 mL/min. at 240 nm; LOD from 0.836 to 2.512 | [45] |
| 9 | Pseudoephedrine, Fexofenadine, and Cetirizine | TEA solution (0.5%, pH 4.5) MeOH-ACN (50:20:30, v/v) | Zorbax-C8 (150 × 4.6 mm) 5 μm | 218 and 222 nm; LOD from 0.10 to 1.75 µg/mL; recovery 97.52 to 100.98% | [46] |
| 10 | Desloratadine HCl and Loratadine | 0.1 M SDS, 1% octanol, 10% n-propanol and 0.3% TEA in 0.02 M phosphoric acid, pH 3.0 | Cyano Propyl bonded stationary-phase | 1 mL/min at 247 nm; LOD was 0.8 and 0.2 µg/mL; LOQ was 2.3 and 0.6 µg/mL for both drugs | [47] |
| 11 | Ketotifen, olopatadine, cetirizine, and ibudilast | Acetonitrile-rich mobile phase | Polymer column (MSpak GF) | 0.2 mL/min at 260 nm; LOD = 0.5 ng/mL; recovery 51.7–95.5% | [48] |
| 12 | Cetirizine | ACN-water-CH3COOH-TFA (93:7:1:0.025, v/v) | Betasil silica (50 × 3, 5 m). | 0.5 mL/min; recoveries 84.5 to 88.0% | [49] |
| 13 | Desloratadine HCl | Methanol-0.03 M Heptane sulphonic acid sodium- Glacial acetic acid (70:30:4, v/v), | Diamonsil BDS C18 | 1 mL/min at 247 nm | [50] |
| 14 | Desloratadine HCl | MeOH-ACN-Phosphate buffer 0.01 mol/L (35:35:30, v/v) (pH-5.5) | Hypersil CN Column (150 mm × 5 mm), 5 μm | 0.8 mL/min at 241 nm; LOQ5.0 ng/mL | [51] |
| 15 | Cetirizine dihydrochloride | 0.05 M dihydrogen phosphate-ACN-MeOH-THF(12:5:2:1, v/v) | Hypersil BDS C18 (4.6 × 250 mm), 5 µm | 1 mL/min at 230 nm; LOD and LOQ were 0.10 and 0.34 µg/mL | [52] |
| 16 | Loratadine HCl | ACN-water-0.5 M KH2PO4-H3PO4 (440:480: 80:1, v/v) | Supelcosil LC18-DB column | 1 mL/min. at 200 nm; LOQ was 0.5 ng/mL | [53] |
| 17 | Bilastine | Formic acid and MeOH(1:1 ratio) | Gemini C18 column (150 × 4.6), 5 µm | 0.8 ml/min at 282 nm; LOD and LOQ were 0.08931 µg/mL and 0.27063 µg/mL | [54] |
| 18 | Azelastine | Potassium dihydrogen phosphate buffer and acetonitrile (50:50, v/v); | Spherisorb CN column (250 × 4.6 mm, 5-μm) | 1.0 mL/min at 290 nm; LOD and LOQ were 0.81 µg/mL and 2.44 µg/mL Recovery = 99 and 102% | [55] |
| S. N. | Drug Name | Mobile Phase | Column | Other Conditions | Ref |
|---|---|---|---|---|---|
| 1 | Levocetirizine and pseudoephedrine | 10 mM aqueous NH4OAc and acetonitrile (9:1, v/v) | Ultron ES-OVM chiral column | 1 mL/min; LOQ for levocetirizine 5.9–15.0% and 7.7–17.9% for pseudoephedrine | [61] |
| 2 | Terfenadine and fexofenadine | Isopropyl alcohol and n-hexane (5:95, v/v containing 0.01% diethylamine) | Chiralcel (250 mm × 4.6 mm, 5 µm) | 0.4 mL/min at 225 nm | [62] |
| 3 | Pheniramine and cetirizine | 2-PrOH-n-Hexane-DEA (15:85:0.1, v/v), and 2-PrOH-n-hexane-DEA (30:70:0.2, v/v) | AmyCoat (150 mm × 4 6 mm, 5 µm) and Chiralpak AD (250 × 4.6 mm, 5 µm) | 0.5 mL/min at 220 and 225 nm; LOD ranged from 1.0–2.5 ng/mL; LOQ were 5.0–10.0 ng/mL | [63] |
| 4 | Terfenadine and active metabolite fexofenadine | IPA and n-Hexane (5:95, v/v) containing 0.01% DEA | Chiralcel column | 0.4 mL/min at 225 nm | [64] |
| 5 | pheniramine, oxybutynin, cetirizine, and brinzolamide | n-hexane-2-propanol-DEA (85:15:0.1, v/v) and n-hexane-2-propanol-DEA (70:30:0.2, v/v) a | AmyCoat (150 mm × 4.6 mm) Chiralpak AD (250 mm × 4.6 mm id) | 0.5 mL/min at 220 and 225 nm | [65] |
| 6 | Pseudoephedrine Sulfate | n-Hexane- Isopropyl alcohol- ethanol-DEA (980:10:10:1, v/v) | Chiralpak AD-H column (250 mm × 4.6 mm, 5 µm) | 2.0 mL/min at 254 nm; LOD and LOQ were 0.04% and 0.16% | [66] |
| 7 | Doxylamine | Mobile phase consists of n-hexane-IAP-DEA (98:2:0.025, v/v) | Chiralpak AD-H column (250 mm × 4.6 mm, 5 µm) | 1.0 mL/min at 262 nm | [67] |
| 8 | Flezelastine | Mixture of n-Hexane-IPA-DEA (88:12:0.5, v/v) | Chiralpak AD column (250 mm x 4.6 mm, 10 µm) | 1.0 mL/min at 292 nm | [68] |
| 9 | Cetirizine, doxylamine and hydroxyzine | n-Hexane-ethanol-DEA (90:10:0.1, v/v); n-hexane-isopropanol-DEA (60:40:0.1, v/v); and n-hexane-isopropanol-DEA (90:10:0.1 v/v) | Chiralpak IC column | 0.8 mL/min at 227 and 262 nm | [69] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, I.; Alam, S.D.; Raja, R.; Khan, S.A.; Anjum, R.; Jain, A.K.; Aboul-Enein, H.Y.; Locatelli, M. Advances in Simple and Chiral-HPLC Methods for Antiallergic Drugs and Chiral Recognition Mechanism. Analytica 2023, 4, 66-83. https://doi.org/10.3390/analytica4010007
Ali I, Alam SD, Raja R, Khan SA, Anjum R, Jain AK, Aboul-Enein HY, Locatelli M. Advances in Simple and Chiral-HPLC Methods for Antiallergic Drugs and Chiral Recognition Mechanism. Analytica. 2023; 4(1):66-83. https://doi.org/10.3390/analytica4010007
Chicago/Turabian StyleAli, Imran, Syed Dilshad Alam, Rupak Raja, Shafat Ahmad Khan, Rushda Anjum, Arvind Kumar Jain, Hassan Y. Aboul-Enein, and Marcello Locatelli. 2023. "Advances in Simple and Chiral-HPLC Methods for Antiallergic Drugs and Chiral Recognition Mechanism" Analytica 4, no. 1: 66-83. https://doi.org/10.3390/analytica4010007
APA StyleAli, I., Alam, S. D., Raja, R., Khan, S. A., Anjum, R., Jain, A. K., Aboul-Enein, H. Y., & Locatelli, M. (2023). Advances in Simple and Chiral-HPLC Methods for Antiallergic Drugs and Chiral Recognition Mechanism. Analytica, 4(1), 66-83. https://doi.org/10.3390/analytica4010007