Covid19Risk.ai: An Open Source Repository and Online Calculator of Prediction Models for Early Diagnosis and Prognosis of Covid-19

 , ,
, , 
Abstract
:1. Introduction
2. Methods
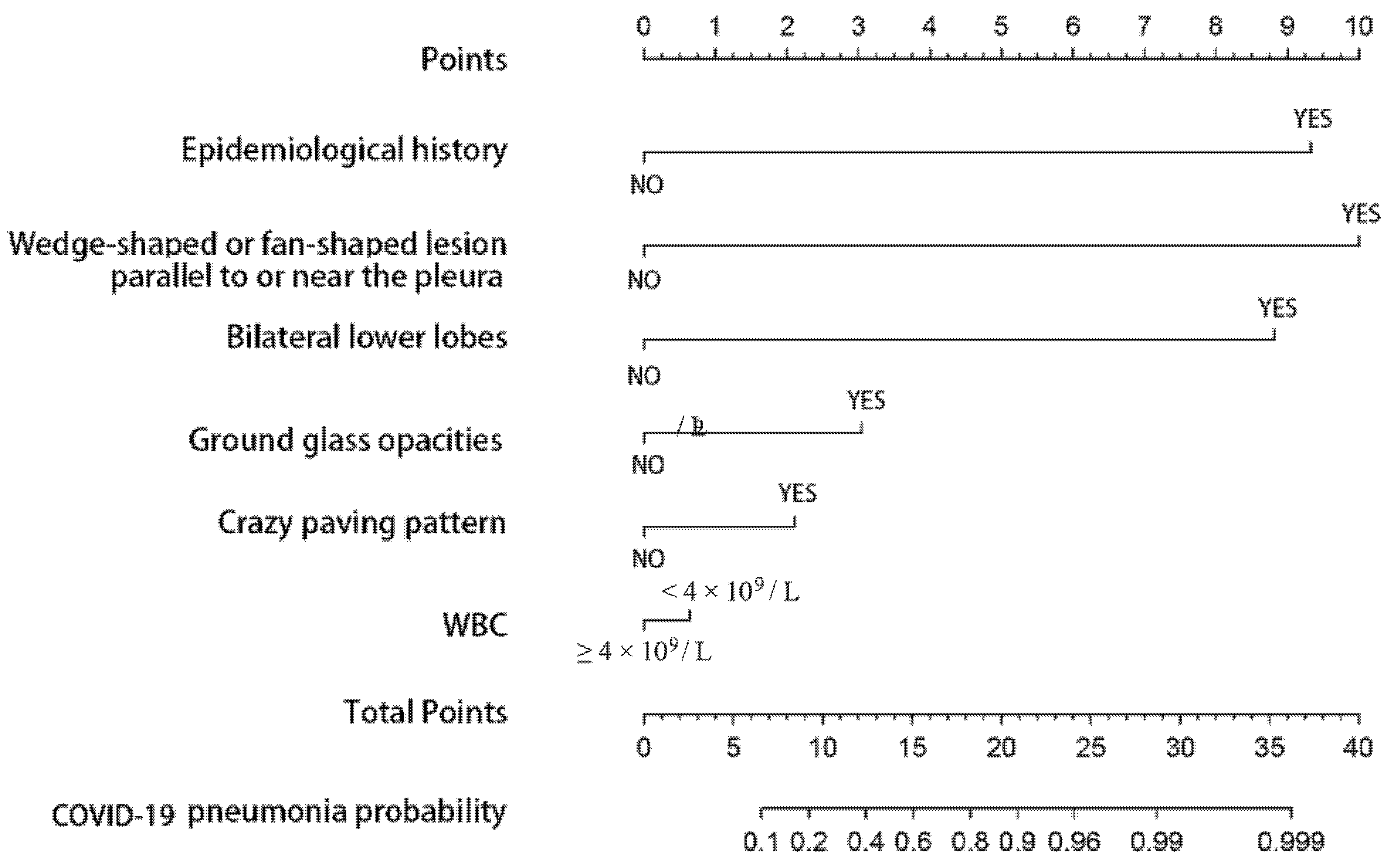
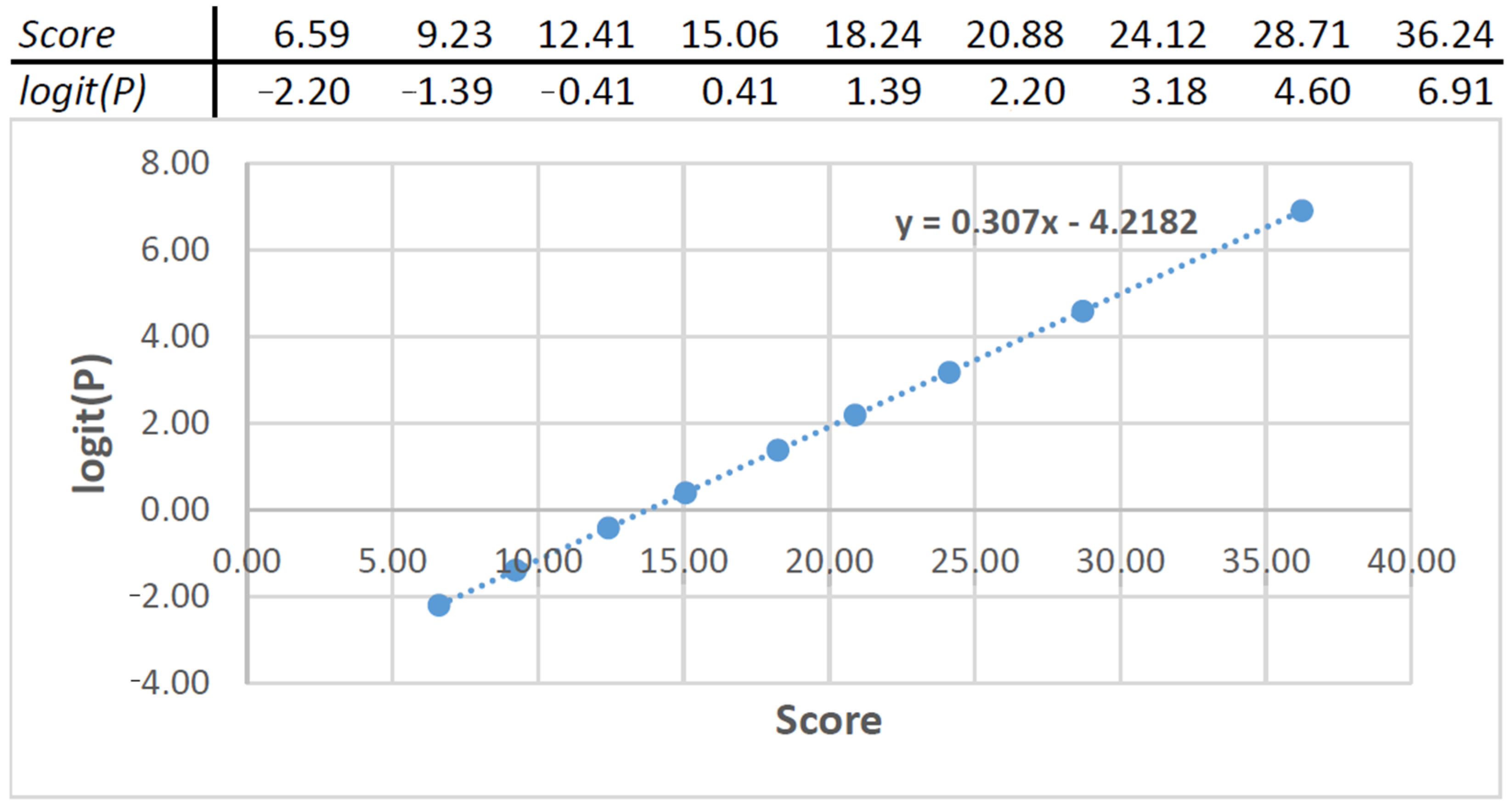
Getting Model Coefficients from a Nomogram
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, G.; Yang, P.; Xie, Y.; Woodruff, H.C.; Rao, X.; Guiot, J.; Frix, A.-N.; Louis, R.; Moutschen, M.; Li, J.; et al. Development of a Clinical Decision Support System for Severity Risk Prediction and Triage of COVID-19 Patients at Hospital Admission: An International Multicenter Study. Eur. Respir. J. 2020, 56, 2001104. [Google Scholar] [CrossRef] [PubMed]
- Song, C.-Y.; Xu, J.; He, J.-Q.; Lu, Y.-Q. COVID-19 early warning score: A multi-parameter screening tool to identify highly suspected patients. MedXRiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Weng, J.; Li, Z.; Hou, R.; Zhou, L.; Ye, H.; Chen, Y.; Yang, T.; Chen, D.; Wang, L.; et al. Development and Validation of a Diagnostic Nomogram to Predict COVID-19 Pneumonia. MedRxiv 2020. [Google Scholar] [CrossRef]
- Wynants, L.; Van Calster, B.; Collins, G.S.; Riley, R.D.; Heinze, G.; Schuit, E.; Bonten, M.M.J.; Dahly, D.L.; Damen, J.A.; Debray, T.P.A.; et al. Prediction models for diagnosis and prognosis of covid-19: Systematic review and critical appraisal. BMJ 2020, 369, m1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.; Gallant, A.J.; Rasmussen, S.; Nicholls, L.A.B.; Cogan, N.; Deakin, K.; Young, D.; Flowers, P. Towards intervention development to increase the uptake of COVID-19 vaccination among those at high risk: Outlining evidence-based and theoretically informed future intervention content. Br. J. Health Psychol. 2020, 25, 1039–1054. [Google Scholar] [CrossRef] [PubMed]
- Persad, G.; Peek, M.E.; Emanuel, E.J. Fairly Prioritizing Groups for Access to COVID-19 Vaccines. JAMA 2020, 324, 1601–1602. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis); Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Jehi, L.; Ji, X.; Milinovich, A.; Erzurum, S.; Merlino, A.; Gordon, S.; Young, J.B.; Kattan, M.W. Development and validation of a model for individualized prediction of hospitalization risk in 4,536 patients with COVID-19. PLoS ONE 2020, 15, e0237419. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD Statement. Eur. Urol. 2015, 67, 1142–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naseem, M.; Akhund, R.; Arshad, H.; Ibrahim, M.T. Exploring the Potential of Artificial Intelligence and Machine Learning to Combat COVID-19 and Existing Opportunities for LMIC: A Scoping Review. J. Prim. Care Community Health 2020, 11, 2150132720963634. [Google Scholar] [CrossRef] [PubMed]
- Van Wijk, Y.; Halilaj, I.; Van Limbergen, E.; Walsh, S.; Lutgens, L.; Lambin, P.; Vanneste, B.G. Decision Support Systems in Prostate Cancer Treatment: An Overview. Biomed. Res. Int. 2019, 2019, 4961768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gong, J.; Ou, J.; Qiu, X.; Jie, Y.; Chen, Y.; Yuan, L.; Cao, J.; Tan, M.; Xu, W.; Zheng, F.; et al. A Tool to Early Predict Severe Corona Virus Disease 2019 (COVID-19): A Multicenter Study using the Risk Nomogram in Wuhan and Guangdong, China. Clin Infect Dis. 2020, 71, 833–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- COVID-19 Vulnerability Index (cv19index)—ClosedLoop.ai. Available online: https://closedloop.ai/c19index/ (accessed on 15 December 2020).
- COVID-19 Prognostic Tool. Available online: https://qxmd.com/calculate (accessed on 15 December 2020).
- Villa, E.; Critelli, R.; Lasagni, S.; Melegari, A.; Curatolo, A.; Celsa, C.; Romagnoli, D.; Melegari, G.; Pivetti, A.; Di Marco, L.; et al. Dynamic angiopoietin-2 assessment predicts survival and chronic course in hospitalized patients with COVID-19. Blood Adv. 2021, 5, 662–673. [Google Scholar] [CrossRef] [PubMed]
- HaHalasz, G.; Sperti, M.; Villani, M.; Michelucci, U.; Agostoni, P.; Biagi, A.; Rossi, L.; Botti, A.; Mari, C.; Maccarini, M.; et al. A Machine Learning Approach for Mortality Prediction in COVID-19 Pneumonia: Development and Evaluation of the Piacenza Score. J. Med. Internet Res. 2021, 23, e29058. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter (Unit) | Equation | Value | Points |
|---|---|---|---|
| Epidemiological history (yes/no, Boolean) | x1 | 1 | 9.32 |
| 0 | 0.00 | ||
| Wedge/fan-shaped lesion (yes/no, Boolean) | x2 | 1 | 10.00 |
| 0 | 0 | ||
| Bilateral lower lobes (yes/no, Boolean) | x3 | 1 | 8.82 |
| 0 | 0.00 | ||
| Ground glass opacities (yes/no, Boolean) | x4 | 1 | 3.04 |
| 0 | 0.00 | ||
| Crazy paving pattern (yes/no, Boolean) | x5 | 1 | 2.10 |
| 0 | 0.00 | ||
| WBC (<4 × 109/L, Boolean) | x6 | 1 | 0.63 |
| 0 | 0.00 |
| Parameter (Unit) | Coefficient |
|---|---|
| Epidemiological history | 0.93 |
| Wedge/fan-shaped lesion | 0.64 |
| Bilateral lower lobes | 0.19 |
| Ground glass opacities | 0.93 |
| Crazy paving pattern | 0.64 |
| WBC | 0.19 |
| Intercept | −4.23 |
| Model Nr | Input Features-Output | Cohort Type | Tripod Type |
|---|---|---|---|
| Model 1 | Input features: Age, hospital staff (Yes/No). Output: Probability of severe illness [1]. | Asymptomatic COVID positive patients | Type 2b |
| Model 2 | Input features: Age, hospital staff (Yes/No), body temperature, days since onset of symptoms. Output: Probability of severe illness [1]. | Symptomatic COVID positive patients | Type 2b |
| Model 3 | Input features: Age, CT lesion score (0 = no lung parenchyma involved, 1 = up to 5% of lung parenchyma involved, 2 = 5–25%, 3 = 26–50%, 4 = 51–75%, 5 = 76–100% of lung parenchyma involved; final CT score is a total score from five lobes). Output: Probability of severe illness [1]. | COVID positive patients with semantic CT features | Type 2b |
| Model 4 | Input features: Age, Lymphocyte, C-reactive protein, Lactate dehydrogenase, Creatine kinase, Urea, Calcium. Output: Probability of severe illness [1]. | COVID-19 positive patients with blood test results | Type 3 |
| Model 5 | Input features: Signs of pneumonia on CT, History of close contact with Covid-19 confirmed, Patient(yes/No), Fever, Age, Gender, Max temperature, Respiratory symptoms, Neutrophil-to-lymphocyte ratio. Output: Probability of severe illness [2]. | COVID-19 positive patients | Type 2b |
| Model 6 | Input features: Age, Direct bilirubin, Red blood cell distribution width, Blood urea nitrogen, C-reactive protein, Lactate dehydrogenase, Albumin. Output: Probability of severe illness [13]. | COVID-19 positive patients | Type 2b |
| Model 7 | Input features: Age, Sex, Diabetes, COPD or emphysema, or chronic Bronchitis, Asthma, Cystic fibrosis, Hypertension, Had a heart attack, had a stroke, Coronary atherosclerosis or other heart disease, Congestive heart failure, Rheumatic kidney disease, Chronic kidney disease, Liver disease, Cancer, Neurocognitive conditions, Sickle cell anemia, HIV infection (Yes/No). Health history: Organ transplant, Hemodialysis treatment, pneumonia, acute bronchitis, influenza or other acute respiratory infection, pregnant last 2 weeks, hospital admission/emergency last year, height, weigh.Symptoms: fever, shortness in breath, cough, fatigue, body aches, headache, diarrhea, sore throat, decrease smell and taste (Yes/No). Output: Predicts vulnerability score to serious illness from COVID-19 [14]. | COVID-19 positive patients (vulnerable to develop serious complications) | Type 3 |
| Model 8 | Input features: Age, cardiovascular disease, diabetes, chronic respiratory disease, hypertension, cancer, prior stroke, heart disease, chronic kidney disease. Output: Estimate mortality rates in patients with COVID-19 [15]. | COVID-19 positive patients | Type 3 |
| Model 9 | Input features: Epidemiological history, wedge-shaped or fan-shaped lesion parallel or near to the pleura, bilateral lower lobes, ground glass opacities, crazy paving pattern, WBC. Output: Probability of severe illness [3]. | Suspected COVID-19 pneumonia patients | Type 2b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halilaj, I.; Chatterjee, A.; van Wijk, Y.; Wu, G.; van Eeckhout, B.; Oberije, C.; Lambin, P. Covid19Risk.ai: An Open Source Repository and Online Calculator of Prediction Models for Early Diagnosis and Prognosis of Covid-19. BioMed 2021, 1, 41-49. https://doi.org/10.3390/biomed1010003
Halilaj I, Chatterjee A, van Wijk Y, Wu G, van Eeckhout B, Oberije C, Lambin P. Covid19Risk.ai: An Open Source Repository and Online Calculator of Prediction Models for Early Diagnosis and Prognosis of Covid-19. BioMed. 2021; 1(1):41-49. https://doi.org/10.3390/biomed1010003
Chicago/Turabian StyleHalilaj, Iva, Avishek Chatterjee, Yvonka van Wijk, Guangyao Wu, Brice van Eeckhout, Cary Oberije, and Philippe Lambin. 2021. "Covid19Risk.ai: An Open Source Repository and Online Calculator of Prediction Models for Early Diagnosis and Prognosis of Covid-19" BioMed 1, no. 1: 41-49. https://doi.org/10.3390/biomed1010003
APA StyleHalilaj, I., Chatterjee, A., van Wijk, Y., Wu, G., van Eeckhout, B., Oberije, C., & Lambin, P. (2021). Covid19Risk.ai: An Open Source Repository and Online Calculator of Prediction Models for Early Diagnosis and Prognosis of Covid-19. BioMed, 1(1), 41-49. https://doi.org/10.3390/biomed1010003