
Physiological Responses of Anemic Women to Exercise under Hypoxic Conditions

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design and Procedure
2.3. Protocol
2.4. Measurements and Calculations
2.5. Statistical Analysis
3. Results
3.1. Participants
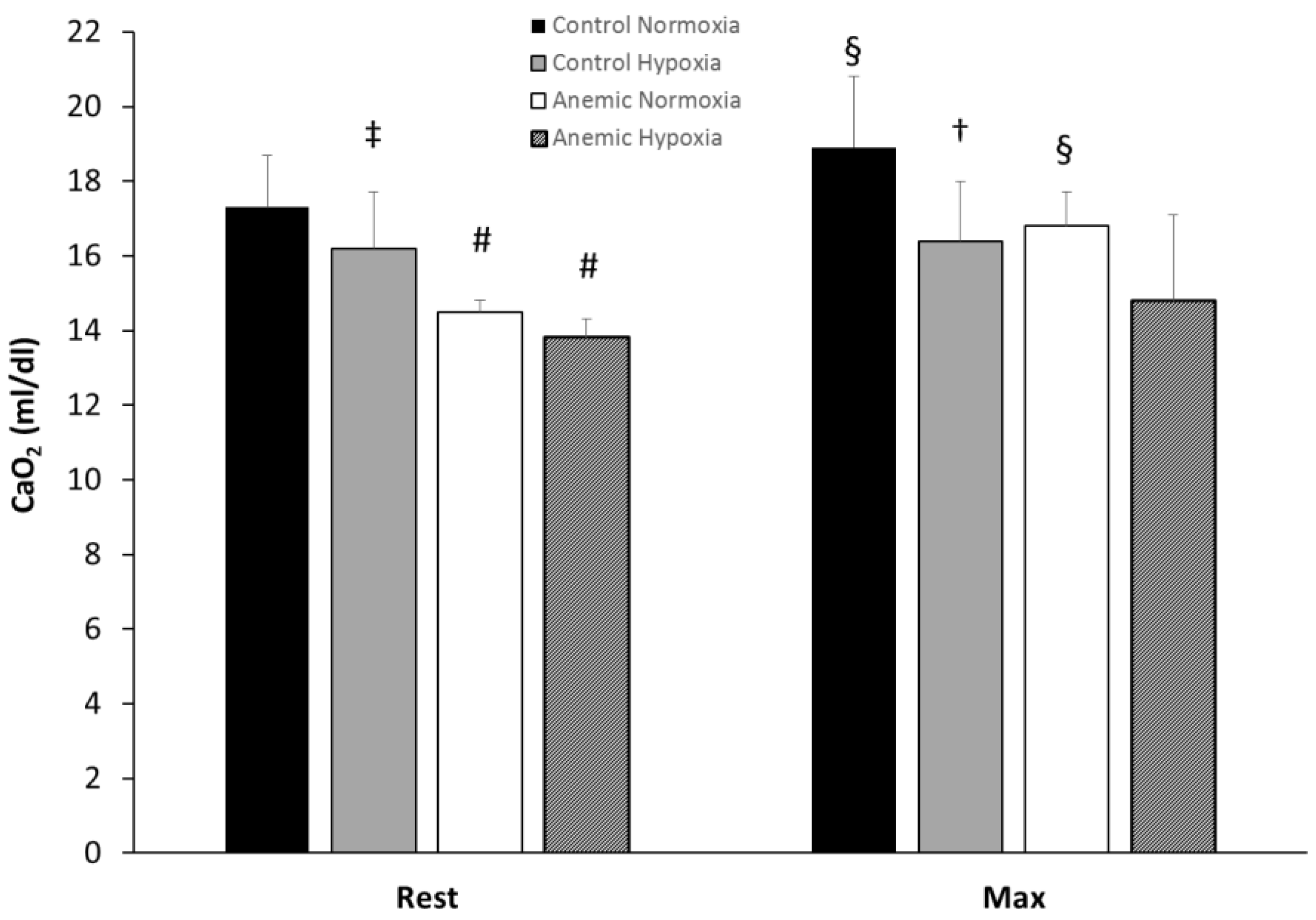
3.2. Hematological Variables
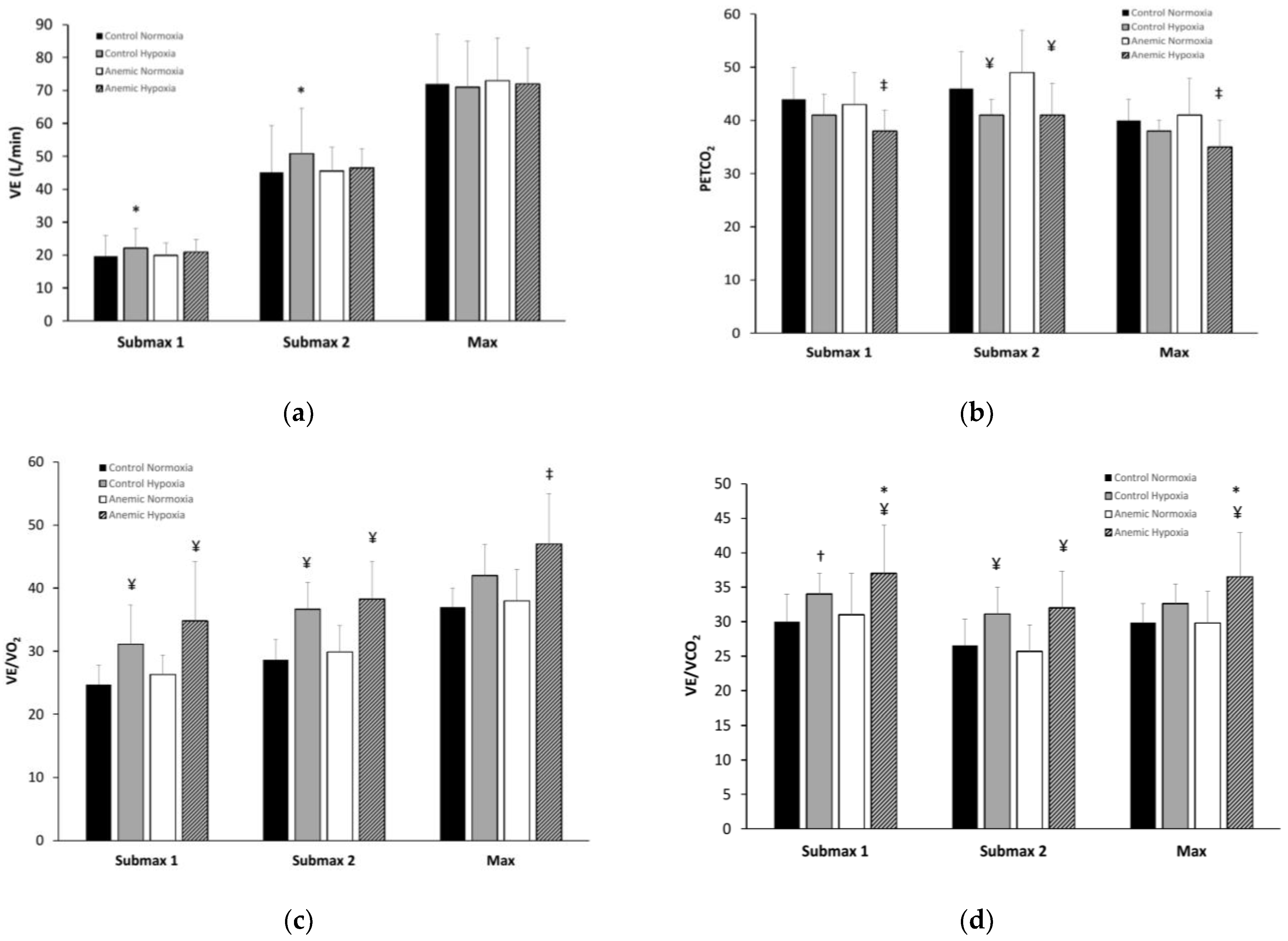
3.3. Respiratory Variables
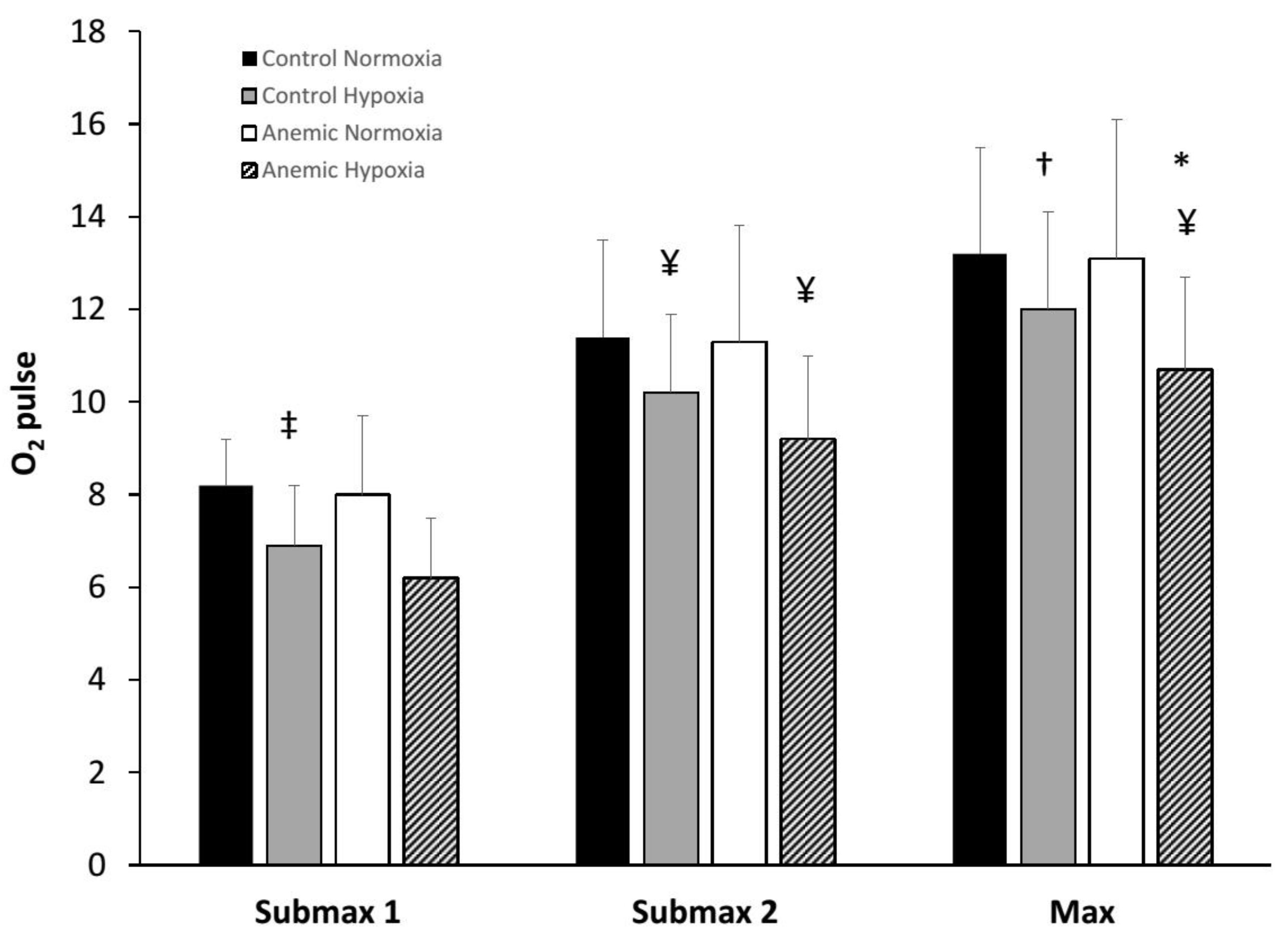
3.4. Cardiovascular Variables
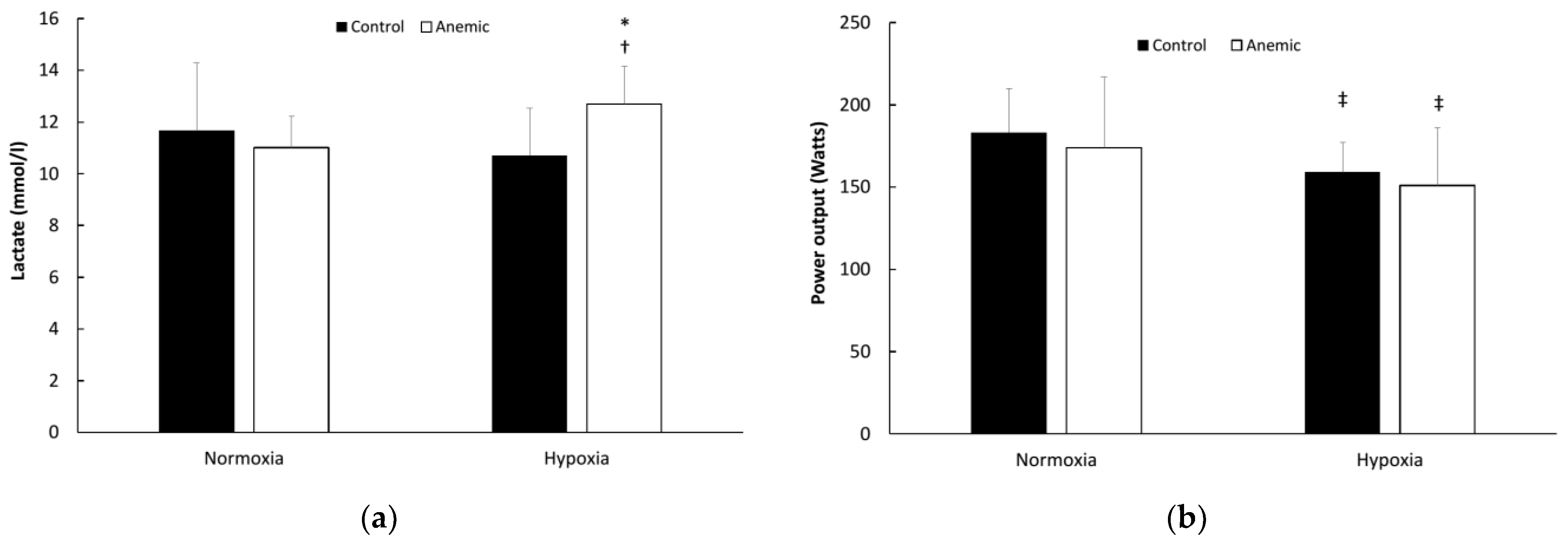
3.5. Maximal Work Variables
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Calbet, J.A.; Boushel, R.; Radegran, G.; Søndergaard, H.; Wagner, P.D.; Saltin, B. Determinants of maximal oxygen uptake in severe acute hypoxia. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2003, 284, R291–R303. [Google Scholar] [CrossRef] [PubMed]
- Koskolou, M.D.; Calbet, J.A.; Radegran, G.; Roach, R.C. Hypoxia and the cardiovascular response to dynamic knee-extensor exercise. Am. J. Physiol.-Heart Circ. Physiol. 1997, 272, H2655–H2663. [Google Scholar] [CrossRef] [PubMed]
- Calbet, J.A. Oxygen tension and content in the regulation of limb blood flow. Acta Physiol. Scand. 2000, 168, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Calbet, J.A.L.; Rådegran, G.; Boushel, R.; Saltin, B. On the mechanisms that limit oxygen uptake during exercise in acute and chronic hypoxia: Role of muscle mass. J. Physiol. 2009, 587, 477–490. [Google Scholar] [CrossRef]
- Stenberg, J.; Ekblom, B.; Messin, R. Hemodynamic response to work at simulated altitude, 4000 m. J. Appl. Physiol. 1966, 21, 1589–1594. [Google Scholar] [CrossRef]
- Knight, D.R.; Poole, D.C.; Hogan, M.C.; Bebout, D.E.; Wagner, P.D. Effect of inspired O2 concentration on leg lactate release during incremental exercise. J. Appl. Physiol. 1996, 81, 246–251. [Google Scholar] [CrossRef]
- Macedo, D.V.; Lazarim, F.; Da Silva, F.O.C.; Tessuti, L.S.; Hohl, R.; Da Silva, F.O.C. Is lactate production related to muscular fatigue? A pedagogical proposition using empirical facts. Adv. Physiol. Educ. 2009, 33, 302–307. [Google Scholar] [CrossRef]
- Celsing, F.; Nyström, J.; Pihlstedt, P.; Werner, B.; Ekblom, B. Effect of long-term anemia and retransfusion on central circulation during exercise. J. Appl. Physiol. 1986, 61, 1358–1362. [Google Scholar] [CrossRef]
- Ekblom, B.; Wilson, G.; Astrand, P.O. Central circulation during exercise after venesection and reinfusion of red blood cells. J. Appl. Physiol. 1976, 40, 379–383. [Google Scholar] [CrossRef]
- Woodson, R.D.; Wills, R.E.; Lenfant, C. Effect of acute and established anemia on O2 transport at rest, submaximal and maximal work. J. Appl. Physiol. 1978, 44, 36–43. [Google Scholar] [CrossRef]
- Koskolou, M.D.; Roach, R.; Calbet, J.A.; Rådegran, G.; Saltin, B. Cardiovascular responses to dynamic exercise with acute anemia in humans. Am. J. Physiol.-Heart Circ. Physiol. 1997, 273, H1787–H1793. [Google Scholar] [CrossRef]
- Calbet, J.A.; Lundby, C.; Koskolou, M.; Boushel, R. Importance of hemoglobin concentration to exercise: Acute manipulations. Respir. Physiol. Neurobiol. 2006, 151, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Gardner, G.W.; Edgerton, V.R.; Senewiratne, B.; Barnard, R.J.; Ohira, Y. Physical work capacity and metabolic stress in subjects with iron deficiency anemia. Am. J. Clin. Nutr. 1977, 30, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Roach, R.C.; Koskolou, M.D.; Calbet, J.A.L.; Saltin, B. Arterial O2 content and tension in regulation of cardiac output and leg blood flow during exercise in humans. Am. J. Physiol.-Heart Circ. Physiol. 1999, 276, H438–H445. [Google Scholar] [CrossRef] [PubMed]
- González-Alonso, J.; Mortensen, S.P.; Dawson, E.; Secher, N.H.; Damsgaard, R. Erythrocytes and the regulation of human skeletal muscle blood flow and oxygen delivery: Role of erythrocyte count and oxygenation state of haemoglobin. J. Physiol. 2006, 572, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Dugan, C.; MacLean, B.; Cabolis, K.; Abeysiri, S.; Khong, A.; Sajic, M.; Richards, T. The misogyny of iron deficiency. Anaesthesia 2021, 76 (Suppl. 4), 56–62. [Google Scholar] [CrossRef] [PubMed]
- WHO. Nutritional Anaemias: Tools for Effective Prevention and Control; World Health Organization: Geneva, Switzerland, 2017. Available online: https://apps.who.int/iris/handle/10665/259425 (accessed on 14 February 2023).
- WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011. Available online: https://apps.who.int/iris/handle/10665/85839 (accessed on 14 February 2023).
- WHO. WHO Guideline on Use of Ferritin Concentrations to Assess Iron Status in Individuals and Populations; World Health Organization: Geneva, Switzerland, 2020. Available online: https://apps.who.int/iris/handle/10665/331505 (accessed on 14 February 2023).
- Kuipers, H.; Verstappen, F.T.J.; Keizer, H.A.; Geurten, P.; van Kranenburg, G. Variability of Aerobic Performance in the Laboratory and Its Physiologic Correlates. Int. J. Sports Med. 1985, 6, 197–201. [Google Scholar] [CrossRef]
- Haas, J.D.; Brownlie, T. Iron Deficiency and Reduced Work Capacity: A Critical Review of the Research to Determine a Causal Relationship. J. Nutr. 2001, 131, 676S–690S. [Google Scholar] [CrossRef]
- Woodson, R.D. Hemoglobin Concentration and Exercise Capacity. Am. Rev. Respir. Dis. 1984, 129, S72–S75. [Google Scholar] [CrossRef]
- Viteri, F.E.; Torun, B. Anemia and physical work capacity. In Clinics in Hematology; Garby, L., Ed.; WB Saunders: London, UK, 1974; Volume 3, pp. 609–626. [Google Scholar]
- Torre-Bueno, J.R.; Wagner, P.D.; Saltzman, H.A.; Gale, G.E.; Moon, R.E. Diffusion limitation in normal humans during exercise at sea level and simulated altitude. J. Appl. Physiol. 1985, 58, 989–995. [Google Scholar] [CrossRef]
- Wagner, P.D.; Gale, G.E.; Moon, R.E.; Torre-Bueno, J.R.; Stolp, B.W.; Saltzman, H.A. Pulmonary gas exchange in humans exercising at sea level and simulated altitude. J. Appl. Physiol. 1986, 61, 260–270. [Google Scholar] [CrossRef] [PubMed]
- Friedmann, B.; Frese, F.; Menold, E.; Bärtsch, P. Individual Variation in the Reduction of Heart Rate and Performance at Lactate Thresholds in Acute Normobaric Hypoxia. Int. J. Sports Med. 2005, 26, 531–536. [Google Scholar] [CrossRef]
- Bärtsch, P.; Saltin, B. General introduction to altitude adaptation and mountain sickness. Scand. J. Med. Sci. Sports 2008, 18 (Suppl. S1), 1–10. [Google Scholar] [CrossRef] [PubMed]
- Rowell, L.B. Human Cardiovascular Control; Oxford University Press: New York, NY, USA, 1993; pp. 162–203. ISBN 0-19-507362-2. [Google Scholar]
- Beard, J.L.; Haas, J.D.; Tufts, D.; Spielvogel, H.; Vargas, E.; Rodriguez, C. Iron deficiency anemia and steady-state work performance at high altitude. J. Appl. Physiol. 1988, 64, 1878–1884. [Google Scholar] [CrossRef]
- Sproule, B.J.; Mitchell, J.H.; Miller, W.F. Cardiopulmonary physiological responses to heavy exercise in patients with anemia. J. Clin. Investig. 1960, 39, 378–388. [Google Scholar] [CrossRef]
- Wasserman, K.; Hansen, L.E.; Sue, D.Y.; Casaburi, R.; Whipp, B.J. Principles of Exercise Testing and Interpretation, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1999; pp. 109–110. ISBN 0-683-30646-4. [Google Scholar]
- Macdonald, R. Red cell 2,3-diphosphoglycerate and oxygen affinity. Anaesthesia 1977, 32, 544–553. [Google Scholar] [CrossRef]
- Płoszczyca, K.; Czuba, M.; Chalimoniuk, M.; Gajda, R.; Baranowski, M. Red Blood Cell 2,3-Diphosphoglycerate Decreases in Response to a 30 km Time Trial Under Hypoxia in Cyclists. Front. Physiol. 2021, 12, 670977. [Google Scholar] [CrossRef]
- Ellsworth, M.L.; Forrester, T.; Ellis, C.G.; Dietrich, H.H. The erythrocyte as a regulator of vascular tone. Am. J. Physiol.-Heart Circ. Physiol. 1995, 269, H2155–H2161. [Google Scholar] [CrossRef]
- Stamler, J.S.; Jia, L.; Eu, J.P.; McMahon, T.J.; Demchenko, I.T.; Bonaventura, J.; Gernert, K.; Piantadosi, C.A. Blood Flow Regulation by S -Nitrosohemoglobin in the Physiological Oxygen Gradient. Science 1997, 276, 2034–2037. [Google Scholar] [CrossRef]
- González-Alonso, J.; Olsen, D.B.; Saltin, B. Erythrocyte and the regulation of human skeletal muscle blood flow and oxygen delivery: Role of circulating ATP. Circ. Res. 2002, 91, 1046–1055. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | Anemic | |
|---|---|---|
| Age (y) | 22.1 ± 3.4 (19–27) | 23.4 ± 4.6 (19–32) |
| Weight (kg) | 59.9 ± 7 (46–74) | 61.8 ± 6.19 (57–76) |
| Height (cm) | 169.4 ± 5.3 (159–177) | 168.6 ± 8.4 (160–188) |
| Hematocrit (%) | 40.1 ± 1.7 (38.3–41.8) | 36.1 ± 0.6 (35.1–36.8) ** |
| Hemoglobin (g/dL) | 13.2 ± 0.7 (12.4–14.2) | 10.5 ± 0.3 (10.0–10.9) ** |
| Ferritin (μg/L) | 42.5 ± 28.5 (18–90) | 7.8 ± 2.4 (5–11) * |
| Control | Anemic | |||
|---|---|---|---|---|
| Normoxia | Hypoxia | Normoxia | Hypoxia | |
| Hb (g/dL) | 13.0 ± 1.1 | 13.0 ± 1.2 | 10.9 ± 0.2 # | 11.1 ± 0.4 # |
| Hct (%) | 40.5 ± 1.8 | 41.3 ± 2.1 | 36.1 ± 1.2 # | 36.3 ± 1.2 # |
| SaO2 (%) | 99 ± 1 | 93 ± 1 ¥ | 99 ± 1 | 93 ± 2 ¥ |
| CaO2 (mL/dL) | 17.3 ± 1.4 | 16.2 ± 1.5 ‡ | 14.5 ± 0.3 # | 13.8 ± 0.5 # |
| VE (L/min) | 7.9 ± 1.34 | 9.2 ± 1.80 | 9.1 ± 1.69 | 10.2 ± 1.24 |
| RR | 16 ± 2 | 18 ± 4 | 19 ± 2 * | 19 ± 3 |
| VT (mL) | 689 ± 82 | 680 ± 87 | 660 ± 87 | 722 ± 88 |
| VO2 (mL/kg/min) | 5.43 ± 0.87 | 4.22 ± 0.83 † | 5.32 ± 0.78 | 4.51 ± 0.73 † |
| VE/VO2 | 31.5 ± 5.24 | 48.8 ± 6.41 † | 36.1 ± 4.43 | 49.5 ± 4.74 † |
| VCO2 (mL/min) | 264 ± 32 | 254 ± 48 | 277 ± 42 | 285 ± 30 |
| VE/VCO2 | 39.0 ± 6.19 | 46.5 ± 4.42 † | 41.8 ± 5.07 | 44.8 ± 5.82 |
| PETO2 (mmHg) | 104 ± 7 | 69 ± 7 ¥ | 112 ± 5 | 74 ± 10 ¥ |
| PETCO2 (mmHg) | 40 ± 4 | 38 ± 3 | 39 ± 3 | 39 ± 3 |
| HR (bpm) | 76 ± 5 | 83 ± 9 † | 83 ± 9 | 87 ± 9 † |
| O2 pulse (mL/beat) | 4.23 ± 0.62 | 3.07 ± 0.92 ‡ | 3.90 ± 0.66 | 3.20 ± 0.53 |
| Lactate (mmol/L) | 1.76 ± 1.19 | 1.27 ± 0.36 | 1.55 ± 0.81 | 2.00 ± 1.57 |
| Normoxia | Hypoxia | |||||
|---|---|---|---|---|---|---|
| Submax1 40% VO2max | Submax2 80% VO2max | Max | Submax1 40% VO2max | Submax2 80% VO2max | Max | |
| Control | ||||||
| Hb (g/dL) | - * | - * | 14.5 ± 1.6 | - * | - * | 14.7 ± 1.4 |
| Hct (%) | - * | - * | 43.6 ± 2.1 | - * | - * | 44.6 ± 2.5 |
| SaO2 (%) | 99 ± 1 | 98 ± 1 | 97 ± 1 | 89 ± 2 ¥ | 84 ± 3 ¥ | 83 ± 3 ¥ |
| RR | 24 ± 5 | 34 ± 3 | 50 ± 7 | 25 ± 4 | 36 ± 3 | 48 ± 8 |
| VT (mL) | 1056 ± 330 | 1680 ± 160 | 1821 ± 335 | 1163 ± 275 | 1815 ± 110 | 1926 ± 180 |
| VO2 (mL/kg/min) | 16.3 ± 1.5 | 32.5 ± 2.9 | 40.8 ± 3.6 | 14.7 ± 1.6 † | 29.2 ± 3.4 † | 36.7 ± 4.1 † |
| VCO2 (mL/min) | 806 ± 197 | 2101 ± 359 | 2981 ± 377 | 813 ± 167 | 2037 ± 295 | 2706 ± 319 † |
| PETO2 (mmHg) | 99 ± 8 | 107 ± 8 | 116 ± 6 | 56 ± 6 ¥ | 64 ± 5 ¥ | 72 ± 6 ¥ |
| HR (bpm) | 118 ± 10 | 170 ± 8 | 185 ± 8 | 127 ± 5 † | 170 ± 7 | 183 ± 5 |
| Power output (Watts) | 59 ± 18 | 143 ± 26 | 183 ± 27 | 52 ± 11 | 133 ± 26 | 159 ± 18 |
| Exercise time (s) | - | - | 706 ± 107 | - | - | 610 ± 77 † |
| Lactate (mmol/L) | 11.67 ± 2.61 | 10.70 ± 1.83 | ||||
| Anemic | ||||||
| Hb (g/dL) | - * | - * | 13.1 ± 0.7 # | - * | - * | 13.4 ± 1.3 # |
| Hct (%) | - * | - * | 39.4 ± 1.3 # | - * | - * | 39.6 ± 1.4 # |
| SaO2 (%) | 99 ± 1 | 98 ± 1 | 96 ± 1 | 92 ± 1 | 84 ± 4 | 82 ± 4 |
| RR | 26 ± 8 | 34 ± 3 | 52 ± 11 | 25 ± 8 | 36 ± 3 | 54 ± 13 |
| VT (mL) | 1091 ± 212 | 1710 ± 102 | 1762 ± 296 | 1147 ± 312 | 1700 ± 48 | 1745 ± 294 |
| VO2 (mL/kg/min) | 15.4 ± 2.1 | 30.6 ± 4.4 | 38.2 ± 5.3 | 12.5 ± 1.6 † # | 24.9 ± 3.1 †# | 31.1 ± 3.9 † # |
| VCO2 (mL/min) | 803 ± 187 | 2217 ± 415 | 3043 ± 550 | 716 ± 85 | 1835 ± 267 ¥ | 2485 ± 331 ¥ |
| PETO2 (mmHg) | 104 ± 12 | 111 ± 9 | 120 ± 7 | 60 ± 8 ¥ | 66 ± 5 ¥ | 73 ± 3 ¥ |
| HR (bpm) | 122 ± 10 | 169 ± 8 | 184 ± 7 | 125 ± 9 † | 167 ± 7 | 180 ± 5 |
| Power output (Watts) | 53 ± 23 | 142 ± 39 | 174 ± 43 | 41 ± 12 | 120 ± 23 | 151 ± 35 |
| Exercise time (s) | - | - | 666 ± 179 | - | - | 579 ± 123 † |
| Lactate (mmol/L) | 11.01 ± 1.22 | 12.69 ± 1.46 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koskolou, M.D.; Komboura, S.; Zacharakis, E.; Georgopoulou, O.; Keramidas, M.E.; Geladas, N. Physiological Responses of Anemic Women to Exercise under Hypoxic Conditions. Physiologia 2023, 3, 247-258. https://doi.org/10.3390/physiologia3020017
Koskolou MD, Komboura S, Zacharakis E, Georgopoulou O, Keramidas ME, Geladas N. Physiological Responses of Anemic Women to Exercise under Hypoxic Conditions. Physiologia. 2023; 3(2):247-258. https://doi.org/10.3390/physiologia3020017
Chicago/Turabian StyleKoskolou, Maria D., Stamatia Komboura, Emmanouil Zacharakis, Olga Georgopoulou, Michail E. Keramidas, and Nickos Geladas. 2023. "Physiological Responses of Anemic Women to Exercise under Hypoxic Conditions" Physiologia 3, no. 2: 247-258. https://doi.org/10.3390/physiologia3020017
APA StyleKoskolou, M. D., Komboura, S., Zacharakis, E., Georgopoulou, O., Keramidas, M. E., & Geladas, N. (2023). Physiological Responses of Anemic Women to Exercise under Hypoxic Conditions. Physiologia, 3(2), 247-258. https://doi.org/10.3390/physiologia3020017