A Permutation Disalignment Index-Based Complex Network Approach to Evaluate Longitudinal Changes in Brain-Electrical Connectivity

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials: Study Population
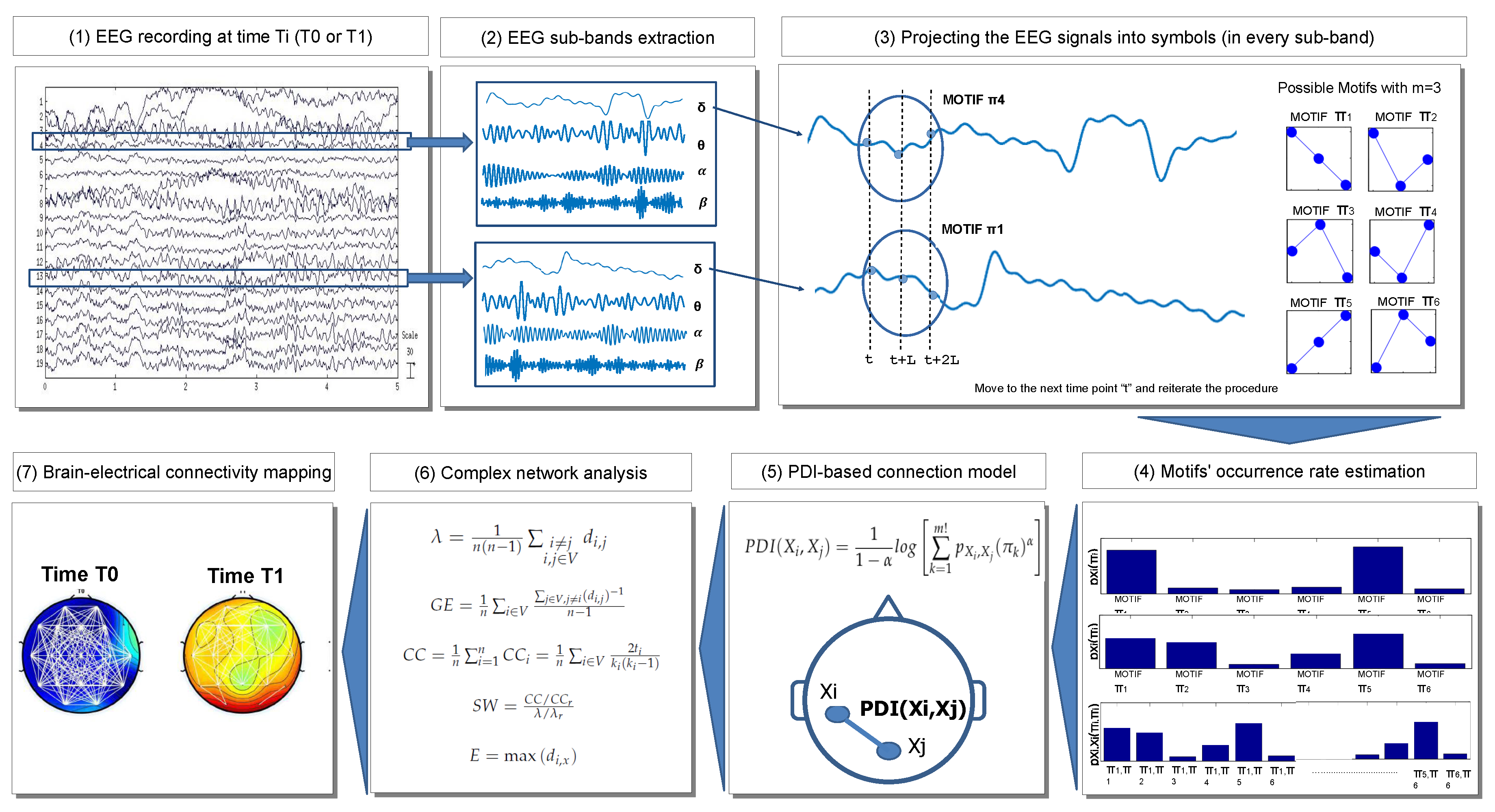
3. Methodology: PDI-Based EEG Complex Network Analysis
3.1. EEG Recording
3.2. EEG Sub-Band Extraction
3.3. Projecting the EEG Signals into Symbols
3.4. Motif Occurrence Rate Estimation
3.5. PDI-Based Connection Model
3.6. Complex Network Analysis Based on PDI
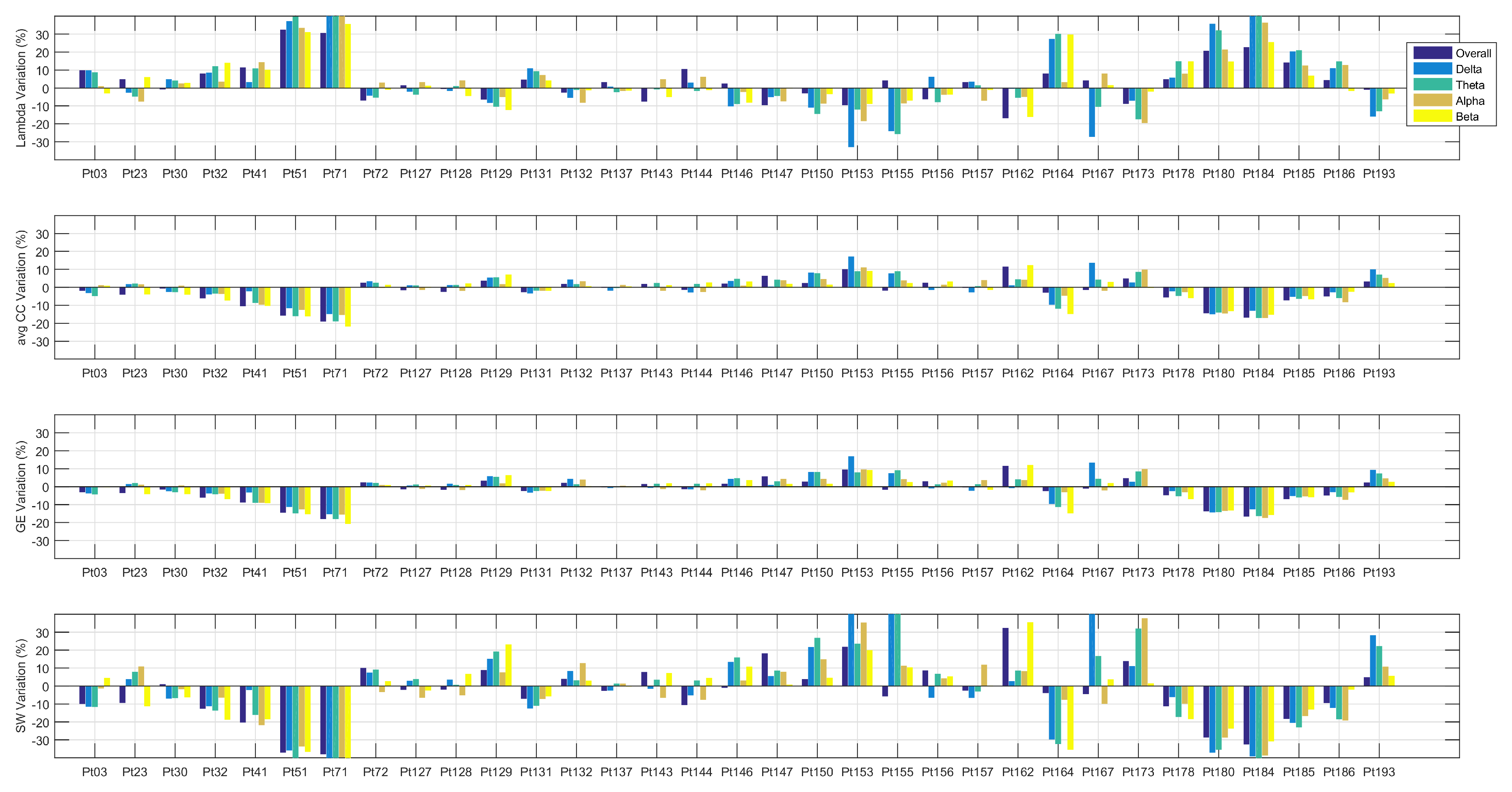
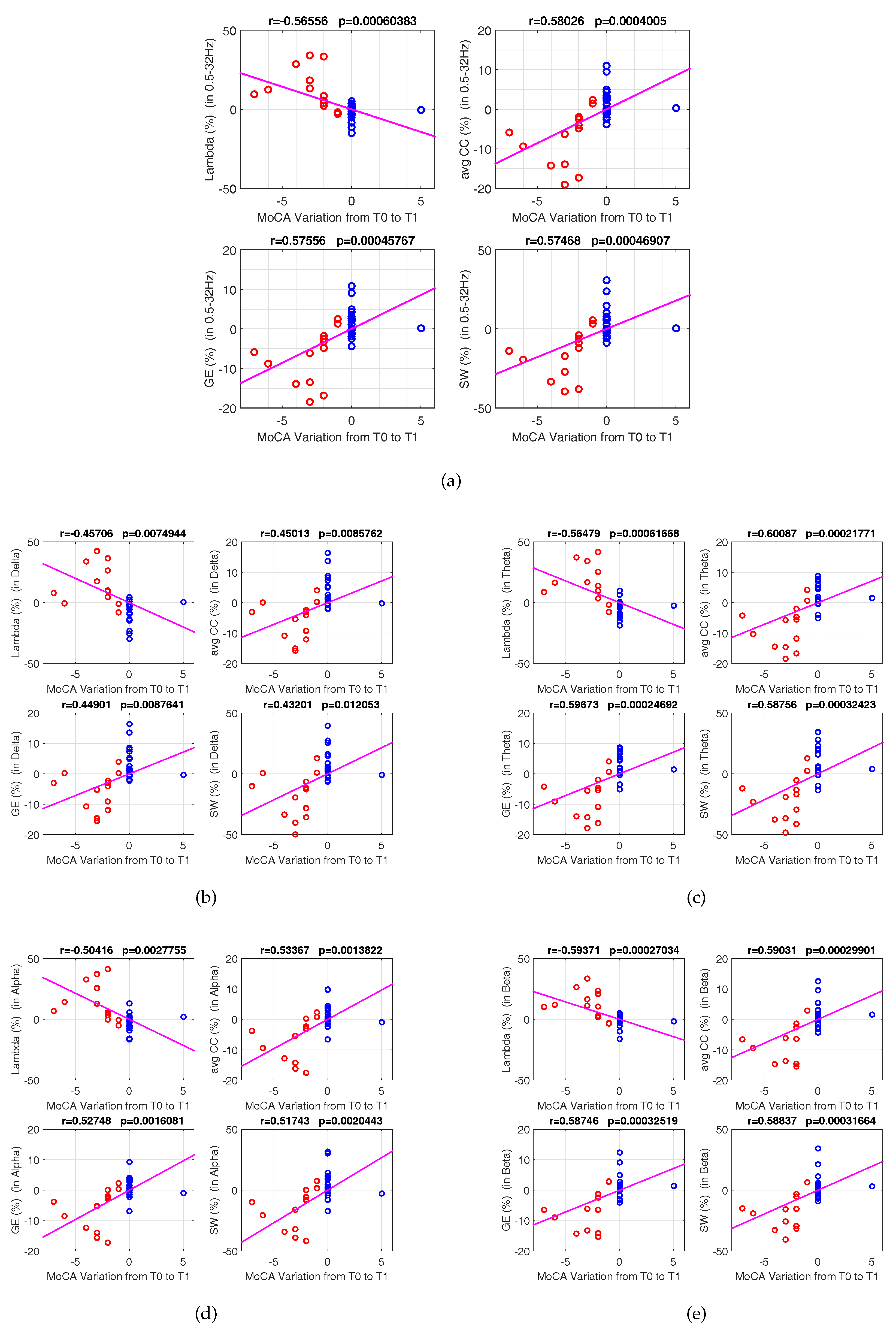
4. Results
- Delta range (, and ; , and ; , and ; , and );
- Theta range (, and ; , and ; , and ; , and );
- Alpha range (, and 3; , and ; , and ; , and );
- Beta range (, and ; , and ; , and ; , and ).
5. Discussion
6. Conclusions
Author Contributions
Conflicts of Interest
References
- Nunez, P.L.; Srinivasan, R. Electric Fields of the Brain, the Neurophysics of EEG; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Dauwels, J.; Vialatte, F.; Cichocki, A. Diagnosis of Alzheimer’s disease from EEG signals: Where are we standing? Curr. Alzheimer Res. 2010, 7, 487–505. [Google Scholar] [CrossRef] [PubMed]
- Gong, N.J.; Wong, C.S.; Chan, C.C.; Leung, L.M.; Chu, Y.C. Correlations between microstructural alterations and severity of cognitive deficiency in Alzheimer’s disease and mild cognitive impairment: A diffusional kurtosis imaging study. Magn. Reson. Imaging 2013, 31, 688–694. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, L.; Lamberton, F.; Bokde, A.L.W.; Ewers, M.; Faluyi, Y.; Tanner, C.; Mazoyer, B.; O’Neill, D.; Bartley, M.; Collins, D.R.; et al. Using support vector machines with multiple indices of diffusion for automated classification of mild cognitive impairment. PLoS ONE 2012, 7, e32441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varghese, T.; Sheelakumari, R.; James, J.S.; Mathuranath, P. A review of neuroimaging biomarkers of Alzheimer’s disease. Neurol. Asia 2013, 18, 239–248. [Google Scholar] [PubMed]
- McEvoy, L.K.; Fennema-Notestine, C.; Roddey, J.C.; Hagler, D.J.; Holland, D.; Karow, D.S.; Pung, C.J.; Brewer, J.B.; Dale, A.M. Alzheimer’s Disease Neuroimaging Initiative. Alzheimer disease: Quantitative structural neuroimaging for detection and prediction of clinical and structural changes in mild cognitive impairment. Radiology 2009, 251, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Alberdi, A.; Aztiria, A.; Basarab, A. On the early diagnosis of Alzheimer’s Disease from multimodal signals: A survey. Artif. Intell. Med. 2016, 71, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Bramanti, A.; Bonanno, L.; Celona, A.; Bertuccio, S.; Calisto, A.; Lanzafame, P.; Bramanti, P. GIS and spatial analysis for costs and services optimization in neurological telemedicine. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Buenos Aires, Argentina, 31 August–4 September 2010; pp. 2204–2207. [Google Scholar]
- Trzepacz, P.T.; Hochstetler, H.; Wang, S.; Walker, B.; Saykin, A.J. Relationship between the Montreal Cognitive Assessment and Mini-mental State Examination for assessment of mild cognitive impairment in older adults. BMC Geriatr. 2015, 15, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo Re, G.; De Luca, R.; Muscarneri, F.; Dorangricchia, P.; Picone, D.; Vernuccio, F.; Salerno, S.; La Tona, G.; Pinto, A.; Midiri, M.E.A. Relationship between anxiety level and radiological investigation. Comparison among different diagnostic imaging exams in a prospective single-center study. Radiol. Med. 2016, 121, 763–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adeli, H.; Ghosh-Dastidar, S.; Dadmehr, N. Alzheimer’s disease and models of computation: Imaging, classification, and neural models. J. Alzheimers Dis. 2005, 7, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Fiscon, G.; Weitschek, E.; Felici, G.; Bertolazzi, P.; De Salvo, S.; Bramanti, P.; De Cola, M.C. Alzheimer’s disease patients classification through EEG signals processing. In Proceedings of the 2014 IEEE Symposium on Computational Intelligence and Data Mining (CIDM), Orlando, FL, USA, 9–12 December 2014; pp. 105–112. [Google Scholar]
- Koenig, T.; Prichep, L.; Dierks, T.; Hubl, D.; Wahlund, L.O.; John, E.R.; Jelic, V. Decreased EEG synchronization in Alzheimer’s disease and mild cognitive impairment. Neurobiol. Aging 2005, 26, 165–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labate, D.; La Foresta, F.; Palamara, I.; Morabito, G.; Bramanti, A.; Zhang, Z.; Morabito, F.C. EEG complexity modifications and altered compressibility in mild cognitive impairment and Alzheimer’s disease. In Recent Advances of Neural Network Models and Applications; Springer: Berlin, Germany, 2014; pp. 163–173. [Google Scholar]
- Moretti, D.V. Conversion of Mild Cognitive Impairment patients in Alzheimer’s disease: Prognostic value of Alpha3/Alpha2 electroencephalographic rhythms power ratio. Alzheimers Res. Ther. 2015, 7, 80. [Google Scholar] [CrossRef] [PubMed]
- Babiloni, C.; Frisoni, G.B.; Pievani, M.; Vecchio, F.; Lizio, R.; Buttiglione, M.; Geroldi, C.; Fracassi, C.; Eusebi, F.; Ferri, R.; et al. Hippocampal volume and cortical sources of EEG alpha rhythms in mild cognitive impairment and Alzheimer disease. Neuroimage 2008, 44, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Stam, C.J.; van der Made, Y.; Pijnenburg, Y.A.; Scheltens, P. EEG synchronization in Mild Cognitive Impairment and Alzheimer’s disease. Acta Neurol. Scand. 2003, 108, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Ahmadlou, M.; Adeli, H. Wavelet-synchronization methodology: A new approach for EEG-based diagnosis of ADHD. Clin. EEG Neurosci. 2010, 41, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Frantzidis, C.A.; Vivas, A.B.; Tsolaki, A.; Klados, M.A.; Tsolaki, M.; Bamidis, P.D. Functional disorganization of small-world brain networks in mild Alzheimer’s Disease and amnestic Mild Cognitive Impairment: An EEG study using Relative Wavelet Entropy (RWE). Front. Aging Neurosci. 2014, 26. [Google Scholar] [CrossRef] [PubMed]
- Ahmadlou, M.; Adeli, A.; Bajo, R.; Adeli, H. Complexity of functional connectivity networks in mild cognitive impairment subjects during a working memory task. Clin. Neurophysiol. 2014, 125, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Vecchio, F.; Miraglia, F.; Quaranta, D.; Granata, G.; Romanello, R.; Marra, C.; Bramanti, P.; Rossini, P.M. Cortical connectivity and memory performance in cognitive decline: A study via graph theory from EEG data. Neuroscience 2016, 316, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Morabito, F.C.; Campolo, M.; Labate, D.; Morabito, G.; Bonanno, L.; Bramanti, A.; de Salvo, S.; Marra, A.; Bramanti, P. A longitudinal EEG study of Alzheimer’s disease progression based on a complex network approach. Int. J. Neural Syst. 2015, 25. [Google Scholar] [CrossRef] [PubMed]
- Buscema, M.; Grossi, E.; Capriotti, M.; Babiloni, C.; Rossini, P. The IFAST Model allows the prediction of conversion to Alzheimer disease in patients with mild cognitive impairment with high degree of accuracy. Curr. Alzheimer Res. 2010, 7, 173–187. [Google Scholar] [CrossRef] [PubMed]
- Buscema, M.; Vernieri, F.; Massini, G.; Scrascia, F.; Breda, M.; Rossini, P.; Grossi, E. An improved I-FAST system for the diagnosis of Alzheimer’s disease from unprocessed electroencephalograms by using robust invariant features. Artif. Intell. Med. 2015, 64, 59–74. [Google Scholar] [CrossRef] [PubMed]
- Mammone, N.; Bonanno, L.; De Salvo, S.; Marino, S.; Bramanti, P.; Bramanti, A.; Morabito, M.F. Permutation disalignment index as an indirect, egg-based, measure of brain connectivity in MCI and AD patients. Int. J. Neural Syst. 2017, 27. [Google Scholar] [CrossRef] [PubMed]
- Seidkhani, H.; Nikolaev, A.R.; Meghanathan, R.N.; Pezeshk, H.; Masoudi-Nejad, A.; van Leeuwen, C. Task modulates functional connectivity networks in free viewing behavior. NeuroImage 2017, 159, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Rubinov, M.; Sporns, O. Complex network measures of brain connectivity: Uses and interpretations. Neuroimage 2010, 52, 1059–1069. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association (Ed.) Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Lake St. Louis, MO, USA, 2013. [Google Scholar]
- Vecchio, F.; Babiloni, C. Direction of information flow in Alzheimer’s disease and MCI patients. Int. J. Alzheimers Dis. 2011, 2011. [Google Scholar] [CrossRef] [PubMed]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [PubMed]
- What is EEGLAB? Available online: https://sccn.ucsd.edu/eeglab/index.php (accessed on 14 October 2017).
- Bandt, C.; Pompe, B. Permutation Entropy: A Natural Complexity Measure for Time Series. Phys. Rev. Lett. 2002, 88. [Google Scholar] [CrossRef] [PubMed]
- Renyi, A. On measures of information and entropy. In Proceedings of the Fourth Berkeley Symposium on Mathematical Statistics and Probability, Berkeley, CA, USA, 20–30 July 1960; pp. 547–561. [Google Scholar]
- Hild, K.E., II; Erdogmus, D.; Principe, J. Blind source separation using Renyi’s mutual information. IEEE Signal Proc. Lett. 2001, 8, 174–176. [Google Scholar] [CrossRef]
- Chapela, V.; Criado, R.; Moral, S.; Romance, M. Mathematical Foundations: Complex Networks and Graphs (A Review). In Intentional Risk Management through Complex Networks Analysis; Springer: Berlin, Germany, 2015; pp. 9–36. [Google Scholar]
- Fornito, A.; Zalesky, A.; Bullmore, E. Fundamentals of Brain Network Analysis; Academic Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Latora, V.; Marchiori, M. Efficient behavior of small-world networks. Phys. Rev. Lett. 2001, 87, 198701. [Google Scholar] [CrossRef] [PubMed]
- Ansmann, G.; Lehnertz, K. Surrogate-assisted analysis of weighted functional brain networks. J. Neurosci. Methods 2012, 208, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Watts, D.J.; Strogatz, S.H. Collective dynamics of small-world networks. Nature 1998, 393, 440–442. [Google Scholar] [CrossRef] [PubMed]
- Mann, H.B.; Whitney, D.R. On a test of whether one of two random variables is stochastically larger than the tther. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Bastos, A.M.; Schoffelen, J.M. A tutorial review of functional connectivity analysis methods and their interpretational pitfalls. Front. Syst. Neurosci. 2016, 9, 175. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pt ID | GENDER | AGE | MoCA Variation |
|---|---|---|---|
| Pt 3 | M | 68.00 | −2.00 |
| Pt 23 | F | 84.00 | 0.00 |
| Pt 30 | M | 78.00 | 0.00 |
| Pt 32 | M | 78.00 | −7.00 |
| Pt 41 | M | 78.00 | −6.00 |
| Pt 51 | F | 72.00 | −4.00 |
| Pt 71 | F | 79.00 | −3.00 |
| Pt 72 | F | 65.00 | 0.00 |
| Pt 127 | M | 74.00 | 0.00 |
| Pt 128 | F | 80.00 | 0.00 |
| Pt 129 | M | 78.00 | 0.00 |
| Pt 131 | F | 78.00 | −2.00 |
| Pt 132 | F | 73.00 | 0.00 |
| Pt 137 | F | 69.00 | 0.00 |
| Pt 143 | F | 78.00 | 5.00 |
| Pt 144 | M | 71.00 | 0.00 |
| Pt 146 | F | 56.00 | −1.00 |
| Pt 147 | M | 78.00 | 0.00 |
| Pt 150 | F | 58.00 | 0.00 |
| Pt 153 | M | 75.00 | 0.00 |
| Pt 155 | F | 75.00 | 0.00 |
| Pt 156 | F | 70.00 | −1.00 |
| Pt 157 | M | 79.00 | 0.00 |
| Pt 162 | M | 71.00 | 0.00 |
| Pt 164 | M | 76.00 | −2.00 |
| Pt 167 | M | 75.00 | 0.00 |
| Pt 173 | F | 70.00 | 0.00 |
| Pt 178 | M | 71.00 | −2.00 |
| Pt 180 | F | 78.00 | −3.00 |
| Pt 184 | F | 69.00 | −2.00 |
| Pt 185 | F | 79.00 | −3.00 |
| Pt 186 | M | 72.00 | 0.00 |
| Pt 193 | F | 67.00 | 0.00 |
| Patient | 0.5–32 Hz | Delta | Theta | Alpha | Beta |
|---|---|---|---|---|---|
| Pt 03 | 1.01 × 10 | 3.88 × 10 | 5.18 × 10 | 7.21 × 10 | 9.23 × 10 |
| Pt 23 | 2.57 × 10 | 5.80 × 10 | −8.90 × 10 | 1.05 × 10 | 1.04 × 10 |
| Pt 30 | 9.01 × 10 | 4.38 × 10 | 3.38 × 10 | 4.91 × 10 | 4.40 × 10 |
| Pt 32 | 1.58 × 10 | 9.91 × 10 | 2.82 × 10 | 1.36 × 10 | 3.59 × 10 |
| Pt 41 | 5.34 × 10 | 3.33 × 10 | 7.36 × 10 | 9.70 × 10 | 8.52 × 10 |
| Pt 51 | 1.01 × 10 | 7.81 × 10 | 6.50 × 10 | 8.20 × 10 | 1.16 × 10 |
| Pt 71 | 1.50 × 10 | 3.46 × 10 | 2.52 × 10 | 1.82 × 10 | 5.26 × 10 |
| Pt 72 | 2.06 × 10 | 1.93 × 10 | 7.33 × 10 | 8.37 × 10 | 3.14 × 10 |
| Pt 127 | 3.38 × 10 | 2.93 × 10 | 9.69 × 10 | 4.60 × 10 | 7.41 × 10 |
| Pt 128 | 9.42 × 10 | 4.03 × 10 | 6.49 × 10 | 4.72 × 10 | 5.45 × 10 |
| Pt 129 | 1.38 × 10 | 4.61 × 10 | 1.36 × 10 | 2.78 × 10 | 1.77 × 10 |
| Pt 131 | 4.58 × 10 | 3.85 × 10 | 1.26 × 10 | 5.29 × 10 | 3.45 × 10 |
| Pt 132 | 3.02 × 10 | 7.94 × 10 | 3.21 × 10 | 4.02 × 10 | 7.74 × 10 |
| Pt 137 | 4.04 × 10 | 6.08 × 10 | 2.08 × 10 | 7.93 × 10 | 2.99 × 10 |
| Pt 143 | 9.31 × 10 | 5.87 × 10 | 3.58 × 10 | 1.61 × 10 | 1.85 × 10 |
| Pt 144 | 6.91 × 10 | 1.70 × 10 | 8.17 × 10 | 5.27 × 10 | 1.75 × 10 |
| Pt 146 | 1.49 × 10 | 4.46 × 10 | 1.21 × 10 | 5.46 × 10 | 7.81 × 10 |
| Pt 147 | 1.57 × 10 | 9.49 × 10 | 7.73 × 10 | 1.57 × 10 | 7.40 × 10 |
| Pt 150 | 3.57 × 10 | 3.90 × 10 | 3.04 × 10 | 1.20 × 10 | 5.52 × 10 |
| Pt 153 | 6.36 × 10 | 5.56 × 10 | 3.41 × 10 | 1.54 × 10 | 9.68 × 10 |
| Pt 155 | 2.12 × 10 | 7.39 × 10 | 4.20 × 10 | 5.64 × 10 | 2.24 × 10 |
| Pt 156 | 3.72 × 10 | 5.76 × 10 | 1.72 × 10 | 1.08 × 10 | 8.28 × 10 |
| Pt 157 | 2.69 × 10 | 1.64 × 10 | 4.03 × 10 | 4.61 × 10 | 6.17 × 10 |
| Pt 162 | 7.74 × 10 | 4.91 × 10 | 4.33 × 10 | 7.97 × 10 | 1.06 × 10 |
| Pt 164 | 1.24 × 10 | 1.54 × 10 | 2.39 × 10 | 1.42 × 10 | 5.47 × 10 |
| Pt 167 | 6.93 × 10 | 1.61 × 10 | 2.03 × 10 | 6.05 × 10 | 2.75 × 10 |
| Pt 173 | 1.75 × 10 | 5.98 × 10 | 1.15 × 10 | 3.29 × 10 | 8.70 × 10 |
| Pt 178 | 1.34 × 10 | 3.66 × 10 | 1.10 × 10 | 3.05 × 10 | 2.30 × 10 |
| Pt 180 | 7.47 × 10 | 1.36 × 10 | 1.25 × 10 | 1.24 × 10 | 8.17 × 10 |
| Pt 184 | 2.20 × 10 | 5.46 × 10 | 1.27 × 10 | 6.22 × 10 | 1.57 × 10 |
| Pt 185 | 3.12 × 10 | 1.72 × 10 | 6.75 × 10 | 1.23 × 10 | 1.21 × 10 |
| Pt 186 | 2.80 × 10 | 1.41 × 10 | 7.03 × 10 | 2.27 × 10 | 3.62 × 10 |
| Pt 193 | 6.45 × 10 | 3.51 × 10 | 2.55 × 10 | 7.70 × 10 | 2.59 × 10 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mammone, N.; De Salvo, S.; Ieracitano, C.; Marino, S.; Marra, A.; Corallo, F.; Morabito, F.C. A Permutation Disalignment Index-Based Complex Network Approach to Evaluate Longitudinal Changes in Brain-Electrical Connectivity. Entropy 2017, 19, 548. https://doi.org/10.3390/e19100548
Mammone N, De Salvo S, Ieracitano C, Marino S, Marra A, Corallo F, Morabito FC. A Permutation Disalignment Index-Based Complex Network Approach to Evaluate Longitudinal Changes in Brain-Electrical Connectivity. Entropy. 2017; 19(10):548. https://doi.org/10.3390/e19100548
Chicago/Turabian StyleMammone, Nadia, Simona De Salvo, Cosimo Ieracitano, Silvia Marino, Angela Marra, Francesco Corallo, and Francesco C. Morabito. 2017. "A Permutation Disalignment Index-Based Complex Network Approach to Evaluate Longitudinal Changes in Brain-Electrical Connectivity" Entropy 19, no. 10: 548. https://doi.org/10.3390/e19100548
APA StyleMammone, N., De Salvo, S., Ieracitano, C., Marino, S., Marra, A., Corallo, F., & Morabito, F. C. (2017). A Permutation Disalignment Index-Based Complex Network Approach to Evaluate Longitudinal Changes in Brain-Electrical Connectivity. Entropy, 19(10), 548. https://doi.org/10.3390/e19100548