A Comparison of Postural Stability during Upright Standing between Normal and Flatfooted Individuals, Based on COP-Based Measures

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Equipment
2.3. COP-Based Measures
2.3.1. Traditional COP Methods
2.3.2. Entropy Methods
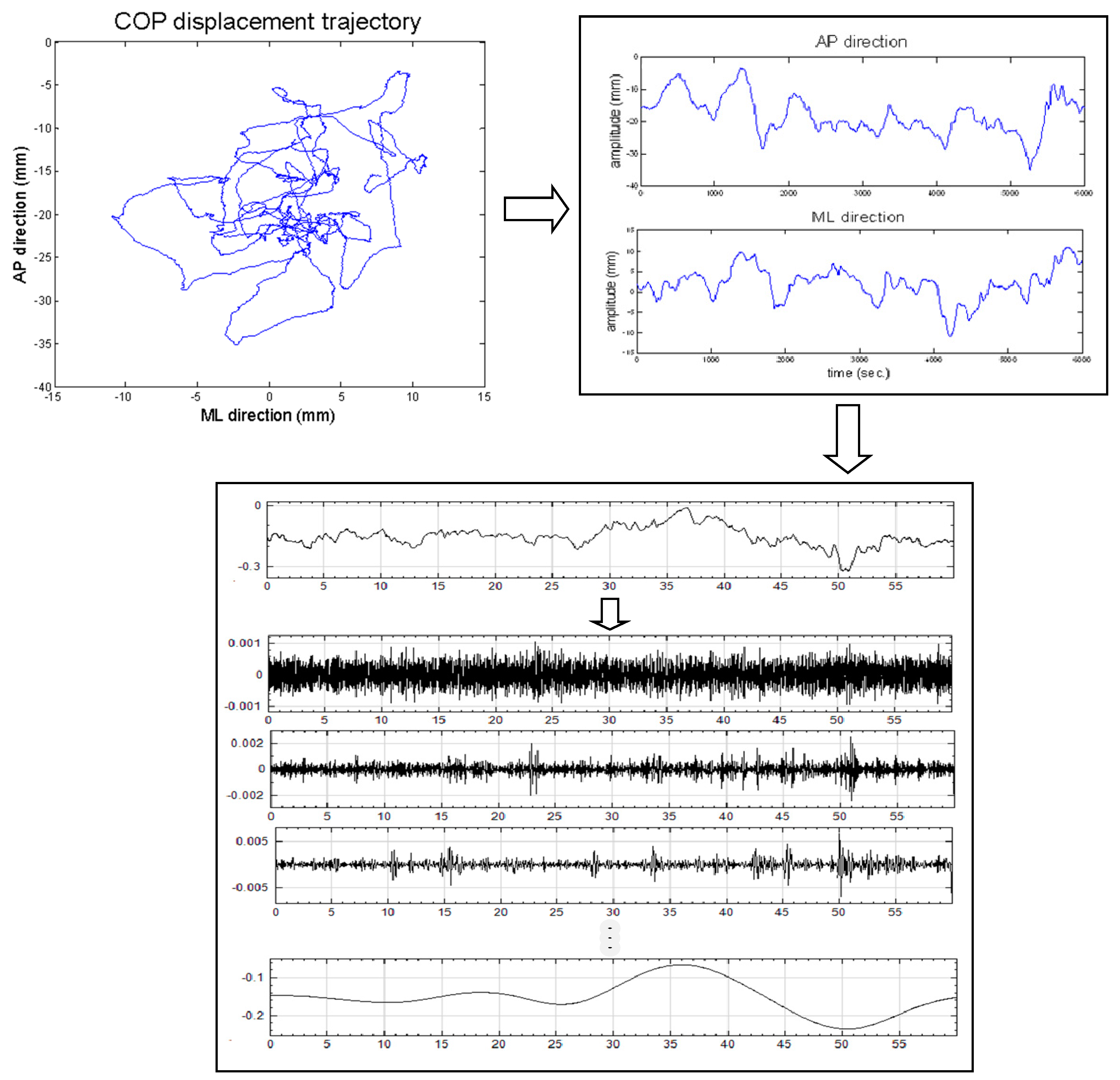
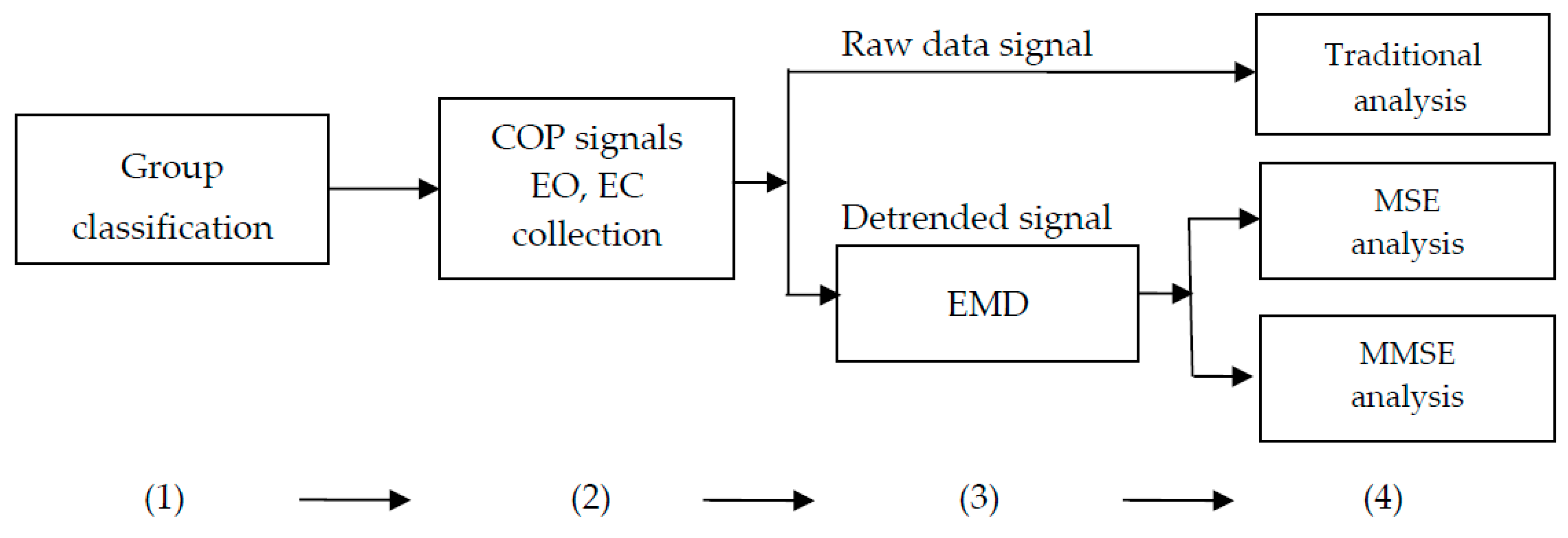
2.4. Data Analysis
2.5. Statistics
3. Results
3.1. Traditional COP-Based Measures
3.2. Entropy Measures
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Scott, G.; Menz, H.B.; Newcombe, L. Age-related differences in foot structure and function. Gait Posture 2007, 26, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Staheli, L.T.; Chew, D.E.; Corbett, M. The longitudinal arch: A survey of eight hundred and eighty-two feet in normal children and adults. J. Bone Jt. Surg. Am. 1987, 69, 426–428. [Google Scholar]
- Hue, O.; Simoneau, M.; Marcotte, J.; Berrigan, F.; Doré, J.; Marceau, P.; Marceau, S.; Tremblay, A.; Teasdale, N. Body weight is a strong predictor of postural stability. Gait Posture 2007, 26, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Christensen, K. Flat Feet in Adults. Available online: http://www.dynamicchiropractic.com/mpacms/dc/article.php?id=17842 (accessed on 15 February 2017).
- Otman, S.; Basgöze, O.; Gökce-Kutsal, Y. Energy cost of walking with flat feet. Prosthet. Orthot. Int. 1988, 12, 73–76. [Google Scholar] [PubMed]
- Laughton, C.A.; Slavin, M.; Katdare, K.; Nolan, L.; Bean, J.F.; Kerrigan, D.C.; Phillips, E.; Lipsitz, L.A.; Collins, J.J. Aging, muscle activity, and balance control: Physiologic changes. Gait Posture 2003, 18, 101–108. [Google Scholar] [CrossRef]
- Badlissi, F.; Dunn, J.E.; Link, C.L.; Keysor, J.J.; McKinlay, J.B.; Felson, D.T. Foot musculoskeletal disorders, pain, and foot-related functional limitation in older persons. J. Am. Geriatr. Soc. 2005, 53, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- Anzai, E.; Nakajima, K.; Iwakami, Y.; Sato, M.; Ino, S.; Ifukube, T.; Yamashita, K.; Ohta, Y. Effects of foot arch structure on postural stability. Clin. Res. Foot Ankle 2014. [Google Scholar] [CrossRef]
- Cobb, S.C.; Bazett-Jones, D.M.; Joshi, M.N.; Earl-Boehm, J.E.; James, C.R. The relationship among foot posture, core and lower extremity muscle function, and postural stability. J. Athl. Train. 2014, 49, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Tsai, L.C.; Yu, B.; Mercer, V.S.; Gross, M.T. Comparison of different structural foot types for measures of standing postural control. J. Orthop. Sports Phys. Ther. 2006, 36, 942–953. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Lou, S.Z.; Huang, C.Y.; Su, F.C. Effects of foot orthoses on gait patterns of flat feet patients. Clin. Biomech. 2010, 25, 265–270. [Google Scholar] [CrossRef]
- Evans, A.M.; Rome, K.A. Cochrane review of the evidence for non-surgical interventions for flexible pediatric flat feet. Eur. J. Phys. Rehabil. Med. 2011, 47, 69–89. [Google Scholar] [PubMed]
- MacKenzie, A.J.; Rome, K.; Evans, A.M. The efficacy of nonsurgical interventions for pediatric flexible flat foot: A critical review. J. Pediatr. Orthop. 2012, 32, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Banwell, H.A.; Mackintosh, S.; Thewlis, D. Foot orthoses for adults with flexible pes planus: A systematic review. J. Foot Ankle Res. 2014, 7. [Google Scholar] [CrossRef]
- Prieto, T.E.; Myklebust, J.B.; Hoffmann, R.G.; Lovett, E.G.; Myklebust, B.M. Measures of postural steadiness: differences between healthy young and elderly adults. IEEE Trans. Biomed. Eng. 1996, 43, 956–966. [Google Scholar] [CrossRef]
- Van Emmerik, R.E.A.; van Wegen, E.E.H. On variability and stability in human movement. J. Appl. Biomech. 2000, 16, 394–406. [Google Scholar] [CrossRef]
- Van Wegen, E.E.H.; van Emmerik, R.E.A.; Riccio, G.E. Postural orientation: Age-related changes in variability and time-to-boundary. Hum. Mov. Sci. 2002, 21, 61–84. [Google Scholar] [CrossRef]
- Huang, C.W.; Sue, P.D.; Abbod, M.F.; Jiang, B.C.; Shieh, J.-S. Measuring center of pressure signals to quantify human balance using multivariate multiscale entropy by designing a force platform. Sensors 2013, 13, 10151–10166. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.; Priplata, A.A.; Lipsitz, L.A.; Wu, Z.; Huang, N.E.; Goldberger, A.L.; Peng, C.K. Noise and poise: Enhancement of postural complexity in the elderly with a stochastic-resonance-based therapy. Europhys. Lett. 2007, 77, 68008. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.C.; Yang, W.H.; Shieh, J.S.; Fan, J.S.Z.; Peng, C.K. Entropy-based method for COP data analysis. Theor. Issues Ergon. Sci. 2013, 14, 227–246. [Google Scholar] [CrossRef]
- Pincus, S.M. Approximate entropy as a measure of system complexity. Proc. Natl. Acad. Sci. USA 1991, 88, 2297–2301. [Google Scholar] [CrossRef]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of complex physiologic time series. Phys. Rev. Lett. 2002, 89, 068102. [Google Scholar] [CrossRef] [PubMed]
- Huang, N.E.; Shen, Z.; Long, S.R.; Wu, M.C.; Shih, H.H.; Zheng, Q.; Yen, N.C.; Tung, C.C.; Liu, H.H. The empirical mode decomposition and the Hilbert spectrum for nonlinear and non-stationary time series analysis. Proc. R. Soc. Lond. A 1998, 454, 903–995. [Google Scholar] [CrossRef]
- Ahmed, M.U.; Mandic, D.P. Multivariate multiscale entropy: A tool for complexity analysis of multichannel data. Phys. Rev. E 2011, 84, 061918. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.U.; Rehman, N.; Looney, D.; Rutkowski, T.M.; Mandic, D.P. Dynamical complexity of human responses: A multivariate data-adaptive framework. Bull. Pol. Acad. Sci. Tech. 2012, 60, 433–445. [Google Scholar] [CrossRef]
- Ahmed, M.U.; Mandic, D.P. Multivariate multiscale entropy analysis. IEEE Signal Process. Lett. 2012, 19, 91–94. [Google Scholar] [CrossRef]
- Looney, D.; Ahmed, M.U.; Mandic, D.P. Human-centred multivariate complexity analysis. Nat. Intell. 2012, 1, 40–43. [Google Scholar]
- Acharya, U.R.; Fujita, H.; Sudarshan, V.K.; Bhat, S.; Koh, J.E. Application of entropies for automated diagnosis of epilepsy using EEG signals: A review. Knowl. Based Syst. 2015, 88, 85–96. [Google Scholar] [CrossRef]
- Sharma, R.; Pachori, R.B.; Acharya, U.R. Application of entropy measures on intrinsic mode functions for the automated identification of focal electroencephalogram signals. Entropy 2015, 17, 669–691. [Google Scholar] [CrossRef]
- Huang, J.R.; Fan, S.Z.; Abbod, M.F.; Jen, K.K.; Wu, J.F.; Shieh, J.S. Application of multivariate empirical mode decomposition and sample entropy in EEG signals via artificial neural networks for interpreting depth of anesthesia. Entropy 2013, 15, 3325–3339. [Google Scholar] [CrossRef]
- Wei, Q.; Liu, D.H.; Wang, K.H.; Liu, Q.; Abbod, M.F.; Jiang, B.C.; Chen, K.P.; Wu, C.; Shieh, J.S. Multivariate multiscale entropy applied to center of pressure signals analysis: An effect of vibration stimulation of shoes. Entropy 2012, 14, 2157–2172. [Google Scholar] [CrossRef]
- Chao, T.C.; Jiang, B.C. Multi-scale entropy analysis for evaluating the balance of the flatfeet. In Advances in Usability Evaluation, 1st ed.; Soarse, M.M., Rebelo, F., Eds.; CRC Press: Boca Raton, FL, USA, 2012; pp. 76–86. [Google Scholar]
- Razeghi, M.; Batt, M.E. Foot type classification: A critical review of current methods. Gait Posture 2002, 15, 282–291. [Google Scholar] [CrossRef]
- Le Clair, K.; Riach, C. Postural stability measures: What to measure and for how long. Clin. Biomech. 1996, 11, 176–178. [Google Scholar] [CrossRef]
- Hafström, A.; Fransson, P.A.; Karlberg, M.; Ledin, T.; Magnusson, M. Visual influence on postural control, with and without visual motion feedback. Acta Oto-laryngol. 2002, 122, 392–397. [Google Scholar] [CrossRef]
- Cost, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of biological signals. Phys. Rev. E 2005, 71, 021906. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.H.; Jiang, B.C. Multi-scale entropy analysis for postural sway signals with attention influence for elderly and young subjects. In Advances in Human Factors and Ergonomics in Healthcare; Duffy, V.G., Ed.; CRC Press: Boca Raton, FL, USA, 2010; pp. 422–431. [Google Scholar]
- Ramdani, S.; Seigle, B.; Lagarde, J.; Bouchara, F.; Bernard, P.L. On the use of sample entropy to analyze human postural sway data. Med. Eng. Phys. 2009, 31, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Gow, B.J.; Peng, C.K.; Wayne, P.M.; Ahn, A.C. Multiscale entropy analysis of center-of-pressure dynamics in human postural control: Methodological considerations. Entropy 2015, 17, 7926–7947. [Google Scholar] [CrossRef]
- Freitas, S.M.; Wieczorek, S.A.; Marchetti, P.H.; Duarte, M. Age-related changes in human postural control of prolonged standing. Gait Posture 2005, 22, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Duarte, M.; Zatsiorsky, V.M. Effects of body lean and visual information on the equilibrium maintenance during stance. Exp. Brain Res. 2002, 146, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Dabholkar, A.; Shah, A.; Yardi, S. Comparison of dynamic balance between flat feet and normal individuals using star excursion balance test. Indian J. Physiother. Occup. Ther. 2012, 6, 27–31. [Google Scholar]
- Han, J.T.; Koo, H.M.; Jung, J.M.; Kim, Y.J.; Lee, J.H. Differences in plantar foot pressure and COP between flat and normal feet during walking. J. Phys. Ther. Sci. 2011, 23, 683–685. [Google Scholar] [CrossRef]
- Kim, J.A.; Lim, O.B.; Yi, C.H. Difference in static and dynamic stability between flexible flatfeet and neutral feet. Gait Posture 2015, 41, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Hilliard, M.J.; Martinez, K.M.; Janssen, I.; Edwards, B.; Mille, M.L.; Zhang, Y.; Rogers, M.W. Lateral balance factors predict future falls in community-living older adults. Arch. Phys. Med. Rehabil. 2008, 89, 1708–1713. [Google Scholar] [CrossRef] [PubMed]
- Lizama, L.E.C.; Pijnappels, M.; Reeves, N.P.; Verschueren, S.M.; van Dieën, J.H. Frequency domain mediolateral balance assessment using a center of pressure tracking task. J. Biomech. 2013, 46, 2831–2836. [Google Scholar] [CrossRef] [PubMed]
- Harrison, P.L.; Littlewood, C. Relationship between pes planus foot type and postural stability. Indian J. Physiother. Occup. Ther. 2010, 4, 21–24. [Google Scholar]
- Ur Rehman, N.; Mandic, D.P. Filter bank property of multivariate empirical mode decomposition. IEEE Trans. Signal Proces. 2011, 59, 2421–2426. [Google Scholar] [CrossRef]
- Mandic, D.P.; Ur Rehman, N.; Wu, Z.; Huang, N.E. Empirical mode decomposition-based time-frequency analysis of multivariate signals: The power of adaptive data analysis. IEEE Signal Proc. Mag. 2013, 30, 74–86. [Google Scholar] [CrossRef]
- Ur Rehman, N.; Park, C.; Huang, N.E.; Mandic, D.P. EMD via MEMD: Multivariate noise-aided computation of standard EMD. Adv. Adapt. Data Anal. 2013, 5. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Participants | Footprint Type (mean ± SD) | p-Value | |
|---|---|---|---|
| Flatfooted (n = 17) | Normal (n = 37) | ||
| Males | 13 | 16 | |
| Females | 4 | 21 | |
| Arch index (R) | 1.26 ± 0.17 | 0.71 ± 0.09 | 0.000 |
| Age (years) | 22.53 ± 1.42 | 23.62 ± 2.29 | 0.076 |
| Height (cm) | 169.79 ± 7.93 | 165.76 ± 7.63 | 0.081 |
| Weight (kg) | 68.44 ± 13.23 | 60.93 ± 10.35 | 0.051 |
| BMI (kg/m2) | 23.59 ± 3.06 | 22.06 ± 2.56 | 0.062 |
| Measures (Units) | EO | EC | ||||||
|---|---|---|---|---|---|---|---|---|
| Flatfooted (n = 17) | Normal (n = 37) | t-Value | p-Value | Flatfooted (n = 17) | Normal (n = 37) | t-Value | p-Value | |
| MDIST (mm) | 3.51 ± 1.23 | 2.77 ± 1.10 | 2.23 | 0.030 * | 3.83 ± 2.27 | 3.05 ± 1.19 | 1.66 | 0.102 |
| MDIST_AP (mm) | 2.68 ± 1.01 | 2.18 ± 0.89 | 1.81 | 0.077 | 3.01 ± 1.77 | 2.41 ± 0.92 | 1.65 | 0.106 |
| MDIST_ML (mm) | 1.73 ± 0.77 | 1.26 ± 0.63 | 2.38 | 0.021 * | 1.77 ± 1.22 | 1.39 ± 0.85 | 1.32 | 0.192 |
| RDIST (mm) | 4.03 ± 1.40 | 3.20 ± 1.26 | 2.17 | 0.034 * | 4.44 ± 2.57 | 3.54 ± 1.37 | 1.67 | 0.100 |
| RDIST_AP (mm) | 3.32 ± 1.23 | 2.73 ± 1.11 | 1.74 | 0.087 | 3.78 ± 2.19 | 3.02 ± 1.11 | 1.70 | 0.094 |
| RDIST_ML (mm) | 2.17 ± 0.95 | 1.57 ± 0.77 | 2.47 | 0.017 * | 2.22 ± 1.51 | 1.73 ± 1.04 | 1.39 | 0.171 |
| TOTEX (mm) | 523.8 ± 106.6 | 508.8 ± 81.9 | 0.57 | 0.572 | 602.2 ± 161.6 | 579.7 ± 103.2 | 0.62 | 0.540 |
| TOTEX_AP (mm) | 376.6 ± 83.4 | 358.7 ± 52.3 | 0.96 | 0.339 | 442.5 ± 124.9 | 424.3 ± 76.6 | 0.66 | 0.512 |
| TOTEX_ML (mm) | 282.6 ± 63.4 | 283.0 ± 57.2 | −0.02 | 0.985 | 312.2 ± 96.8 | 304.0 ± 69.9 | 0.36 | 0.723 |
| MVELO (mm/s) | 8.73 ± 1.78 | 8.48 ± 1.37 | 0.57 | 0.572 | 10.04 ± 2.69 | 9.66 ± 1.72 | 0.62 | 0.540 |
| MVELO_AP (mm/s) | 6.28 ± 1.39 | 5.98 ± 0.87 | 0.96 | 0.339 | 7.37 ± 2.08 | 7.07 ± 1.28 | 0.66 | 0.512 |
| MVELO_ML (mm/s) | 4.71 ± 1.06 | 4.72 ± 0.95 | −0.02 | 0.985 | 5.20 ± 1.61 | 5.07 ± 1.16 | 0.36 | 0.723 |
| AREA_CC (mm2) | 160.8 ± 126.9 | 106.3 ± 89.6 | 1.82 | 0.075 | 231.6 ± 370.1 | 130.4 ± 126.3 | 1.50 | 0.141 |
| AREA_SW (mm2/s) | 9.84 ± 5.03 | 5.03 ± 7.45 | 1.78 | 0.081 | 12.62 ± 11.85 | 9.06 ± 5.46 | 1.52 | 0.135 |
| Measures | EO | EC | ||||||
|---|---|---|---|---|---|---|---|---|
| Flatfooted (n = 17) | Normal (n = 37) | t-Value | p-Value | Flatfooted (n = 17) | Normal (n = 37) | t-Value | p-Value | |
| CI_AP_IMF1 | 26.15 ± 4.51 | 27.64 ± 2.15 | −1.65 | 0.105 | 24.78 ± 4.93 | 26.71 ± 3.3 | −1.69 | 0.098 |
| CI_AP_IMF2 | 15.75 ± 4.84 | 17.56 ± 4.07 | −1.43 | 0.16 | 15.69 ± 6.45 | 15.59 ± 5.65 | 0.06 | 0.954 |
| CI_AP_IMF3 | 10.17 ± 3.34 | 11.03 ± 3.04 | −0.93 | 0.357 | 10.36 ± 3.08 | 10.17 ± 2.87 | 0.22 | 0.829 |
| CI_AP_IMF4 | 11.21 ± 1.30 | 11.44 ± 1.83 | −0.45 | 0.655 | 11.26 ± 1.71 | 10.81 ± 1.71 | 0.91 | 0.368 |
| CI_AP_IMF5 | 8.92 ± 0.53 | 9.00 ± 0.780 | −0.37 | 0.711 | 8.54 ± 0.89 | 8.70 ± 0.90 | −0.61 | 0.544 |
| CI_AP_IMF6 | 6.47 ± 0.69 | 6.74 ± 0.826 | −1.18 | 0.245 | 6.22 ± 0.67 | 6.67 ± 0.73 | −2.15 | 0.036 * |
| CI_AP_IMF7 | 3.46 ± 0.85 | 3.63 ± 1.02 | −0.60 | 0.549 | 3.13 ± 0.82 | 3.59 ± 0.68 | −2.16 | 0.036 * |
| Measures | EO | EC | ||||||
|---|---|---|---|---|---|---|---|---|
| Flatfooted (n = 17) | Normal (n = 37) | t-Value | p-Value | Flatfooted (n = 17) | Normal (n = 37) | t-Value | p-Value | |
| CI_ML_IMF1 | 28.30 ± 1.35 | 28.44 ± 1.16 | −0.39 | 0.695 | 28.20 ± 1.16 | 28.516 ± 0.66 | −1.29 | 0.201 |
| CI_ML_IMF2 | 21.00 ± 4.15 | 22.24 ± 4.03 | −0.98 | 0.332 | 18.34 ± 6.4 | 21.33 ± 5.36 | −1.78 | 0.081 |
| CI_ML_IMF3 | 10.54 ± 4.76 | 11.26 ± 4.65 | −0.53 | 0.599 | 9.44 ± 4.41 | 10.24 ± 3.92 | −0.67 | 0.507 |
| CI_ML_IMF4 | 9.37 ± 2.09 | 9.04 ± 2.59 | 0.46 | 0.65 | 9.39 ± 2.19 | 8.79 ± 2.11 | 0.95 | 0.346 |
| CI_ML_IMF5 | 8.71 ± 1.19 | 8.85 ± 1.36 | −0.38 | 0.705 | 8.66 ± 1.32 | 8.80 ± 1.32 | −0.36 | 0.719 |
| CI_ML_IMF6 | 7.05 ± 0.78 | 7.38 ± 0.86 | −1.33 | 0.188 | 6.75 ± 1.17 | 7.21 ± 0.80 | −1.70 | 0.095 |
| CI_ML_IMF7 | 3.72 ± 0.98 | 4.16 ± 0.97 | −1.54 | 0.129 | 3.82 ± 0.82 | 4.07 ± 0.85 | −1.02 | 0.312 |
| Measures | EO | EC | ||||||
|---|---|---|---|---|---|---|---|---|
| Flatfooted (n = 17) | Normal (n = 37) | t-Value | p-Value | Flatfooted (n = 17) | Normal (n = 37) | t-Value | p-Value | |
| CI_IMF1 | 5.80 ± 0.45 | 5.78 ± 0.41 | 0.13 | 0.894 | 5.74 ± 0.50 | 5.78 ± 0.52 | −0.27 | 0.787 |
| CI_IMF2 | 7.94 ± 1.68 | 7.81 ± 1.07 | 0.33 | 0.74 | 7.48 ± 1.94 | 7.53 ± 1.37 | −0.12 | 0.905 |
| CI_IMF3 | 7.30 ± 2.71 | 7.57 ± 2.19 | −0.40 | 0.693 | 7.08 ± 2.40 | 7.16 ± 1.84 | −0.13 | 0.895 |
| CI_IMF4 | 9.86 ± 2.22 | 9.63 ± 2.51 | 0.33 | 0.741 | 10.37 ± 2.28 | 9.41 ± 1.96 | 1.58 | 0.119 |
| CI_IMF5 | 12.53 ± 1.45 | 12.02 ± 1.78 | 1.04 | 0.303 | 12.49 ± 1.71 | 12.22 ± 1.85 | 0.50 | 0.619 |
| CI_IMF6 | 12.24 ± 1.11 | 12.41 ± 1.26 | −0.48 | 0.633 | 11.88 ± 1.34 | 12.27 ± 1.47 | −0.93 | 0.357 |
| CI_IMF7 | 10.64 ± 1.94 | 10.82 ± 1.23 | −0.42 | 0.679 | 10.36 ± 1.43 | 10.74 ± 1.16 | −1.06 | 0.296 |
| Measures | EO | EC | ||||||
|---|---|---|---|---|---|---|---|---|
| Flatfooted (n = 17) | Normal (n = 37) | t-Value | p-Value | Flatfooted (n = 17) | Normal (n = 37) | t-Value | p-Value | |
| CI_AP_IMF5,6 | 8.41 ± 0.72 | 8.65 ± 0.75 | −1.12 | 0.266 | 8.06 ± 0.92 | 8.35 ± 0.83 | −1.17 | 0.249 |
| CI_ML_IMF5,6 | 8.93 ± 1.00 | 9.39 ± 1.19 | −1.37 | 0.176 | 8.67 ± 1.31 | 9.37 ± 0.86 | −2.35 | 0.023 * |
| CI_IMF5,6 | 13.13 ± 1.36 | 13.52 ± 1.05 | −1.14 | 0.258 | 12.85 ± 1.23 | 13.41 ± 1.30 | −1.48 | 0.144 |
| CI_AP_IMF6,7 | 5.06 ± 0.92 | 5.53 ± 0.67 | −2.09 | 0.042 * | 4.50 ± 0.94 | 5.51 ± 0.73 | −4.30 | 0.000 * |
| CI_ML_IMF6,7 | 5.71 ± 0.82 | 6.22 ± 0.83 | −2.12 | 0.039 * | 5.76 ± 1.12 | 6.18 ± 0.83 | −1.53 | 0.133 |
| CI_IMF6,7 | 11.36 ± 1.43 | 11.57 ± 1.20 | −0.58 | 0.564 | 11.04 ± 1.05 | 11.54 ± 1.09 | −1.59 | 0.118 |
| CI_AP_IMF5,67 | 7.29 ± 1.04 | 7.69 ± 1.10 | −1.24 | 0.222 | 7.26 ± 0.82 | 7.71 ± 0.68 | −2.12 | 0.039 * |
| CI_ML_IMF5,67 | 8.09 ± 1.13 | 8.82 ± 1.31 | −1.97 | 0.054 | 8.15 ± 1.49 | 8.92±0.96 | −2.31 | 0.025 * |
| CI_IMF5,6,7 | 12.57 ± 1.04 | 12.82 ± 1.40 | −0.66 | 0.512 | 12.57 ± 0.97 | 13.19 ± 1.13 | −1.94 | 0.058 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chao, T.-C.; Jiang, B.C. A Comparison of Postural Stability during Upright Standing between Normal and Flatfooted Individuals, Based on COP-Based Measures. Entropy 2017, 19, 76. https://doi.org/10.3390/e19020076
Chao T-C, Jiang BC. A Comparison of Postural Stability during Upright Standing between Normal and Flatfooted Individuals, Based on COP-Based Measures. Entropy. 2017; 19(2):76. https://doi.org/10.3390/e19020076
Chicago/Turabian StyleChao, Tsui-Chiao, and Bernard C. Jiang. 2017. "A Comparison of Postural Stability during Upright Standing between Normal and Flatfooted Individuals, Based on COP-Based Measures" Entropy 19, no. 2: 76. https://doi.org/10.3390/e19020076
APA StyleChao, T. -C., & Jiang, B. C. (2017). A Comparison of Postural Stability during Upright Standing between Normal and Flatfooted Individuals, Based on COP-Based Measures. Entropy, 19(2), 76. https://doi.org/10.3390/e19020076