
Multiscale Entropy Analysis of the Differential RR Interval Time Series Signal and Its Application in Detecting Congestive Heart Failure


Abstract
:1. Introduction
2. Methods
2.1. Data
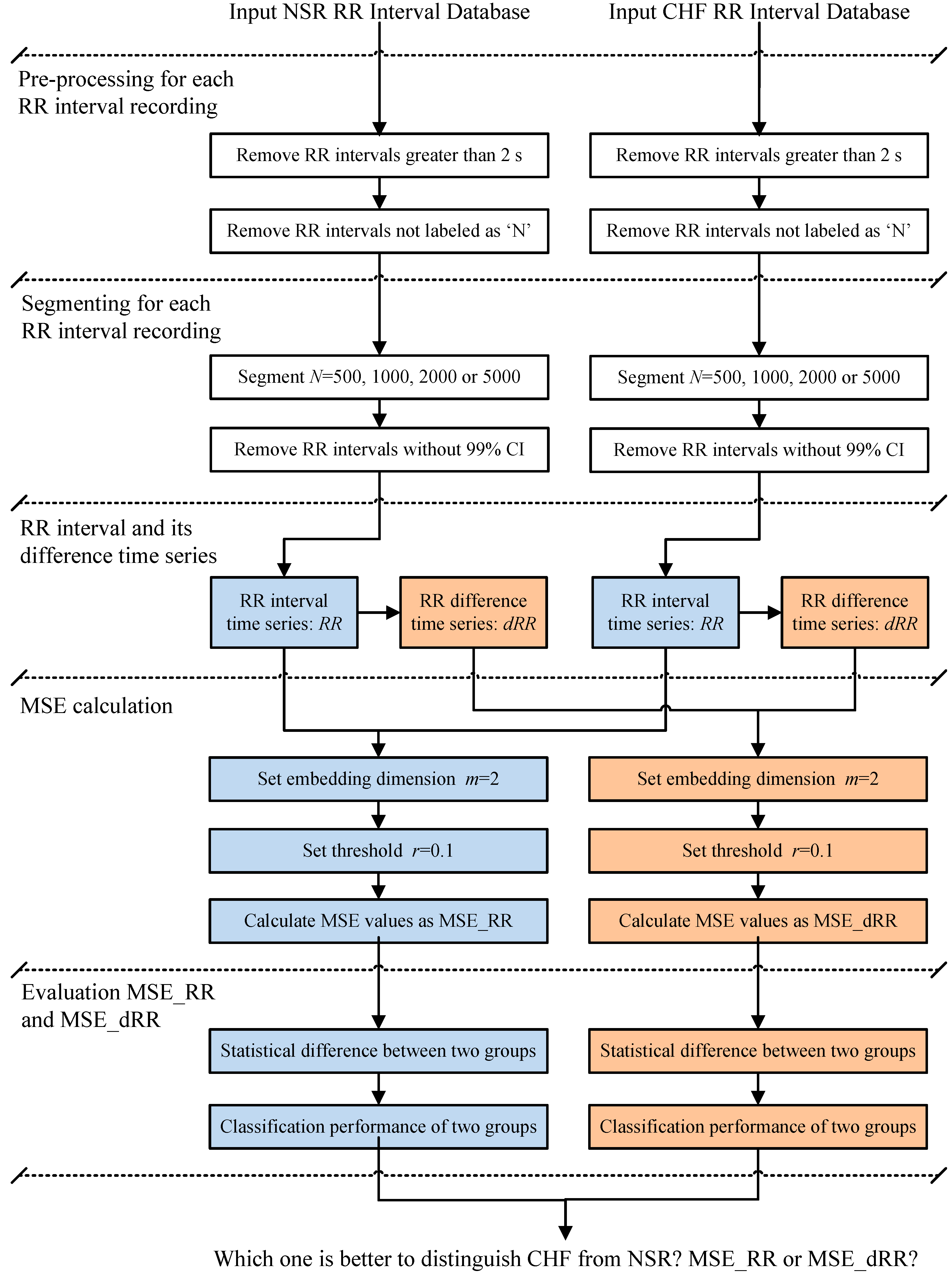
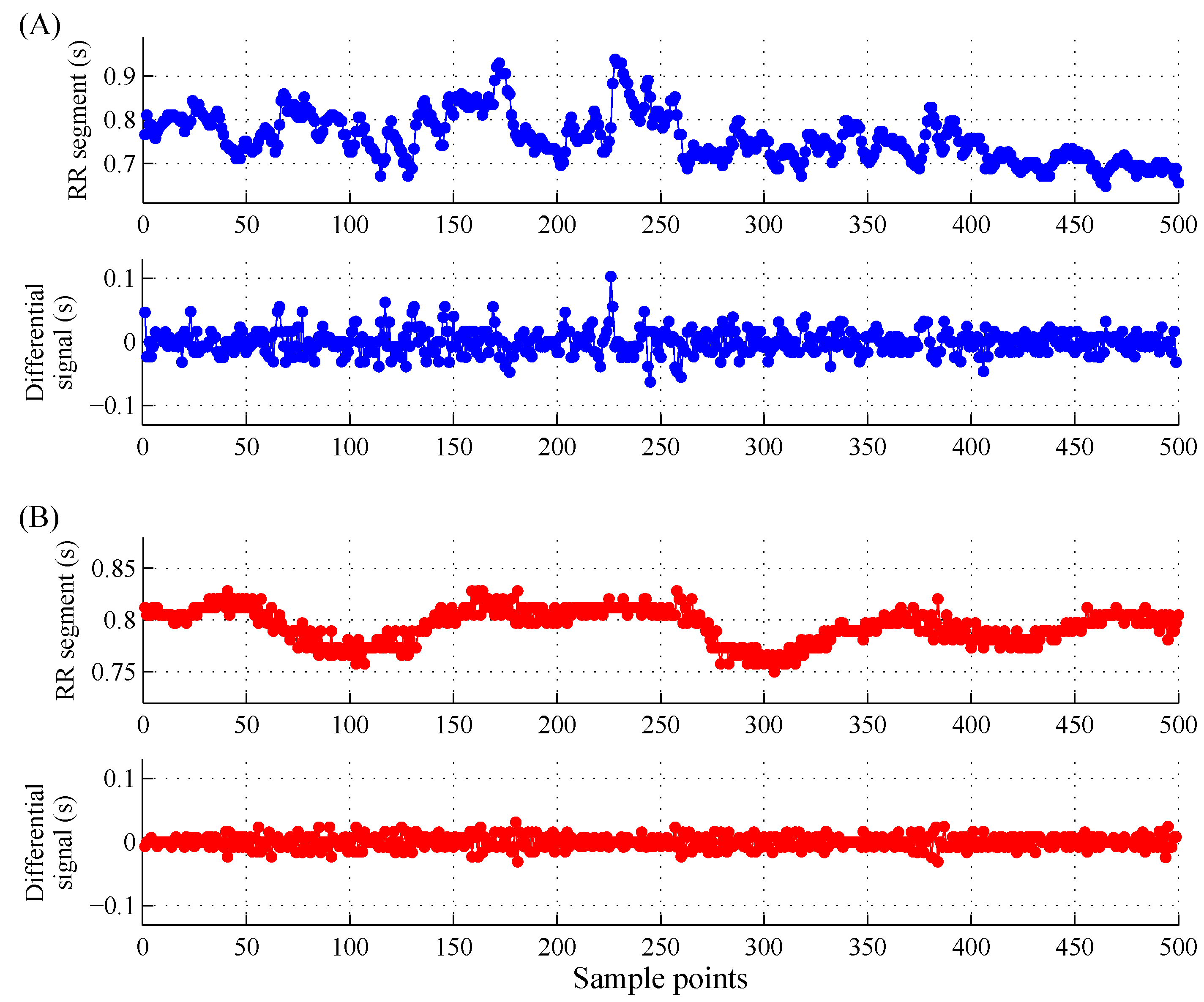
2.2. Method Description
2.3. Multiscale Entropy (MSE)
2.4. Statistical Analysis
3. Results
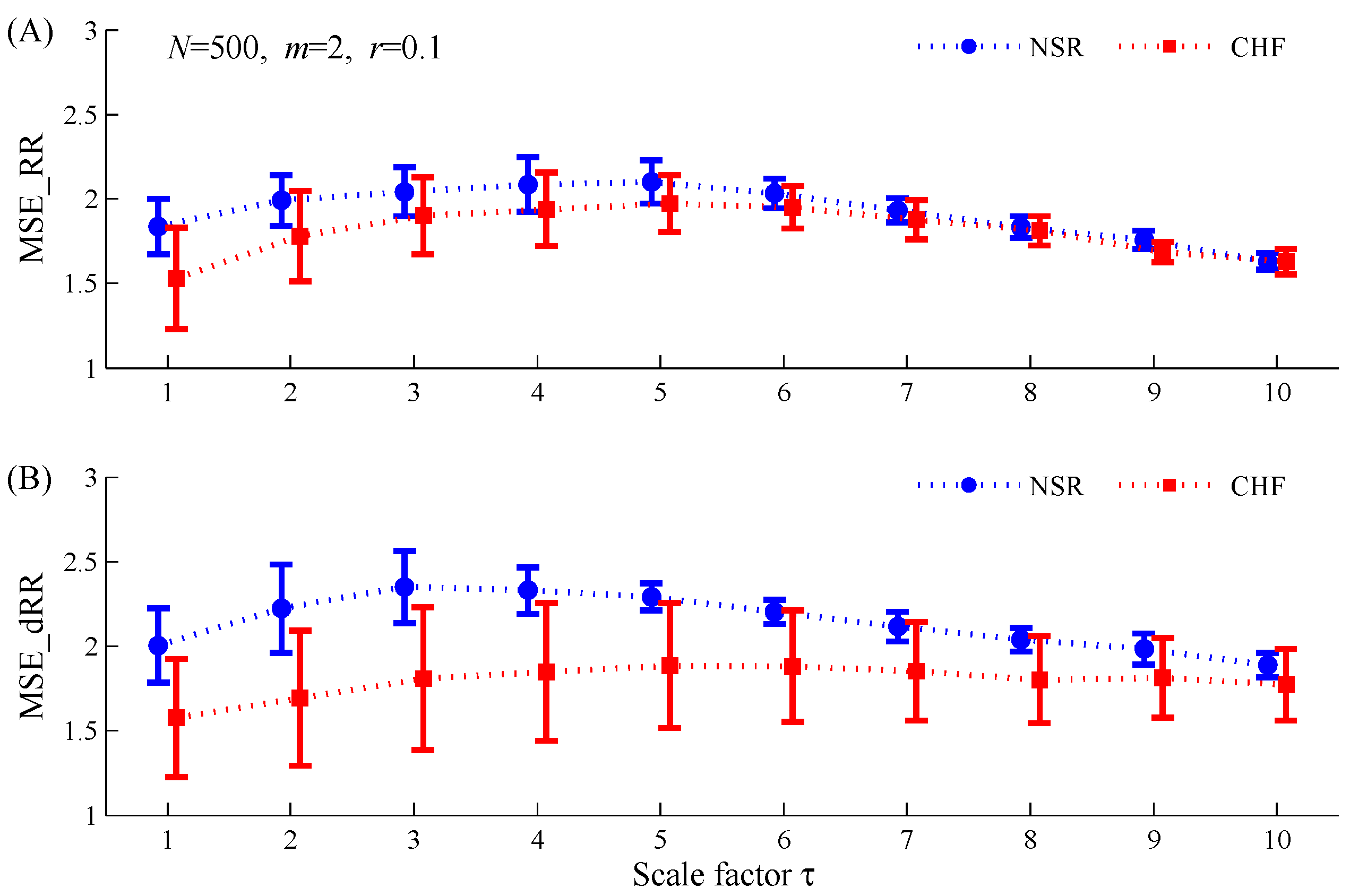
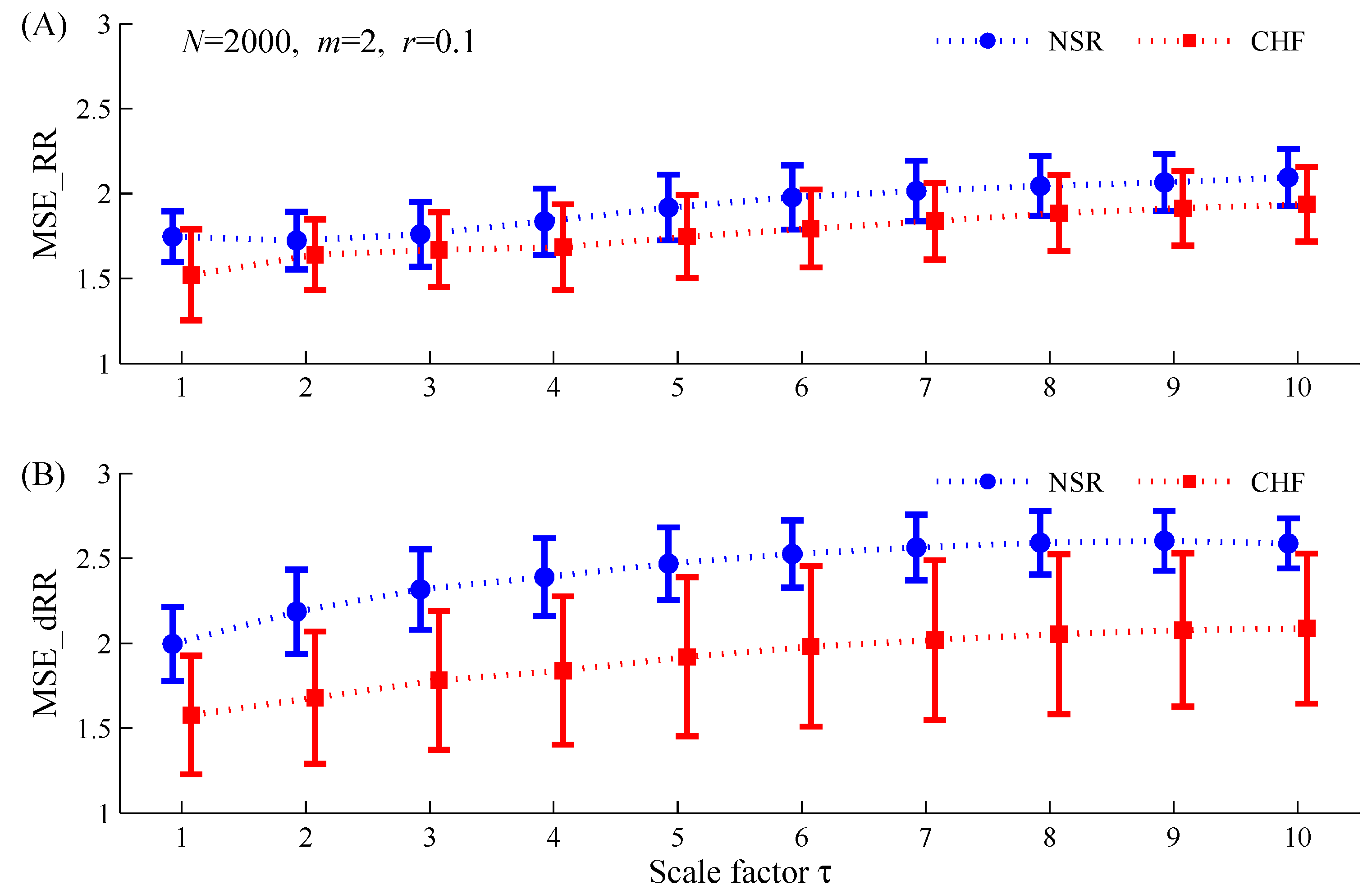
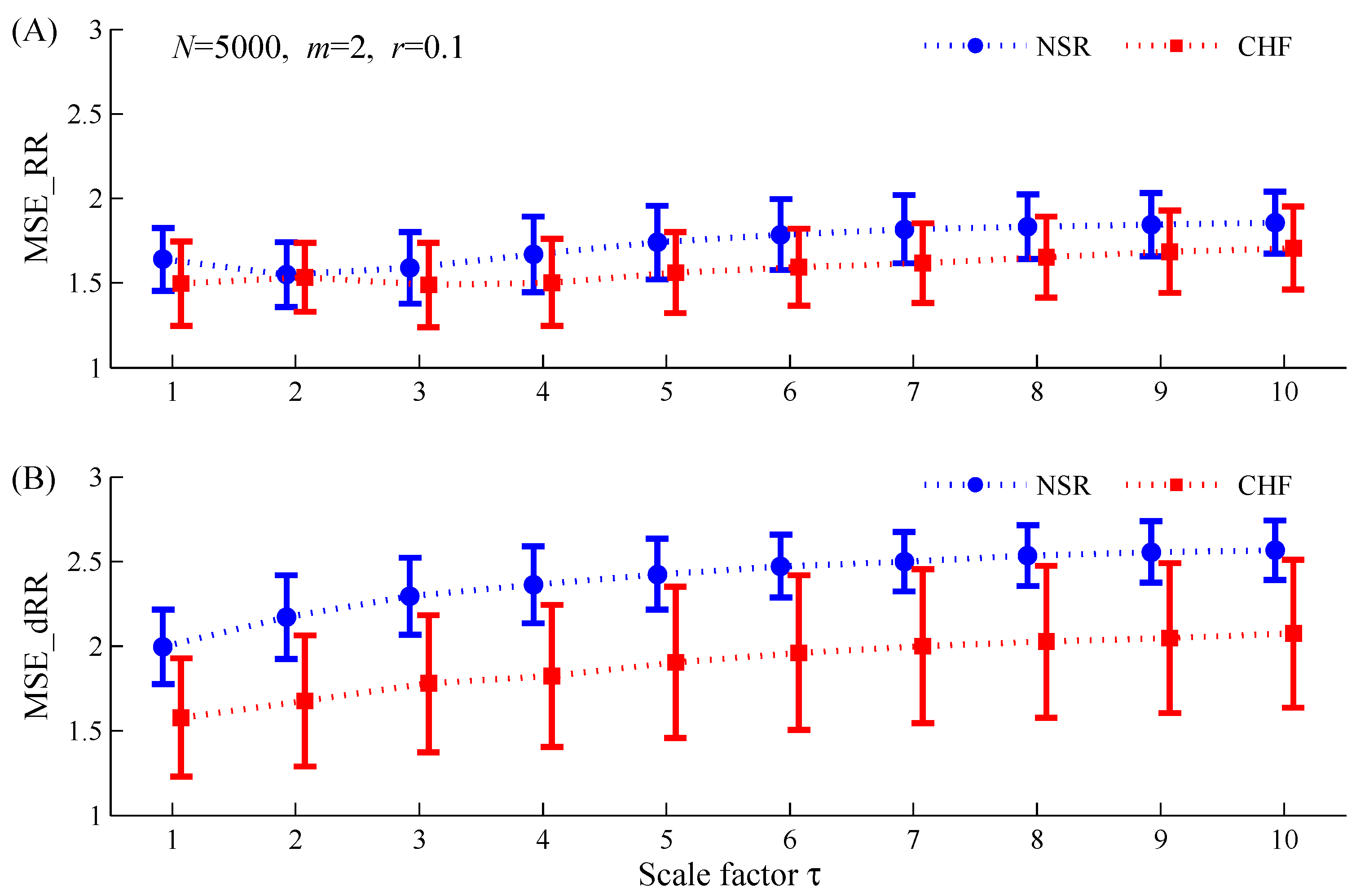
3.1. Statistical Differences of MSE_RR and MSE_dRR between the Two Groups
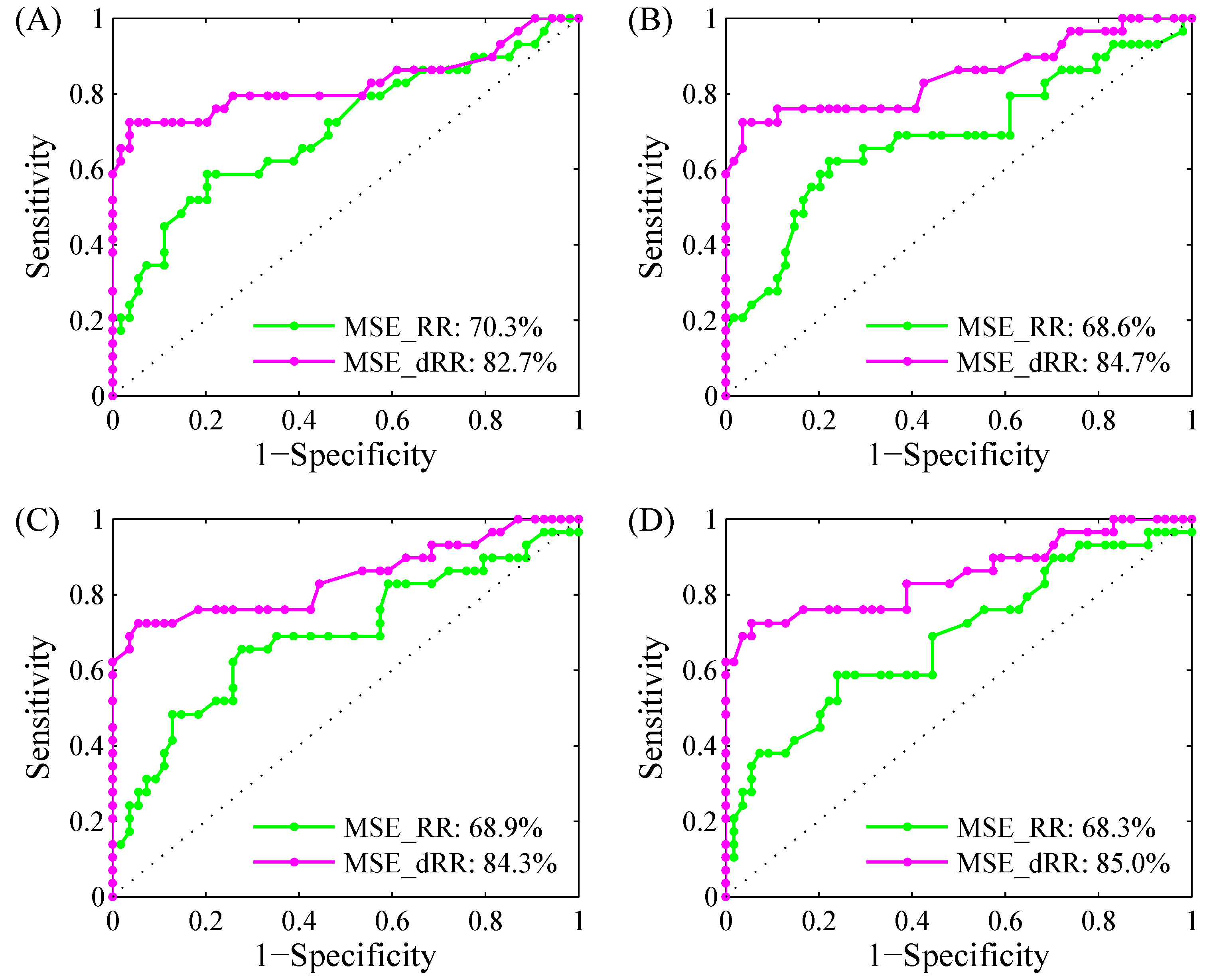
3.2. Classification Results Using ROC Curve Analysis
3.3. Classification Results Using 5-Fold Cross Validation SVM Classifier
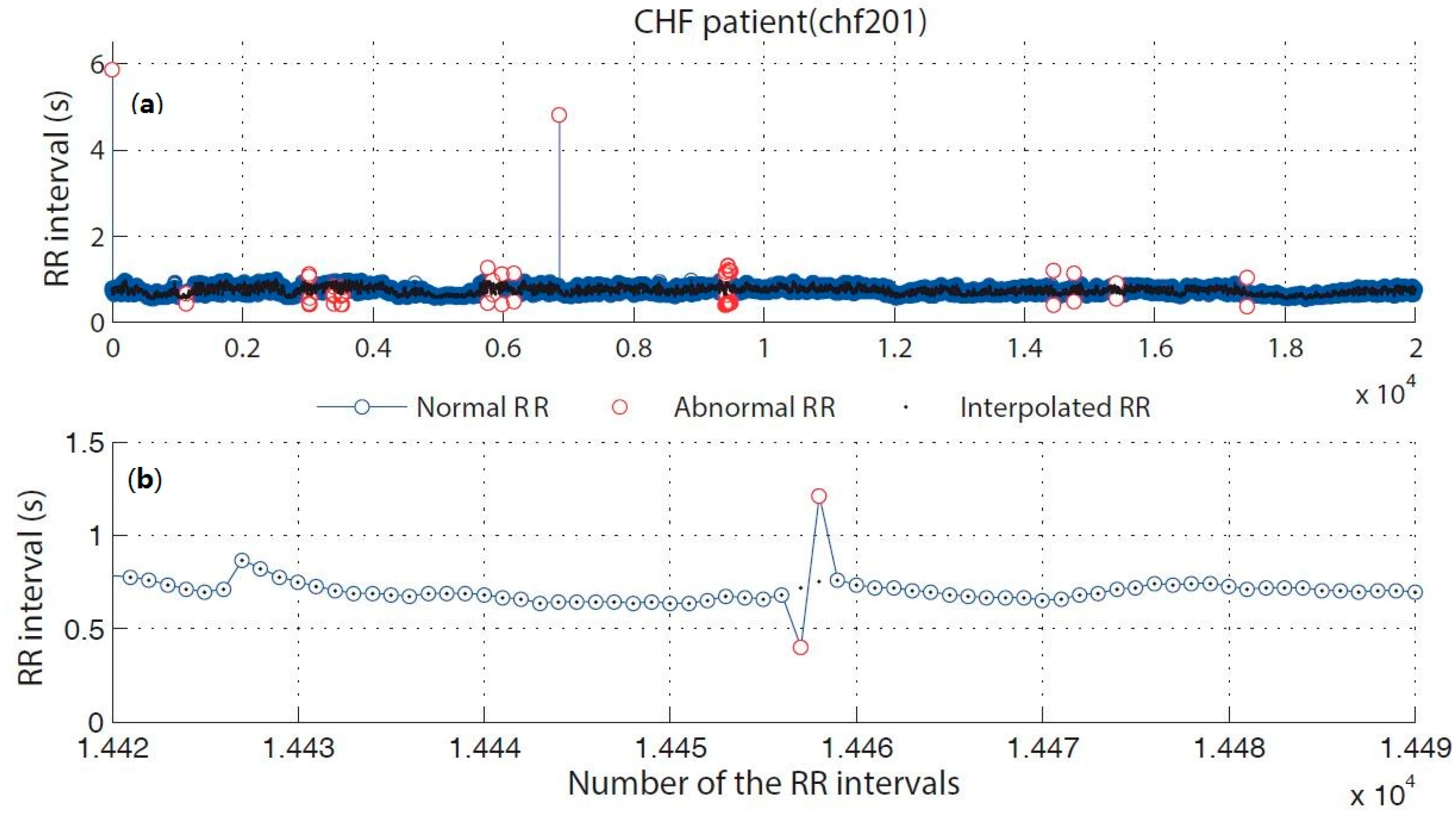
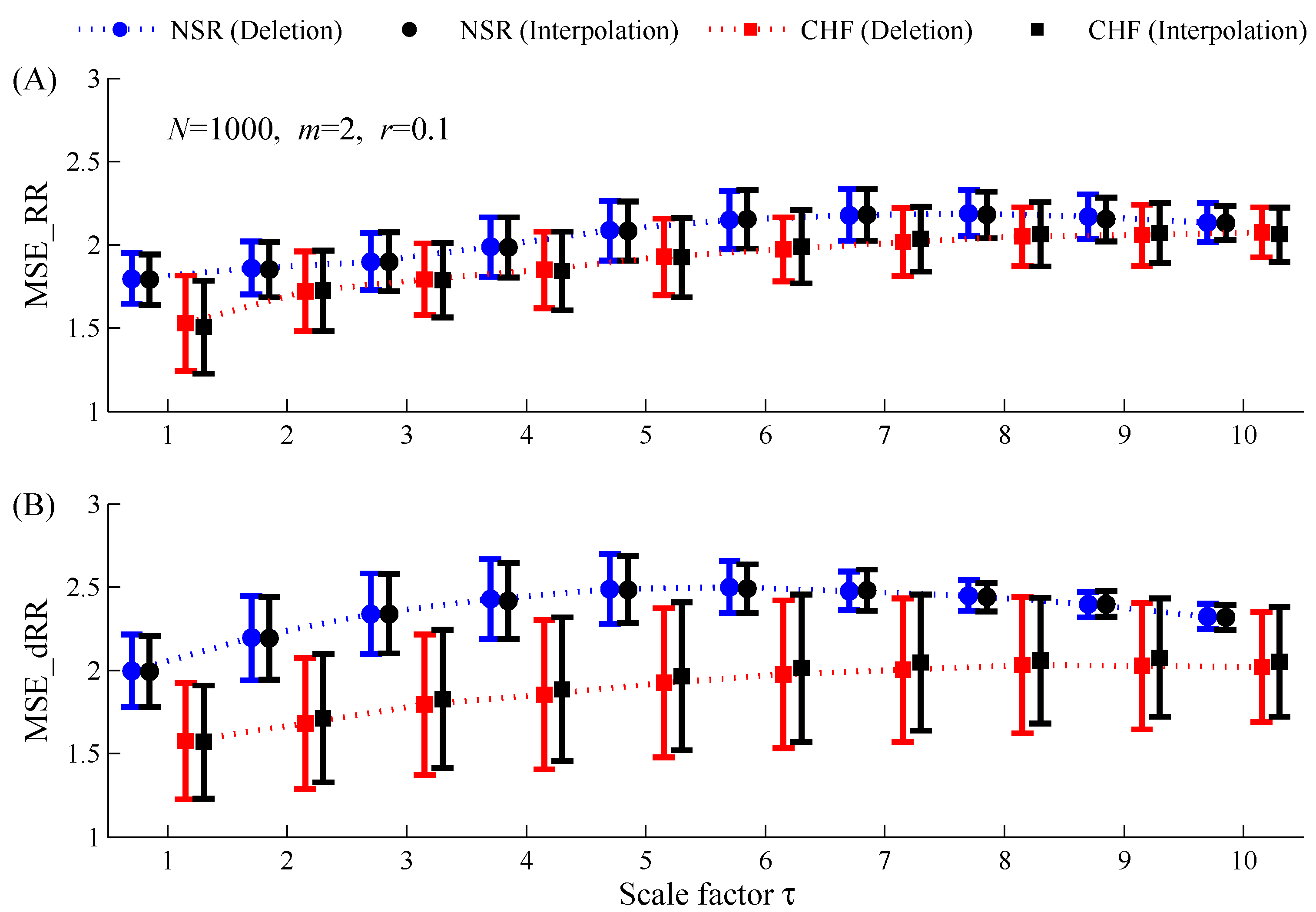
3.4. Comparison of Different Editing Methods for Abnormal RR Intervals
4. Discussions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Xiao, X.S.; Mullen, T.J.; Mukkamala, R. System identification: A multi-signal approach for probing neural cardiovascular regulation. Physiol. Meas. 2005, 26, R41–R71. [Google Scholar] [CrossRef] [PubMed]
- Bravi, A.; Longtin, A.; Seely, A.J. Review and classification of variability analysis techniques with clinical applications. Biomed. Eng. Online 2011, 10, 90. [Google Scholar] [CrossRef] [PubMed]
- İşler, Y.; Kuntalp, M. Combining classical HRV indices with wavelet entropy measures improves to performance in diagnosing congestive heart failure. Comput. Biol. Med. 2007, 37, 1502–1510. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.J.; Cohn, J.N. The management of chronic heart failure. N. Engl. J. Med. 1996, 335, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.; Batin, P.D.; Andrews, R.; Lindsay, S.J.; Brooksby, P.; Mullen, M.; Baig, W.; Flapan, A.D.; Cowley, A.; Prescott, R.J. Prospective study of heart rate variability and mortality in chronic heart. Circulation 1998, 98, 1510–1516. [Google Scholar] [CrossRef] [PubMed]
- Rector, T.S.; Cohn, J.N. Prognosis in congestive heart failure. Annu. Rev. Med. 1994, 45, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Arbolishvili, G.N.; Mareev, V.I.; Orlova, I.A.; Belenkov, I.N. Heart rate variability in chronic heart failure and its role in prognosis of the disease. Kardiologiia 2005, 46, 4–11. [Google Scholar]
- Smilde, T.D.J.; van Veldhuisen, D.J.; van den Berg, M.P. Prognostic value of heart rate variability and ventricular arrhythmias during 13-year follow-up in patients with mild to moderate heart failure. Clin. Res. Cardiol. 2009, 98, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Acharya, U.R.; Fujita, H.; Sudarshan, V.K.; Oh, S.L.; Muhammad, A.; Koh, J.E.W.; Tan, J.H.; Chua, C.K.; Chua, K.P.; Tan, R.S. Application of empirical mode decomposition (EMD) for automated identification of congestive heart failure using heart rate signals. Neural Comput. Appl. 2016, 1–22. [Google Scholar] [CrossRef]
- Yu, S.N.; Lee, M.Y. Bispectral analysis and genetic algorithm for congestive heart failure recognition based on heart rate variability. Comput. Biol. Med. 2012, 42, 816–825. [Google Scholar] [CrossRef] [PubMed]
- Narin, A.; Isler, Y.; Ozer, M. Investigating the performance improvement of hrv indices in chf using feature selection methods based on backward elimination and statistical significance. Comput. Biol. Med. 2013, 45, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Jong, T.L.; Chang, B.; Kuo, C.D. Optimal timing in screening patients with congestive heart failure and healthy subjects during circadian observation. Ann. Biomed. Eng. 2011, 39, 835–849. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Pachori, R.B.; Acharya, U.R. Use of accumulated entropies for automated detection of congestive heart failure in flexible analytic wavelet transform framework based on short-term hrv signals. Entropy 2017, 19, 92. [Google Scholar] [CrossRef]
- Poon, C.S.; Merrill, C.K. Decrease of cardiac chaos in congestive heart failure. Nature 1997, 389, 492–495. [Google Scholar] [CrossRef] [PubMed]
- Woo, M.A.; Stevenson, W.G.; Moser, D.K.; Middlekauff, H.R. Complex heart rate variability and serum norepinephrine levels in patients with advanced heart failure. J. Am. Coll. Cardiol. 1994, 23, 565–569. [Google Scholar] [CrossRef]
- Binkley, P.F.; Nunziata, E.; Haas, G.J.; Nelson, S.D.; Cody, R.J. Parasympathetic withdrawal is an integral component of autonomic imbalance in congestive heart failure: Demonstration in human subjects and verification in a paced canine model of ventricular failure. J. Am. Coll. Cardiol. 1991, 18, 464–472. [Google Scholar] [CrossRef]
- La Rovere, M.T.; Pinna, G.D.; Maestri, R.; Mortara, A.; Capomolla, S.; Febo, O.; Ferrari, R.; Franchini, M.; Gnemmi, M.; Opasich, C.; et al. Short-term heart rate variability strongly predicts sudden cardiac death in chronic heart failure patients. Circulation 2003, 107, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Hadase, M.; Azuma, A.; Zen, K.; Asada, S.; Kawasaki, T.; Kamitani, T.; Kawasaki, S.; Sugihara, H.; Matsubara, H. Very low frequency power of heart rate variability is a powerful predictor of clinical prognosis in patients with congestive heart failure. Circ. J. 2004, 68, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Maestri, R.; Pinna, G.D.; Accardo, A.; Allegrini, P.; Balocchi, R.; D’Addio, G.; Ferrario, M.; Menicucci, D.; Porta, A.; Sassi, R.; et al. Nonlinear indices of heart rate variability in chronic heart failure patients: Redundancy and comparative clinical value. J. Cardiovasc. Electrophysiol. 2000, 18, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Mäkikallio, T.H.; Huikuri, H.V.; Hintze, U.; Videbaek, J.; Mitrani, R.D.; Castellanos, A.; Myerburg, R.J.; Møller, M. DIAMOND Study Group. Fractal analysis and time- and frequency-domain measures of heart rate variability as predictors of mortality in patients with heart failure. Am. J. Cardiol. 2001, 87, 178–182. [Google Scholar] [CrossRef]
- Peng, C.K.; Havlin, S.; Stanley, H.E.; Goldberger, A.L. Quantification of scaling exponents and crossover phenomena in nonstationary heartbeat time series. Chaos 1995, 5, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Pincus, S.M. Approximate entropy as a measure of system complexity. Proc. Natl. Acad. Sci. USA 1991, 88, 2297–2301. [Google Scholar] [CrossRef] [PubMed]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [PubMed]
- Humeau-Heurtier, A. The multiscale entropy algorithm and its variants: A review. Entropy 2015, 17, 3110–3123. [Google Scholar] [CrossRef]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of biological signals. Phys. Rev. E 2005, 71, 021906. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of complex physiologic time series. Phys. Rev. Lett. 2002, 89, 068102. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.K.; Fang, P.C.; Ding, M.S.; Jin, N.D. Multivariate weighted complex network analysis for characterizing nonlinear dynamic behavior in two-phase flow. Exp. Therm. Fluid Sci. 2015, 60, 157–164. [Google Scholar] [CrossRef]
- Labate, D.; La Foresta, F.; Morabito, G.; Palamara, I.; Morabito, F.C. Entropic measures of eeg complexity in alzheimer’s disease through a multivariate multiscale approach. IEEE Sens. J. 2013, 13, 3284–3292. [Google Scholar] [CrossRef]
- Azami, H.; Escudero, J. Refined composite multivariate generalized multiscale fuzzy entropy: A tool for complexity analysis of multichannel signals. Physica A 2017, 465, 261–276. [Google Scholar] [CrossRef]
- Zhao, L.N.; Wei, S.S.; Tong, H.; Liu, C.Y. Multivariable fuzzy measure entropy analysis for heart rate variability and heart sound amplitude variability. Entropy 2016, 18, 430. [Google Scholar] [CrossRef]
- Li, P.; Liu, C.Y.; Li, L.P.; Ji, L.Z.; Yu, S.Y.; Liu, C.C. Multiscale multivariate fuzzy entropy analysis. Acta Phys. Sin. 2013, 62, 120512. [Google Scholar]
- Ahmed, M.U.; Mandic, D.P. Multivariate multiscale entropy analysis. IEEE Signal Proc. Lett. 2012, 19, 91–94. [Google Scholar] [CrossRef]
- Ahmed, M.U.; Mandic, D.P. Multivariate multiscale entropy: A tool for complexity analysis of multichannel data. Phys. Rev. E 2011, 84, 061918. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Y.; Liu, C.C.; Shao, P.; Li, L.P.; Sun, X.; Wang, X.P.; Liu, F. Comparison of different threshold values r for approximate entropy: Application to investigate the heart rate variability between heart failure and healthy control groups. Physiol. Meas. 2011, 32, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Y.; Li, K.; Zhao, L.N.; Liu, F.; Zheng, D.C.; Liu, C.C.; Liu, S.T. Analysis of heart rate variability using fuzzy measure entropy. Comput. Biol. Med. 2013, 43, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.N.; Wei, S.S.; Zhang, C.Q.; Zhang, Y.T.; Jiang, X.E.; Liu, F.; Liu, C.Y. Determination of sample entropy and fuzzy measure entropy parameters for distinguishing congestive heart failure from normal sinus rhythm subjects. Entropy 2015, 17, 6270–6288. [Google Scholar] [CrossRef]
- Costa, M.; Cygankiewicz, I.; Zareba, W.; Bayes de Luna, A.; Goldberger, A.L.; Lobodzinski, S. Multiscale Complexity Analysis of Heart Rate Dynamics in Heart Failure: Preliminary Findings from the Music Study. In Proceedings of the Computing in Cardiology, Valencia, Spain, 17–20 September 2006. [Google Scholar]
- Costa, M.; Healey, J.A. Multiscale entropy analysis of complex heart rate dynamics: Discrimination of age and heart failure effects. In Proceedings of the Computing in Cardiology, Thessaloniki Chalkidiki, Greece, 21–24 September 2003. [Google Scholar]
- Von Tscharnerb, V.; Zandiyeh, P. Multi-scale transitions of fuzzy sample entropy of RR-intervals and their phase-randomized surrogates: A possibility to diagnose congestive heart failure. Biomed. Signal Process. Control 2017, 31, 350–356. [Google Scholar] [CrossRef]
- Valencia, J.F.; Porta, A.; Vallverdu, M.; Claria, F.; Baranowski, R.; Orlowska-Baranowska, E.; Caminal, P. Refined multiscale entropy: Application to 24-h holter recordings of heart period variability in healthy and aortic stenosis subjects. IEEE Trans. Biomed. Eng. 2009, 56, 2202–2213. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.D.; Wu, C.W.; Lin, S.G.; Wang, C.C.; Lee, K.Y. Time series analysis using composite multiscale entropy. Entropy 2013, 15, 1069–1084. [Google Scholar] [CrossRef]
- Wu, S.D.; Wu, C.W.; Lin, S.G.; Lee, K.Y.; Peng, C.K. Analysis of complex time series using refined composite multiscale entropy. Phys. Lett. A 2014, 378, 1369–1374. [Google Scholar] [CrossRef]
- Costa, M.; Goldberger, A.L. Generalized multiscale entropy analysis: Application to quantifying the complex volatility of human heartbeat time series. Entropy 2015, 17, 1197–1203. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Extremera, M.; Carpena, P.; Ivanov, P.C.; Bernaola-Galván, P.A. Magnitude and sign of long-range correlated time series: Decomposition and surrogate signal generation. Phys. Rev. E 2016, 93, 042201. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, D.T.; Stein, P.K.; Ivanov, P.C. Stratification pattern of static and scale-invariant dynamic measures of heartbeat fluctuations across sleep stages in young and elderly. IEEE Trans. Biomed. Eng. 2009, 56, 1564–1573. [Google Scholar] [CrossRef] [PubMed]
- Ashkenazy, Y.; Havlin, S.; Ivanov, P.C.; Peng, C.K.; Schulte-Frohlinde, V.; Stanley, H.E. Magnitude and sign scaling in power-law correlated time series. Physica A 2003, 323, 19–41. [Google Scholar] [CrossRef]
- Ashkenazy, Y.; Ivanov, P.C.; Havlin, S.; Peng, C.K.; Goldberger, A.L.; Stanley, H.E. Magnitude and sign correlations in heartbeat fluctuations. Phys. Rev. Lett. 2001, 86, 1900–1903. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. Physiobank, physiotoolkit, and physionet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, 215–220. [Google Scholar] [CrossRef]
- Liu, C.Y.; Li, L.P.; Zhao, L.N.; Zheng, D.C.; Li, P.; Liu, C.C. A combination method of improved impulse rejection filter and template matching for identification of anomalous intervals in electrocardiographic RR sequences. J. Med. Biol. Eng. 2012, 32, 245–250. [Google Scholar] [CrossRef]
- Peltola, M.A. Role of editing of r-r intervals in the analysis of heart rate variability. Front. Physiol. 2012, 23, 148. [Google Scholar] [CrossRef] [PubMed]
- Salo, M.A.; Huikuri, H.V.; Seppänen, T. Ectopic beats in heart rate variability analysis: Effects of editing on time and frequency domain measures. Ann. Noninvasive Electrocardiol. 2001, 6, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Kamath, M.V.; Fallen, E.L. Correction of the Heart Rate Variability Signal for Ectopics and Missing Beats; Futura Publishing Company: Armonk, NY, USA, 1995; pp. 75–85. [Google Scholar]
- Chang, C.C.; Lin, C.J. Libsvm: A library for support vector machines. ACM Trans. Intell. Syst. Technol. 2011, 2, 1–27. [Google Scholar] [CrossRef]
- Liu, C.Y.; Zhao, L.N. Using fuzzy measure entropy to improve the stability of traditional entropy measures. In Proceedings of the Computing in Cardiology, Hangzhou, China, 18–21 September 2011. [Google Scholar]
- Chen, W.T.; Zhuang, J.; Yu, W.X.; Wang, Z.Z. Measuring complexity using FuzzyEn, ApEn, and SampEn. Med. Eng. Phys. 2009, 31, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Pincus, S.M. Assessing serial irregularity and its implications for health. Ann. N. Y. Acad. Sci. 2001, 954, 245–267. [Google Scholar] [CrossRef] [PubMed]
- Nikulin, V.V.; Brismar, T. Comment on “multiscale entropy analysis of complex physiologic time series”. Phys. Rev. Lett. 2004, 92, 089804. [Google Scholar] [CrossRef] [PubMed]
- Dao, Q.; Krishnaswamy, P.; Kazanegra, R.; Harrison, A.; Amirnovin, R.; Lenert, L.; Clopton, P.; Alberto, J.; Hlavin, P.; Maisel, A.S. Utility of b-type natriuretic peptide in the diagnosis of congestive heart failure in an urgent-care setting. J. Am. Coll. Cardiol. 2001, 37, 379–385. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | NSR Group | CHF Group |
|---|---|---|
| Name of RR interval recordings | nsr001–nsr054 | chf201–chf229 |
| No. of RR interval recordings | 54 | 29 |
| No. of RR intervals | 5,790,504 | 3,312,195 |
| No. of RR intervals after removing greater than 2 s | 5,780,148 | 3,306,394 |
| No. of RR intervals after removing abnormal heartbeats | 5,738,937 | 3,102,120 |
| No. of RR segments when setting N = 500 | 11,452 | 6192 |
| No. of RR segments when setting N = 1000 | 5711 | 3089 |
| No. of RR segments when setting N = 2000 | 2843 | 1540 |
| No. of RR segments when setting N = 5000 | 1123 | 607 |
| Length of RR Segment | Scale Factor | MSE_RR (Original RR Segment) | MSE_dRR (Difference Time Series) | ||||
|---|---|---|---|---|---|---|---|
| NSR | CHF | p-Value | NSR | CHF | p-Value | ||
| 500 | 1 | 1.84 ± 0.16 | 1.53 ± 0.30 | 4 × 10−8 | 2.00 ± 0.22 | 1.58 ± 0.35 | 1 × 10−9 |
| 2 | 1.99 ± 0.15 | 1.78 ± 0.27 | 2 × 10−5 | 2.22 ± 0.26 | 1.69 ± 0.40 | 2 × 10−10 | |
| 3 | 2.04 ± 0.15 | 1.90 ± 0.23 | 9 × 10−4 | 2.35 ± 0.21 | 1.81 ± 0.42 | 2 × 10−11 | |
| 4 | 2.09 ± 0.16 | 1.94 ± 0.22 | 8 × 10−4 | 2.33 ± 0.14 | 1.85 ± 0.41 | 1 × 10−11 | |
| 5 | 2.10 ± 0.13 | 1.97 ± 0.17 | 2 × 10−4 | 2.29 ± 0.08 | 1.89 ± 0.37 | 3 × 10−11 | |
| 6 | 2.03 ± 0.09 | 1.95 ± 0.13 | 9 × 10−4 | 2.20 ± 0.07 | 1.88 ± 0.33 | 2 × 10−8 | |
| 7 | 2.11 ± 0.09 | 1.85 ± 0.29 | 7 × 10−5 | ||||
| 8 | 2.04 ± 0.07 | 1.80 ± 0.26 | 0.003 | ||||
| 9 | 1.76 ± 0.05 | 1.68 ± 0.06 | 5 × 10−4 | ||||
| 10 | |||||||
| 1000 | 1 | 1.80 ± 0.15 | 1.53 ± 0.29 | 3 × 10−7 | 2.00 ± 0.22 | 1.58 ± 0.35 | 2 × 10−9 |
| 2 | 1.86 ± 0.16 | 1.72 ± 0.24 | 0.002 | 2.20 ± 0.25 | 1.68 ± 0.39 | 2 × 10−10 | |
| 3 | 2.34 ± 0.24 | 1.79 ± 0.42 | 9 × 10−11 | ||||
| 4 | 1.99 ± 0.18 | 1.85 ± 0.23 | 0.003 | 2.43 ± 0.24 | 1.85 ± 0.45 | 4 × 10−11 | |
| 5 | 2.09 ± 0.18 | 1.93 ± 0.23 | 8 × 10−4 | 2.49 ± 0.21 | 1.92 ± 0.45 | 2 × 10−11 | |
| 6 | 2.15 ± 0.17 | 1.97 ± 0.19 | 6 × 10−5 | 2.50 ± 0.16 | 1.98 ± 0.44 | 1 × 10−11 | |
| 7 | 2.18 ± 0.16 | 2.02 ± 0.20 | 1 × 10−4 | 2.48 ± 0.12 | 2.00 ± 0.43 | 4 × 10−11 | |
| 8 | 2.19 ± 0.14 | 2.05 ± 0.17 | 1 × 10−4 | 2.45 ± 0.09 | 2.03 ± 0.41 | 3 × 10−10 | |
| 9 | 2.17 ± 0.13 | 2.06 ± 0.18 | 0.002 | 2.40 ± 0.08 | 2.03 ± 0.38 | 9 × 10−10 | |
| 10 | 2.32 ± 0.08 | 2.02 ± 0.33 | 7 × 10−9 | ||||
| 2000 | 1 | 1.75 ± 0.15 | 1.52 ± 0.27 | 4 × 10−6 | 2.00 ± 0.22 | 1.58 ± 0.35 | 3 × 10−9 |
| 2 | 2.19 ± 0.25 | 1.68 ± 0.39 | 3 × 10−10 | ||||
| 3 | 2.32 ± 0.24 | 1.78 ± 0.41 | 6 × 10−11 | ||||
| 4 | 1.83 ± 0.20 | 1.68 ± 0.25 | 0.003 | 2.39 ± 0.23 | 1.84 ± 0.44 | 6 × 10−11 | |
| 5 | 1.92 ± 0.19 | 1.75 ± 0.24 | 8 × 10−4 | 2.47 ± 0.21 | 1.92 ± 0.47 | 2 × 10−10 | |
| 6 | 1.98 ± 0.19 | 1.79 ± 0.23 | 2 × 10−4 | 2.53 ± 0.20 | 1.98 ± 0.47 | 1 × 10−10 | |
| 7 | 2.02 ± 0.18 | 1.84 ± 0.23 | 2 × 10−4 | 2.56 ± 0.19 | 2.02 ± 0.47 | 8 × 10−11 | |
| 8 | 2.04 ± 0.18 | 1.88 ± 0.22 | 6 × 10−4 | 2.59 ± 0.19 | 2.05 ± 0.47 | 1 × 10−10 | |
| 9 | 2.06 ± 0.17 | 1.91 ± 0.22 | 8 × 10−4 | 2.60 ± 0.18 | 2.08 ± 0.45 | 5 × 10−11 | |
| 10 | 2.09 ± 0.17 | 1.94 ± 0.22 | 5 × 10−4 | 2.59 ± 0.15 | 2.09 ± 0.44 | 4 × 10−11 | |
| 5000 | 1 | 1.64 ± 0.19 | 1.50 ± 0.25 | 0.004 | 2.00 ± 0.22 | 1.58 ± 0.35 | 3 × 10−9 |
| 2 | 2.17 ± 0.25 | 1.68 ± 0.39 | 4 × 10−10 | ||||
| 3 | 2.30 ± 0.23 | 1.78 ± 0.41 | 9 × 10−11 | ||||
| 4 | 1.67 ± 0.22 | 1.50 ± 0.26 | 0.003 | 2.36 ± 0.23 | 1.82 ± 0.42 | 4 × 10−11 | |
| 5 | 1.74 ± 0.22 | 1.56 ± 0.24 | 0.001 | 2.43 ± 0.21 | 1.90 ± 0.45 | 2 × 10−10 | |
| 6 | 1.79 ± 0.21 | 1.59 ± 0.23 | 2 × 10−4 | 2.47 ± 0.19 | 1.96 ± 0.46 | 3 × 10−10 | |
| 7 | 1.82 ± 0.20 | 1.62 ± 0.24 | 9 × 10−5 | 2.50 ± 0.18 | 2.00 ± 0.45 | 3 × 10−10 | |
| 8 | 1.83 ± 0.19 | 1.65 ± 0.24 | 3 × 10−4 | 2.53 ± 0.18 | 2.03 ± 0.45 | 2 × 10−10 | |
| 9 | 1.84 ± 0.19 | 1.68 ± 0.24 | 0.001 | 2.56 ± 0.18 | 2.05 ± 0.44 | 1 × 10−10 | |
| 10 | 1.86 ± 0.18 | 1.71 ± 0.25 | 0.002 | 2.57 ± 0.17 | 2.07 ± 0.44 | 2 × 10−10 | |
| Scale Factor | ||||||||
|---|---|---|---|---|---|---|---|---|
| MSE_RR | MSE_dRR | MSE_RR | MSE_dRR | MSE_RR | MSE_dRR | MSE_RR | MSE_dRR | |
| 1 | 79.7 | 82.8 | 78.9 | 82.4 | 77.4 | 82.5 | 69.1 | 82.5 |
| 2 | 75.2 | 84.4 | 67.3 | 84.4 | 61.0 | 83.9 | 52.7 | 83.6 |
| 3 | 69.0 | 84.9 | 64.3 | 84.6 | 62.5 | 84.9 | 64.4 | 84.9 |
| 4 | 70.3 | 82.7 | 68.6 | 84.7 | 68.9 | 84.3 | 68.3 | 85.0 |
| 5 | 71.4 | 84.1 | 71.9 | 85.9 | 71.5 | 83.5 | 69.8 | 83.5 |
| 6 | 70.0 | 80.0 | 74.5 | 83.7 | 73.1 | 82.8 | 71.1 | 82.1 |
| 7 | 63.9 | 80.5 | 71.9 | 83.8 | 72.2 | 83.7 | 72.1 | 81.9 |
| 8 | 55.7 | 80.4 | 71.7 | 81.0 | 69.5 | 83.2 | 69.8 | 82.7 |
| 9 | 84.0 | 73.7 | 66.9 | 79.1 | 69.1 | 83.1 | 66.8 | 83.4 |
| 10 | 46.7 | 61.5 | 61.6 | 81.1 | 70.6 | 83.0 | 66.8 | 81.7 |
| Mean | 68.6 | 79.5 | 69.8 | 83.1 | 69.6 | 83.5 | 67.1 | 83.1 |
| SD | 11.0 | 7.1 | 5.1 | 2.1 | 4.8 | 0.7 | 5.5 | 1.2 |
| Length of RR Segment | Fold | MSE_RR (Original RR Segment) | MSE_dRR (Difference Signal) | ||||
|---|---|---|---|---|---|---|---|
| (%) | (%) | (%) | (%) | (%) | (%) | ||
| 1000 | 1 | 71.4 | 66.7 | 68.8 | 80.0 | 90.9 | 87.5 |
| 2 | 80.0 | 75.0 | 76.5 | 100 | 76.9 | 81.3 | |
| 3 | 57.1 | 80.0 | 70.6 | 80.0 | 83.3 | 82.4 | |
| 4 | 66.7 | 81.8 | 76.5 | 80.0 | 91.7 | 88.2 | |
| 5 | 75.0 | 75.0 | 75.0 | 90.9 | 83.3 | 88.2 | |
| Mean | 70.1 | 75.7 | 73.5 | 86.2 | 85.2 | 85.5 | |
| SD | 8.7 | 5.9 | 3.6 | 9.1 | 6.1 | 3.4 | |
| 2000 | 1 | 71.4 | 66.7 | 68.8 | 80.0 | 90.9 | 87.5 |
| 2 | 80.0 | 83.3 | 82.4 | 100 | 84.6 | 87.5 | |
| 3 | 71.4 | 80.0 | 76.5 | 80.0 | 83.3 | 82.4 | |
| 4 | 66.7 | 72.7 | 70.6 | 80.0 | 91.7 | 88.2 | |
| 5 | 75.0 | 83.3 | 81.3 | 81.8 | 83.3 | 82.4 | |
| Mean | 72.9 | 77.2 | 75.9 | 84.4 | 86.8 | 85.6 | |
| SD | 5.0 | 7.3 | 6.1 | 8.8 | 4.2 | 3.0 | |
| 5000 | 1 | 71.4 | 55.6 | 62.5 | 80.0 | 90.9 | 87.5 |
| 2 | 80.0 | 83.3 | 82.4 | 100 | 84.6 | 87.5 | |
| 3 | 71.4 | 80.0 | 76.5 | 80.0 | 83.3 | 82.4 | |
| 4 | 66.7 | 72.7 | 70.6 | 80.0 | 91.7 | 88.2 | |
| 5 | 75.0 | 83.3 | 81.3 | 81.8 | 83.3 | 82.4 | |
| Mean | 72.9 | 75.0 | 74.6 | 84.4 | 86.8 | 85.6 | |
| SD | 5.0 | 11.7 | 8.2 | 8.8 | 4.2 | 3.0 | |
| Length of RR Segment | Scale Factor | MSE_RR (Original RR Segment) | MSE_dRR (Difference Time Series) | ||||
|---|---|---|---|---|---|---|---|
| NSR | CHF | p-Value | NSR | CHF | p-Value | ||
| 1000 | 1 | 1.79 ± 0.15 | 1.51 ± 0.28 | 4 × 10−8 | 1.99 ± 0.22 | 1.57 ± 0.34 | 8 × 10−10 |
| 2 | 1.85 ± 0.17 | 1.72 ± 0.24 | 0.005 | 2.19 ± 0.25 | 1.71 ± 0.38 | 9 × 10−10 | |
| 3 | 2.34 ± 0.24 | 1.83 ± 0.42 | 4 × 10−10 | ||||
| 4 | 1.98 ± 0.18 | 1.84 ± 0.23 | 0.003 | 2.42 ± 0.23 | 1.89 ± 0.43 | 1 × 10−10 | |
| 5 | 2.08 ± 0.18 | 1.92 ± 0.24 | 0.001 | 2.48 ± 0.20 | 1.96 ± 0.44 | 2 × 10−10 | |
| 6 | 2.15 ± 0.18 | 1.99 ± 0.22 | 4 × 10−4 | 2.49 ± 0.15 | 2.01 ± 0.44 | 2 × 10−10 | |
| 7 | 2.18 ± 0.16 | 2.03 ± 0.19 | 4 × 10−4 | 2.48 ± 0.12 | 2.05 ± 0.41 | 2 × 10−10 | |
| 8 | 2.18 ± 0.14 | 2.06 ± 0.19 | 0.002 | 2.44 ± 0.08 | 2.06 ± 0.38 | 4 × 10−10 | |
| 2.40 ± 0.08 | 2.08 ± 0.36 | 9 × 10−9 | |||||
| 2.32 ± 0.07 | 2.05 ± 0.33 | 2 × 10−7 | |||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, C.; Gao, R. Multiscale Entropy Analysis of the Differential RR Interval Time Series Signal and Its Application in Detecting Congestive Heart Failure. Entropy 2017, 19, 251. https://doi.org/10.3390/e19060251
Liu C, Gao R. Multiscale Entropy Analysis of the Differential RR Interval Time Series Signal and Its Application in Detecting Congestive Heart Failure. Entropy. 2017; 19(6):251. https://doi.org/10.3390/e19060251
Chicago/Turabian StyleLiu, Chengyu, and Rui Gao. 2017. "Multiscale Entropy Analysis of the Differential RR Interval Time Series Signal and Its Application in Detecting Congestive Heart Failure" Entropy 19, no. 6: 251. https://doi.org/10.3390/e19060251
APA StyleLiu, C., & Gao, R. (2017). Multiscale Entropy Analysis of the Differential RR Interval Time Series Signal and Its Application in Detecting Congestive Heart Failure. Entropy, 19(6), 251. https://doi.org/10.3390/e19060251