Refined Multiscale Fuzzy Entropy to Analyse Post-Exercise Cardiovascular Response in Older Adults With Orthostatic Intolerance



Abstract
:1. Introduction
2. Materials
3. Methods
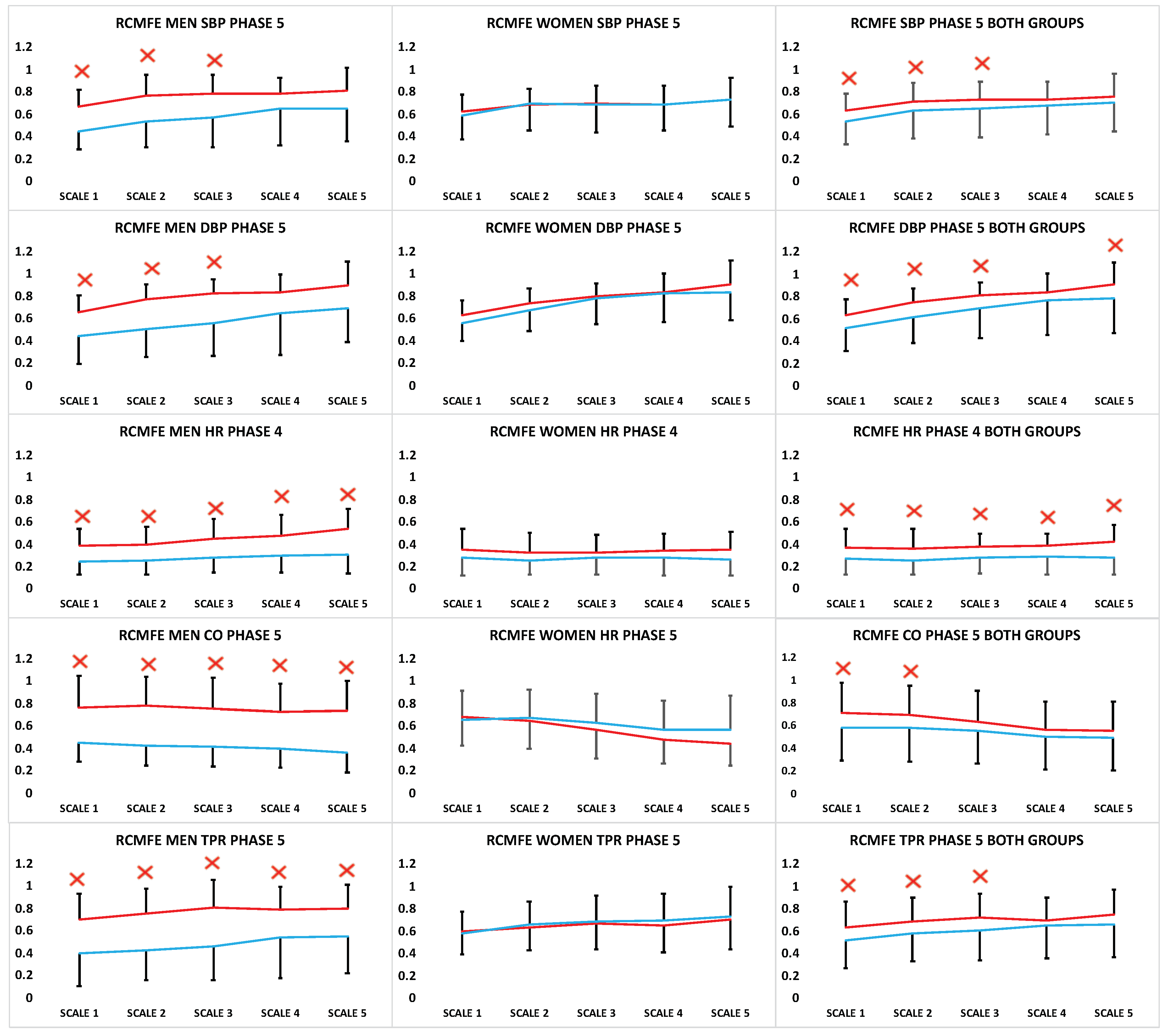
- SBP (mmHg): the maximum blood pressure (systole).
- DBP (mmHg): as the minimum value of pressure (diastole).
- MBP (mmHg): the mean arterial blood pressure during the cardiac cycle.
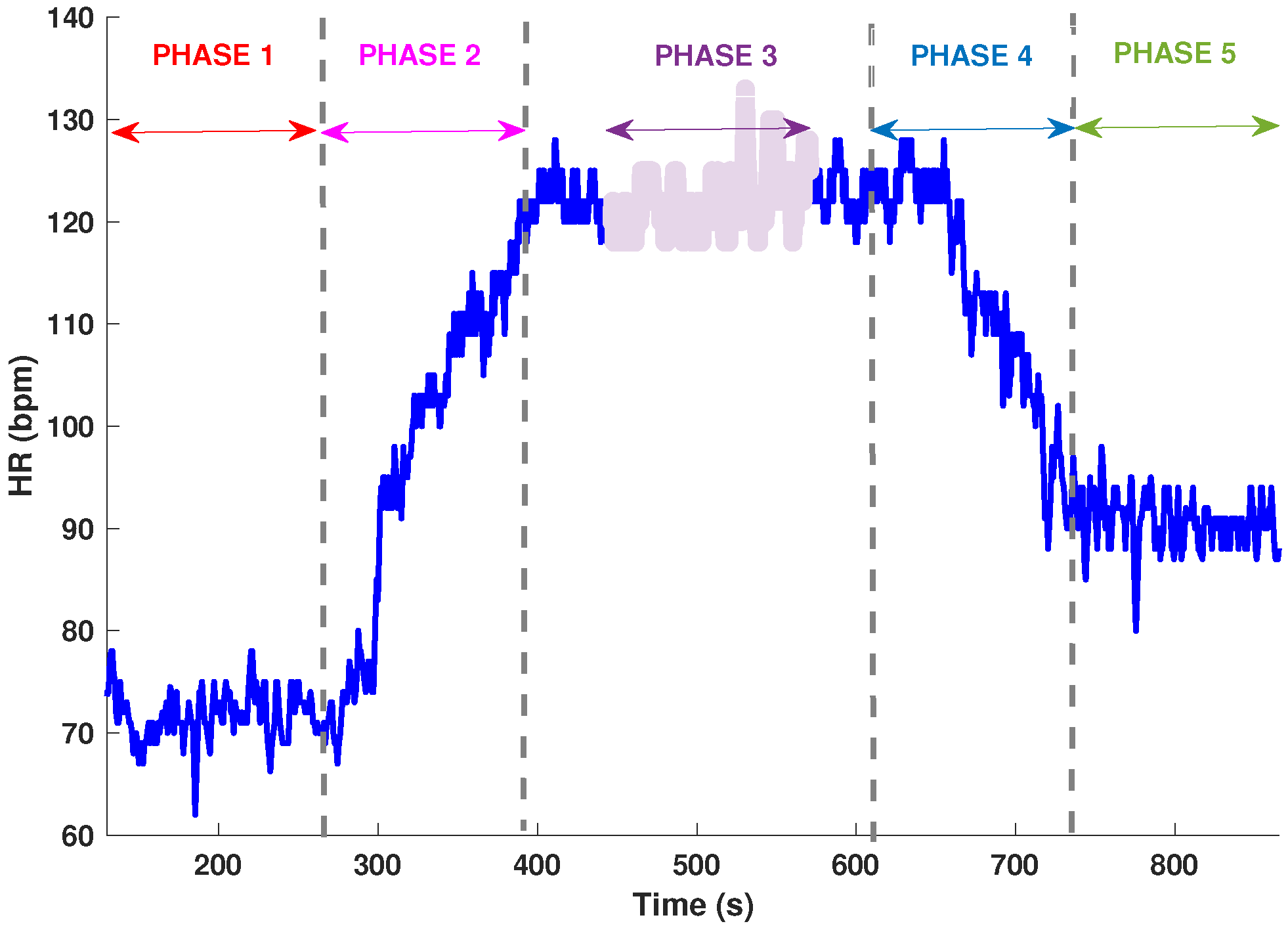
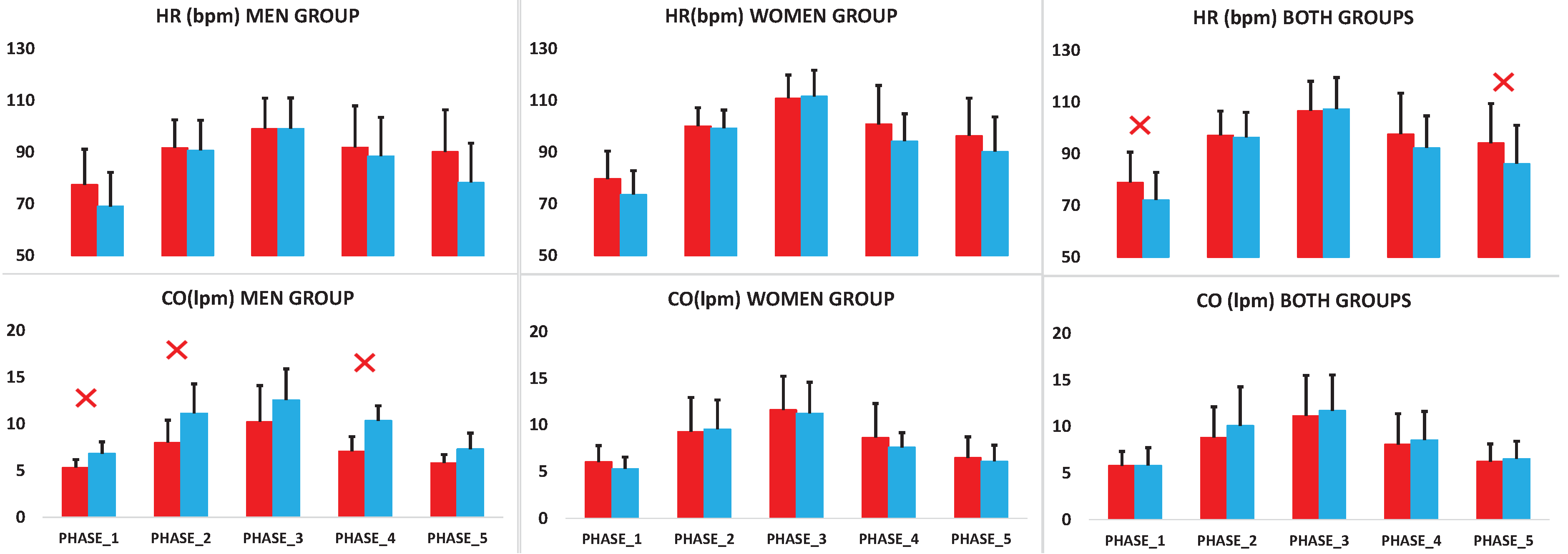
- HR (bpm): heart rate or cardiac frequency, derived from the pulse interval.
- CO (lpm): blood volume expelled by each ventricle per minute.
- TPR (mmHg/lpm): Total peripheral resistance, the overall resistance to blood flow through the systemic blood vessels.
3.1. Fuzzy Entropy Method
3.2. Coarse-Graining Process for a Multiscale Approach
3.3. Refined Composite Multiscale Fuzzy Entropy Method
3.4. Statistical Analysis
4. Results
4.1. Parameters Analysis
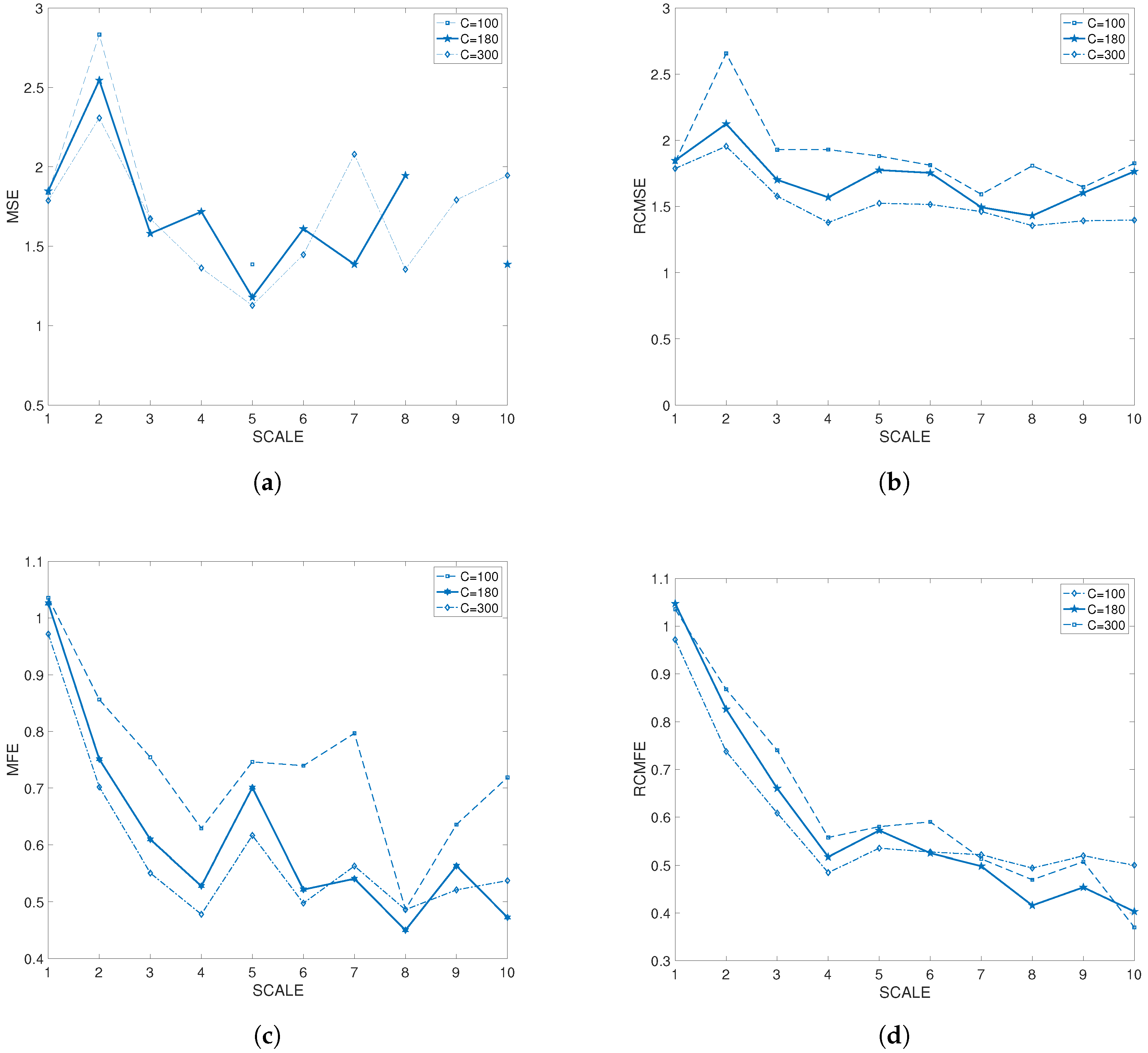
4.2. Refined Composite Multiscale Fuzzy Entropy Results
5. Discussion
Supplementary Materials
Supplementary File 1Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BP | Blood Pressure |
| DBP | Dyastolic Blood Pressure |
| CO | Cardiac Output |
| FE | Fuzzy Entropy |
| HR | Heart Rate |
| MBP | Mean Arterial Blood Pressure |
| MFE | Multiscale Fuzzy Entropy |
| MSE | Multiscale entropy |
| OI | Orthostatic Intolerance |
| OH | Orthostatic Hypotension |
| RCMSE | Refined composite multiscale entropy |
| RCMFE | Refined composite multiscale fuzzy entropy |
| SBP | Systolic Blood Pressure |
| SE | Sample Entropy |
| TPR | Total Peripheral Resistance |
References
- Gangavati, A.; Hajjar, I.; Quach, L.; Jones, R.N.; Kiely, D.K.; Gagnon, P.; Lipsitz, L.A. Hypertension, Orthostatic Hypotension, and the Risk of Falls in a Community-Dwelling Elderly Population: The Maintenance of Balance, Independent Living, Intellect, and Zest in the Elderly of Boston Study. J. Am. Geriatr. Soc. 2011, 59, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Heitterachi, E.; Lord, S.R.; Meyerkort, P.; McCloskey, I.; Fitzpatrick, R. Blood pressure changes on upright tilting predict falls in older people. Age Ageing 2002, 31, 181–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goswami, N.; Blaber, A.P.; Hinghofer-Szalkay, H.; Montani, J.P. Orthostatic Intolerance in Older Persons: Etiology and Countermeasures. Front. Physiol. 2017, 8, 803. [Google Scholar] [CrossRef] [PubMed]
- Blaber, A.P.; Goswami, N.; Bondar, R.L.; Kassam, M.S. Impairment of cerebral blood flow regulation in astronauts with orthostatic intolerance after flight. Stroke 2011, 42, 1844–1850. [Google Scholar] [CrossRef] [PubMed]
- Gharib, C.; Custaud, M.A. Orthostatic tolerance after spaceflight or simulated weightlessness by head-down bed-rest. Bull. Acad. Natl. Med. 2002, 186, 733–746, discussion 747–749. [Google Scholar] [PubMed]
- Weimer, L.H.; Williams, O. Syncope and orthostatic intolerance. Med. Clin. N. Am. 2003, 87, 835–865. [Google Scholar] [CrossRef]
- Lee, H.; Kim, H.A. Orthostatic hypertension: An underestimated cause of orthostatic intolerance. Clin. Neurophysiol. 2016, 127, 2102–2107. [Google Scholar] [CrossRef] [PubMed]
- Hachiya, T.; Hashimoto, I.; Saito, M.; Blaber, A.P. Peripheral vascular responses of men and women to LBNP. Aviat. Space Environ. Med. 2012, 83, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Fu, Q.; Arbab-Zadeh, A.; Perhonen, M.A.; Zhang, R.; Zuckerman, J.H.; Levine, B.D. Hemodynamics of orthostatic intolerance: Implications for gender differences. Am. J. Physiol. Heart Circ. Physiol. 2004, 55, H449–H457. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.E.; Hudson, D.L.; Deedwania, P.C. Applying continuous chaotic modeling to cardiac signal analysis. IEEE Eng. Med. Biol. Mag. 1996, 15, 97–102. [Google Scholar] [CrossRef]
- Costa, M.; Healey, J. Multiscale entropy analysis of complex heart rate dynamics: Discrimination of age and heart failure effects. In Proceedings of the Computers in Cardiology, Thessaloniki Chalkidiki, Greece, 21–24 September 2003; pp. 705–708. [Google Scholar]
- Makowiec, D.; Wejer, D.; Graff, B.; Struzik, Z.R. Dynamical Pattern Representation of Cardiovascular Couplings Evoked by Head-up Tilt Test. Entropy 2018, 20, 235. [Google Scholar] [CrossRef]
- Grassberger, P. Information and complexity measures in dynamical systems. In Information Dynamics; Springer: New York, NY, USA, 1991; pp. 15–33. [Google Scholar]
- Bar-Yam, Y. Dynamics of Complex Systems; Addison-Wesley: Reading, MA, USA, 1997; Volume 213. [Google Scholar]
- Humeau-Heurtier, A. The multiscale entropy algorithm and its variants: A review. Entropy 2015, 17, 3110–3123. [Google Scholar] [CrossRef] [Green Version]
- Busa, M.A.; van Emmerik, R.E. Multiscale entropy: A tool for understanding the complexity of postural control. J. Sport Health Sci. 2016, 5, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Azami, H.; Fernández, A.; Escudero, J. Refined multiscale fuzzy entropy based on standard deviation for biomedical signal analysis. Med. Biol. Eng. Comput. 2017, 55, 2037–2052. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.D.; Wu, C.W.; Lin, S.G.; Lee, K.Y.; Peng, C.K. Analysis of complex time series using refined composite multiscale entropy. Phys. Lett. A 2014, 378, 1369–1374. [Google Scholar] [CrossRef]
- Kenny, R.A.; Dishongh, T.; Newell, F.; Scanail, C.N. Osteoporosis special article-Insight-Research to reduce falls in older people: The TRIL centre. Geriatr. Med. 2009, 39, 326–327. [Google Scholar]
- Cullen, B.; Fahy, S.; Cunningham, C.J.; Coen, R.F.; Bruce, I.; Greene, E.; Coakley, D.; Walsh, J.B.; Lawlor, B.A. Screening for dementia in an Irish community sample using MMSE: A comparison of norm-adjusted versus fixed cut-points. Int. J. Geriatr. Psychiatry 2005, 20, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Jansen, J.R.; Schreuder, J.J.; Mulier, J.P.; Smith, N.T.; Settels, J.J.; Wesseling, K.H. A comparison of cardiac output derived from the arterial pressure wave against thermodilution in cardiac surgery patients. Br. J. Anaesth. 2001, 87, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Iwama, A.M.; Andrade, G.N.D.; Shima, P.; Tanni, S.E.; Godoy, I.D.; Dourado, V.Z. The six-minute walk test and body weight-walk distance product in healthy Brazilian subjects. Braz. J. Med. Biol. Res. 2009, 42, 1080–1085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.; Wang, Z.; Xie, H.; Yu, W. Characterization of surface EMG signal based on fuzzy entropy. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zhuang, J.; Yu, W.; Wang, Z. Measuring complexity using fuzzyen, apen, and sampen. Med. Eng. Phys. 2009, 31, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Li, M.A.; Liu, H.N.; Zhu, W.; Yang, J.F. Applying Improved Multiscale Fuzzy Entropy for Feature Extraction of MI-EEG. Appl. Sci. 2017, 7, 92. [Google Scholar] [CrossRef]
- Xie, H.B.; He, W.X.; Liu, H. Measuring time series regularity using nonlinear similarity-based sample entropy. Phys. Lett. A 2008, 372, 7140–7146. [Google Scholar] [CrossRef]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of complex physiologic time series. Phys. Rev. Lett. 2002, 89, 068102. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of biological signals. Phys. Rev. E 2005, 71, 021906. [Google Scholar] [CrossRef] [PubMed]
- Angelini, L.; Maestri, R.; Marinazzo, D.; Nitti, L.; Pellicoro, M.; Pinna, G.D.; Stramaglia, S.; Tupputi, S.A. Multiscale analysis of short term heart beat interval, arterial blood pressure, and instantaneous lung volume time series. Artif. Intell. Med. 2007, 41, 237–250. [Google Scholar] [CrossRef] [PubMed]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol.-Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.U.; Mandic, D.P. Multivariate multiscale entropy: A tool for complexity analysis of multichannel data. Phys. Rev. E 2011, 84, 061918. [Google Scholar] [CrossRef] [PubMed]
- Carey, B.J.; Manktelow, B.N.; Panerai, R.B.; Potter, J.F. Cerebral autoregulatory responses to head-up tilt in normal subjects and patients with recurrent vasovagal syncope. Circulation 2001, 104, 898–902. [Google Scholar] [CrossRef] [PubMed]
- Porta, A.; Gnecchi-Ruscone, T.; Tobaldini, E.; Guzzetti, S.; Furlan, R.; Montano, N. Progressive decrease of heart period variability entropy-based complexity during graded head-up tilt. J. Appl. Physiol. 2007, 103, 1143–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turianikova, Z.; Javorka, K.; Baumert, M.; Calkovska, A.; Javorka, M. The effect of orthostatic stress on multiscale entropy of heart rate and blood pressure. Physiol. Meas. 2011, 32, 1425–1437. [Google Scholar] [CrossRef] [PubMed]
- Valente, M.; Javorka, M.; Porta, A.; Bari, V.; Krohova, J.; Czippelova, B.; Turianikova, Z.; Nollo, G.; Faes, L. Univariate and multivariate conditional entropy measures for the characterization of short-term cardiovascular complexity under physiological stress. Physiol. Meas. 2018, 39, 014002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hortelano, M.; Reilly, R.B.; Cervigon, R. Multiscale time irreversibility to predict orthostatic intolerance in older people. In Proceedings of the 2016 IEEE Statistical Signal Processing Workshop (SSP), Palma de Mallorca, Spain, 26–29 June 2016; pp. 1–5. [Google Scholar]
- Valencia, J.F.; Porta, A.; Vallverdú, M.; Clarià, F.; Baranowski, R.; Orłowska-Baranowska, E.; Caminal, P. Refined multiscale entropy: Application to 24-h Holter recordings of heart period variability in healthy and aortic stenosis subjects. IEEE Trans. Biomed. Eng. 2009, 56, 2202–2213. [Google Scholar] [CrossRef] [PubMed]
- Nikulin, V.V.; Brismar, T. Comment on “Multiscale Entropy Analysis of Complex Physiologic Time Series”. Phys. Rev. Lett. 2004, 92, 089803. [Google Scholar] [CrossRef] [PubMed]
- Faes, L.; Porta, A.; Javorka, M.; Nollo, G. Efficient Computation of Multiscale Entropy over Short Biomedical Time Series Based on Linear State-Space Models. Complexity 2017, 13. [Google Scholar] [CrossRef]
- Parvaneh, S.; Howe, C.L.; Toosizadeh, N.; Honarvar, B.; Slepian, M.J.; Fain, M.; Mohler, J.; Najafi, B. Regulation of cardiac autonomic nervous system control across frailty statuses: A systematic review. Gerontology 2015, 62, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Baumert, M.; Czippelova, B.; Ganesan, A.; Schmidt, M.; Zaunseder, S.; Javorka, M. Entropy analysis of RR and QT interval variability during orthostatic and mental stress in healthy subjects. Entropy 2014, 16, 6384–6393. [Google Scholar] [CrossRef]
- Streeten, D. Pathogenesis of hyperadrenergic orthostatic hypotension. Evidence of disordered venous innervation exclusively in the lower limbs. J. Clin. Investig. 1990, 86, 1582. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.C.; Vyas, A.; Hymen, E.; Perlmuter, L.C. Gender differences in orthostatic hypotension. Am. J. Med. Sci. 2011, 342, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Convertino, V.A. Gender differences in autonomic functions associated with blood pressure regulation. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 1998, 275, R1909–R1920. [Google Scholar] [CrossRef]
- Joyner, M.J.; Wallin, B.G.; Charkoudian, N. Sex differences and blood pressure regulation in humans. Exp. Physiol. 2016, 101, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Shoemaker, J.K.; Hogeman, C.S.; Khan, M.; Kimmerly, D.S.; Sinoway, L.I. Gender affects sympathetic and hemodynamic response to postural stress. Am. J. Physiol. Heart Circ. Physiol. 2001, 281, H2028–H2035. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Women | Men | Total | ||
|---|---|---|---|---|
| Symptomatic | Participants | 23 | 13 | 36 |
| Age | 69.65 ± 5.29 | 71.77 ± 6.47 | 70.42 ± 5.74 | |
| Weight | 72.39 ± 14.32 | 84.23 ± 12.81 | 76.67 ± 14.78 | |
| Height | 163.96 ± 7.57 | 173.85 ± 5.88 | 167.53 ± 8.43 | |
| Body mass index | 26.77 ± 5.36 | 26.09 ± 4.01 | 26.86 ± 5.44 | |
| Asymptomatic | Participants | 19 | 10 | 29 |
| Age | 70.63 ± 5.34 | 68.00 ± 7.21 | 69.72 ± 6.05 | |
| Weight | 70.89 ± 10.57 | 81.60 ± 10.78 | 74.59 ± 11.66 | |
| Height | 163.84 ± 7.42 | 176.00 ± 2.94 | 168.03 ± 8.53 | |
| Body mass index | 26.09 ± 4.01 | 25.72 ± 3.97 | 25.96 ± 3.93 | |
| Phase 5 | Men | Women | Both Gender | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Symptomatic OI | Asymptomatic OI | p | Symptomatic OI | Asymptomatic OI | p | Symptomatic OI | Asymptomatic OI | p | |
| SBP (mmHg) | 134.97 ± 21.80 | 140.47 ± 20.43 | >0.05 | 127.37 ± 25.72 | 130.54 ± 18.67 | >0.05 | 130.11 ± 24.34 | 133.96 ± 19.53 | >0.05 |
| DBP (mmHg) | 70.18 ± 13.83 | 66.33 ± 11.37 | >0.05 | 62.78 ± 10.56 | 62.70 ± 8.41 | >0.05 | 65.45 ± 12.19 | 63.95 ± 9.50 | >0.05 |
| HR (bpm) | 90.17 ± 16.18 | 78.32 ± 15.19 | >0.05 | 96.34 ± 14.59 | 90.20 ± 13.40 | >0.05 | 94.11 ± 15.25 | 86.10 ± 14.92 | 0.022 |
| CO (lpm) | 5.80 ± 0.91 | 7.31 ± 2.03 | >0.05 | 6.47 ± 2.24 | 6.12 ± 1.71 | >0.05 | 6.23 ± 1.88 | 6.53 ± 1.88 | >0.05 |
| TPR (mmHg/lpm) | 17.67 ± 6.05 | 15.94 ± 5.71 | >0.05 | 16.35 ± 5.44 | 16.86 ± 3.86 | >0.05 | 16.22 ± 5.62 | 16.54 ± 4.50 | >0.05 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hortelano, M.; Reilly, R.B.; Castells, F.; Cervigón, R. Refined Multiscale Fuzzy Entropy to Analyse Post-Exercise Cardiovascular Response in Older Adults With Orthostatic Intolerance. Entropy 2018, 20, 860. https://doi.org/10.3390/e20110860
Hortelano M, Reilly RB, Castells F, Cervigón R. Refined Multiscale Fuzzy Entropy to Analyse Post-Exercise Cardiovascular Response in Older Adults With Orthostatic Intolerance. Entropy. 2018; 20(11):860. https://doi.org/10.3390/e20110860
Chicago/Turabian StyleHortelano, Marcos, Richard B. Reilly, Francisco Castells, and Raquel Cervigón. 2018. "Refined Multiscale Fuzzy Entropy to Analyse Post-Exercise Cardiovascular Response in Older Adults With Orthostatic Intolerance" Entropy 20, no. 11: 860. https://doi.org/10.3390/e20110860
APA StyleHortelano, M., Reilly, R. B., Castells, F., & Cervigón, R. (2018). Refined Multiscale Fuzzy Entropy to Analyse Post-Exercise Cardiovascular Response in Older Adults With Orthostatic Intolerance. Entropy, 20(11), 860. https://doi.org/10.3390/e20110860