Sample Entropy of sEMG Signals at Different Stages of Rectal Cancer Treatment



Abstract
:1. Introduction
2. Methods
2.1. Sample Entropy
2.2. Multiscale Entropy
3. Material
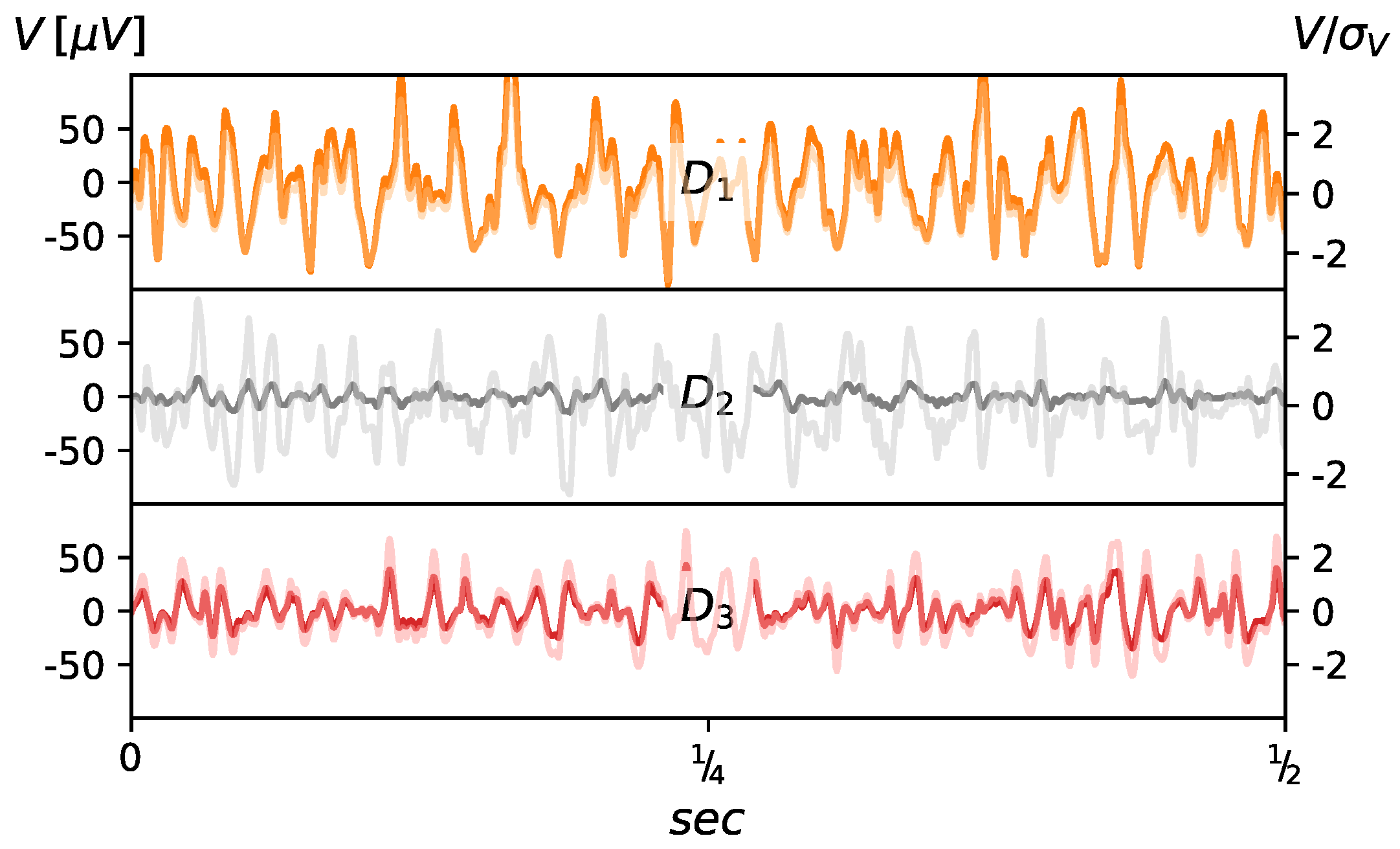
3.1. sEMG Signal Source
3.2. Patients
4. Results
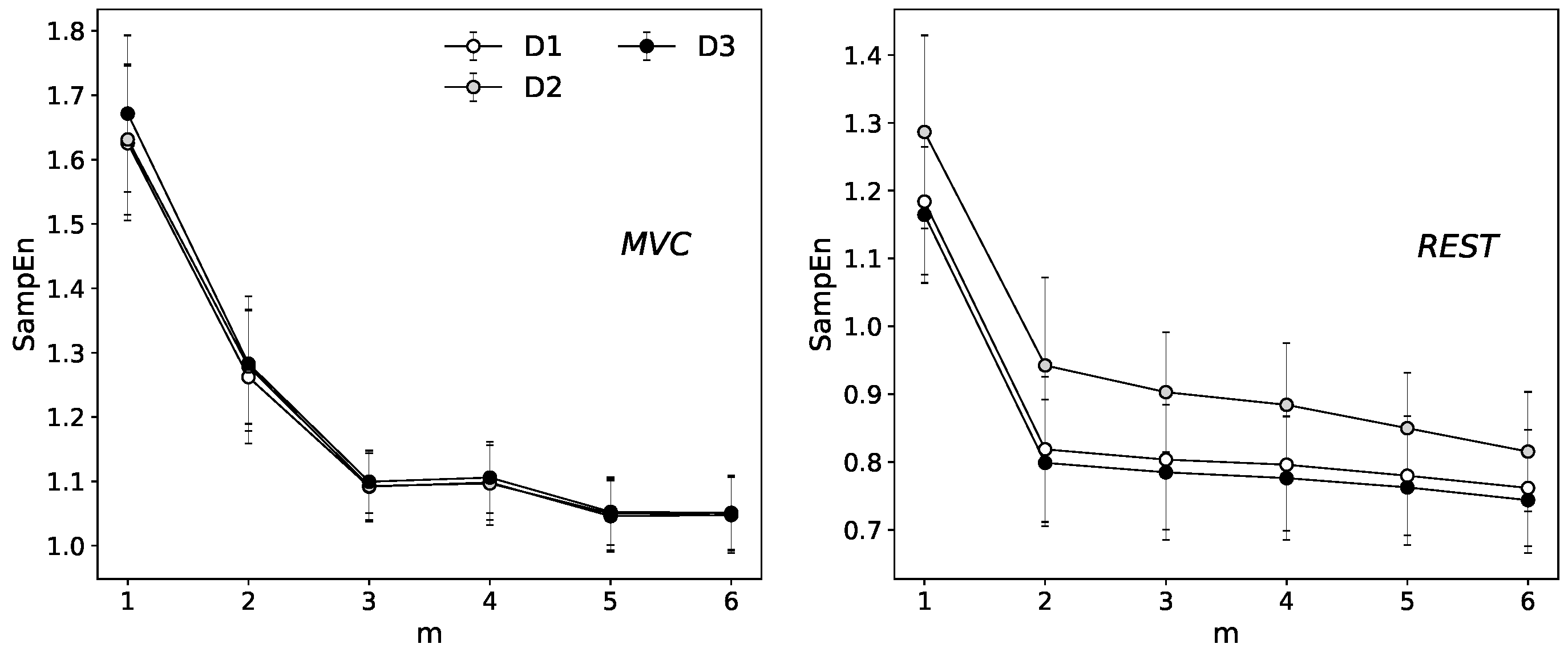
4.1. Choice of Embedding Dimension Parameter
4.2. Single Scale Entropy
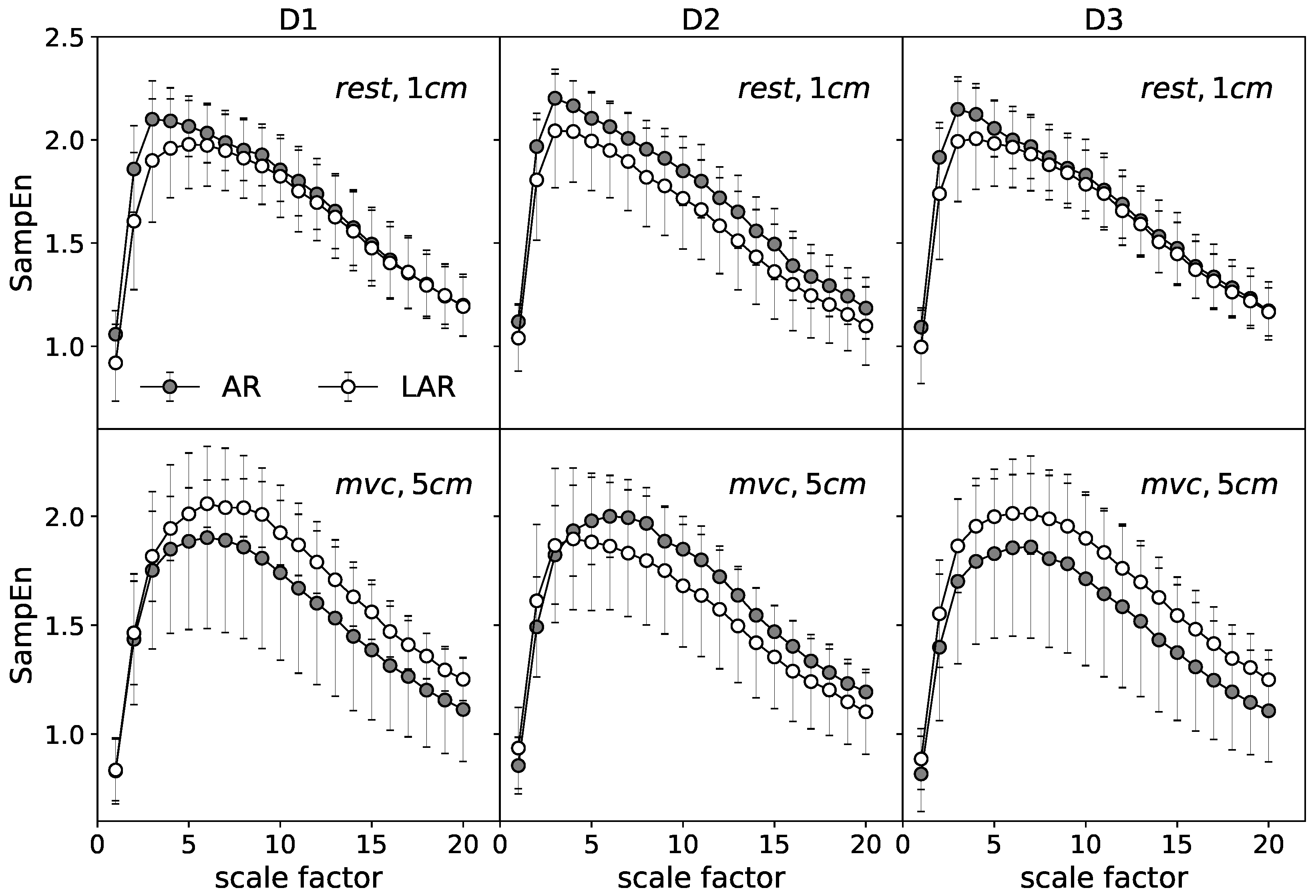
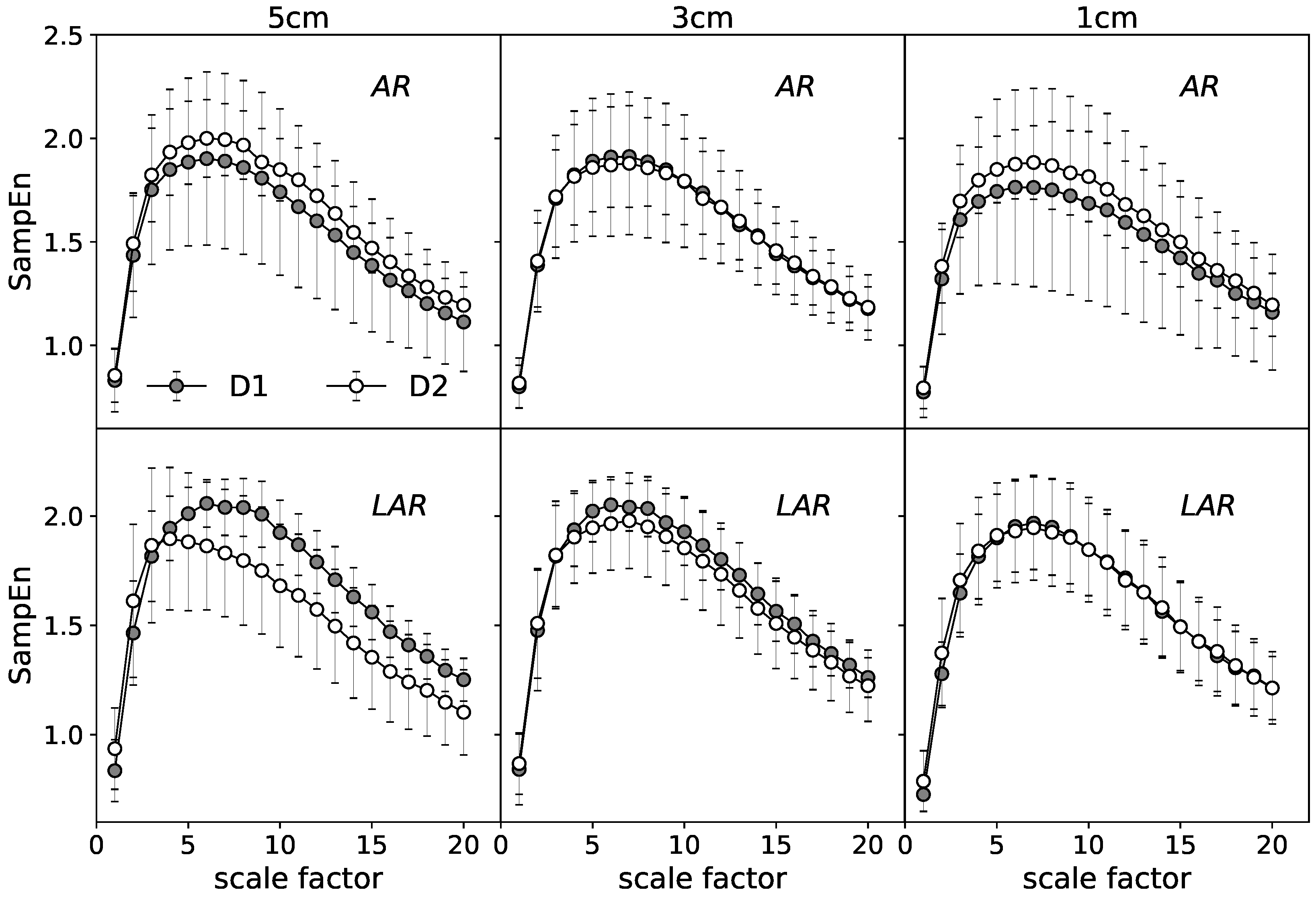
4.3. Multiscale Entropy (MSE)
5. Statistics
6. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| EAS | external anal sphincter |
| sEMG | surface electromyography |
| AR | anterior resection |
| LAR | lower anterior resection |
| MVC | maximum voluntary contraction |
References
- Bray, F.; Jemal, A.; Grey, N.; Ferlay, J.; Forman, D. Global cancer transitions according to the Human Development Index (2008–2030): A population-based study. Lancet Oncol. 2012, 13, 790–801. [Google Scholar] [CrossRef]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Chen, H.P.; Liu, K.W. Fecal incontinence and quality of life in adults with rectal cancer after lower anterior resection. J. Wound Ostomy Cont. Nurs. 2015, 42, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Bruheim, K.; Guren, M.G.; Skovlund, E.; Hjermstad, M.J.; Dahl, O.; Frykholm, G.; Carlsen, E.; Tveit, K.M. Late side effects and quality of life after radiotherapy for rectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 1005–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juul, T.; Ahlberg, M.; Biondo, S.; Espin, E.; Jimenez, L.M.; Matzel, K.E.; Palmer, G.J.; Sauermann, A.; Trenti, L.; Zhang, W.; et al. Low anterior resection syndrome and quality of life: An international multicenter study. Dis. Colon Rectum 2014, 57, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Ridolfi, T.J.; Berger, N.; Ludwig, K.A. Low Anterior Resection Syndrome: Current Management and Future Directions. Clin. Colon Rect. Surg. 2016, 29, 239–245. [Google Scholar] [Green Version]
- Rao, G.; Drew, P.; Lee, P.; Monson, J.; Duthie, G. Anterior resection syndrome is secondary to sympathetic denervation. Int. J. Colorectal Dis. 1996, 11, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Hinninghofen, H.; Wietek, B.; Enck, P. Asymmetry of anal sphincter innervation is related to gender, incontinence, and childbirth. Neurogastroenterol. Motil. 2003, 15, 90. [Google Scholar] [CrossRef]
- Enck, P.; Hinninghofen, H.; Wietek, B.; Becker, H.D. Functional asymmetry of pelvic floor innervation and its role in the pathogenesis of fecal incontinence. Digestion 2004, 69, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Podnar, S.; Rodi, Z.; Lukanovic, A.; Trsinar, B.; Vodusek, D. Standardization of anal sphincter EMG: Technique of needle examination. Muscle Nerve 1999, 22, 400–403. [Google Scholar] [CrossRef]
- Enck, P.; Hinninghofen, H.; Merletti, R.; Azpiroz, F. The external anal sphincter and the role of surface electromyography. Neurogastroenterol. Motil. 2005, 17, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Mesin, L.; Gazzoni, M.; Merletti, R. Automatic localisation of innervation zones: A simulation study of the external anal sphincter. J. Electromyogr. Kinesiol. 2009, 19, e413–e421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cescon, C.; Mesin, L.; Nowakowski, M.; Merletti, R. Geometry assessment of anal sphincter muscle based on monopolar multichannel surface EMG signals. J. Electromyogr. Kinesiol. 2011, 21, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Cescon, C.; Raimondi, E.E.; Začesta, V.; Drusany-Starič, K.; Martsidis, K.; Merletti, R. Characterization of the motor units of the external anal sphincter in pregnant women with multichannel surface EMG. Int. Urogynecol. J. 2014, 25, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Nowakowski, M.; Tomaszewski, K.A.; Machura, Ł.; Trybek, P.; Herman, R.M. Sensitivity and specificity of multichannel surface electromyography in diagnosing fecal incontinence. Folia Med. Cracov. 2017, 57, 29–38. [Google Scholar] [PubMed]
- Merletti, R.; Farina, D. Surface Electromyography: Physiology, Engineering and Applications; John Wiley Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Clancy, E.; Morin, E.L.; Merletti, R. Sampling, noise-reduction and amplitude estimation issues in surface electromyography. J. Electromyogr. Kinesiol. 2002, 12, 1–16. [Google Scholar] [CrossRef]
- Trybek, P.; Nowakowski, M.; Machura, L. Multifractal characteristics of external anal sphincter based on sEMG signals. Med. Eng. Phys. 2018, 55, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckers, F.; Ramaekers, D.; Aubert, A.E. Approximate entropy of heart rate variability: Validation of methods and application in heart failure. Cardiovasc. Eng. 2001, 1, 177–182. [Google Scholar] [CrossRef]
- Gao, J.; Hu, J.; Liu, F.; Cao, Y. Multiscale entropy analysis of biological signals: A fundamental bi-scaling law. Front. Comput. Neurosci. 2015, 9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Chen, X.; Barkhaus, P.E.; Zhou, P. Multiscale entropy analysis of different spontaneous motor unit discharge patterns. IEEE J. Biomed. Health Inf. 2013, 17, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Trybek, P.; Nowakowski, M.; Salowka, J.; Machura, L. The distribution of information for sEMG signals in the rectal cancer treatment process. arXiv, 2018; arXiv:1809.07147. [Google Scholar]
- Goldberger, A.L.; Peng, C.K.; Lipsitz, L.A. What is physiologic complexity and how does it change with aging and disease? Neurobiol. Aging 2002, 23, 23–26. [Google Scholar] [CrossRef]
- Shannon, C.E. A mathematical theory of communication. Bell Syst. Tech. J. 1948, 27, 379–423. [Google Scholar] [CrossRef]
- Chen, W.; Wang, Z.; Xie, H.; Yu, W. Characterization of surface EMG signal based on fuzzy entropy. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.; Goldberger, A.; Peng, C.K. Multiscale entropy to distinguish physiologic and synthetic RR time series. Comput. Cardiol. 2002. [Google Scholar] [CrossRef]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of complex physiologic time series. Phys. Rev. Lett. 2002, 89, 068102. [Google Scholar] [CrossRef] [PubMed]
- Kang, X.; Jia, X.; Geocadin, R.G.; Thakor, N.V.; Maybhate, A. Multiscale entropy analysis of EEG for assessment of post-cardiac arrest neurological recovery under hypothermia in rats. IEEE Trans. Biomed. Eng. 2009, 56, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Humeau-Heurtier, A. The multiscale entropy algorithm and its variants: A review. Entropy 2015, 17, 3110–3123. [Google Scholar] [CrossRef] [Green Version]
- Faes, L.; Porta, A.; Javorka, M.; Nollo, G. Efficient Computation of Multiscale Entropy over Short Biomedical Time Series Based on Linear State-Space Models. Complexity 2017, 2017. [Google Scholar] [CrossRef]
- Valencia, J.F.; Porta, A.; Vallverdu, M.; Claria, F.; Baranowski, R.; Orlowska-Baranowska, E.; Caminal, P. Refined multiscale entropy: Application to 24-h holter recordings of heart period variability in healthy and aortic stenosis subjects. IEEE Trans. Biomed. Eng. 2009, 56, 2202–2213. [Google Scholar] [CrossRef] [PubMed]
- Castiglioni, P.; Coruzzi, P.; Bini, M.; Parati, G.; Faini, A. Multiscale Sample Entropy of cardiovascular signals: Does the choice between fixed-or varying-tolerance among scales influence its evaluation and interpretation? Entropy 2017, 19, 590. [Google Scholar] [CrossRef]
- Wu, H.T.; Jiang, Y.H.; Liu, A.B.; Liu, C.W.; Ou, Y.N.; Kuo, H.C.; Sun, C.K. Multiscale Entropy Analysis of Surface Electromyographic Signals from the Urethral Sphincter as a Prognostic Indicator for Surgical Candidates with Primary Bladder Neck Obstruction. Entropy 2015, 17, 8089–8098. [Google Scholar] [CrossRef] [Green Version]
- Istenič, R.; Kaplanis, P.A.; Pattichis, C.S.; Zazula, D. Multiscale entropy-based approach to automated surface EMG classification of neuromuscular disorders. Med. Biol. Eng. Comput. 2010, 48, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Pincus, S.M. Approximate entropy as a measure of system complexity. Pro. Nat. Acad. Sci. USA 1991, 88, 2297–2301. [Google Scholar] [CrossRef]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of biological signals. Phys. Rev. E 2005, 71, 021906. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.; Peng, C.K.; Goldberger, A.L.; Hausdorff, J.M. Multiscale entropy analysis of human gait dynamics. Phys. A Stat. Mech. Appl. 2003, 330, 53–60. [Google Scholar] [CrossRef]
- Semmlow, J.L.; Griffel, B. Biosignal and Medical Image Processing; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]
- Kenig, J.; Richter, P. Definition of the rectum and level of the peritoneal reflection–still a matter of debate? Videosurg. Miniinvasive Tech. 2013, 8, 183. [Google Scholar] [CrossRef] [PubMed]
- Merletti, R.; Di Torino, P. Standards for reporting EMG data. J. Electromyogr. Kinesiol. 1999, 9, 3–4. [Google Scholar]
- Merletti, R.; Parker, P.A. Electromyography: Physiology, Engineering, and Non-Invasive Applications; John Wiley & Sons: Hoboken, NJ, USA, 2004; Volume 11, pp. 121–127. [Google Scholar]
- Wałęga, P.; Herman, R.; Popiela, T. Long term results of anorectal functioning in patients with anterior resection of the rectum. Pol. Prz. Chir. 2001, 73, 327–39. [Google Scholar]
- Herman, RM.; Walega, P.; Kenig, J.; Smeder, K.; Salowka, J.; Nowakowski, M.; Zelazny, D. A Hydraulic Sphincter Prosthesis (artificial Bowel Sphincter) For Faecal Incontinence Treatment. Colorectal Dis. 2006, 8, 39. [Google Scholar]
- Giandomenico, F.; Gavaruzzi, T.; Lotto, L.; Del Bianco, P.; Barina, A.; Perin, A.; Pucciarelli, S. Quality of life after surgery for rectal cancer: A systematic review of comparisons with the general population. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 1227–1242. [Google Scholar] [CrossRef] [PubMed]
- Couwenberg, A.M.; Burbach, J.P.; van Grevenstein, W.M.; Smits, A.B.; Consten, E.C.; Schiphorst, A.H.; Wijffels, N.A.; Heikens, J.T.; Intven, M.P.; Verkooijen, H.M. Effect of Neoadjuvant Therapy and Rectal Surgery on Health-related Quality of Life in Patients With Rectal Cancer During the First 2 Years After Diagnosis. Clin. Colorectal Cancer 2018, 17, e499–e512. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (All Scales) | ||||||
|---|---|---|---|---|---|---|
| rest | 5 | 3 | 1 | 5 | 3 | 1 |
| 0.050 | 0.001 | 0.000 | 0.027 | 0.579 | 0.000 | |
| 0.004 | 0.062 | 0.000 | 0.007 | 0.181 | 0.000 | |
| 0.000 | 0.001 | 0.000 | 0.901 | 0.245 | 0.000 | |
| MVC | 5 | 3 | 1 | 5 | 3 | 1 |
| 0.602 | 0.228 | 0.000 | 0.000 | 0.000 | 0.000 | |
| 0.000 | 0.004 | 0.464 | 0.000 | 0.000 | 0.000 | |
| 0.000 | 0.001 | 0.000 | 0.000 | 0.000 | 0.000 | |
| rest | 5 | 3 | 1 | 5 | 3 | 1 | |
| Anova | 57.07 | 106.64 | 86.14 | 413.45 | 384.08 | 43.51 | |
| Kendall coeff. | 0.009 | 0.017 | 0.014 | 0.065 | 0.060 | 0.007 | |
| p-value | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| MVC | 5 | 3 | 1 | 5 | 3 | 1 | |
| Anova | 110.17 | 55.77 | 261.24 | 517.23 | 302.40 | 55.61 | |
| Kendall coeff. | 0.017 | 0.009 | 0.408 | 0.081 | 0.047 | 0.009 | |
| p-value | 0.000 | 0.001 | 0.000 | 0.000 | 0.000 | 0.000 | |
| rest | ||||||
| Anova | 24.05 | 173.95 | 8.612 | 110.88 | 2.974 | 28.67 |
| Kendall coeff. | 0.004 | 0.027 | 0.001 | 0.017 | 0.46 × | 0.004 |
| p-value | 0.000 | 0.000 | 0.013 | 0.000 | 0.226 | 0.000 |
| MVC | 5 | 3 | 1 | 5 | 3 | 1 |
| Anova | 0.645 | 96.11 | 294.97 | 350.50 | 351.96 | 447.34 |
| Kendall coeff. | 0.1 × | 0.015 | 0.046 | 0.055 | 0.055 | 0.070 |
| p-value | 0.724 | 0.001 | 0.000 | 0.000 | 0.000 | 0.000 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trybek, P.; Nowakowski, M.; Salowka, J.; Spiechowicz, J.; Machura, L. Sample Entropy of sEMG Signals at Different Stages of Rectal Cancer Treatment. Entropy 2018, 20, 863. https://doi.org/10.3390/e20110863
Trybek P, Nowakowski M, Salowka J, Spiechowicz J, Machura L. Sample Entropy of sEMG Signals at Different Stages of Rectal Cancer Treatment. Entropy. 2018; 20(11):863. https://doi.org/10.3390/e20110863
Chicago/Turabian StyleTrybek, Paulina, Michal Nowakowski, Jerzy Salowka, Jakub Spiechowicz, and Lukasz Machura. 2018. "Sample Entropy of sEMG Signals at Different Stages of Rectal Cancer Treatment" Entropy 20, no. 11: 863. https://doi.org/10.3390/e20110863
APA StyleTrybek, P., Nowakowski, M., Salowka, J., Spiechowicz, J., & Machura, L. (2018). Sample Entropy of sEMG Signals at Different Stages of Rectal Cancer Treatment. Entropy, 20(11), 863. https://doi.org/10.3390/e20110863