Performance Evaluations on Using Entropy of Ultrasound Log-Compressed Envelope Images for Hepatic Steatosis Assessment: An In Vivo Animal Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Preparations
2.2. Ultrasound Data Acquisition
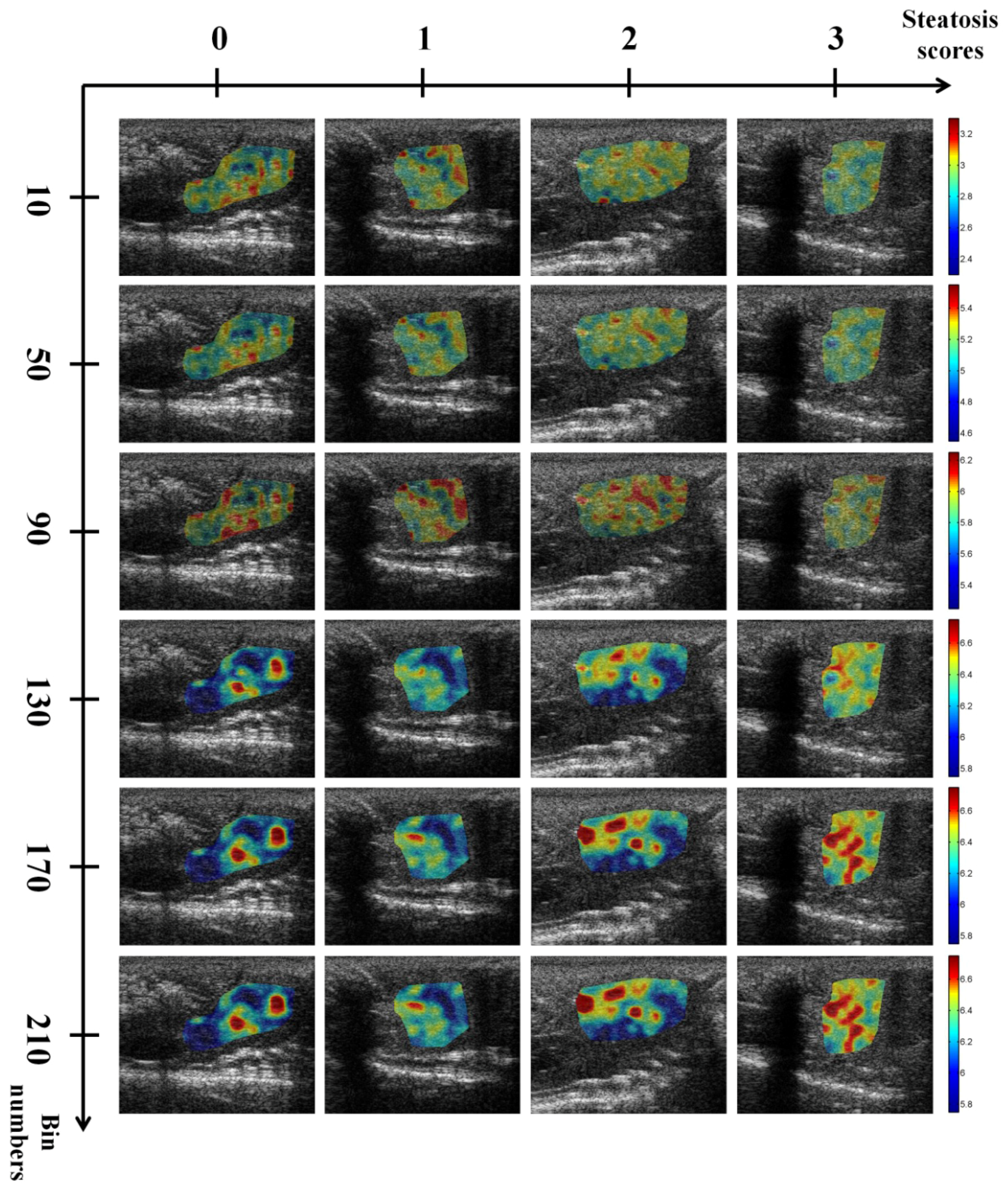
2.3. Ultrasound Entropy Imaging
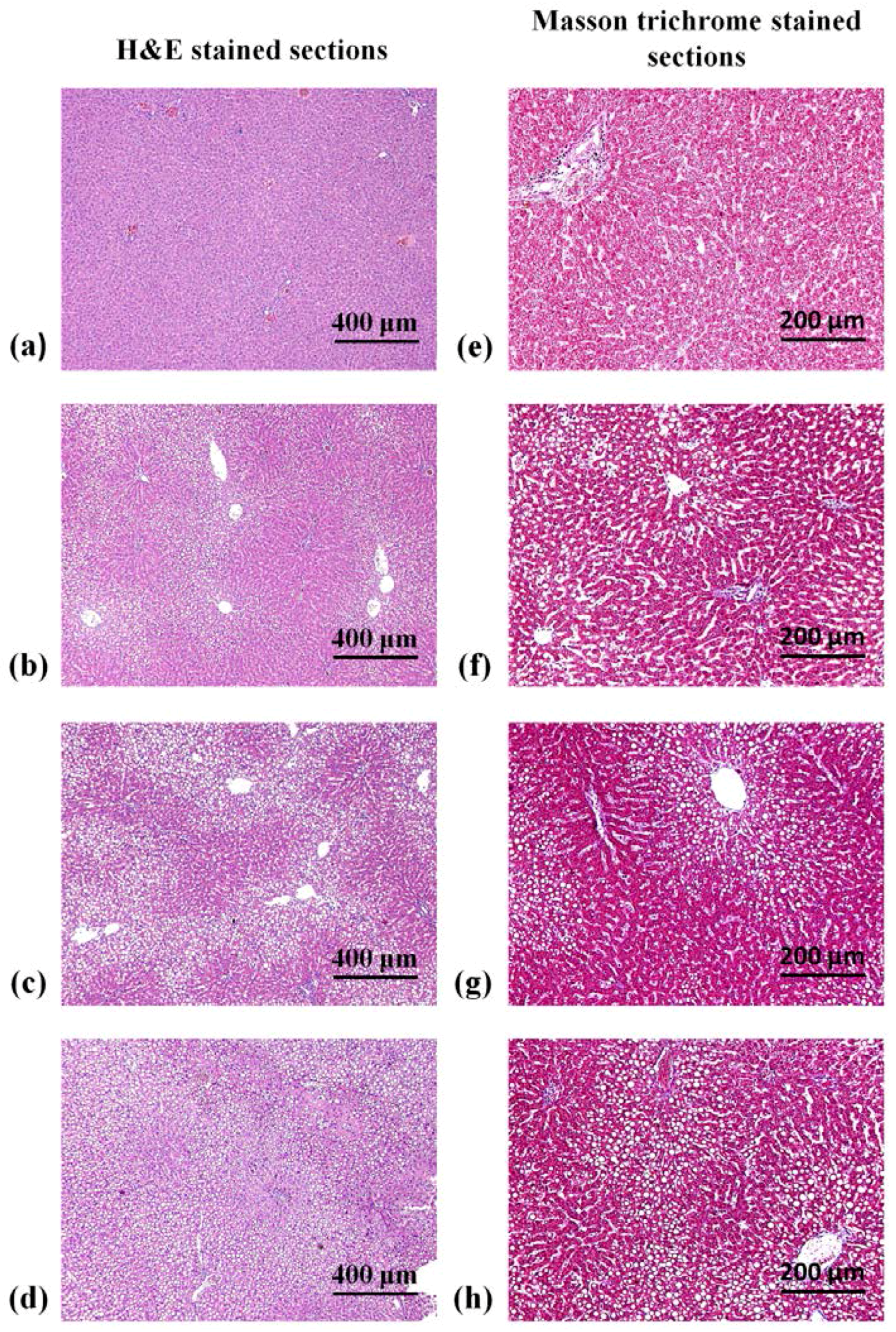
2.4. Histopathological Examinations
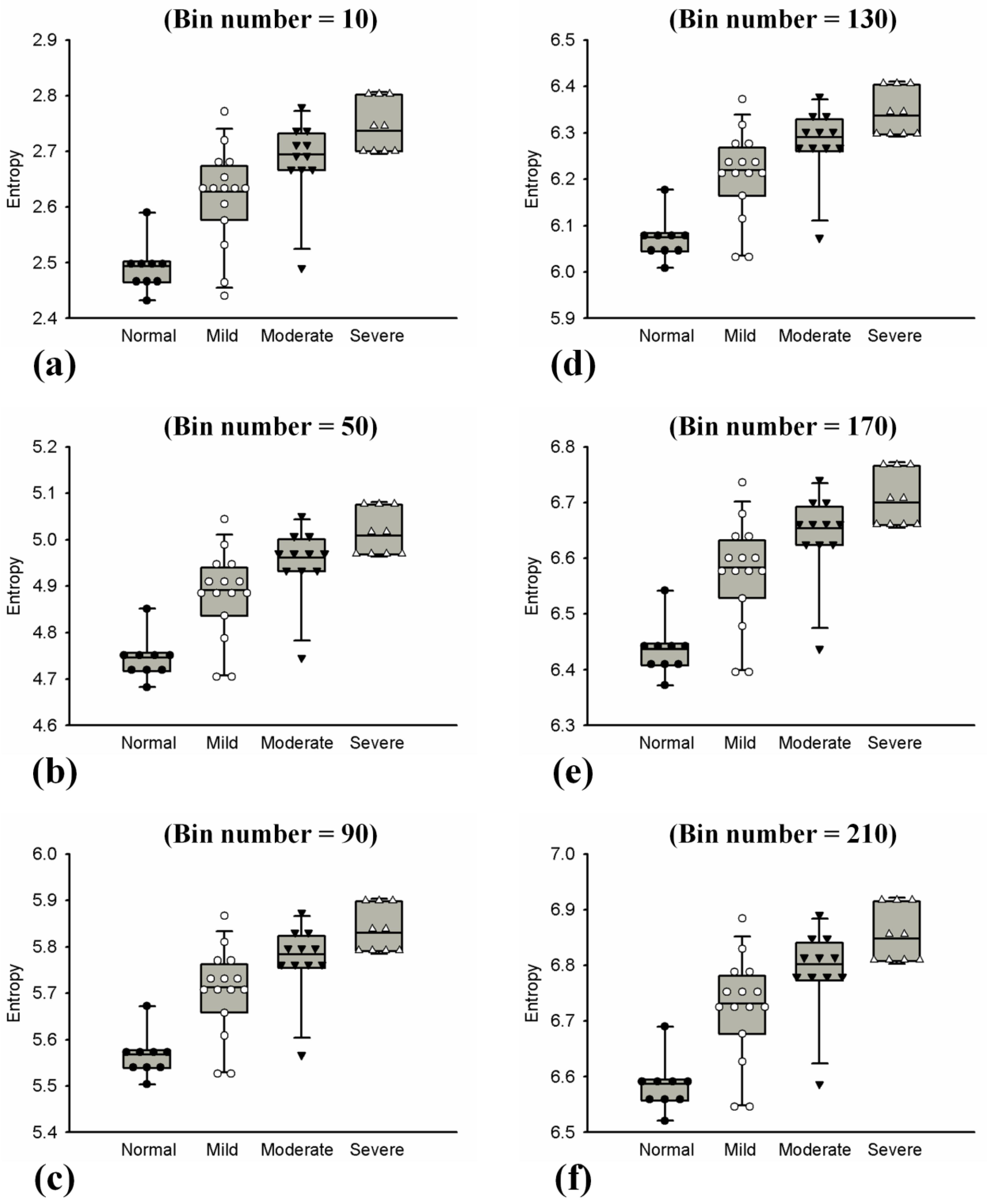
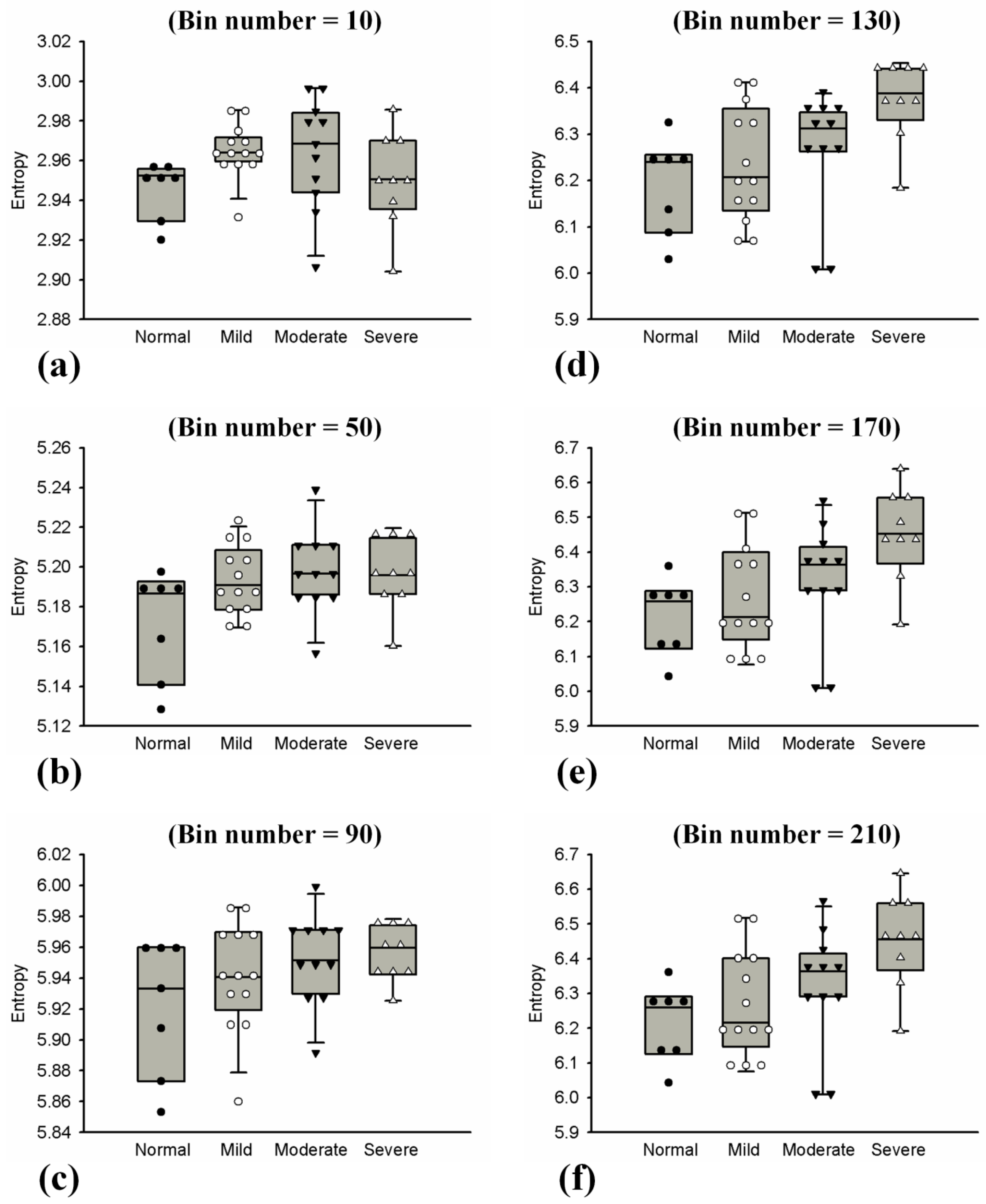
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Significance of This Study
4.2. Effects of Hepatic Steatosis On Entropy
4.3. Effects of NB on Entropy
4.4. Future Challenges and Work
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Zelber-Sagi, S.; Ratziu, V.; Oren, R. Nutrition and physical activity in NAFLD: An overview of the epidemiological evidence. World J. Gastroenterol. 2011, 17, 3377–3389. [Google Scholar] [CrossRef] [PubMed]
- Straub, B.K.; Schirmacher, P. Pathology and biopsy assessment of non-alcoholic fatty liver disease. Dig. Dis. 2010, 28, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Subramanya, M.B.; Kumar, V.; Mukherjee, S.; Saini, M. A CAD system for B-mode fatty liver ultrasound images using texture features. J. Med. Eng. Technol. 2015, 39, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Neuschwander-Tetri, B.A.; Caldwell, S.H. Nonalcoholic steatohepatitis: Summary of an AASLD Single Topic Conference. Hepatology 2003, 37, 1202–1219. [Google Scholar] [CrossRef] [PubMed]
- Raff, E.J.; Kakati, D.; Bloomer, J.R.; Shoreibah, M.; Rasheed, K.; Singal, A.K. Diabetes mellitus predicts occurrence of cirrhosis and hepatocellular cancer in alcoholic liver and non-alcoholic fatty liver diseases. J. Clin. Transl. Hepatol. 2015, 3, 9–16. [Google Scholar] [PubMed]
- Bravo, A.A.; Sheth, S.G.; Chopra, S. Liver biopsy. N. Engl. J. Med. 2001, 344, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Wieckowska, A.; McCullough, A.J.; Feldstein, A.E. Noninvasive diagnosis and monitoring of nonalcoholic steatohepatitis: Present and future. Hepatology 2007, 46, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, T.; Tadkod, A.; Hepburn, I.; Schade, R.R. Nonalcoholic fatty liver disease: Diagnosis and management. Am. Fam. Phys. 2013, 88, 35–42. [Google Scholar]
- Meisamy, S.; Hines, C.D.G.; Hamilton, G.; Sirlin, C.B.; McKenzie, C.A.; Yu, H.; Brittain, J.H.; Reeder, S.B. Quantification of hepatic steatosis with T1-independent, T2-corrected MR imaging with spectral modeling of fat: Blinded comparison with MR spectroscopy. Radiology 2011, 258, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.R.; Thomas, E.L.; Bell, J.D.; Johnston, D.G.; Taylor-Robinson, S.D. Non-invasive means of measuring hepatic fat content. World J. Gastroenterol. 2008, 14, 3476–3483. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Sirlin, C.B.; Schwimmer, J.B.; Lavine, J.E. Advances in pediatric nonalcoholic fatty liver disease. Hepatology 2009, 50, 1282–1293. [Google Scholar] [CrossRef] [PubMed]
- Schwenzer, N.F.; Springer, F.; Schraml, C.; Stefan, N.; Machann, J.; Schick, F. Non-invasive assessment and quantification of liver steatosis by ultrasound, computed tomography and magnetic resonance. J. Hepatol. 2009, 51, 433–445. [Google Scholar] [CrossRef] [PubMed]
- Destrempes, F.; Clotier, G. 2010 A critical review and uniformized representation of statistical distributions modeling the ultrasound echo envelope. Ultrasound Med. Biol. 2010, 36, 1037–1051. [Google Scholar] [CrossRef] [PubMed]
- Rubert, N.; Varghese, T. Mean scatterer spacing estimation using multi-taper coherence. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2013, 60, 1061–1073. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.L.; Tai, D.I.; Ma, Y.H.; Chiang, B.H.; Chen, C.K.; Tsui, P.H. Effects of fatty infiltration in human livers on the backscattered statistics of ultrasound imaging. Proc. Inst. Mech. Eng. Part H 2015, 229, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Son, J.Y.; Lee, J.Y.; Yi, N.; Lee, K.W.; Suh, K.S.; Lee, J.M.; Han, J.K.; Choi, B.I. Hepatic steatosis: Assessment with acoustic structure quantification of US imaging. Radiology 2016, 278, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Tsui, P.H.; Zhou, Z.; Lin, Y.H.; Hung, C.M.; Chung, S.J.; Wan, Y.L. Effect of ultrasound frequency on the Nakagami statistics of human liver tissues. PLoS ONE 2017, 12, e0181789. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.C.; Lee, Y.H.; Jeng, Y.M.; Chen, C.N.; Chang, K.J.; Tsui, P.H. Relationship between ultrasound backscattered statistics and the concentration of fatty droplets in livers: An animal study. PLoS ONE 2013, 8, e63543. [Google Scholar] [CrossRef] [PubMed]
- Ghoshal, G.; Lavarello, R.J.; Kemmerer, J.P.; Miller, R.J.; Oelze, M.L. Ex vivo study of quantitative ultrasound parameters in fatty rabbit livers. Ultrasound Med. Biol. 2012, 38, 2238–2248. [Google Scholar] [CrossRef] [PubMed]
- Tsui, P.H.; Huang, C.C.; Sun, L.; Dailey, S.H.; Shung, K.K. Characterization of lamina propria and vocal muscle in human vocal fold tissue by ultrasound Nakagami imaging. Med. Phys. 2011, 38, 2019–2026. [Google Scholar] [CrossRef] [PubMed]
- Bibicu, D.; Moraru, L.; Biswas, A. Thyroid nodule recognition based on feature selection and pixel classification methods. J. Digit. Imaging 2013, 26, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Moraru, L.; Moldovanu, S.; Culea-Florescu, A.-L.; Bibicu, D.; Ashour, A.S.; Dey, N. Texture analysis of parasitological liver fibrosis images. Microsc. Res. Tech. 2017, 80, 862–869. [Google Scholar] [CrossRef] [PubMed]
- Shannon, C.E. A Mathematical Theory of Communication. Bell Syst. Tech. J. 1948, 27, 379–423. [Google Scholar] [CrossRef]
- Hughes, M.S. Analysis of ultrasonic waveforms using Shannon entropy. IEEE Ultrason. Symp. Proc. 1992, 1, 1205–1209. [Google Scholar]
- Hughes, M.S. Analysis of digitized waveforms using Shannon entropy. II. High speed algorithms based on Green’s functions. J. Acoust. Soc. Am. 1994, 95, 2582–2588. [Google Scholar] [CrossRef]
- Hughes, M.S.; Marsh, J.N.; Wallace, K.D.; Donahue, T.A.; Connolly, A.M.; Lanza, G.M.; Wickline, A.S. Sensitive ultrasonic detection of dystrophic skeletal muscle in patients with duchenne muscular dystrophy using an entropy-based signal receiver. Ultrasound Med. Biol. 2007, 33, 1236–1243. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Huang, C.C.; Shung, K.K.; Tsui, P.H.; Fang, J.; Ma, H.Y.; Wu, S.; Lin, C.C. Entropic imaging of cataract lens: An in vitro study. PLoS ONE 2014, 9, e96195. [Google Scholar] [CrossRef] [PubMed]
- Tsui, P.H.; Wan, Y.L. Effects of fatty infiltration of the liver on the Shannon entropy of ultrasound backscattered signals. Entropy 2016, 18, 341. [Google Scholar] [CrossRef]
- Hebbard, L.; George, J. Animal models of nonalcoholic fatty liver disease. Nat. Rev. Gastroenterol. Hepatol. 2011, 8, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Dongiovanni, P.; Lanti, C.; Riso, P.; Valenti, L. Nutritional therapy for nonalcoholic fatty liver disease. J. Nutr. Biochem. 2015, 29, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kanuri, G.; Bergheim, I. In vitro and in vivo models of non-alcoholic fatty liver disease (NAFLD). Int. J. Mol. Sci. 2013, 14, 11963–11980. [Google Scholar] [CrossRef] [PubMed]
- Azhari, H. Basics of Biomedical Ultrasound for Engineers; Wiley: New York, NY, USA, 2010. [Google Scholar]
- Tsui, P.H.; Chang, C.C. Imaging local scatterer concentrations by the Nakagami statistical model. Ultrasound Med. Biol. 2007, 33, 608–619. [Google Scholar] [CrossRef] [PubMed]
- Han, D. Comparison of commonly used image interpolation methods. In Proceedings of the 2nd International Conference on Computer Science and Electronics Engineering, Los Angeles, CA, USA, 1–2 July 2013; pp. 1556–1559. [Google Scholar]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, E.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.C.; Torbenson, M.S.; Umalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Pike, R.; Sabatier, P. Scattering and Inverse Scattering in Pure and Applied Science; Academic Press: Burlington, MA, USA, 2001. [Google Scholar]
- Shung, K.K.; Thieme, G.A. Ultrasonic Scattering in Biological Tissues; CRC Press: Boca Raton, FL, USA, 1993. [Google Scholar]
- Nyquist, H. Certain topics in telegraph transmission theory. J. Am. Inst. Electr. Eng. 1928, 47, 617–644. [Google Scholar] [CrossRef]
- Shannon, C.E. Communication in the presence of noise. Proc. Inst. Radio Eng. 1949, 37, 10–21. [Google Scholar] [CrossRef]
- Ortiz, S.H.C.; Chiu, T.; Fox, M.D. Ultrasound image enhancement: A review. Biomed. Signal Process. Control 2012, 7, 419–428. [Google Scholar] [CrossRef]
- Oelze, M.L.; Mamou, J. Review of quantitative ultrasound-Envelope statistics and backscatter coefficient imaging and contributions to diagnostic ultrasound. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2016, 63, 336–351. [Google Scholar] [CrossRef] [PubMed]
- Suffern, K. Ray Tracing from the Ground Up; A K Peters: Natick, MA, USA, 2007. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group | MCD for 1 Week | MCD for 1.5 Weeks | MCD for 2 Weeks | |
|---|---|---|---|---|
| Steatosis (score, 0–3) | 0, 0, 0, 1, 1, 1, 0, 0, 0, 0, 0, 0 | 1, 1, 1, 0, 2, 1, 1, 1, 1, 2, 1, 1 | 3, 1, 3, 2, 2, 1, 3, 2, 2, 2, 2, 2 | 3, 3, 1, 2, 3, 1, 3, 3, 2, 2, 3, 2 |
| Lobular inflammation (score, 0–3) | 0, 0, 0, 0, 1, 1, 0, 0, 0, 0, 0, 0 | 1, 1, 1, 1, 1, 0, 1, 0, 1, 0, 0, 0 | 1, 1, 1, 0, 1, 1, 1, 1, 0, 0, 0, 0 | 1, 0, 1, 0, 1, 0, 1, 1, 0, 0, 0, 0 |
| Hepatocyte ballooning (score, 0–2) | 0, 0, 0, 0, 0, 0, 0, 0, 0, 0, 0, 1 | 1, 1, 0, 0, 1, 1, 1, 0, 1, 2, 1, 0 | 1, 1, 1, 1, 0, 1, 0, 1, 1, 1, 0, 0 | 1, 1, 1, 1, 1, 1, 1, 1, 1, 1, 0, 1 |
| Steatohepatitis (score, 0–8) | 0, 0, 0, 1, 2, 2, 0, 0, 0, 0, 0, 1 | 3, 3, 2, 1, 4, 2, 3, 1, 3, 4, 2, 1 | 5, 3, 5, 3, 3, 3, 4, 4, 3, 3, 2, 2 | 5, 4, 3, 3, 5, 2, 5, 5, 3, 3, 3, 3 |
| Fibrosis (stage, 0–4) | 0, 0, 0, 0, 0, 0, 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0, 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0, 0, 0, 0, 0, 0, 0 | 0, 0, 0, 0, 0, 0, 0, 0, 0, 0, 0, 0 |
| Cut off Value | AUC (95% CI) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Accuracy (%) | |
|---|---|---|---|---|---|---|---|
| Bin number = 10 | |||||||
| ≥mild | 2.5093 | 0.9302 (0.8106–1) | 88.8889 | 91.4286 | 72.7273 | 96.9697 | 90.9091 |
| ≥moderate | 2.6468 | 0.8979 (0.8029–1) | 83.3333 | 95 | 95.2381 | 82.6087 | 88.6364 |
| ≥severe | 2.6945 | 0.8952 (0.7984–0.992) | 80 | 100 | 100 | 56.25 | 84.0909 |
| Bin number = 50 | |||||||
| ≥mild | 4.7636 | 0.9316 (0.8106–1) | 88.8889 | 91.4286 | 72.7273 | 96.9697 | 90.9091 |
| ≥moderate | 4.9913 | 0.8979 (0.8029–0.9929) | 83.3333 | 95 | 95.2381 | 82.6087 | 88.6364 |
| ≥severe | 4.9616 | 0.8952 (0.7984–0.992) | 80 | 100 | 100 | 56.25 | 84.0909 |
| Bin number = 90 | |||||||
| ≥mild | 5.5846 | 0.9302 (0.8106–1) | 88.8889 | 91.4286 | 72.7273 | 96.9697 | 90.9091 |
| ≥moderate | 5.7329 | 0.8979 (0.8029–0.9929) | 83.3333 | 95 | 95.2381 | 82.6087 | 88.6364 |
| ≥severe | 5.784 | 0.8952 (0.7984–0.992) | 80 | 100 | 100 | 56.25 | 84.0909 |
| Bin number = 130 | |||||||
| ≥mild | 6.0903 | 0.9302 (0.8106-1) | 88.8889 | 91.4286 | 72.7273 | 96.9697 | 90.9091 |
| ≥moderate | 6.2392 | 0.8979 (0.8029–0.9929) | 83.3333 | 95 | 95.2381 | 82.6087 | 88.6364 |
| ≥severe | 6.2901 | 0.8952 (0.7984–0.992) | 80 | 100 | 100 | 56.25 | 84.0909 |
| Bin number = 170 | |||||||
| ≥mild | 6.4544 | 0.9302 (0.8106–1) | 88.8889 | 91.4286 | 72.7273 | 96.9697 | 90.9091 |
| ≥moderate | 6.6021 | 0.8979 (0.8029–0.9929) | 83.3333 | 95 | 95.2381 | 82.6087 | 88.6364 |
| ≥severe | 6.6535 | 0.8952 (0.7984-0.992) | 80 | 100 | 100 | 56.25 | 84.0909 |
| Bin number = 210 | |||||||
| ≥mild | 6.6027 | 0.9302 (0.8106-1) | 88.8889 | 91.4286 | 72.7273 | 96.9697 | 90.9091 |
| ≥moderate | 6.7518 | 0.8979 (0.8029-0.9929) | 83.3333 | 95 | 95.2381 | 82.6087 | 88.6364 |
| ≥severe | 6.8022 | 0.8952 (0.7984-0.992) | 80 | 100 | 100 | 56.25 | 84.0909 |
| Cut off Value | AUC (95% CI) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Accuracy (%) | |
|---|---|---|---|---|---|---|---|
| Bin number = 10 | |||||||
| ≥mild | 2.9578 | 0.7489 (0.5231–0.9747) | 100 | 63.6364 | 36.8421 | 100 | 70 |
| ≥moderate | 2.9683 | 0.51 (0.3246–0.6954) | 85 | 45 | 60.7143 | 75 | 65 |
| ≥severe | 2.9511 | 0.629 (0.4074–0.8507) | 66.6667 | 74.1935 | 42.8571 | 88.4615 | 72.5 |
| Bin number = 50 | |||||||
| ≥mild | 5.1926 | 0.7532 (0.5286–0.9979) | 85.7143 | 57.5758 | 30 | 95 | 62.5 |
| ≥moderate | 5.1926 | 0.6425 (0.467–0.818) | 65 | 65 | 65 | 65 | 65 |
| ≥severe | 5.1936 | 0.6129 (0.4071–0.8187) | 61.2903 | 66.6667 | 86.3636 | 33.3333 | 62.5 |
| Bin number = 90 | |||||||
| ≥mild | 5.9331 | 0.7056 (0.4701–0.9411) | 57.1429 | 75.7576 | 33.3333 | 89.2857 | 72.5 |
| ≥moderate | 5.9463 | 0.6575 (0.4841–0.8308) | 60 | 70 | 66.6667 | 63.3636 | 65 |
| ≥severe | 5.9467 | 0.6237 (0.4201-0.8272) | 51.6129 | 66.6667 | 84.2105 | 28.5714 | 55 |
| Bin number = 130 | |||||||
| ≥mild | 6.2553 | 0.7359 (0.5069–0.965) | 85.7143 | 66.6667 | 35.2941 | 95.6521 | 70 |
| ≥moderate | 6.2253 | 0.7425 (0.5857–0.8993) | 70 | 85 | 82.3529 | 73.913 | 77.5 |
| ≥severe | 6.3475 | 0.8351 (0.7033–0.967) | 83.871 | 77.7778 | 92.8571 | 58.3333 | 82.5 |
| Bin number = 170 | |||||||
| ≥mild | 6.2879 | 0.7446 (0.5176–0.9715) | 85.7143 | 66.6667 | 35.2941 | 95.6522 | 70 |
| ≥moderate | 6.2879 | 0.75 (0.595–0.905) | 70 | 85 | 82.3529 | 73.913 | 77.5 |
| ≥severe | 6.3914 | 0.8172 (0.6771–0.9573) | 80.6451 | 77.7778 | 92.5926 | 53.8461 | 80 |
| Bin number = 210 | |||||||
| ≥mild | 6.2907 | 0.7593 (0.5069–0.965) | 85.7143 | 63.6364 | 33.3333 | 95.4545 | 67.5 |
| ≥moderate | 6.2907 | 0.7475 (0.5919–0.9031) | 70 | 80 | 77.7778 | 72.7273 | 75 |
| ≥severe | 6.3946 | 0.8136 (0.6719-0.9553) | 80.6452 | 77.7778 | 92.5926 | 53.8462 | 80 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fang, J.; Chang, N.-F.; Tsui, P.-H. Performance Evaluations on Using Entropy of Ultrasound Log-Compressed Envelope Images for Hepatic Steatosis Assessment: An In Vivo Animal Study. Entropy 2018, 20, 120. https://doi.org/10.3390/e20020120
Fang J, Chang N-F, Tsui P-H. Performance Evaluations on Using Entropy of Ultrasound Log-Compressed Envelope Images for Hepatic Steatosis Assessment: An In Vivo Animal Study. Entropy. 2018; 20(2):120. https://doi.org/10.3390/e20020120
Chicago/Turabian StyleFang, Jui, Ning-Fang Chang, and Po-Hsiang Tsui. 2018. "Performance Evaluations on Using Entropy of Ultrasound Log-Compressed Envelope Images for Hepatic Steatosis Assessment: An In Vivo Animal Study" Entropy 20, no. 2: 120. https://doi.org/10.3390/e20020120
APA StyleFang, J., Chang, N. -F., & Tsui, P. -H. (2018). Performance Evaluations on Using Entropy of Ultrasound Log-Compressed Envelope Images for Hepatic Steatosis Assessment: An In Vivo Animal Study. Entropy, 20(2), 120. https://doi.org/10.3390/e20020120