Nasal Delivery of High Molecular Weight Drugs

Abstract
:Introduction
Nasal Mucosa and Enhancing Drug Passage through the Nasal Route
Nasal route
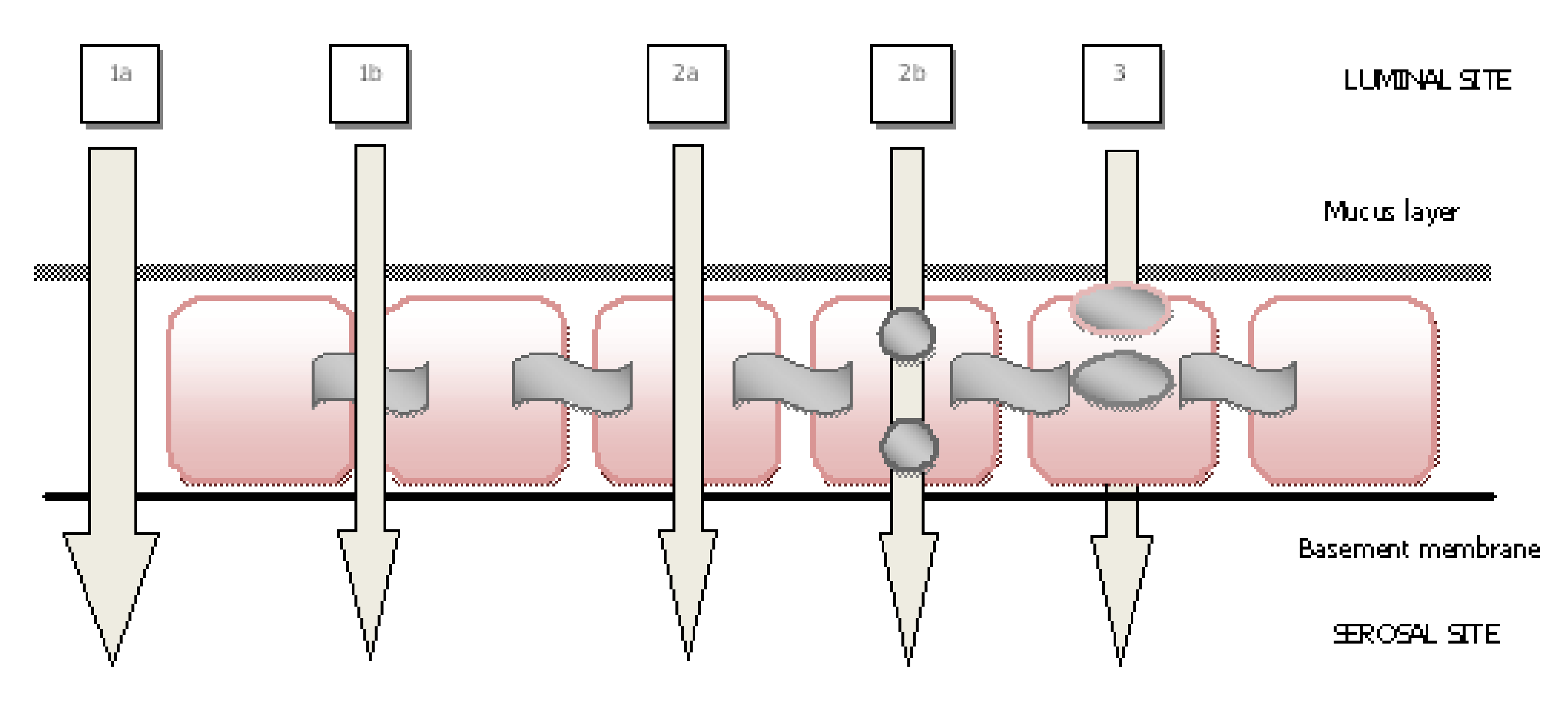
Passage routes of drugs via nasal mucosa
Improving nasal mucosa transport
- (a)
- Modification of the chemical structure of the peptide to increase metabolic stability and/or membrane permeability [19].
- (b)
- There are oxidative, conjugative enzymes, and exopeptidases and endopeptidases in the nasal cavity [22]. This vast diversity of enzymes leads to a “pseudo first pass effect” which hinders the absorption of protein peptide drugs. The drug may be applied with enzyme inhibitors to protect them from the activity of these enzymes in the mucosa [21].
- (c)
- (d)
Nano-/ micro-particulate systems
Macromolecular Drugs
Insulin
Desmopressin
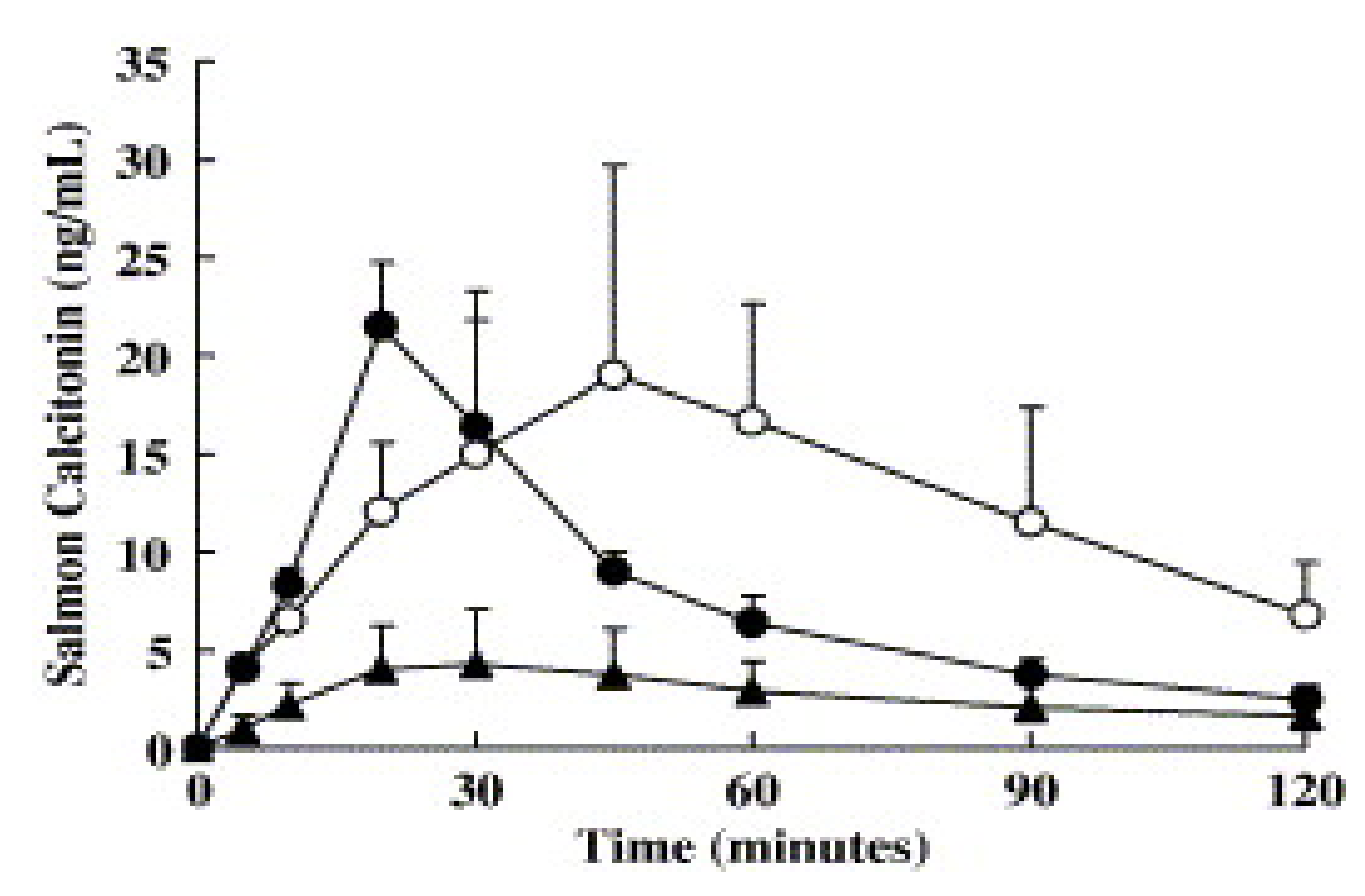
Salmon calcitonin
LHRH-agonists
Human growth hormone
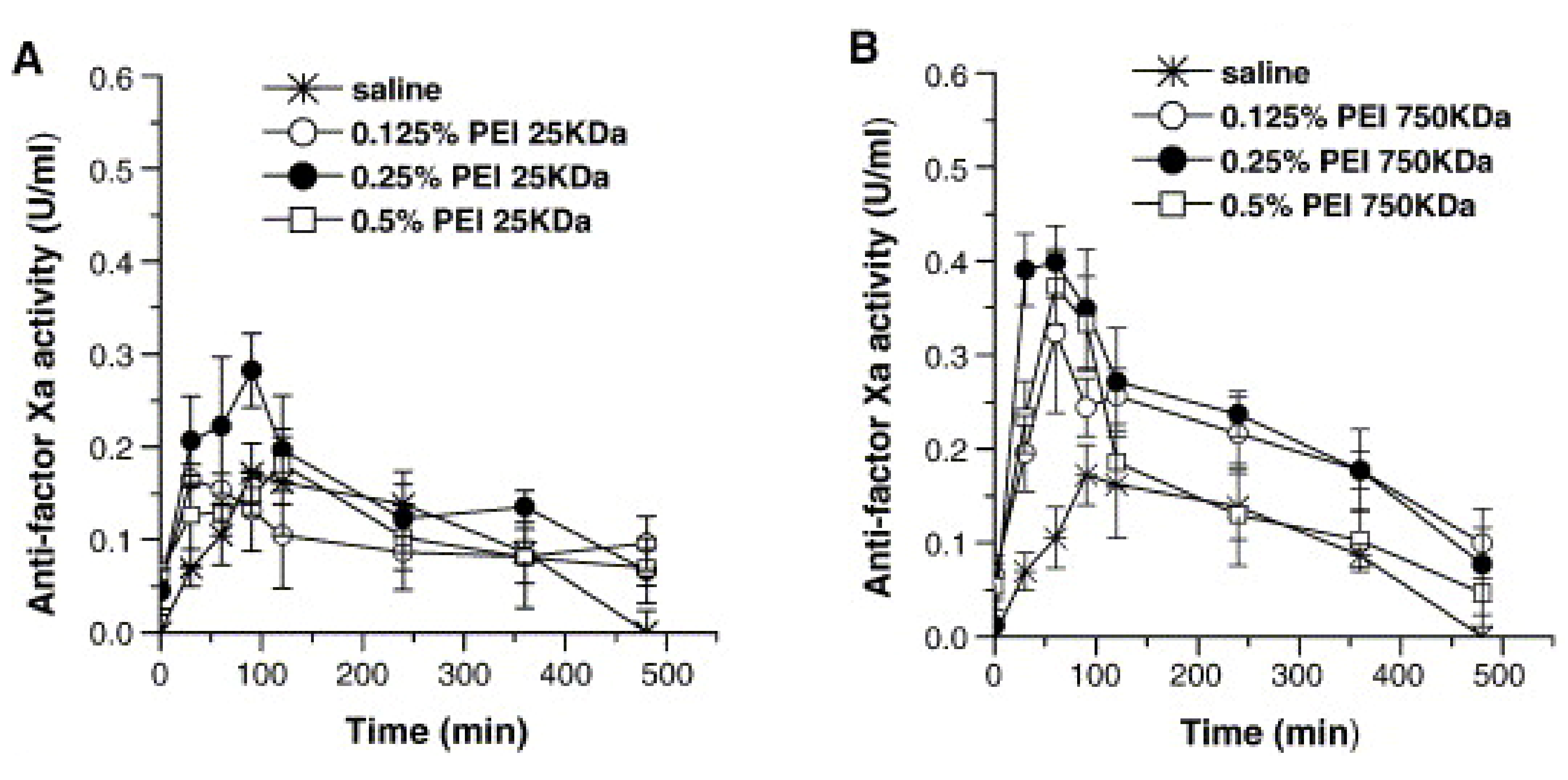
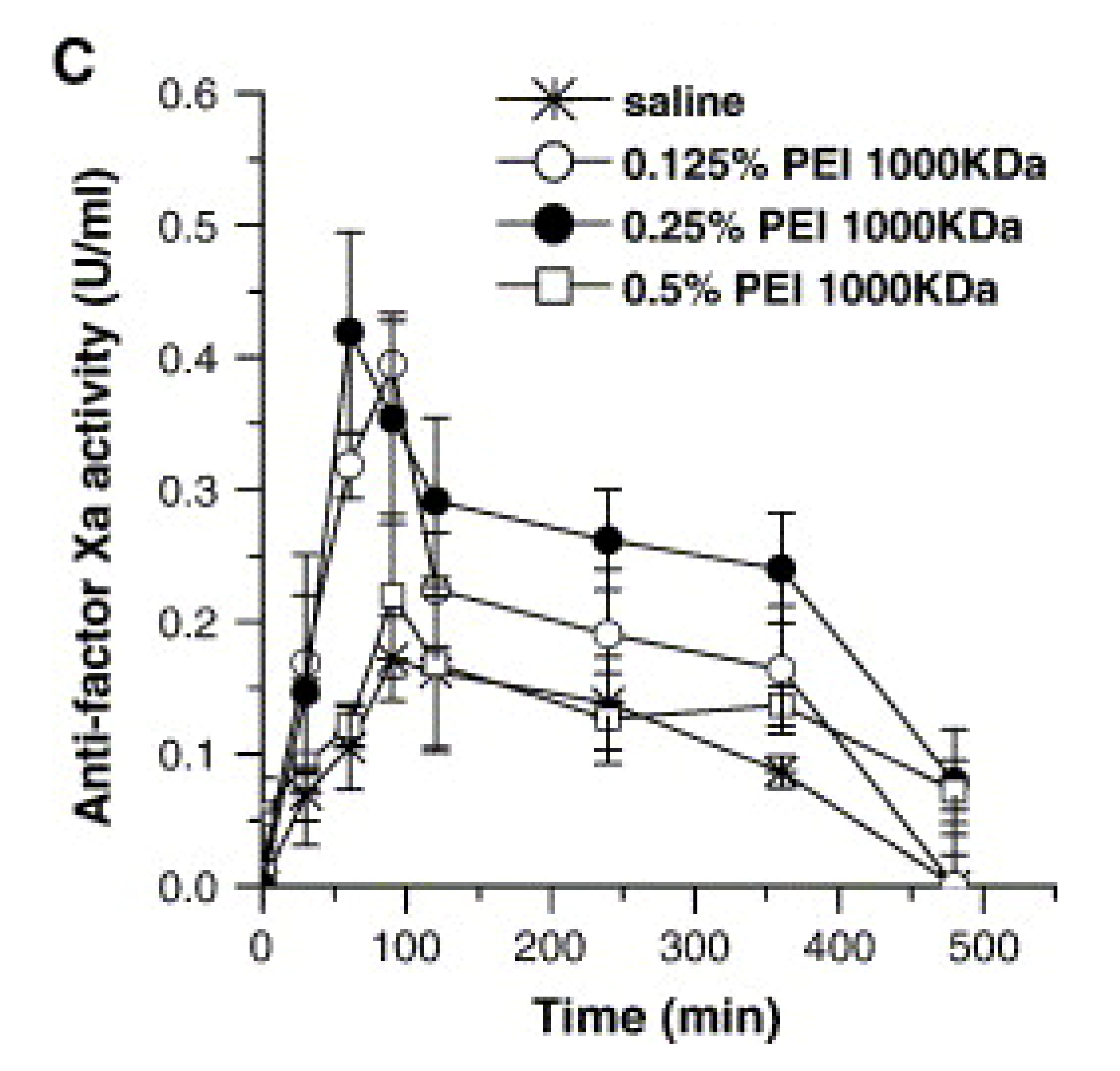
Heparin
Other macromolecules
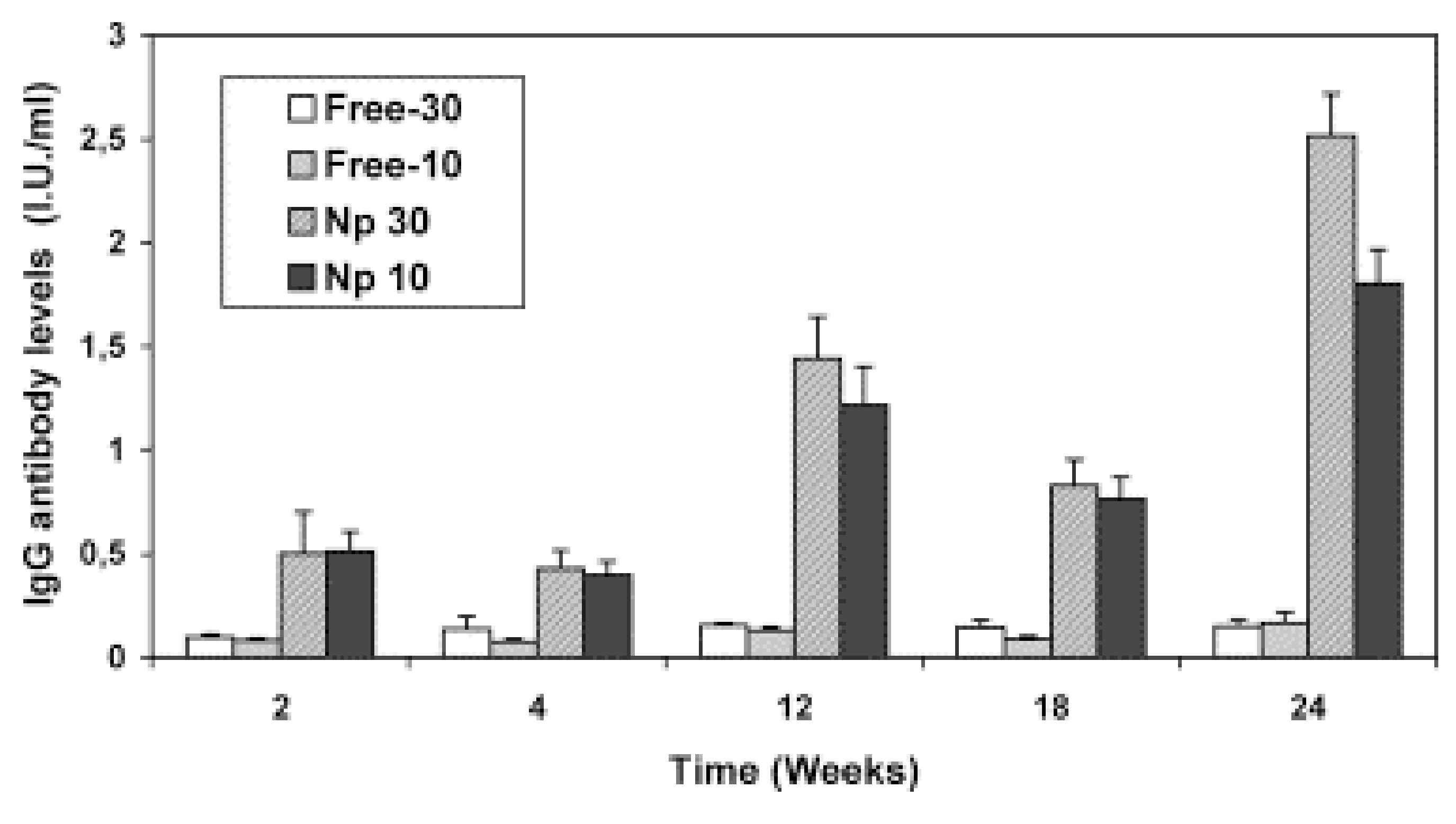
Vaccines
Conclusions
References
- Ugwoke, M.I.; Verbeke, N.; Kinget, R. The biopharmaceutical aspects of nasal mucoadhesive drug delivery. J. Pharm. Pharmacol. 2001, 53, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Behl, C.R.; Pimplaskar, H.K.; Sileno, A.P.; deMeireles, J.; Romeo, V.D. Effects of physicochemical properties and other factors on systemic nasal drug delivery. Adv. Drug Deliv. Rev. 1998, 29, 89–116. [Google Scholar] [CrossRef]
- Arora, P.; Sharma, S.; Garg, S. Permeability issues in nasal drug delivery. Drug Discov. Today 2002, 7, 967–975. [Google Scholar] [CrossRef]
- Cornaz, A.L.; Buri, P. Nasal Mucosa as an Absorption Barrier. Eur. J. Pharm. Biopharm. 1994, 40, 261–270. [Google Scholar]
- Jones, N. The Nose and paranasal sinuses physiology and anatomy. Adv. Drug Deliv. Rev. 2001, 51, 5–19. [Google Scholar] [CrossRef]
- Sciarra, J.J. Remington: The Science and Practice of Pharmacy; Gennaro, A.R., Ed.; Mack Publishing Company: Easton, PA, USA, 1995; Chapter 95; p. 1676. [Google Scholar]
- Sanders, P.; Washington, N.; Frier, M.; Wilson, C.G.; Feely, L.C.; Washington, C. The deposition of solution-based and suspension-based aerosols from metered dose inhalers in healthy subjects and asthmatic patients. S.T.P. Pharm. Sci. 1997, 7, 300–306. [Google Scholar]
- Schipper, N.G.; Verhoef, J.C.; Merkus, F.W. The nasal mucociliary clearance: Relevance to nasal drug delivery. Pharm. Res. 1991, 8, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Ingemann, M.; Frokjaer, S.; Hovgaard, L.; Brøndsted, H. Peptide and Protein Drug Delivery Systems for Non-Parenteral Routes of Administration. In Pharmaceutical Formulation Development of Peptides and Proteins; Frokjaer, S., Hovgaard, L., Eds.; Taylor & Francis: Philadelphia, PA, USA, 2000; Chapter 10; p. 189. [Google Scholar]
- Wermeling, D.P.; Miller, J.L. Intranasal Drug Delivery. In Modified Release Drug Delivery Technology; Rathbone, M.J., Hadgraft, J., Roberts, M.S., Eds.; Marcel Dekker, Inc.: New York, NY, USA, 2002; Chapter 61; p. 727. [Google Scholar]
- Ungell, A.L.; Andreasson, A.; Lundin, K.; Utter, L. Effects of enzymatic inhibition and increased paracellular shunting on transport of vasopressin analogues in the rat. J. Pharm. Sci. 1992, 81, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Corbo, D.C.; Liu, J.C.; Chien, Y.W. Drug absorption through mucosal membranes: Effect of mucosal route and penetrant hydrophilicity. Pharm. Res. 1989, 6, 848–852. [Google Scholar] [CrossRef] [PubMed]
- McMartin, C.; Hutchinson, L.E.; Hyde, R.; Peters, G.E. Analysis of structural requirements for the absorption of drugs and macromolecules from the nasal cavity. J. Pharm. Sci. 1987, 76, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Tuma, P.L.; Hubbard, L. Transcytosis: Crossing cellular barriers. Physiol. Rev. 2003, 83, 871–932. [Google Scholar] [CrossRef] [PubMed]
- Illum, L. Nasal Drug delivery-possibilities, problems and solutions. J. Control. Release 2003, 87, 187–198. [Google Scholar] [CrossRef]
- Hussain, A.A. Intranasal drug delivery. Adv. Drug Deliv. Rev. 1998, 29, 39–49. [Google Scholar] [CrossRef]
- O’Hagan, D.T.; Illum, L. Absorption of peptides and proteins from the respiratory tract and the potential for development of locally administered vaccine. Crit. Rev. Ther. Drug Carrier Syst. 1990, 7, 35–97. [Google Scholar] [PubMed]
- Irwin, W.J.; Dwivedi, A.K.; Holbrook, P.A.; Dey, M.J. The Effect of cyclodextrins on the stability of peptides in nasal enzymic systems. Pharm. Res. 1994, 11, 1698–1703. [Google Scholar] [CrossRef] [PubMed]
- Morita, T.; Yamahara, H. Encyclopedia of Pharmaceutical Technology, 3rd ed.; Swarbrick, J., Ed.; Informa Healthcare: London, UK, 2007; Vol. 4, p. 2678. [Google Scholar]
- Stolnic, S.; Shakesheff, K. Formulation for delivery the therapeutics proteins. Biotechnol. Lett. 2009, 31, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Romeo, V.D.; deMeireles, J.C.; Gries, W.J.; Xia, W.J.; Sileno, A.P.; Pimplaskar, H.K.; Behl, C.R. Optimization of systemic nasal drug delivery with pharmaceutical excipients. Adv. Drug Deliv. Rev. 1998, 29, 117–133. [Google Scholar] [PubMed]
- Sarkar, M.A. Drug Metabolism in the nasal mucosa. Pharm. Res. 1992, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ozsoy, Y.; Tunçel, T.; Can, A.; Akev, N.; Birteksöz, S.; Gerçeker, A. In vivo studies on nasal preparations of ciprofloxacin hydrochloride. Pharmazie 2000, 55, 607–609. [Google Scholar] [PubMed]
- Davis, S.S.; Illum, L. Absorption enhancers for nasal drug delivery. Clin. Pharmacokinet. 2003, 42, 1107–1128. [Google Scholar] [CrossRef] [PubMed]
- Law, S.L.; Huang, K.J.; Chou, H.Y. Preparation of desmopressin-containing liposomes for intranasal delivery. J. Control. Release 2001, 70, 375–382. [Google Scholar] [CrossRef]
- Mitra, R.; Pezron, I.; Chu, W.A.; Mitra, A.K. Lipid emulsions as vehicles for enhanced nasal delivery of insulin. Int. J. Pharm. 2000, 205, 127–134. [Google Scholar] [CrossRef]
- Kumar, M.; Pathak, K.; Misra, A. Formulation and characterization of nanoemulsion-based drug delivery system of risperidone. Drug Dev. Ind. Pharm. 2009, 35, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Gungor, S.; Okyar, A.; Erturk-Toker, S.; Baktir, G.; Ozsoy, Y. Ondansetron-loaded biodegradable microspheres as a nasal sustained delivery system: In vitro/in vivo studies. Pharm. Dev. Tech. 2009. [Google Scholar] [CrossRef]
- Gungor, S.; Okyar, A.; Erturk-Toker, S.; Baktir, G.; Ozsoy, Y. In Vitro and in Vivo Studies on Ondansetron HCl-Loaded Chitosan Microspheres for Nasal Drug Delivery. 6th World Meeting on Pharmaceutics, Biopharmaceutics and Pharmaceutical Technology, Barcelona, Spain, 7–10 April 2008. [Google Scholar]
- Brooking, J.; Davis, S.S.; Illum, L. Transport of nanoparticles accross the rat nasal mucosa. J. Drug Target. 2001, 9, 267–279. [Google Scholar] [CrossRef] [PubMed]
- McGinity, J.W.; O’Donnell, P.B. Preparation of microspheres by the solvent evaporation technique. Adv. Drug Deliv. Rev. 1997, 28, 25–42. [Google Scholar] [PubMed]
- Rajaonarivony, M.; Vauthier, C.; Couarraze, G.; Puisieux, F.; Couvreur, P. Development of a new drug carrier made from alginate. J. Pharm. Sci. 1993, 82, 912–917. [Google Scholar] [CrossRef] [PubMed]
- Chowdary, K.P.; Rao, Y.S. Mucoadhesive microspheres for controlled drug delivery. Biol. Pharm. Bull. 2004, 27, 1717–1724. [Google Scholar] [CrossRef] [PubMed]
- Agnihotri, S.A.; Mallikarjuna, N.N.; Aminabhavi, T.M. Recent advances on chitosan-based micro- and nanoparticles in drug delivery. J. Control. Release 2004, 100, 5–28. [Google Scholar] [CrossRef] [PubMed]
- Ozsoy, Y. Handbook of Particulate Drug Delivery; Kumar, M.N.V.R., Ed.; American Scientific Publisher: Stevenson Ranch, CA, USA, 2008; Vol. 2, Chapter 8; p. 143. [Google Scholar]
- van der Lubben, I.M.; Verhoef, J.C.; Borchard, G.; Junginger, H.E. Chitosan and its derivatives in mucosal drug and vaccine delivery. Eur. J. Pharm. Sci. 2001, 14, 201–207. [Google Scholar] [CrossRef]
- Wong, T.W. Chitosan and its use in design of insulin delivery system. Recent Pat. Drug Deliv. Formul. 2009, 3, 8–25. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, I.; Green, K.L.; Smart, J.D.; Smistad, G.; Karlsen, J. Bioadhesion of hydrated chitosan: An in vitro and in vivo study. Int. J. Pharm. 1996, 145, 231–240. [Google Scholar] [CrossRef]
- Schipper, N.G.; Olsson, S.; Hoogstraate, J.A.; deBoer, A.G.; Varum, K.M.; Artursson, P. Chitosans as absorption enhancers for poorly absorbable drugs 2: Mechanism of absorption enhancement. Pharm. Res. 1997, 14, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Lehr, C.M.; Bouwstra, J.A.; Schacht, E.H.; Junginger, H.E. In vitro evaluation of mucoadhesive properties of chitosan and some other natural polymers. Int. J. Pharm. 1992, 78, 43–48. [Google Scholar] [CrossRef]
- Artursson, P.; Lindmark, T.; Davis, S.S.; Illum, L. Effect of chitosan on the permeability of monolayers of intestinal epithelial cells (Caco-2). Pharm. Res. 1994, 11, 1358–1361. [Google Scholar] [CrossRef] [PubMed]
- Alpar, H.O.; Eyles, J.E.; Williamson, E.D.; Somavarapu, S. Intranasal vaccination against plague, tetanus and diphtheria. Adv. Drug Deliv. Rev. 2001, 51, 173–201. [Google Scholar] [CrossRef]
- Vila, A.; Sánchez, A.; Tobío, M.; Calvo, P.; Alonso, M.J. Design of biodegradable particles for protein delivery. J. Control. Release 2002, 78, 15–24. [Google Scholar] [CrossRef]
- Vila, A.; Sánchez, A.; Evora, C.; Soriano, I.; Vila Jato, J.L.; Alonso, M.J. PEG-PLA nanoparticles as carriers for nasal vaccine delivery. J. Aerosol. Med. 2004, 17, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Farraj, N.F.; Johansen, B.R.; Davis, SS.; Illum, L. Nasal administration of insulin using bioadhesive microspheres as a delivery system. J. Control. Release 1990, 13, 253–261. [Google Scholar] [CrossRef]
- Björk, E.; Edman, P. Characterization of degradable starch microspheres as a nasal delivery system for drugs. Int. J. Pharm. 1990, 62, 187–192. [Google Scholar] [CrossRef]
- Edman, P.; Björk, E.; Ryden, L. Microspheres as a nasal delivery system for peptide drugs. J. Control. Release 1992, 21, 165–172. [Google Scholar] [CrossRef]
- Callens, C.; Remon, J.P. Evaluation of starch-maltodextrin-carbopol 974 P mixtures for the nasal delivery of insulin in rabbits. J. Control. Release 2000, 66, 215–220. [Google Scholar] [CrossRef]
- Illum, L.; Fisher, A.N.; Jabbal-Gill, I.; Davis, S.S. Bioadhesive starch microspheres and absorption enhancing agents act synergistically to enhance the nasal absorption of polypeptides. Int. J. Pharm. 2001, 222, 109–119. [Google Scholar] [CrossRef]
- Callens, C.; Pringels, E.; Remon, J.P. Influence of multiple nasal administrations of bioadhesive powders on the insulin bioavailability. Int. J. Pharm. 2003, 250, 415–422. [Google Scholar] [CrossRef]
- Pringels, E.; Vervaet, C.; Verbeeck, R.; Foreman, P.; Remon, J.P. The addition of calcium ions to starch/carbopol mixtures enhances the nasal bioavailability of insulin. Eur. J. Pharm. Biopharm. 2008, 68, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.K.; Khar, R. K.; Ahmed, F. J.; Diwan, P.V. Effective insulin delivery using starch nanoparticles as a potential trans-nasal mucoadhesive carrier. Eur. J. Pharm. Biopharm. 2008, 69, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Pereswetoff-Morath, L.; Edman, P. Dextran microspheres as a potential nasal drug delivery system for insulin-in vitro and in vivo properties. Int. J. Pharm. 1995, 124, 37–44. [Google Scholar] [CrossRef]
- Takenaga, M.; Serizawa, Y.; Azechi, Y.; Ochiai, A.; Kosaka, Y.; Igarashi, R.; Mizushima, Y. Microparticle resins as a potential nasal drug delivery system for insulin. J. Control. Release 1998, 52, 81–87. [Google Scholar] [CrossRef]
- Illum, L.; Farraj, N.F.; Fisher, A.N.; Gill, I.; Miglietta, M.; Benedetti, L.M. Hyaluronic acid ester microspheres as a nasal delivery system for insulin. J. Control. Release 1994, 29, 133–141. [Google Scholar] [CrossRef]
- Fernandez-Urrusuno, R.; Romani, D.; Calvo, P.; Vila-Jato, J.L.; Alonso, M.J. Development of a freeze-dried formulation of insulin-loaded chitosan nanoparticles intended for nasal administration. S.T.P. Pharma. Sci. 1999, 9, 429–436. [Google Scholar]
- Varshosaz, J.; Sadrai, H.; Alinagari, R. Nasal delivery of insulin using chitosan microspheres. J. Microencapsul. 2004, 21, 761–774. [Google Scholar] [CrossRef] [PubMed]
- Krauland, A.H.; Leitner, V.M.; Grabovac, V.; Bernkop-Schnürch, A. In vivo evealuation of a nasal insulin delivery system based on thiolated chitosan. J. Pharm. Sci. 2006, 95, 2463–2472. [Google Scholar] [CrossRef] [PubMed]
- Krauland, A.H.; Alonso, M.J. Chitosan/cyclodextrin nanoparticles as macromolecular drug delivery system. Int. J. Pharm. 2007, 340, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Bhumkar, D.R.; Joshi, H.M.; Sastry, M.; Pokharkar, V.B. Chitosan reduced gold nanoparticles as novel carriers for transmucosal delivery of insulin. Pharm. Res. 2007, 24, 1415–1426. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zheng, C.; Wu, Z.; Teng, D.; Zhang, X.; Wang, Z.; Li, C. Chitosan-NAC nanoparticles as a Vehicle for nasal absorption enhancement of insulin. J. Biomed. Mater. Res. 2009, 88, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Teijeiro-Osorio, D.; Remunán-López, C.; Alonso, M.J. New generation of hybrid poly/oligosaccharide nanoparticles as carriers for the nasal delivery of macromolecules. Biomacromolecules 2009, 10, 243–249. [Google Scholar] [CrossRef] [PubMed]
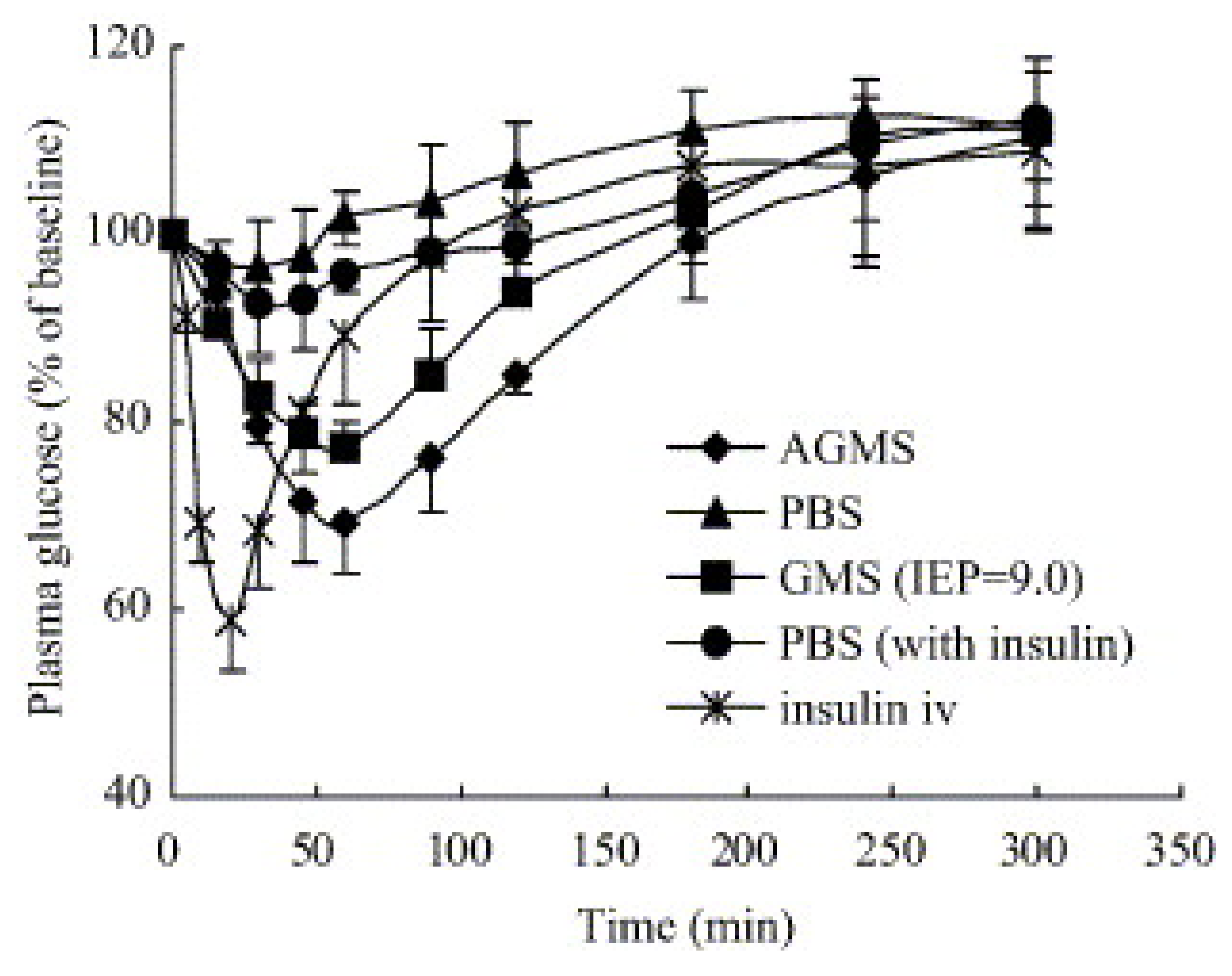
- Wang, J.; Tabata, Y.; Morimoto, K. Aminated gelatin microspheres as a nasal delivery system for peptide drugs: Evaluation of in vitro release and in vivo absorption in rats. J. Control. Release 2006, 113, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Khafagy, E.S.; Morishita, M.; Isowa, K.; Imai, J.; Takayama, K. Effect of cell-penetrating peptides on the nasal absorption of insulin. J. Control. Release 2009, 133, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Moeller, E.M.; Jorgensen, L. Alternative routes of administration for systemic delivery of protein pharmaceuticals. Drug Discov. Today Technol. 2008. [Google Scholar] [CrossRef] [PubMed]
- Critchley, H.; Davis, S.S.; Farraj, N.F.; Illum, L. Nasal absorption of desmopressin in rats and sheep. Effect of a bioadhesive microsphere delivery system. J. Pharm. Pharmacol. 1994, 46, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Fransén, N.; Bredenberg, S.; Björk, E. Clinical study shows improved absorption of desmopressin with novel formulation. Pharm. Res. 2009, 26, 1618–1625. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, K.; Katsumata, H.; Yabuta, T.; Iwanaga, K.; Kakemi, M.; Tabata, Y.; Ikada, Y. Evaluation of gelatin microspheres for nasal and intramuscular administrations of salmon calcitonin. Eur. J. Pharm. Sci. 2001, 13, 179–185. [Google Scholar] [CrossRef]
- Hinchcliffe, M.; Jabbal-Gill, I.; Smith, A. Effect of chitosan on the intranasal absorption of salmon calcitonin in sheep. J. Pharm. Pharmacol. 2005, 57, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.C.; Park, M.O.; Na, D.H.; Youn, Y.S.; Lee, S.D.; Yoo, S.D.; Lee, H.S.; DeLuca, P.P. Intranasal delivery of pegylated salmon calcitonins: Hypocalcemic effects in rats. Calcif. Tissue Int. 2003, 73, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, F.; Katsura, M.; Tamai, I.; Tsuji, A. Improved nasal bioavailability of elcatonin by insoluble powder formulation. Int. J. Pharm. 2001, 224, 105–114. [Google Scholar] [CrossRef]
- Lee, W.A.; Ennis, R.D.; Longenecker, J.P.; Bengtsson, P. The bioavailability of intranasal salmon calcitonin in healthy volunteers with and without a permeation enhancer. Pharm. Res. 1994, 11, 747–750. [Google Scholar] [CrossRef] [PubMed]
- Pontiroli, A.E.; Pajetta, E; Calderara, A.; Alberetto, M.; Pozza, G.; Manganelli, V.; Resmini, G.; Tessari, L.; Maresca, V. Intranasal and intramuscular human calcitonin in female osteoporosis and in paget’s disease of bones: A pilot study. J. Endocrinol. Invest. 1991, 14, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, T.; Morita, T.; Horikiri, Y.; Yamahara, H.; Yoshino, H. Improved nasal absorption of salmon calcitonin by powdery formulation with N-acetyl-L-cysteine as a mucolytic agent. J. Control. Release 2006, 115, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, T.; Morita, T.; Horikiri, Y.; Yamahara, H.; Yoshino, H. Enhancement of nasal absorption of large molecular weight compounds by combination of mucolytic agent and nonionic surfactant. J. Control. Release 2006, 110, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Adjei, A.; Sundberg, D.; Miller, J.; Chun, A. Bioavailability of leuprolide acetate following nasal and inhalation delivery to rats and healthy humans. Pharm. Res. 1992, 9, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Abe, K.; Irie, T.; Uekama, K. Enhanced nasal delivery of luteinizing hormone releasing hormone agonist buserelin by oleic acid solubilized and stabilized in hydroxypropyl-beta–cyclodextrin. Chem. Pharm. Bull. 1995, 43, 2232–2237. [Google Scholar] [CrossRef] [PubMed]
- Illum, L.; Watts, P.; Fisher, A.N.; Jabbal Gill, I.; Davis, S.S. Novel chitosan-based delivery systems for the nasal administration of a LHRH-analogue. S.T.P. Pharma Sci. 2000, 10, 89–94. [Google Scholar]
- Illum, L.; Farraj, N.F.; Davis, S.S.; Johansen, B.R.; O’Hagan, D.T. Investigation of the nasal absorption of biosynthetic human growth hormone in sheep – use of a bioadhesive microsphere delivery system. Int. J. Pharm. 1990, 63, 207–211. [Google Scholar] [CrossRef]
- Laursen, T.; Grandjean, B.; Jorgensen, J.O.; Christiansen, J.S. Bioavailability and bioactivity of three different doses of nasal growth hormone (GH) administered to GH-deficient patients: Comparison with intravenous and subcutaneous administration. Eur. J. Endocrinol. 1996, 135, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Agerholm, C.; Bastholm, L.; Johansen, P.B.; Nielsen, M.H.; Elling, F. Epithelial transport and bioavailability of intranasally administered human growth hormone formulated with the absorption enhancers Didecanoyl-L-alpha-phosphatidylcholine and Alpha-cyclodextrin in rabbits. J. Pharm. Sci. 1994, 83, 1706–1711. [Google Scholar] [CrossRef] [PubMed]
- Hedin, L.; Olsson, B.; Diczfalusy, M.; Flyg, C.; Petersson, A.S.; Rosberg, S.; Albertsson-Wikland, K. Intranasal administration of human growth hormone (hGH) in combination with a membrane permeation enhancer in patients with GH deficiency: A pharmacokinetic study. J. Clinical Endocrinol. Metab. 1993, 76, 962–967. [Google Scholar]
- Leitner, V.M.; Guggi, D.; Krauland, A.H.; Bernkop-Schnürch, A. Nasal Delivery of human growth hormone: In vitro and in vivo evaluation of a thiomer/glutathione microparticulate delivery system. J. Control. Release 2004, 100, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Vancheri, C.; Mastruzzo, C.; Armato, F.; Tomaselli, V.; Magrì, S.; Pistorio, M.P.; LaMicela, M.; D’Amico, L.; Crimi, N. Intranasal heparin reduces eosinophil recruitment after nasal allergen challenge in patients with allergic rhinitis. J. Allergy Clin. Immunol. 2001, 108, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Zeng, D.; Prosperini, G.; Russo, C.; Spicuzza, L.; Cacciola, R.R.; Di Maria, G.U.; Polosa, R. Heparin attenuates symptoms and mast cell degranulation induced by AMP nasal provocation. J. Allergy Clin. Immunol. 2004, 114, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Yıldız, A.; Okyar, A.; Baktır, G.; Araman, A.; Ozsoy, Y. Nasal administration of heparin-loaded microspheres based on poly(lactic acid). Il Farmaco 2005, 60, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Arnold, J.; Ahsan, F.; Meezan, E.; Pillion, D.J. Nasal administration of low molecular weight heparin. J. Pharm. Sci. 2002, 91, 1707–1714. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Hussain, A.; Paulson, J.; Abbruscato, T.J.; Ahsan, F. Cyclodextrins in nasal delivery of low-molecular-weight heparins in vivo and in vitro studies. Pharm. Res. 2004, 21, 1127–1136. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, F.; Yang, T.; Khan, M.A.; Ahsan, F. Chain length-dependent effects of alkylmaltosides on nasal absorption of enoxaparin. J. Pharm. Sci. 2004, 93, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Mustafa, F.; Ahsan, F. Alkanoylsucroses in nasal delivery of low molecular weight heparins: In vivo absorption and reversibility studies in rats. J. Pharm. Pharmacol. 2004, 56, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Hussain, A.; Bai, S.; Khalil, I.A.; Harashima, H.; Ahsan, F. Positively charged polyethylenimines enhance nasal absorption of the negatively charged drug, low molecular weight heparin. J. Control. Release 2006, 115, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Jiang, H.L.; Zhu, K.J.; Liu, J.H.; Hao, Y.L. Preparation, characterization and nasal delivery of α-cobrotoxin-loaded poly(lactide-co-glycolide)/polyanhydride microspheres. J. Control. Release 2005, 108, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Gedulin, B.R.; Smith, P.A.; Jodka, C.M.; Chen, K.; Bhavsar, S.; Nielsen, L.L.; Parkes, D.G.; Young, A.A. Pharmacokinetics and pharmacodynamics of exenatide following alternate routes of administration. Int. J. Pharm. 2008, 356, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Teshima, D.; Yamauchi, A.; Makino, K.; Kataoka, Y.; Arita, Y.; Nawata, H.; Oishi, R. Nasal glucagon delivery using microcrystalline cellulose in healthy volunteers. Int. J. Pharm. 2002, 233, 61–66. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, Q.; Sun, Y.; Sun, J.; Wang, X.; Chen, M. Nasal recombinant hirudin-2 delivery: absorption and its mechanism in vivo and in vitro studies. Biol. Pharm. Bull. 2005, 28, 2263–2267. [Google Scholar] [CrossRef] [PubMed]
- Kissel, T.; Drewe, J.; Bantle, S.; Rummelt, A.; Beglinger, C. Tolerability and absorption enhancement of intranasally administered octreotide by sodium taurodihydrofusidate in healthy subjects. Pharm. Res. 1992, 9, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Oechslein, C.R.; Fricker, G.; Kissel, T. Nasal delivery of octreotide: absorption enhancement by particulate carrier systems. Int. J. Pharm. 1996, 139, 25–32. [Google Scholar] [CrossRef]
- Davis, S.S. Nasal vaccines. Adv. Drug. Deliv. Rev. 2001, 51, 21–42. [Google Scholar] [CrossRef]
- Gutierro, I.G.; Hernandez, R.M.; Igartua, M.; Gascon, A. R.; Pedraz, J. L. Influence of dose and immunization route on the serum IgG antibody response to BSA loaded PLGA microspheres. Vaccine 2002, 20, 2181–2190. [Google Scholar] [CrossRef]
- Olszewska, W.; Steward, M.W. Nasal delivery of epitope based vaccines. Adv. Drug Deliv. Rev. 2001, 51, 161–171. [Google Scholar] [CrossRef]
- Vyas, S.P.; Gupta, P.N. Implication of nanoparticles/microparticles in mucosal vaccine delivery. Expert Rev. Vaccines 2007, 6, 401–418. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Mukkur, T.K.S.; Benson, H.A.E.; Chen, Y. Pharmaceutical aspects of intranasal delivery of vaccines using particulate systems. J. Pharm. Sci. 2009, 98, 812–843. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Chakrapani, A.; O’Hagan, D. Nanoparticles and microparticles as vaccine-delivery systems. Expert Rev. Vaccines 2007, 6, 797–808. [Google Scholar] [CrossRef] [PubMed]
- Csaba, N.; Gargia-Fuentes, M.; Alonso, M.R. Nanoparticles for nasal vaccination. Adv. Drug. Del. Rev. 2009, 61, 140–157. [Google Scholar] [CrossRef] [PubMed]
- Alpar, H.O.; Özsoy, Y.; Bowen, J.; Eyles, J.E.; Conway, B.R.; Williamson, E.D. Potential of Particulate carriers for the mucosal delivery of dna vaccines. Biochem. Soc. Trans. 1997, 25, 337S. [Google Scholar] [CrossRef] [PubMed]
- Salomon, S.K.; Cevher, E.; Somavarapu, S.; Li, X.W.; Brocchini, S.; Sesardic, T.; Alpar, H.O. Novel N-Trimethyl Chitosan- Poly(γ-Glutamic Acid) Nanoparticles for Mucosal Delivery of Vaccines. 34th Annual Meeting & Exposition of the Controlled Release Society, Long Beach, CA, USA, 7–11 July 2007. [Google Scholar]
- Singh, J.; Pandit, S.; Bramwell, V.W.; Alpar, H.O. Diphtheria toxoid loaded poly-(epsilon-caprolactone) nanoparticles as mucosal vaccine delivery systems. Methods 2006, 38, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Illum, L.; Jabbal-Gill, I.; Hincgcliffe, M.; Fisher, A.N.; Davis, S.S. Chitosan as a novel delivery system for vaccines. Adv. Drug. Del. Rev. 2001, 51, 81–96. [Google Scholar] [CrossRef]
- Vila, A.; Sánchez, A.; Janes, K.; Behrens, I.; Kissel, T.; Vila Jato, J.L.; Alonso, M.J. Low molecular weight chitosan nanoparticles as new carriers for nasal vaccine delivery in mice. Eur. J. Pharm. Biopharm. 2004, 57, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Jung, T.; Kamm, W.; Breitenbach, A.; Hungerer, K.D.; Hundt, E.; Kissel, T. Tetanus toxoid loaded nanoparticles from sulfobutylated poly(vinyl alcohol)-graft-poly(lactide-co-glycolide): Evaluation of antibody response after oral and nasal application in mice. Pharm. Res. 2001, 18, 352–360. [Google Scholar] [CrossRef] [PubMed]
Sample availability: Not available. |









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drugs | Molecular weight (Da) | Formulation | Commercial name | Company | FDA approval date |
|---|---|---|---|---|---|
| Desmopressin acetate | 1183 | Solution, Spray | Minirin® | Sanofi-Aventis | 1978 |
| Salmon calcitonin | 3432 | Solution, Spray | Miacalcin® | Novartis | 1995 |
| Buserelin acetate* | 1239 | Solution, Spray | Suprefact® | Sanofi-Aventis | - |
| Nafarelin acetate | 1321 | Solution, Spray | Synarel® | Pfizer | 1990 |
| Oxytocin | 1007 | Solution, Spray | Syntocinon® | Novartis | 1995 |
| Cyanocobalamine | 1355 | Gel | Nascobal® | Par Pharm Co. | 1996 |
| Cyanocobalamine | 1355 | Solution, Spray | Nascobal® | Par Pharm Co. | 2005 |
| Polymers/Others | Delivery system | Enhancer | Animal model | Results | Ref. |
|---|---|---|---|---|---|
| Degradable starch | Microspheres | LFC | Sheep | While the relative bioavailability of insulin from microspheres was 10.7%, addition of enhancer to the formulation, bioavailability of insulin was increased to 31.5%. | [45] |
| Soluble starch | Powder and Microspheres | - | Rats | A comparison between microspheres and starch powders (mw 11000 and 25000) indicated that the insoluble starch of mw 25000 and the microspheres reduced the plasma glucose level to the same extent. Besides water soluble starch powder (mw 11000) did not change the plasma glucose level. | [46] |
| Crosslinked starch and Dextran | Microspheres | Epichlorohydrin | Rats | The effect on the glucose level of insulin from starch and dextran microspheres was rapid and maximum decrease in plasma glucose level was achieved in 30-40 minutes. The effect of starch microspheres was found more efficient than that of dextran microspheres to decrease blood glucose level. | [47] |
| Starch- Carbopol® 974P and maltodextrin -Carbopol® 974P | Freeze-dried powder | - | Rabbits | The nasal bioavailability achieved with the application of Starch-Carbopol® 974P powder was significantly higher than that of the maltodextrin-Carbopol® 974P mixtures. | [48] |
| Starch | Microspheres | Bile salt derivatives (LFC, GDC, STDF) | Sheep | Bioadhesive starch microspheres have improved transport of insulin across nasal membrane in the presence of absorption enhancers. Addition of enhancer to the microspheres has increased insulin absorption than that of absorption enhancer in solution. | [49] |
| Amioca® starch and Carbopol® 974P | Powder | - | Rabbits | Following nasal single-dose application of a physical mixture of Amioca® starch and Carbopol® 974P (9/1) the bioavailability of insulin has been found to be more than 10%. | [50] |
| Crosslinked starch | Nanoparticles | SGC, LFC | Rats | A rapid hypoglycemic effect has been observed with nasal application of nanoparticles. It has been emphasized that the release of insulin from nanoparticles can be modified by adjusting the degree of cross-linking. The release rate of insulin has significantly increased with combination of permeation enhancers and nanoparticles. | [52] |
| Dextran | Microspheres | - | Rats | Microspheres with insulin on the surface were more effective in promoting insulin absorption than those with insulin distributed within the dextran matrix. | [53] |
| Anionic resin (SPS), nonionic resins (PAE, SDBC) and cationic resin (CA) | Powder | - | Rabbits | Nasal administration of insulin mixed with anionic resin caused a rapid increase of the plasma insulin level, while nasal administration of insulin alone caused little increase. Nonionic resin (SDBC) showed similar enhancement in nasal insulin absorption in contrast, the other nonionic resin and cationic resin did not improve insülin absorption. | [54] |
| Hyaluronic acid ester | Microspheres | - | Sheep | Average relative bioavailability of insulin from microspheres was calculated as 11% when compared with insulin administered by subcutaneous route. | [55] |
| Chitosan | Nanoparticles | - | Rabbits | The freeze-dried formulation of insulin-loaded chitosan nanoparticles has led to a greater decrease in plasma glucose level when compared to the insulin chitosan solution. | [56] |
| Cross linked chitosan | Nanoparticles | - | Rats | Microspheres containing chitosan and ascorbyl palmitate caused a 67% reduction of blood glucose compared to intravenous route and absolute bioavailability of insulin was found as 44%. | [57] |
| Thiolated chitosan | Nanoparticles | - | Rats | Insulin-loaded thiolated chitosan microspheres let to more than 1.5-fold higher bioavailability and more than 7-fold higher pharmacological efficacy than unmodified chitosan microspheres. | [58] |
| Chitosan | Nanoparticles | CM-β-CD | - | The fast release of insulin from chitosan/CM-β-CD nanoparticles was observed (84-97% insulin within 15 min.). | [59] |
| Chitosan | Nanoparticles | - | Rats | Nanoparticles containing insulin have increased the pharmacodynamic activity of the drug. The synthesis of gold nanoparticles prepared by using chitosan has used a new method, and therefore, the surface properties of chitosan were improved for binding of biomolecules. | [60] |
| Chitosan | Nanoparticles | NAC | Rats | Nasal administration of chitosan-NAC nanoparticles increased the insulin absorption compare to unmodified chitosan nanoparticles and control insulin solution. | [61] |
| Chitosan | Nanoparticles | SBE-β-CD and CM-β-CD | Rabbits | The nanoparticles have reversibly increased the transepithel resistance of the cells and increased the membrane permeability in in-vitro cell culture studies. Nasal application of fluorescence-loaded nanoparticles to rats has proved their ability to pass through nasal mucosa. In conclusion, insulin-loaded nanoparticles have decreased the plasma glucose level (more than 35% reduction). | [62] |
| Aminated gelatin | Microspheres | - | Rats | Aminated gelatin microspheres have significantly increased the nasal absorption of insulin when administered in dry formulation but no significant hypoglycemic effect was observed when given as a suspension. | [63] |
| Type of heparin | Formulations | Penetration enhancers | Animal model / Human | Results | Ref. |
|---|---|---|---|---|---|
| UFH | Aqueous solution | - | Human | Heparin showed the protection with respect to nasal allergic challenge. | [84] |
| UFH | Aqueous solution | - | Human | Nasal heparin showed a protective role against AMP provocation by inhibition of mast cell activation. | [85] |
| UFH | Poly(L-lactic acid) microspheres | - | Rats | Nasal application of poly (L-lactic acid)-heparin microspheres had a relative bioavailability of 143% (vs nasal heparin solution). | [86] |
| UFH | Chitosan nanoparticles | carboxymethyl-β-cyclodextrin | - | Heparin was released slowly from chitosan/cyclodextrin nanoparticles (8.3-9.1% heparin within 8 h). | [59] |
| Enoxaparin Dalteparin UFH | Aqueous solution | Tetradecymaltoside | Rats | The addition of tetradecymaltoside into nose drops formulations containing LMWH has let to in a significant increase in the Cmax and AUC of anti-factor Xa activity compare to LMWH in saline. But the addition of tetradecymaltoside into formulations containing UFH has let to much smaller increase in the Cmax and AUC of anti factor Xa activity. | [87] |
| LMWH | Aqueous solution | Dimethyl-β-cyclodextrin | Rats | Dimethyl-β-cyclodextrin was found the most effective enhancer for the absorption of LMWH. | [88] |
| LMWH (Enoxaparin) | Aqueous solution | Alkylmaltosides | Rats | Alkylmaltosides improved the nasal absorption of LMWH without causing an irreversible damage in nasal mucosa. When the alkyl chains of maltosides were increased from 8 to 14 carbons, absolute and relative bioavailability of Enoxaparin were increased by two-fold. | [89] |
| LMWH (Enoxaparin) | Aqueous solution | Alkonoylsucroses | Rats | The enhancers increased the bioavailability of LMWH when compared to saline solution. The potency of these enhancers was dependent on their hydrophobic chain lengths. | [90] |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Ozsoy, Y.; Gungor, S.; Cevher, E. Nasal Delivery of High Molecular Weight Drugs. Molecules 2009, 14, 3754-3779. https://doi.org/10.3390/molecules14093754
Ozsoy Y, Gungor S, Cevher E. Nasal Delivery of High Molecular Weight Drugs. Molecules. 2009; 14(9):3754-3779. https://doi.org/10.3390/molecules14093754
Chicago/Turabian StyleOzsoy, Yıldız, Sevgi Gungor, and Erdal Cevher. 2009. "Nasal Delivery of High Molecular Weight Drugs" Molecules 14, no. 9: 3754-3779. https://doi.org/10.3390/molecules14093754
APA StyleOzsoy, Y., Gungor, S., & Cevher, E. (2009). Nasal Delivery of High Molecular Weight Drugs. Molecules, 14(9), 3754-3779. https://doi.org/10.3390/molecules14093754