
Dietary Polyphenols and Periodontitis—A Mini-Review of Literature



Abstract
:1. Introduction
2. Dietary Polyphenols: Link with Chronic Diseases and Periodontitis
3. Dietary Polyphenols and Periodontitis: Cellular Studies
4. Dietary Polyphenols and Periodontitis: Animal Studies
5. Dietary Polyphenols and Periodontitis: Human Clinical Studies
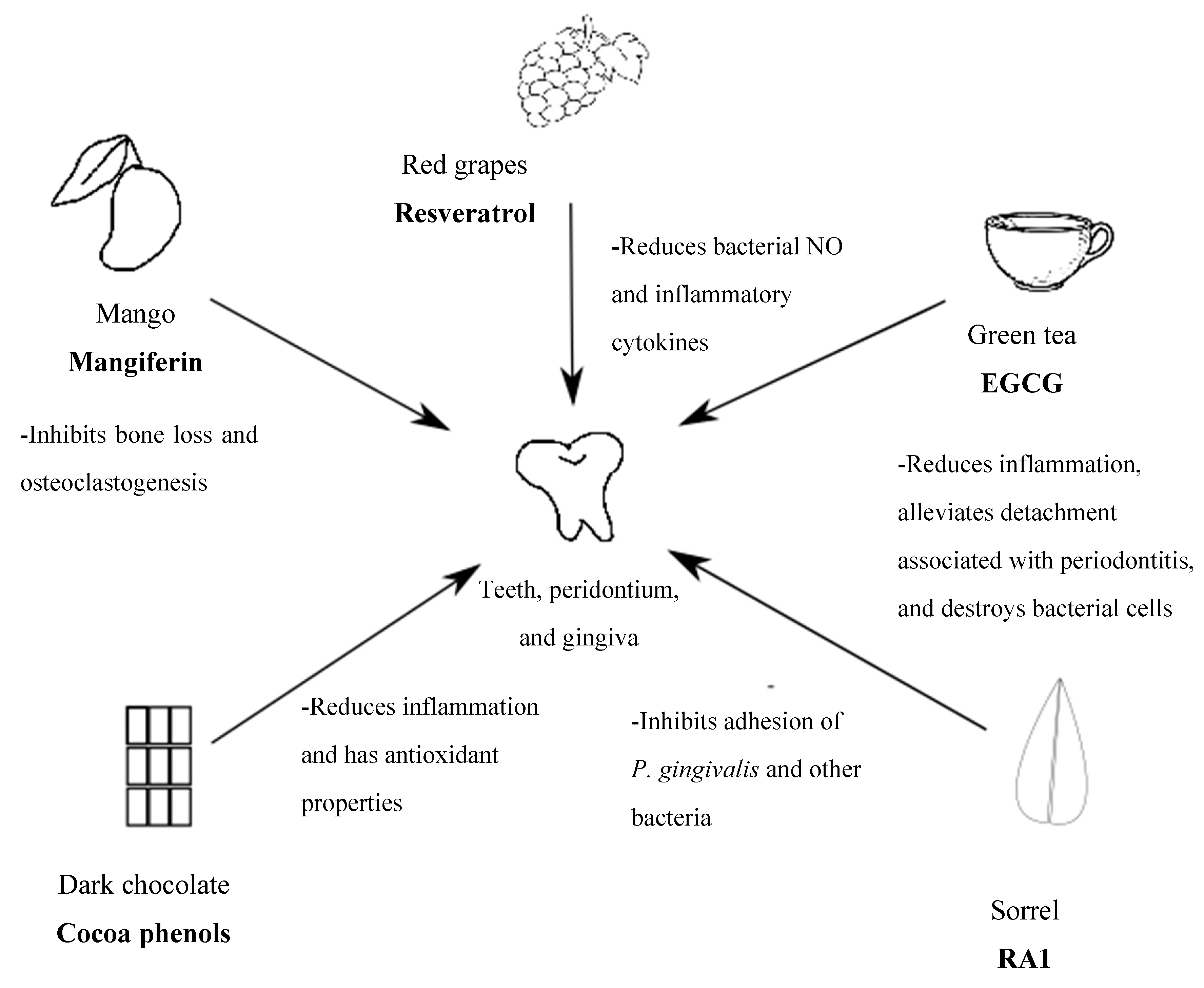
6. Food vs. Purified Polyphenols in Periodontitis
7. Conclusions and Recommendations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Eke, P.I.; Dye, B.A.; Wei, L.; Slade, G.D.; Thornton-Evans, G.O.; Borgnakke, W.S.; Taylor, G.W.; Page, R.C.; Beck, J.D.; Genco, R.J. Update on prevalence of periodontitis in adults in the United States: Nhanes 2009 to 2012. J. Periodontol. 2015, 86, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Page, R.C.; Eke, P.I. Case definitions for use in population-based surveillance of periodontitis. J. Periodontol. 2007, 78, 1387–1399. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabe, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of severe periodontitis in 1990-2010: A systematic review and meta-regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Zohaib, S.; Almas, K. The role of nutrition in periodontal health: An update. Nutrients 2016, 8, 530. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, L.L.; Fu, R.; Buckley, D.I.; Freeman, M.; Helfand, M. Periodontal disease and coronary heart disease incidence: A systematic review and meta-analysis. J. Gen. Intern. Med. 2008, 23, 2079–2086. [Google Scholar] [CrossRef] [PubMed]
- Spahr, A.; Klein, E.; Khuseyinova, N.; Boeckh, C.; Muche, R.; Kunze, M.; Rothenbacher, D.; Pezeshki, G.; Hoffmeister, A.; Koenig, W. Periodontal infections and coronary heart disease: Role of periodontal bacteria and importance of total pathogen burden in the coronary event and periodontal disease (corodont) study. Arch. Intern. Med. 2006, 166, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M.; Alba, A.L.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Leong, X.F.; Ng, C.Y.; Badiah, B.; Das, S. Association between hypertension and periodontitis: Possible mechanisms. Sci. World J. 2014, 2014, 768237. [Google Scholar] [CrossRef] [PubMed]
- Morozumi, T.; Yashima, A.; Gomi, K.; Ujiie, Y.; Izumi, Y.; Akizuki, T.; Mizutani, K.; Takamatsu, H.; Minabe, M.; Miyauchi, S.; et al. Increased systemic levels of inflammatory mediators following one-stage full-mouth scaling and root planing. J. Period. Res. 2018. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L.; Kirakodu, S.; Novak, M.J.; Stromberg, A.J.; Shen, S.; Orraca, L.; Gonzalez-Martinez, J.; Burgos, A.; Gonzalez, O.A. Cytokine gene expression profiles during initiation, progression and resolution of periodontitis. J. Clin. Periodontol. 2014, 41, 853–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanri, H.; Yamada, Y.; Itoi, A.; Yamagata, E.; Watanabe, Y.; Yoshida, T.; Miyake, M.; Date, H.; Ishikawa-Takata, K.; Yoshida, M.; et al. Frequency of fruit and vegetable consumption and the oral health-related quality of life among japanese elderly: A cross-sectional study from the kyoto-kameoka study. Nutrients 2017, 9, 1362. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.; Bouchard, P.; Cagetti, M.G.; Campus, G.; Carra, M.C.; Cocco, F.; Nibali, L.; Hujoel, P.; Laine, M.L.; Lingstrom, P.; et al. Interaction of lifestyle, behaviour or systemic diseases with dental caries and periodontal diseases: Consensus report of group 2 of the joint efp/orca workshop on the boundaries between caries and periodontal diseases. J. Clin. Periodontol. 2017, 44, S39–S51. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L. Potential mechanisms underpinning the nutritional modulation of periodontal inflammation. J. Am. Dent. Assoc. (1939) 2009, 140, 178–184. [Google Scholar] [CrossRef]
- Kondo, K.; Ishikado, A.; Morino, K.; Nishio, Y.; Ugi, S.; Kajiwara, S.; Kurihara, M.; Iwakawa, H.; Nakao, K.; Uesaki, S.; et al. A high-fiber, low-fat diet improves periodontal disease markers in high-risk subjects: A pilot study. Nutr. Res. (New York) 2014, 34, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Sakagami, H.; Tomomura, M. Dental application of natural products. Medicines (Basel) 2018, 5, 21. [Google Scholar] [CrossRef] [PubMed]
- Knaze, V.; Rothwell, J.A.; Zamora-Ros, R.; Moskal, A.; Kyro, C.; Jakszyn, P.; Skeie, G.; Weiderpass, E.; Santucci de Magistris, M.; Agnoli, C.; et al. A new food-composition database for 437 polyphenols in 19,899 raw and prepared foods used to estimate polyphenol intakes in adults from 10 European countries. Am. J. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Vetrani, C.; Vitale, M.; Bozzetto, L.; Della Pepa, G.; Cocozza, S.; Costabile, G.; Mangione, A.; Cipriano, P.; Annuzzi, G.; Rivellese, A.A. Association between different dietary polyphenol subclasses and the improvement in cardiometabolic risk factors: Evidence from a randomized controlled clinical trial. Acta Diabetol. 2018, 55, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, A.; Mukamal, K.J.; Liu, L.; Franz, M.; Eliassen, A.H.; Rimm, E.B. High anthocyanin intake is associated with a reduced risk of myocardial infarction in young and middle-aged women. Circulation 2013, 127, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Cassidy, A.; Schwarzschild, M.A.; Rimm, E.B.; Ascherio, A. Habitual intake of dietary flavonoids and risk of parkinson disease. Neurology 2012, 78, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Wedick, N.M.; Pan, A.; Cassidy, A.; Rimm, E.B.; Sampson, L.; Rosner, B.; Willett, W.; Hu, F.B.; Sun, Q.; van Dam, R.M. Dietary flavonoid intakes and risk of type 2 diabetes in us men and women. Am. J. Clin. Nutr. 2012, 95, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Zhu, W.; Jia, L.; Sun, X.; Chen, G.; Zhao, X.; Li, X.; Meng, X.; Kong, L.; Xing, L.; et al. Phase i study of topical epigallocatechin-3-gallate (EGCG) in patients with breast cancer receiving adjuvant radiotherapy. Br. J. Radiol. 2016, 89, 20150665. [Google Scholar] [CrossRef] [PubMed]
- Ryden, L.; Buhlin, K.; Ekstrand, E.; de Faire, U.; Gustafsson, A.; Holmer, J.; Kjellstrom, B.; Lindahl, B.; Norhammar, A.; Nygren, A.; et al. Periodontitis increases the risk of a first myocardial infarction: A report from the parokrank study. Circulation 2016, 133, 576–583. [Google Scholar] [PubMed]
- Chapple, I.L.; Genco, R. Diabetes and periodontal diseases: Consensus report of the joint efp/aap workshop on periodontitis and systemic diseases. J. Periodontol. 2013, 84, S106–S112. [Google Scholar] [CrossRef] [PubMed]
- Hirasawa, M.; Takada, K.; Makimura, M.; Otake, S. Improvement of periodontal status by green tea catechin using a local delivery system: A clinical pilot study. J. Period. Res. 2002, 37, 433–438. [Google Scholar] [CrossRef]
- Shahzad, M.; Millhouse, E.; Culshaw, S.; Edwards, C.A.; Ramage, G.; Combet, E. Selected dietary (poly)phenols inhibit periodontal pathogen growth and biofilm formation. Food Function 2015, 6, 719–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben Lagha, A.; Dudonne, S.; Desjardins, Y.; Grenier, D. Wild blueberry (vaccinium angustifolium ait.) polyphenols target fusobacterium nucleatum and the host inflammatory response: Potential innovative molecules for treating periodontal diseases. J. Agric. Food Chem. 2015, 63, 6999–7008. [Google Scholar] [CrossRef] [PubMed]
- Ben Lagha, A.; Haas, B.; Grenier, D. Tea polyphenols inhibit the growth and virulence properties of fusobacterium nucleatum. Sci. Rep. 2017, 7, 44815. [Google Scholar] [CrossRef] [PubMed]
- Schmuch, J.; Beckert, S.; Brandt, S.; Lohr, G.; Hermann, F.; Schmidt, T.J.; Beikler, T.; Hensel, A. Extract from rumex acetosa l. For prophylaxis of periodontitis: Inhibition of bacterial in vitro adhesion and of gingipains of porphyromonas gingivalis by epicatechin-3-O-(4beta-->8)-epicatechin-3-O-gallate (procyanidin-B2-Di-gallate). PLoS ONE 2015, 10, e0120130. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Caleare, A.; Hensel, A.; Mello, J.C.; Pinha, A.B.; Panizzon, G.P.; Lechtenberg, M.; Petereit, F.; Nakamura, C.V. Flavan-3-ols and proanthocyanidins from limonium brasiliense inhibit the adhesion of porphyromonas gingivalis to epithelial host cells by interaction with gingipains. Fitoterapia 2017, 118, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Lombardo Bedran, T.B.; Palomari Spolidorio, D.; Grenier, D. Green tea polyphenol epigallocatechin-3-gallate and cranberry proanthocyanidins act in synergy with cathelicidin (ll-37) to reduce the lps-induced inflammatory response in a three-dimensional co-culture model of gingival epithelial cells and fibroblasts. Arch. Oral Biol. 2015, 60, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Bevilacqua, N.; Guida, L.; Annunziata, M.; Romano Carratelli, C.; Paolillo, R. Effect of resveratrol and modulation of cytokine production on human periodontal ligament cells. Cytokine 2012, 60, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Chen, Z.; Liu, H.; Xuan, Y.; Wang, X.; Luan, Q. Green tea epigallocatechin-3-gallate alleviates porphyromonas gingivalis-induced periodontitis in mice. Int. Immunopharmacol. 2015, 29, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Correa, M.G.; Pires, P.R.; Ribeiro, F.V.; Pimentel, S.Z.; Casarin, R.C.; Cirano, F.R.; Tenenbaum, H.T.; Casati, M.Z. Systemic treatment with resveratrol and/or curcumin reduces the progression of experimental periodontitis in rats. J. Period. Res. 2017, 52, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Paterniti, I.; Briguglio, E.; Mazzon, E.; Galuppo, M.; Oteri, G.; Cordasco, G.; Cuzzocrea, S. Effects of hypericum perforatum, in a rodent model of periodontitis. BMC Complement. Altern. Med. 2010, 10, 73. [Google Scholar] [CrossRef] [PubMed]
- Yoshinaga, Y.; Ukai, T.; Nakatsu, S.; Kuramoto, A.; Nagano, F.; Yoshinaga, M.; Montenegro, J.L.; Shiraishi, C.; Hara, Y. Green tea extract inhibits the onset of periodontal destruction in rat experimental periodontitis. J. Period. Res. 2014, 49, 652–659. [Google Scholar] [CrossRef]
- Huang, J.; Wu, C.; Tian, B.; Zhou, X.; Ma, N.; Qian, Y. Myricetin prevents alveolar bone loss in an experimental ovariectomized mouse model of periodontitis. Int. J. Mol. Sci. 2016, 17, 422. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wang, Q.; Ding, Y.; Bao, C.; Li, W. Mangiferin ameliorates porphyromonas gingivalis-induced experimental periodontitis by inhibiting phosphorylation of nuclear factor-kappab and janus kinase 1-signal transducer and activator of transcription signaling pathways. J. Period. Res. 2017, 52, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Erlund, I.; Marniemi, J.; Hakala, P.; Alfthan, G.; Meririnne, E.; Aro, A. Consumption of black currants, lingonberries and bilberries increases serum quercetin concentrations. Eur. J. Clin. Nutr. 2003, 57, 37–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, A.L.; Hsu, C.H.; Lin, J.K.; Hsu, M.M.; Ho, Y.F.; Shen, T.S.; Ko, J.Y.; Lin, J.T.; Lin, B.R.; Ming-Shiang, W.; et al. Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-risk or pre-malignant lesions. Anticancer Res. 2001, 21, 2895–2900. [Google Scholar] [PubMed]
- Hujoel, P.P.; Lingstrom, P. Nutrition, dental caries and periodontal disease: A narrative review. J. Clin. Periodontol. 2017, 44, S79–S84. [Google Scholar] [CrossRef] [PubMed]
- Lula, E.C.; Ribeiro, C.C.; Hugo, F.N.; Alves, C.M.; Silva, A.A. Added sugars and periodontal disease in young adults: An analysis of nhanes III data. Am. J. Clin. Nutr. 2014, 100, 1182–1187. [Google Scholar] [CrossRef] [PubMed]
- Kote, S.; Kote, S.; Nagesh, L. Effect of pomegranate juice on dental plaque microorganisms (streptococci and lactobacilli). Anc. Sci. Life 2011, 31, 49–51. [Google Scholar] [PubMed]
- Bhatia, M.; Urolagin, S.S.; Pentyala, K.B.; Urolagin, S.B.; K, B.M.; Bhoi, S. Novel therapeutic approach for the treatment of periodontitis by curcumin. J. Clin. Diagn. Res. 2014, 8, ZC65–ZC69. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.; Milward, M.R.; Ling-Mountford, N.; Weston, P.; Carter, K.; Askey, K.; Dallal, G.E.; De Spirt, S.; Sies, H.; Patel, D.; et al. Adjunctive daily supplementation with encapsulated fruit, vegetable and berry juice powder concentrates and clinical periodontal outcomes: A double-blind rct. J. Clin. Periodontol. 2012, 39, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.; Tewari, S.; Sharma, R.K.; Singh, G.; Yadav, A.; Naula, S.C. Effect of subgingivally delivered 10% emblica officinalis gel as an adjunct to scaling and root planing in the treatment of chronic periodontitis—A randomized placebo-controlled clinical trial. Phytother. Res. 2016, 30, 956–962. [Google Scholar] [CrossRef] [PubMed]
- Chava, V.K.; Vedula, B.D. Thermo-reversible green tea catechin gel for local application in chronic periodontitis: A 4-week clinical trial. J. Periodontol. 2013, 84, 1290–1296. [Google Scholar] [CrossRef] [PubMed]
- Hrishi, T.S.; Kundapur, P.P.; Naha, A.; Thomas, B.S.; Kamath, S.; Bhat, G.S. Effect of adjunctive use of green tea dentifrice in periodontitis patients—A randomized controlled pilot study. Int. J. Dent. Hyg. 2016, 14, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Roodgaryan, R.; Jenabian, N.; Moghadamnia, A.A.; Pouramir, M.; Khadir, F. Clinical and biochemical effects of dark chocolate in moderate chronic periodontitis. Casp. J. Dent. Res. 2015, 4, 43–49. [Google Scholar]
- Tipton, D.A.; Hatten, A.A.; Babu, J.P.; Dabbous, M. Effect of glycated albumin and cranberry components on interleukin-6 and matrix metalloproteinase-3 production by human gingival fibroblasts. J. Period. Res. 2016, 51, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Lucas, E.A. Mechanisms and effects of green tea on cardiovascular health. Nutr. Rev. 2007, 65, 361–375. [Google Scholar] [CrossRef] [PubMed]
- Michalska, A.; Lysiak, G. Bioactive compounds of blueberries: Post-harvest factors influencing the nutritional value of products. Int. J. Mol. Sci. 2015, 16, 18642–18663. [Google Scholar] [CrossRef] [PubMed]
- Feghali, K.; Feldman, M.; La, V.D.; Santos, J.; Grenier, D. Cranberry proanthocyanidins: Natural weapons against periodontal diseases. J. Agric. Food Chem. 2012, 60, 5728–5735. [Google Scholar] [CrossRef] [PubMed]
- Yamakoshi, J.; Saito, M.; Kataoka, S.; Kikuchi, M. Safety evaluation of proanthocyanidin-rich extract from grape seeds. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2002, 40, 599–607. [Google Scholar] [CrossRef]
- Seeram, N.P.; Aviram, M.; Zhang, Y.; Henning, S.M.; Feng, L.; Dreher, M.; Heber, D. Comparison of antioxidant potency of commonly consumed polyphenol-rich beverages in the united states. J. Agric. Food Chem. 2008, 56, 1415–1422. [Google Scholar] [CrossRef] [PubMed]
- Hatipoglu, M.; Saglam, M.; Koseoglu, S.; Koksal, E.; Keles, A.; Esen, H.H. The effectiveness of crataegus orientalis m bieber. (hawthorn) extract administration in preventing alveolar bone loss in rats with experimental periodontitis. PLoS ONE 2015, 10, e0128134. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study Design and Model | Polyphenol | Significant Findings | Author, Year |
|---|---|---|---|
| HPLC culture stimulated with LPS of P. gingivalis | Resveratrol (25, 50, and 100 µM) |  NO expression by P. gingivalis in a dose-dependent and time-dependent manner NO expression by P. gingivalis in a dose-dependent and time-dependent manner | Rizzo et al., 2012 [32] |
| F. nucleatum cultures in Todd-Hewitt broth | 70% ethanolic blueberry extract of varying concentrations (500, 250, 125, 62.5, 31.25, 15.62, and 7.9 μg/mL) |  growth of F. nucleatum and biofilm formation growth of F. nucleatum and biofilm formation | Ben Lagha et al., 2015 [27] |
| Human gingival epithelial cells grown in keratinocyte medium | EGCG (1 and 5 mg/mL) & AC-PCs (25 and 50 mg/mL) |  release of several inflammatory cytokines release of several inflammatory cytokines | Lombardo et al., 2015 [29] |
| P. gingivalis culture in sheep blood agar | RA1 (1–100 μg/mL) containing flavan-3-ols, flavonoids, and oligomeric proantho cyanidins |  adhesion of P. gingivalis to human KB cells due to the specific activity of galloylated oligomeric proanthocyanidins, inhibited gingipain activity, and inhibited P. gingivalis-induced hem agglutination adhesion of P. gingivalis to human KB cells due to the specific activity of galloylated oligomeric proanthocyanidins, inhibited gingipain activity, and inhibited P. gingivalis-induced hem agglutination | Schmuch et al., 2015 [30] |
| Bacterial cultures of S. mitis, A actinomycetemcomitans, P. gingivalis, and F. nucleatum | Phenols and polyphenols from different classes including hydroxyl acids, flavanols, flavanones, anthocyanins, and phenolics (0.24–2500 μg/mL, depending on the compound) |  planktonic growth, mostly by curcumin which was followed by pyrogallol, pyrocatechol, and quercetin planktonic growth, mostly by curcumin which was followed by pyrogallol, pyrocatechol, and quercetin | Shahzad et al., 2015 [26] |
| Normal human fibroblasts incubated with HSA, G-HSA, or P. gingivalis LPS | Cranberry high molecular weight NDM (10–50 μg/mL with HSA or G-HSA alone; 50 or 100 μg/mL with HSA, G-HSA, and LPS) |  production of IL-6 and MMP-3 production of IL-6 and MMP-3 | Tipton et al., 2016 [50] |
| P. gingivalis strain cultivated in agar medium and broth | L. brasiliense extract in water/acetone solution (50–500 μg/mL) |  adhesion of P. gingivalis to human KB cells and the activity of Arg-gingipain adhesion of P. gingivalis to human KB cells and the activity of Arg-gingipain | De Oliveira et al., 2017 [31] |
| F. nucleatum in Todd-Hewitt broth | Green tea (20 mg), black tea (10 mg), and theaflavins (20 mg) in solution |  biofilm formation biofilm formation | Ben Lagha et al., 2017 [28] |
| Study Design and Model | Polyphenol | Significant Findings | Author, Year |
|---|---|---|---|
| Adult male Sprague-Dawley rats | Hypericum perforatum extract (2 mg/kg/day) administered orally |  gingivomucosal tissue injury, alveolar bone loss, & expression of NF-κB p65 gingivomucosal tissue injury, alveolar bone loss, & expression of NF-κB p65 | Paterniti et al., 2010 [35] |
| E. coli-induced periodontitis in Lewis rats | Sunphenon BG blend (91.3% polyphenols) administered topically to affected periodontal areas |  periodontal detachment and bone resorption periodontal detachment and bone resorption | Yoshinaga et al., 2014 [36] |
| P. gingivalis induced periodontitis in BALB/c mice | EGCG (0.02%) or vehicle (distilled water) in drinking water |  inflammation e.g., IL-17, IL-1β vs. vehicle inflammation e.g., IL-17, IL-1β vs. vehicle | Cai et al., 2015 [33] |
| Ligation-induced periodontitis in Wistar rats | Hawthorn (Crataeus orientalis M Bieber) extract (100 mg/kg) vs saline administered orogastrically |  osteoclast activity and subsequently ameliorated alveolar bone loss induced by periodontitis osteoclast activity and subsequently ameliorated alveolar bone loss induced by periodontitis | Hatipoğlu et al., 2015 [55] |
| C57BL/J6 ovariectomized female mice | Low or high dose (2 or 5 mg/kg/day) of myricetin, which is a polyphenol derived from fruits and vegetables, administered intraperitoneally vs. placebo |  alveolar bone loss by inhibiting osteoclastogenesis induced by periodontitis alveolar bone loss by inhibiting osteoclastogenesis induced by periodontitis | Huang et al., 2016 [37] |
| Wistar rats | Curcumin (100 mg/kg), resveratrol (10 mg/kg), curcumin + resveratrol or resveratrol alone administered orogastrically |  gingival IL-1β in curcumin+resveratrol gingival IL-1β in curcumin+resveratrol | Corrêa et al., 2017 [34] |
| P. gingivalis induced periodontitis in male C57BL/6J wild-type mice | Mangiferin (50 mg/kg) oral application |  TNF-α production, phosphorylation in the NF-κB and JK-1 signal pathways, and alveolar bone loss TNF-α production, phosphorylation in the NF-κB and JK-1 signal pathways, and alveolar bone loss | Li et al., 2017 [38] |
| Study Design and Model | Polyphenol | Significant Findings | Author, Year |
|---|---|---|---|
| Pre-post intervention, healthy volunteers (n = 30; age 25–30 years) | Pomegranate juice (30 mL) mouth rinse for 2 min |  CFUs of both Streptococci and Lactobacillus spp. CFUs of both Streptococci and Lactobacillus spp. | Kote et al., 2011 [43] |
| Crossover RCT, patients with chronic periodontitis (n = 60, age 30–60 years) | Daily oral intake of 6 FV capsules, 6 FVB capsules, or placebo capsules for 2 months |  PPD in FV compared with placebo PPD in FV compared with placebo | Chapple et al., 2012 [45] |
| Patients with chronic periodontitis (n = 30; age 38.9–10.67 years) | Sustained-release green tea extract gel (1%) containing ECGC administered once |  GI, PD, and rCAL GI, PD, and rCAL | Chava & Vedula, 2013 [47] |
| Patients with chronic periodontitis (n = 25; age 21–45 years) | 1% curcumin gel inserted into periodontal pockets with blunt syringe at intervals of 1, 3, and 6 months following the start of the study |  Bacterial counts of P. gingivalis, P. intermedia, F. nucleatum, and Capnocytophaga spp. Bacterial counts of P. gingivalis, P. intermedia, F. nucleatum, and Capnocytophaga spp. | Bhatia et al., 2014 [44] |
| Crossover RCT; patients with moderate chronic periodontitis (n = 40, age 30–50 years) | Oral intake 3 times a day for 4 weeks of 30 g dark chocolate with 78% cacao (containing flavonoids such as catechin and procyanidins) or white chocolate placebo w/o cacao |  MPBI and lipid peroxidation MPBI and lipid peroxidation | Roodgaryan et al., 2015 [49] |
| Patients treated with root planning and scaling (n = 40, age ≥ 30 years) | 10% E. officinalis extract gel administered subgingivally once and parameters measured 2 and 3 months post-treatment |  Inflammation, mSBI and PPD Inflammation, mSBI and PPD | Grover et al., 2016 [46] |
| Patients with mild to moderate periodontitis (n = 30, age 18–60 years) | Green tea extract dentifrice with 60–90% EGCG or placebo dentifrice with fluoride and triclosan, brushed onto teeth for 2–5 min daily for 4 weeks |  gingival inflammation gingival inflammation | Hrishi et al., 2016 [48] |
| Polyphenol | Mechanisms of Action |
|---|---|
| Resveratrol | Reduces NO expression by P. gingivalis bacteria by inhibiting inflammatory cytokines and improving viability of affected HPLCs [32] |
| Blueberry flavonoids, phenolic acids, and procyanidins e.g., chlorogenic acid, ellagic acid, quercetin, anthocyanins, and proanthocyanidins | Reduce bacterial growth and biofilm formation via antibacterial, inhibitory effects against Gram-negative bacteria such as F. nucleatum [26,27,30] |
| EGCG | Inhibits release of inflammatory cytokines (IL-17, IL-1β) by modulating gene expression pathways (e.g., NF-κB), and decreasing inflammation/oxidation by increasing the activity of GST [33,48] |
| RA1 | Inhibit adhesion of bacteria through a specific activity of galloylated oligomeric proanthocyanidins [30] |
| Curcumin | Inhibits planktonic growth by decreasing metabolic activity of bacterial species [44] |
| Curcumin + Resveratrol | Reduces gingival IL-1β and inhibits NF-κB, which lowers proteasome activity and resulting cell damage and inflammation [34] |
| Pyrogallol | Inhibits planktonic growth by reducing biomass of planktonic films [26] |
| Pyrocatechol | Inhibits planktonic growth by reducing biomass of planktonic films [26] |
| Quercetin | Inhibits planktonic growth by reducing biomass of planktonic films [26] |
| Cranberry flavonoids and proanthocyanidins | Inhibit IL-6 production and MMP-3 by suppressing the NF-κB and MAPK/AP-1 signaling pathways [50] |
| L. brasiliense flavan-3-ols and proanthocyanidins | Reduce adhesion of P. gingivalis to human KB cells by inhibiting Arg-gingipain activity [30,31] |
| Tea polyphenols e.g., theaflavins | Inhibit biofilm formation and adhesion of pathogens to the oral mucosa likely by binding to receptors in the bacterial cell wall [27,28] |
| Hypericum perforatum flavonoids and phenolic acids | Inhibits inflammatory cytokine production by suppressing NF-κB p65 pathway and reducing NO expression by pathogenic bacteria through the suppression of the iNOS system [35] |
| Myricetin | Reduces alveolar bone loss by inhibiting osteoclastogenesis [37] |
| Mangiferin | Suppresses TNF-alpha production and inhibits phosphorylation of NF-κB and JK-1 pathways, which inhibits production of inflammatory cytokines and alleviates tissue injury [38] |
| Pomegranate phenolic compounds | Reduces number of pathogenic Streptococci and Lactobacilli pathogens and inhibits the formation of colony units [43] |
| Cacao flavonoids | Decrease lipid peroxidation and improve gingival bleeding [49] |
| E. officinalis flavonoids, phenols, and tannins | May reduce inflammation by suppressing the action of histamine, serotonin, prostaglandins, and other inflammatory mediators [46] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basu, A.; Masek, E.; Ebersole, J.L. Dietary Polyphenols and Periodontitis—A Mini-Review of Literature. Molecules 2018, 23, 1786. https://doi.org/10.3390/molecules23071786
Basu A, Masek E, Ebersole JL. Dietary Polyphenols and Periodontitis—A Mini-Review of Literature. Molecules. 2018; 23(7):1786. https://doi.org/10.3390/molecules23071786
Chicago/Turabian StyleBasu, Arpita, Emily Masek, and Jeffrey L. Ebersole. 2018. "Dietary Polyphenols and Periodontitis—A Mini-Review of Literature" Molecules 23, no. 7: 1786. https://doi.org/10.3390/molecules23071786
APA StyleBasu, A., Masek, E., & Ebersole, J. L. (2018). Dietary Polyphenols and Periodontitis—A Mini-Review of Literature. Molecules, 23(7), 1786. https://doi.org/10.3390/molecules23071786