
Antimicrobial O-Alkyl Derivatives of Naringenin and Their Oximes Against Multidrug-Resistant Bacteria

 ,
,  ,
,
Abstract
:1. Introduction
2. Results and Discussion
2.1. Chemistry
2.2. Antimicrobial Studies
3. Materials and Methods
3.1. Strains and Culture Conditions
3.2. Antimicrobial Agents
3.3. Chemistry
3.3.1. Chemicals
3.3.2. Analysis
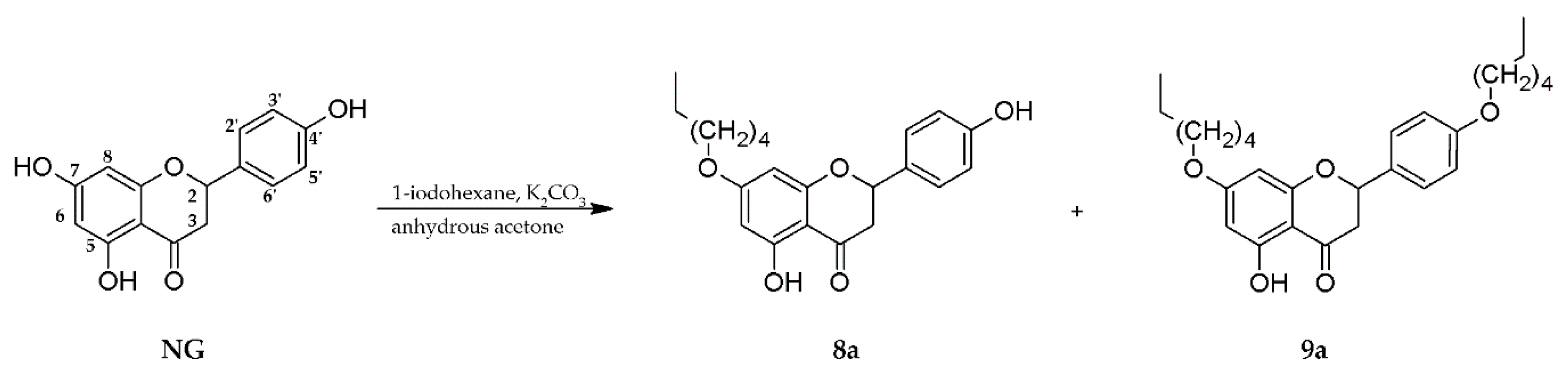
3.3.3. Synthesis of 7-O-hexylnaringenin (8a) and 7,4′-di-O-hexylnaringenin (9a)
3.3.4. Synthesis of Oximes (8b, 9b)
3.4. Susceptibility Testing
3.5. Checkerboard Assay
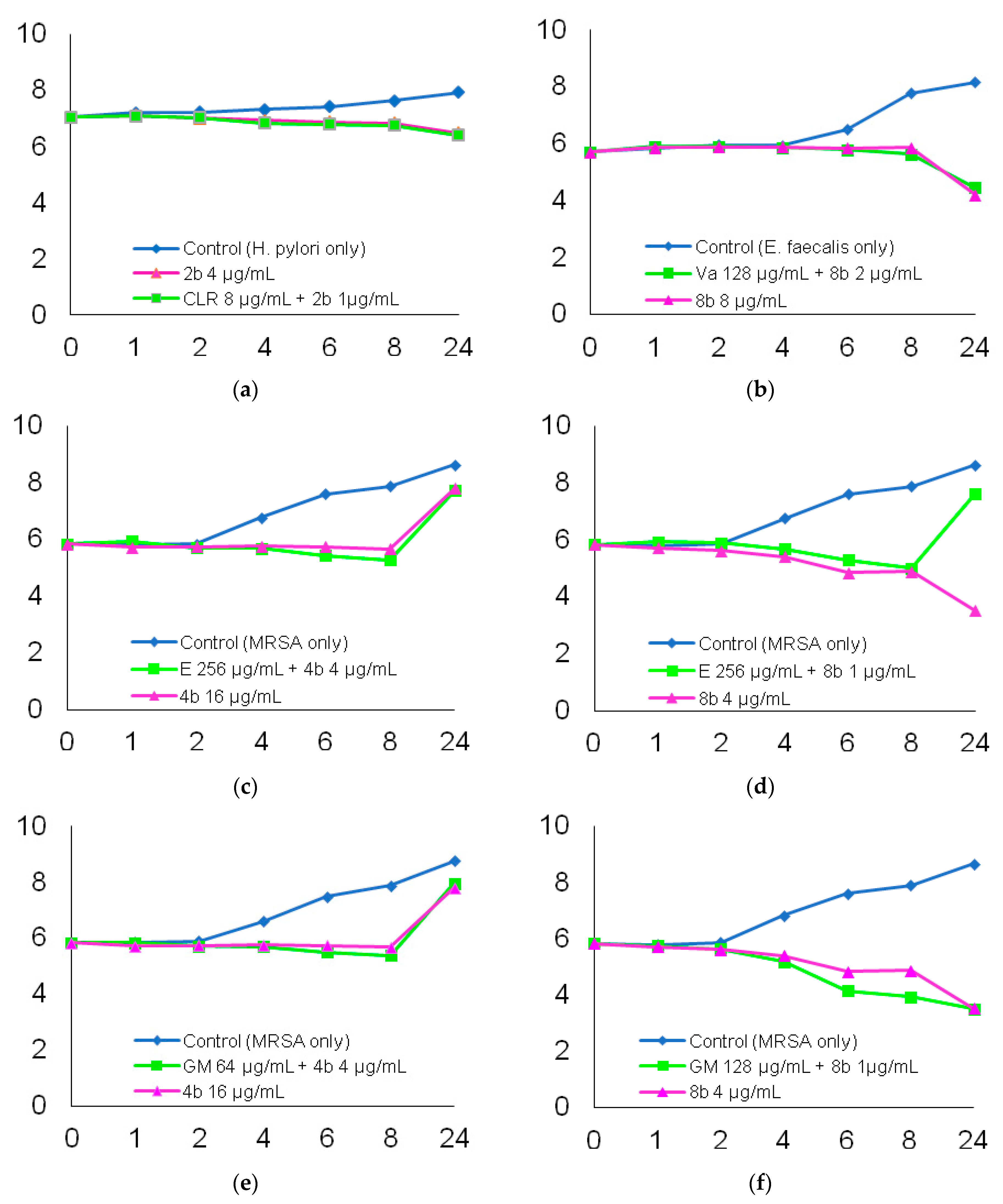
3.6. Time-Kill Analysis
- (a)
- for S. aureus: the gentamicin (64 µg/mL) + compound 4b (4 µg/mL) combination, as well as the gentamicin (128 µg/mL) + compound 8b (1 µg/mL) combination and the erythromycin (256 µg/mL) + compound 4b (4 µg/mL), the erythromycin (256 µg/mL) + compound 8b (1 µg/mL) combination;
- (b)
- for E. faecalis: the vancomycin (128 µg/mL) + compound 8b (2 µg/mL) combination;
- (c)
- for H. pylori: the clarithromycin (8 µg/mL) + compound 2b (1 µg/mL) combination.
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Weiner, L.M.; Webb, A.K.; Limbago, B.; Dudeck, M.A.; Patel, J.; Kallen, A.J.; Edwards, J.R.; Sievert, D.M. Antimicrobial—Resistant Pathogens Associated with Healthcare—Associated Infections: Summary of Data Reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2011–2014. Infect. Control Hosp. Epidemiol. 2016, 37, 1288–1301. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Zhu, Y.; Lu, N.H.; Shi, Q. Recent progress in Helicobacter pylori treatment. Chin. Med. J. 2020, 133, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.J.; Cheng, A.C.; Kennon, J.; Spelman, D.; Hale, D.; Melican, G.; Sidjabat, H.E.; Paterson, D.L.; Kong, D.C.M.; Peleg, A.Y. Prevalence of multidrug-resistant organisms and risk factors for carriage in long-term care facilities: A nested case-control study. J. Antimicrob. Chemother. 2014, 69, 1972–1980. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.E.; Kralovic, S.M.; Simbartl, L.A.; Freyberg, R.W.; Obrosky, D.S.; Roselle, G.A.; Jain, R. Nationwide reduction of health care-associated methicillin-resistant Staphylococcus aureus infections in Veterans Affairs long-term care facilities. Am. J. Infect. Control 2014, 42, 60–62. [Google Scholar] [CrossRef] [PubMed]
- Koulenti, D.; Myrianthefs, P.; Dimopoulos, G.; Baltopoulos, G. Neumonía nosocomial causada por Staphylococcus aureus resistente a meticilina. Enferm. Infecc. Microbiol. Clin. 2005, 23, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Lesher, B.; Gao, X.; Chen, Y.; Liu, Z. Methicillin-resistant Staphylococcus aureus nosocomial pneumonia: Role of linezolid in the People’s Republic of China. Clin. Outcomes Res. 2016, 8, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Kavanagh, K.T.; Abusalem, S.; Calderon, L.E. View point: Gaps in the current guidelines for the prevention of Methicillin-resistant Staphylococcus aureus surgical site infections. Antimicrob. Resist. Infect. Control 2018, 7, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Cooke, F.J.; Brown, N.M. Community-associated methicillin-resistant Staphylococcus aureus infections. Br. Med. Bull. 2010, 94, 215–227. [Google Scholar] [CrossRef] [Green Version]
- Siddiqui, A.H.; Koirala, J. Methicillin Resistant Staphylococcus aureus. Available online: https://europepmc.org/article/med/29489200#free-full-text (accessed on 1 March 2018).
- Lebreton, F.; Valentino, M.D.; Schaufler, K.; Earl, A.M.; Cattoir, V.; Gilmore, M.S. Transferable vancomycin resistance in clade B commensal-type Enterococcus faecium. J. Antimicrob. Chemother. 2018, 73, 1479–1486. [Google Scholar] [CrossRef]
- Peleg, A.Y.; Hooper, D.C. Hospital-acquired infections due to Gram-negative bacteria. N. Engl. J. Med. 2019, 13, 1804–1813. [Google Scholar] [CrossRef]
- Clegg, S.; Murphy, C.N. Epidemiology and Virulence of Klebsiella pneumoniae. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, R.L.; Da Silva, B.C.M.; Rezende, G.S.; Nakamura-Silva, R.; Pitondo-Silva, A.; Campanini, E.B.; Brito, M.C.A.; Da Silva, E.M.L.; De Melo Freire, C.C.; Da Cunha, A.F.; et al. High prevalence of multidrug-resistant Klebsiella pneumoniae harboring several virulence and β-lactamase encoding genes in a brazilian intensive care unit. Front. Microbiol. 2019, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstein, R.A.; Gaynes, R.; Edwards, J.R. Overview of Nosocomial Infections Caused by Gram—Negative Bacilli. Clin. Infect. Dis. 2005, 41, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.; Gosbell, I.B.; Boyle, M.J.; Ferguson, J.K. Cure of multiresistant Acinetobacter baumannii central nervous system infections with intraventricular or intrathecal colistin: Case series and literature review. J. Antimicrob. Chemother. 2006, 58, 1078–1081. [Google Scholar] [CrossRef] [Green Version]
- Garnacho-montero, J.; Gutiérrez-pizarraya, A.; Díaz-martín, A.; Cisneros-herreros, J.M.; Eugenia, M.; Gato, E.; Ruiz, C.; Alegría, D.; Fernández-cuenca, F.; Vila, J.; et al. Epidemiology, Clinical Features and Predictors of Mortality. Enferm. Infecc. Microbiol. Clini. 2016, 34, 5–12. [Google Scholar]
- Zilberberg, M.D.; Nathanson, B.H.; Sulham, K.; Fan, W.; Shorr, A.F. Multidrug resistance, inappropriate empiric therapy, and hospital mortality in Acinetobacter baumannii pneumonia and sepsis. Crit. Care 2016, 20, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Chopra, T.; Marchaim, D.; Awali, R.A.; Krishna, A.; Johnson, P.; Tansek, R.; Chaudary, K.; Lephart, P.; Slim, J.; Hothi, J.; et al. Epidemiology of bloodstream infections caused by Acinetobacter baumannii and impact of drug resistance to both carbapenems and ampicillin-sulbactam on clinical outcomes. Antimicrob. Agents Chemother. 2013, 57, 6270–6275. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; He, L.; Tao, X.; Meng, F.; Zhang, J. Biofilm may not be Necessary for the Epidemic Spread of Acinetobacter baumannii. Sci. Rep. 2016, 6, 1–8. [Google Scholar] [CrossRef]
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.Y.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta—Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [Green Version]
- Dunne, C.; Dolan, B.; Clyne, M. Factors that mediate colonization of the human stomach by Helicobacter pylori. World J. Gastroenterol. 2014, 20, 5610–5624. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence consensus report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ailloud, F.; Didelot, X.; Woltemate, S.; Pfaffinger, G.; Overmann, J.; Bader, R.C.; Schulz, C.; Malfertheiner, P.; Suerbaum, S. Within-host evolution of Helicobacter pylori shaped by niche-specific adaptation, intragastric migrations and selective sweeps. Nat. Commun. 2019, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nkuize, M.; De Wit, S.; Muls, V.; Delforge, M.; Deyi, V.Y.M.; Cadière, G.B.; Buset, M. HIV—Helicobacter pylori Co-Infection: Antibiotic Resistance, Prevalence, and Risk Factors. PLoS ONE 2015, 10, e0145119. [Google Scholar] [CrossRef] [PubMed]
- Kodama, O.; Miyakawa, J.; Akatsuka, T.; Kiyosawa, S. Sakuranetin, a flavanone phytoalexin from ultraviolet-irradiated rice leaves. Phytochemistry 1992, 31, 3807–3809. [Google Scholar] [CrossRef]
- Silva, S.A.S.; Agra, M.D.; Tavares, J.F.; Da-Cunha, E.V.L.; Barbosa-Filho, J.M.; Silva, M.S. Flavanones from aerial parts of Cordia globosa (Jacq.) Kunth, Boraginaceae. Brazilian J. Pharmacogn. 2010, 20, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Potaniec, B.; Grabarczyk, M.; Stompor, M.; Szumny, A.; Zieliński, P.; Zołnierczyk, A.K.; Anioł, M. Antioxidant activity and spectroscopic data of isoxanthohomol oxime and related compounds. Spectrochim. Acta-Part. A Mol. Biomol. Spectrosc. 2014, 118, 716–723. [Google Scholar] [CrossRef]
- Woo, Y.; Shin, S.Y.; Hyun, J.; Lee, S.D.; Lee, Y.H.; Lim, Y. Flavanones inhibit the clonogenicity of HCT116 cololectal cancer cells. Int. J. Mol. Med. 2012, 29, 403–408. [Google Scholar] [CrossRef] [Green Version]
- Céliz, G.; Daz, M.; Audisio, M.C. Antibacterial activity of naringin derivatives against pathogenic strains. J. Appl. Microbiol. 2011, 111, 731–738. [Google Scholar] [CrossRef] [Green Version]
- Kozłowska, J.; Potaniec, B.; Zarowska, B.; Anioł, M. Synthesis and biological activity of novel O-alkyl derivatives of naringenin and their oximes. Molecules 2017, 22, 1485. [Google Scholar] [CrossRef] [Green Version]
- Cory, H.; Passarelli, S.; Szeto, J.; Tamez, M.; Mattei, J. The Role of Polyphenols in Human Health and Food Systems: A Mini-Review. Front. Nutr. 2018, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kozłowska, J.; Grela, E.; Baczynska, D.; Grabowiecka, A.; Anioł, M. Novel O-alkyl derivatives of naringenin and their oximes with antimicrobial and anticancer activity. Molecules 2019, 24, 679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ISO 20776-1: 2006, Clinical Laboratory Testing and In Vitro Diagnostic Test Systems-susceptibility Testing of Infectious Agents and Evaluation of Performance of Antimicrobial Susceptibility Test Devices-part 1: Reference Method for Testing the in Vitro Activity of Antimicrobial Agents against Rapidly Growing Aerobic Bacteria Involved in Infectious Diseases. Available online: https://www.iso.org/standard/70464.html (accessed on 1 March 2018).
- Tsuchiya, H. Membrane interactions of phytochemicals as their molecular mechanism applicable to the discovery of drug leads from plants. Molecules 2015, 20, 18923–18966. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Zang, X.; He, M.; Pan, S.; Xu, X. Structure-activity relationship of flavonoids on their anti- Escherichia coli activity and inhibition of DNA gyrase. J. Agric. Food Chem. 2013, 61, 8185–8190. [Google Scholar] [CrossRef] [PubMed]
- Eumkeb, G.; Chukrathok, S. Synergistic activity and mechanism of action of ceftazidime and apigenin combination against ceftazidime-resistant Enterobacter cloacae. Phytomedicine 2013, 20, 262–269. [Google Scholar] [CrossRef]
- Zambrano, C.; Kerekes, E.B.; Kotogán, A.; Papp, T.; Vágvölgyi, C.; Krisch, J.; Takó, M. Antimicrobial activity of grape, apple and pitahaya residue extracts after carbohydrase treatment against food-related bacteria. Lwt 2019, 100, 416–425. [Google Scholar] [CrossRef]
- Duda-Chodak, A. The inhibitory effect of polyphenols on human gut microbiota. J. Physiol. Pharmacol. 2012, 63, 497–503. [Google Scholar]
- Parkar, S.G.; Stevenson, D.E.; Skinner, M.A. The potential influence of fruit polyphenols on colonic microflora and human gut health. Int. J. Food Microbiol. 2008, 124, 295–298. [Google Scholar] [CrossRef]
- Kozłowska, J.; Potaniec, B.; Baczyńska, D.; Zarowska, B.; Anioł, M. Synthesis and biological evaluation of novel aminochalcones as potential anticancer and antimicrobial agents. Molecules 2019, 24, 4129. [Google Scholar] [CrossRef] [Green Version]
- Breidenstein, E.B.M.; de la Fuente-Núñez, C.; Hancock, R.E.W. Pseudomonas aeruginosa: All roads lead to resistance. Trends Microbiol. 2011, 19, 419–426. [Google Scholar] [CrossRef]
- González, A.; Salillas, S.; Velázquez-Campoy, A.; Espinosa Angarica, V.; Fillat, M.F.; Sancho, J.; Lanas, Á. Identifying potential novel drugs against Helicobacter pylori by targeting the essential response regulator HsrA. Sci. Rep. 2019, 9, 11294. [Google Scholar] [CrossRef] [Green Version]
- Mohammed, N.H.; Mostafa, M.I.; AL-Taher, A.Y. Augmentation effects of novel naringenin analogues and ciprofloxacin as inhibitors for nora efflux pump (EPIs) and pyruvate kinase (PK) against MRSA. J. Anim. Vet. Adv. 2015, 14, 386–392. [Google Scholar]
- Xiao, Z.P.; Wang, X.D.; Wang, P.F.; Zhou, Y.; Zhang, J.W.; Zhang, L.; Zhou, J.; Zhou, S.S.; Hui, O.; Lin, X.Y.; et al. Design, synthesis, and evaluation of novel fluoroquinolone-flavonoid hybrids as potent antibiotics against drug-resistant microorganisms. Eur. J. Med. Chem. 2014, 80, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Bakar, N.S.; Zin, N.M.; Basri, D.F. Synergy of flavone with vancomycin and oxacillin against vancomycin-intermediate Staphyloccus aureus. Pak. J. Pharm. Sci. 2012, 25, 633–638. [Google Scholar] [PubMed]
- Macedo, I.; Da Silva, J.H.; Da Silva, P.T.; Cruz, B.G.; Do Vale, J.P.C.; Dos Santos, H.S.; Bandeira, P.N.; De Souza, E.B.; Xavier, M.R.; Coutinho, H.D.M.; et al. Structural and Microbiological Characterization of 5-Hydroxy-3,7,4-Trimethoxyflavone: A Flavonoid Isolated from Vitex gardneriana Schauer Leaves. Microb. Drug Resist. 2019, 25, 434–438. [Google Scholar] [CrossRef]
- Qu, S.; Dai, C.; Shen, Z.; Tang, Q.; Wang, H.; Zhai, B.; Zhao, L.; Hao, Z. Mechanism of synergy between tetracycline and quercetin against antibiotic resistant Escherichia coli. Front. Microbiol. 2019, 10, 2536. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, G.; Saigal, S.; Elongavan, A. Action and resistance mechanisms of antibiotics: A guide for clinicians. J. Anaesthesiol. Clin. Pharmacol. 2017, 33, 300–305. [Google Scholar] [CrossRef]
- Wang, L.H.; Wang, M.S.; Zeng, X.A.; Xu, X.M.; Brennan, C.S. Membrane and genomic DNA dual-targeting of citrus flavonoid naringenin against: Staphylococcus aureus. Integr. Biol. 2017, 9, 820–829. [Google Scholar] [CrossRef]
- Oh, E.; Jeon, B. Contribution of surface polysaccharides to the resistance of Campylobacter jejuni to antimicrobial phenolic compounds. J. Antibiot. 2015, 68, 591–593. [Google Scholar] [CrossRef]
- Oh, E.; Jeon, B. Synergistic anti-Campylobacter jejuni activity of fluoroquinolone and macrolide antibiotics with phenolic compounds. Front. Microbiol. 2015, 6, 1129. [Google Scholar] [CrossRef] [Green Version]
- Baldim, J.L.; De Alcantara, B.G.V.; Domingos, O.D.S.; Soares, M.G.; Caldas, I.S.; Novaes, R.D.; Oliveira, T.B.; Lago, J.H.G.; Chagas-Paula, D.A. The Correlation between Chemical Structures and Antioxidant, Prooxidant, and Antitrypanosomatid Properties of Flavonoids. Oxid. Med. Cell. Longev. 2017, 2017. [Google Scholar] [CrossRef]
- Dwyer, D.J.; Belenky, P.A.; Yang, J.H.; Cody MacDonald, I.; Martell, J.D.; Takahashi, N.; Chan, C.T.Y.; Lobritz, M.A.; Braff, D.; Schwarz, E.G.; et al. Antibiotics induce redox-related physiological alterations as part of their lethality. Proc. Natl. Acad. Sci. USA 2014, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uckun, Z.; Guzel, S.; Canacankatan, N.; Yalaza, C.; Kibar, D.; Coskun Yilmaz, B. Potential protective effects of naringenin against vancomycin-induced nephrotoxicity via reduction on apoptotic and oxidative stress markers in rats. Drug Chem. Toxicol. 2020, 43, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Bustos, P.S.; Deza-Ponzio, R.; Páez, P.L.; Cabrera, J.L.; Virgolini, M.B.; Ortega, M.G. Flavonoids as protective agents against oxidative stress induced by gentamicin in systemic circulation. Potent protective activity and microbial synergism of luteolin. Food Chem. Toxicol. 2018, 118, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Bertani, B.; Ruiz, N. Function and biogenesis of lipopolysaccharides. EcoSal Plus 2018, 8, 10–1128. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Yang, T.; Liao, T.; Debowski, A.W.; Nilsson, H.-O.; Fulurija, A.; Haslam, S.M.; Mulloy, B.; Dell, A.; Stubbs, K.A.; et al. The redefinition of Helicobacter pylori lipopolysaccharide O-antigen and core-oligosaccharide domains. PLOS Pathog. 2017, 13, e1006280. [Google Scholar] [CrossRef] [PubMed]
- Bahrin, L.G.; Apostu, M.O.; Birsa, L.M.; Stefan, M. The antibacterial properties of sulfur containing flavonoids. Bioorganic Med. Chem. Lett. 2014, 24, 2315–2318. [Google Scholar] [CrossRef]
- Cushnie, T.P.T.; Hamilton, V.E.S.; Chapman, D.G.; Taylor, P.W.; Lamb, A.J. Aggregation of Staphylococcus aureus following treatment with the antibacterial flavonol galangin. J. Appl. Microbiol. 2007, 103, 1562–1567. [Google Scholar] [CrossRef] [Green Version]
- Domaracki, B.E.; Evans, A.M.; Venezia, R.A. Vancomycin and oxacillin synergy for methicillin-resistant staphylococci. Antimicrob. Agents Chemother. 2000, 44, 1394–1396. [Google Scholar] [CrossRef] [Green Version]
- Sieradzki, K.; Tomasz, A. Inhibition of cell wall turnover and autolysis by vancomycin in a highly vancomycin-resistant mutant of Staphylococcus aureus. J. Bacteriol. 1997, 179, 2557–2566. [Google Scholar] [CrossRef] [Green Version]
Sample Availability: Samples of the compounds 1a–9a and 1b–9b are available from the authors. |




{kind=link}
{kind=link}
{kind=link}
| No. | O-alkyl Derivatives | No. | Oximes |
|---|---|---|---|
| 1a |  | 1b |  |
| 7-O-methylnaringenin | 7-O-methylnaringenin oxime | ||
| 2a |  | 2b |  |
| 7,4′-di-O-methylnaringenin | 7,4′-di-O-methylnaringenin oxime | ||
| 3a |  | 3b |  |
| 7-O-ethylnaringenin | 7-O-ethylnaringenin oxime | ||
| 4a |  | 4b |  |
| 7-O-isopropylnaringenin | 7-O-isopropylnaringenin oxime | ||
| 5a |  | 5b |  |
| 7,4′-di-O-isopropylnaringenin | 7,4′-di-O-isopropylnaringenin oxime | ||
| 6a |  | 6b |  |
| 7-O-butylnaringenin | 7-O-butylnaringenin oxime | ||
| 7a |  | 7b |  |
| 7-O-pentylnaringenin | 7-O-pentylnaringenin oxime | ||
| 8a |  | 8b |  |
| 7-O-hexylnaringenin | 7-O-hexylnaringenin oxime | ||
| 9a |  | 9b |  |
| 7,4′-di-O-hexylnaringenin | 7,4′-di-O-hexylnaringenin oxime |
| Strain | Antimicrobial Resistance Profile |
|---|---|
| Helicobacter pylori 7189 | CLR R, MTZ S, LEV S |
| Staphylococcus aureus KJ | FOX R, E R, CLD R, GM S, CIP R,TET S, SXT S, LZD S |
| Enterococcus faecalis 37VRE | VA R, GM R, AMP S, IMP S, TEC S |
| Klebsiella pneumoniae N111 | GM R, TOB R, CIP R, CTX R, CAZ R, CXM R, AMC R, ATM R, FEP R, SAM R, TZP R, IMP S, MEM S, DOR S, CPL S, AKN S |
| Acinetobacter baumannii 2800 | IMP R, MEM R, CIP R, GM R, TOB R, LEV R, FEP R, CAZ R, PIP R, TZP R, AKN R, SXT R, CPL S |
| MIC (MBC) [µg/mL] | |||||
| H. pylori | S. aureus | E. faecalis | K. pneumoniae | A. baumannii | |
| Compounds | |||||
| 1a | 8 (8) | 32 (>1024) | 512 (>1024) | >1024 (>1024) | 512 (>1024) |
| 2a | 16 (64) | >1024 (>1024) | 512 (>1024) | >1024 (>1024) | >1024 (>1024) |
| 3a | 8 (16) | 64 (>1024) | 512 (>1024) | >1024 (>1024) | 1024 (>1024) |
| 4a | 8 (8) | 32 (>1024) | 64 (>1024) | >1024 (>1024) | >1024 (>1024) |
| 5a | 16 (16) | 512 (>1024) | 512 (>1024) | >1024 (>1024) | 1024 (>1024) |
| 6a | 8 (8) | 8 (>1024) | >1024 (>1024) | >1024 (>1024) | 1024 (>1024) |
| 7a | 8 (16) | 32 (>1024) | 512 (>1024) | >1024 (>1024) | 1024 (>1024) |
| 8a | 16 (32) | 1024 (>1024) | 128 (>1024) | >1024 (>1024) | >1024 (>1024) |
| 9a | >1024 (>1024) | 512 (>1024) | >1024 (>1024) | >1024 (>1024) | >1024 (>1024) |
| 1b | 8 (16) | 32 (>1024) | 1024 (>1024) | >1024 (>1024) | 1024 (>1024) |
| 2b | 4 (8) | 512 (>1024) | 1024 (>1024) | >1024 (>1024) | 1024 (>1024) |
| 3b | 4 (32) | 16 (>1024) | 1 (>1024) | >1024 (>1024) | 512 (>1024) |
| 4b | 8 (16) | 16 (32) | 32 (64) | >1024 (>1024) | 512 (>1024) |
| 5b | 16 (16) | 8 (>1024) | 2 (>1024) | >1024 (>1024) | 1024 (>1024) |
| 6b | 8 (16) | 4 (>1024) | 512 (>1024) | 512 (>1024) | 1024 (>1024) |
| 7b | 8 (32) | 8 (128) | 8 (>1024) | >1024 (>1024) | 1024 (>1024) |
| 8b | 16 (16) | 4 (128) | 8 (>1024) | 512 (>1024) | 512 (>1024) |
| 9b | >1024 (>1024) | 512 (>1024) | 512 (>1024) | >1024 (>1024) | 512 (>1024) |
| Antibiotics | |||||
| GM | - | 512 (>512) | >1024 (>1024) | 8 (256) | >512 (>512) |
| VA | - | - | 512 (>1024) | - | - |
| E | - | 1024 (>1024) | 4 (16) | - | - |
| IMP | - | - | - | 0.5 (1) | 32 (32) |
| CPL | - | - | - | 1 (2) | 2 (2) |
| CLR | 32 (64) | - | - | - | - |
| LEV | 0.5 (0.5) | - | - | - | - |
| MTZ | 8 (16) | - | - | - | - |
| Strain | Combination | FICANTIBIOTIC | FICCOMPOUND | FICINDEX | Interaction |
|---|---|---|---|---|---|
| H. pylori 7189 | CLR + 2b | 0.25 | 0.25 | 0.5 | synergistic |
| MTZ + 2b | 0.25 | 0.5 | 0.75 | additive | |
| LEV + 2b | 0.25 | 0.5 | 0.75 | additive | |
| E. faecalis 37VRE | GM + 4b | 0.0625 | 0.5 | 0.5625 | additive |
| IMP + 4b | 1 | 1 | 2 | neutral | |
| VA + 4b | 0.5 | 0.125 | 0.625 | additive | |
| GM + 8b | 1 | 1 | 2 | neutral | |
| IMP + 8b | 1 | 1 | 2 | neutral | |
| VA + 8b | 0.125 | 0.25 | 0.375 | synergistic | |
| S. aureus KJ | GM + 4b | 0.125 | 0.25 | 0.375 | synergistic |
| E + 4b | 0.25 | 0.25 | 0.5 | synergistic | |
| GM + 8b | 0.25 | 0.25 | 0.5 | synergistic | |
| E + 8b | 0.25 | 0.25 | 0.5 | synergistic | |
| K. pneumoniae N111 | GM + 6b | 1 | 1 | 2 | neutral |
| IMP + 6b | 1 | 1 | 2 | neutral | |
| CPL + 6b | 1 | 1 | 2 | neutral | |
| A. baumannii 2800 | GM + 3b | 1 | 1 | 2 | neutral |
| IMP + 3b | 1 | 1 | 2 | neutral | |
| CPL + 3b | 0.5 | 0.0625 | 0.5625 | additive |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duda-Madej, A.; Kozłowska, J.; Krzyżek, P.; Anioł, M.; Seniuk, A.; Jermakow, K.; Dworniczek, E. Antimicrobial O-Alkyl Derivatives of Naringenin and Their Oximes Against Multidrug-Resistant Bacteria. Molecules 2020, 25, 3642. https://doi.org/10.3390/molecules25163642
Duda-Madej A, Kozłowska J, Krzyżek P, Anioł M, Seniuk A, Jermakow K, Dworniczek E. Antimicrobial O-Alkyl Derivatives of Naringenin and Their Oximes Against Multidrug-Resistant Bacteria. Molecules. 2020; 25(16):3642. https://doi.org/10.3390/molecules25163642
Chicago/Turabian StyleDuda-Madej, Anna, Joanna Kozłowska, Paweł Krzyżek, Mirosław Anioł, Alicja Seniuk, Katarzyna Jermakow, and Ewa Dworniczek. 2020. "Antimicrobial O-Alkyl Derivatives of Naringenin and Their Oximes Against Multidrug-Resistant Bacteria" Molecules 25, no. 16: 3642. https://doi.org/10.3390/molecules25163642
APA StyleDuda-Madej, A., Kozłowska, J., Krzyżek, P., Anioł, M., Seniuk, A., Jermakow, K., & Dworniczek, E. (2020). Antimicrobial O-Alkyl Derivatives of Naringenin and Their Oximes Against Multidrug-Resistant Bacteria. Molecules, 25(16), 3642. https://doi.org/10.3390/molecules25163642