
Promising Roles of Alternative Medicine and Plant-Based Nanotechnology as Remedies for Urinary Tract Infections

 , , , and
, , , and 
Abstract
:1. Introduction
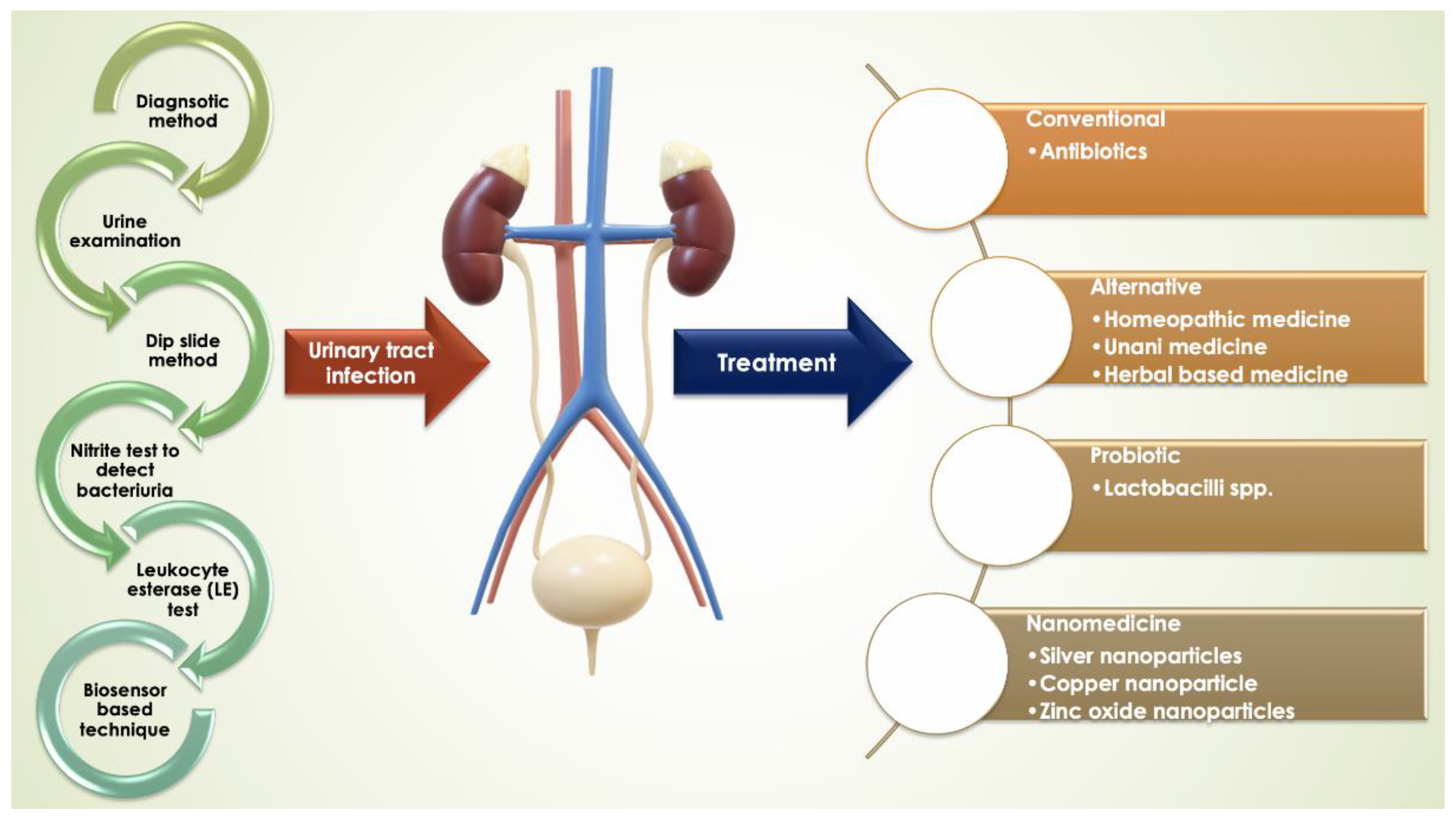
2. Diagnosis of UTI
2.1. Conventional Method of Detecting UTI
2.1.1. Urine Examination
2.1.2. Dip Slide Method
2.1.3. Nitrite Test to Detect Bacteriuria
2.1.4. Leukocyte Esterase (LE) Test for Detection of Pyuria
3. Modern Approach in the Detection of UTI
Biosensor-Based Technique
4. Treatments for UTI
4.1. Antibiotics Prescribed in UTI
4.2. Alternative Traditional Therapies for UTI Treatment
4.2.1. Homeopathic Medicine
4.2.2. Unani Medicine
4.2.3. Herbal-Based Medicine
5. Bacteriophage Therapy
6. Probiotics
7. Nanomedicine in UTI
8. Conclusions and Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Rose, C.; Parker, A.H.; Jefferson, B.; Cartmell, E. The characterization of feces and urine: A review of the literature to inform advanced treatment technology. Crit. Rev. Environ. Sci. Technol. 2015, 45, 1827–1879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaha, D.C.; Bungau, S.; Aleya, S.; Tit, D.M.; Vesa, C.M.; Popa, A.R.; Pantis, C.; Maghiar, O.A.; Bratu, O.G.; Furau, C.; et al. What antibiotics for what pathogens? The sensitivity spectrum of isolated strains in an intensive care unit. Sci. Total. Environ. 2019, 687, 118–127. [Google Scholar] [CrossRef]
- Tamalli, M.; Bioprabhu, S.; Alghazal, M.A. Urinary tract infection during pregnancy at Al-khoms. Int. J. Med. Med. Sci. 2013, 3, 455–459. [Google Scholar]
- Siddiq, D.M.; Darouiche, R.O. New strategies to prevent catheter-associated urinary tract infections. Nat. Rev. Urol. 2012, 9, 305–314. [Google Scholar] [CrossRef]
- Yassin, M.A.; Elkhooly, T.A.; Elsherbiny, S.M.; Reicha, F.M.; Shokeir, A.A. Facile coating of urinary catheter with bio–inspired antibacterial coating. Heliyon 2019, 5, e02986. [Google Scholar] [CrossRef] [Green Version]
- Syed, M.A.; Manzoor, U.; Shah, I.; Bukhari, S.H. Antibacterial effects of Tungsten nanoparticles on the Escherichia coli strains isolated from catheterized urinary tract infection (UTI) cases and Staphylococcus aureus. New Microbiol. 2010, 33, 329–335. [Google Scholar]
- Syed, M.A.; Babar, S.; Bhatti, A.S.; Bokhari, H. Antibacterial effects of silver nanoparticles on the bacterial strains isolated from catheterized urinary tract infection cases. J. Biomed. Nanotechnol. 2009, 5, 209–214. [Google Scholar] [CrossRef]
- Odoki, M.; Aliero, A.A.; Tibyangye, J.; Maniga, J.N.; Wampande, E.; Kato, C.D.; Agwu, E.; Bazira, J. Prevalence of bacterial urinary tract infections and associated factors among patients attending hospitals in Bushenyi district, Uganda. Int. J. Microbiol. 2019, 2019, 1–8. [Google Scholar] [CrossRef]
- Warkulwiz, G.; Hannon, K.; Cabano, D.; Mehta, K. Urinary tract infections (UTIs) in rural Kenya: Screening challenges, treatment pathways, and technological solutions. In Proceedings of the 2017 IEEE Global Humanitarian Technology Conference (GHTC), San Jose, CA, USA, 19–22 October 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Stamm, W.E.; Norrby, S.R. Urinary tract infections: Disease panorama and challenges. J. Infect. Dis. 2001, 183, S1–S4. [Google Scholar] [CrossRef]
- Siakwa, M.; John, M.E.; Kpikpitse, D.; Ankobil, A.; Hansen-Owoo, E. Pregnancy outcomes: A comparison of women with symptomatic and asymptomatic bacteriuria in Cape Coast, Ghana. Afr. J. Pregnancy Childbirth 2014, 2, 27–30. [Google Scholar]
- Tan, C.W.; Chlebicki, M.P. Urinary tract infections in adults. Singap. Med J. 2016, 57, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Rajivgandhi, G.; Vijayan, R.; Kannan, M.; Santhanakrishnan, M.; Manoharan, N. Molecular characterization and antibacterial effect of endophytic actinomycetes Nocardiopsis sp. GRG1 (KT235640) from brown algae against MDR strains of uropathogens. Bioact. Mater. 2016, 1, 140–150. [Google Scholar] [CrossRef] [Green Version]
- Casertano, M.; Menna, M.; Imperatore, C. The ascidian-derived metabolites with antimicrobial properties. Antibiotics 2020, 9, 510. [Google Scholar] [CrossRef] [PubMed]
- Ayuningrum, D.; Liu, Y.; Riyanti; Sibero, M.T.; Kristiana, R.; Asagabaldan, M.A.; Wuisan, Z.G.; Trianto, A.; Radjasa, O.K.; Sabdono, A.; et al. Tunicate-associated bacteria show a great potential for the discovery of antimicrobial compounds. PLoS ONE 2019, 14, e0213797. [Google Scholar] [CrossRef]
- Tit, D.M.; Pallag, A.; Iovan, C.; Furău, G.; Furău, C.; Bungau, S. Somatic-vegetative symptoms evolution in postmenopausal women treated with phytoestrogens and hormone replacement therapy. Iran. J. Public Health 2017, 46, 1528–1534. [Google Scholar]
- Kunin, C.M. Urinary tract infections in females. Clin. Infect. Dis. 1994, 18, 1–12. [Google Scholar] [CrossRef]
- Kant, S.; Lohiya, A.; Kapil, A.; Gupta, S.K. Urinary tract infection among pregnant women at a secondary level hospital in Northern India. Indian J. Public Health 2017, 61, 118–123. [Google Scholar]
- Jenkins, R.D.; Fenn, J.P.; Matsen, J.M. Review of urine microscopy for bacteriuria. JAMA 1986, 255, 3397–3403. [Google Scholar] [CrossRef]
- Bjerrum, L.; Grinsted, P.; Søgaard, P. Detection of bacteriuria by microscopy and dipslide culture in general practice. Eur. J. Gen. Pr. 2001, 7, 55–58. [Google Scholar] [CrossRef]
- Collee, J.G.; Miles, R.S.; Watt, B. Mackie & McCartney Practical Medical Microbiology, 14th ed.; Churchill Livingstone: New York, NY, USA, 1996. [Google Scholar]
- Lenke, R.R.; Van Dorsten, J. The efficacy of the nitrite test and microscopic urinalysis in predicting urine culture results. Am. J. Obstet. Gynecol. 1981, 140, 427–429. [Google Scholar] [CrossRef]
- Chernow, B.; Zaloga, G.P.; Soldano, S.; Quinn, A.; Lyons, P.; McFadden, E.; Cook, D.; Rainey, T.G. Measurement of urinary leukocyte esterase activity: A screening test for urinary tract infections. Ann. Emerg. Med. 1984, 13, 150–154. [Google Scholar] [CrossRef]
- Kaçmaz, B.; Cakir, O.; Aksoy, A.; Biri, A. Evaluation of rapid urine screening tests to detect asymptomatic bacteriuria in pregnancy. Jpn. J. Infect. Dis. 2006, 59, 261–263. [Google Scholar] [PubMed]
- Ronkainen, N.J.; Halsall, H.B.; Heineman, W.R. Electrochemical biosensors. Chem. Soc. Rev. 2010, 39, 1747–1763. [Google Scholar] [CrossRef] [PubMed]
- Nikolaevna, K.A.; Svalova, T.; Malysheva, N.N.; Okhokhonin, A.V.; Vidrevich, M.B.; Brainina, K. Sensors Based on bio and biomimetic receptors in medical diagnostic, environment, and food analysis. Biosens 2018, 8, 35. [Google Scholar] [CrossRef] [Green Version]
- Mach, K.E.; Wong, P.K.; Liao, J.C. Biosensor diagnosis of urinary tract infections: A path to better treatment? Trends Pharmacol. Sci. 2011, 32, 330–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakata, M.; Inoue, T.; Todokoro, M.; Kunitake, M. Limulus Amebocyte Lysate assay for endotoxins by an adsorption method with polycation-immobilized cellulose beads. Anal. Sci. 2010, 26, 291–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehrotra, P. Biosensors and their applications—A review. J. Oral Biol. Craniofacial Res. 2016, 6, 153–159. [Google Scholar] [CrossRef] [Green Version]
- Sin, M.L.Y.; E Mach, K.; Wong, P.K.; Liao, J.C. Advances and challenges in biosensor-based diagnosis of infectious diseases. Expert Rev. Mol. Diagn. 2014, 14, 225–244. [Google Scholar] [CrossRef] [Green Version]
- Reid, G.; Bruce, A.W.; Cook, R.L.; Llano, M. Effect on urogenital flora of antibiotic therapy for urinary tract infection. Scand. J. Infect. Dis. 1990, 22, 43–47. [Google Scholar] [CrossRef]
- E Dyer, I.; Sankary, T.M.; A Dawson, J. Antibiotic resistance in bacterial urinary tract infections, 1991 to 1997. West. J. Med. 1998, 169, 265–268. [Google Scholar]
- Raz, R.; Rottensterich, E.; Leshem, Y.; Tabenkin, H. Double-blind study comparing 3-day regimens of cefixime and ofloxacin in treatment of uncomplicated urinary tract infections in women. Antimicrob. Agents Chemother. 1994, 38, 1176–1177. [Google Scholar] [CrossRef] [Green Version]
- Anderson, V.R.; Perry, C.M. Levofloxacin: A review of its use as a high-dose, short-course treatment for bacterial infection. Drugs 2008, 68, 535–565. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Castrellón, P.; Díaz-García, L.; De Colsa-Ranero, A.; Cuevas-Alpuche, J.; Jiménez-Escobar, I. Efficacy and safety of ciprofloxacin treatment in urinary tract infections (UTIs) in adults: A systematic review with meta-analysis. Gac. Med. Mex. 2015, 151, 225–244. [Google Scholar] [PubMed]
- Odongo, I.; Ssemambo, R.; Kungu, J.M. Prevalence of Escherichia Coli and its antimicrobial susceptibility profiles among patients with UTI at Mulago Hospital, Kampala, Uganda. Interdiscip. Perspect. Infect. Dis. 2020, 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandra, H.; Bishnoi, P.; Yadav, A.; Patni, B.; Mishra, A.P.; Nautiyal, A.R. Antimicrobial resistance and the alternative resources with special emphasis on plant-based antimicrobials—A Review. Plants 2017, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Chandra, H.; Srivastava, J.; Agarwal, R.K. Fundamental Techniques in Microbiology; John Publisher Pvt. Ltd.: New Delhi, India, 2016. [Google Scholar]
- Nwabudike, L.C. Classical homeopathy and bacterial urinary tract infections. Proc. Rom. Acad. 2017, 19, 93–96. [Google Scholar]
- Coelho, C.D.P.; Motta, P.D.; Petrillo, M.; Iovine, R.D.O.; Dalboni, L.C.; Santana, F.R.; Correia, M.S.F.; Casarin, R.C.V.; Carvalho, V.M.; Bonamin, L.V. Homeopathic medicine Cantharis modulates uropathogenic E. coli (UPEC)-induced cystitis in susceptible mice. Cytokine 2017, 92, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Chand, K.S.; Kapoor, P. Two Case Reports of Integrated Management of Antibiotic-Resistant Urinary Tract Infection. Homeopathy 2020, 109, 097–106. [Google Scholar] [CrossRef]
- Kurmann, C.; Imbach, E.; Amsler, F.; Pannek-Rademacher, S.; Pannek, J. In-vitro effects of homeopathic drugs on cultured Escherichia coli. Homeopathy 2018, 107, 150–154. [Google Scholar] [CrossRef]
- Zubair, M.; Nayab, M.; Jameel, S.; Qadeer, A. Effect of Unani formulation on urine composition in the patients of Warm-e-Majra-e-Baul–An observational study. Int. J. Herb. 2014, 1, 47–50. [Google Scholar]
- Nishat, A.; Sultana, S.; Sultana, A. A comparative study of polyherbal Unani formulations in gestational Urinary tract infections. J. Exp. Integr. Med. 2017, 7, 1. [Google Scholar] [CrossRef]
- Ashraf, J.; Latafat, T.; Mohsin, M. Therapeutic evaluation of Safuf Mudir and Sharbat Bazuri Motadil in urinary tract infections (Tadiya Majrae-Baul). HJUM 2012, 7, 21–29. [Google Scholar]
- Ahmad, T.; Khan, A.B.; Latafat, T. Urinary tract infection (tadiya majar-e-baul) in the light of Unani system of medicine: An overview. J. Pharm. Sci. Innov. 2015, 4, 242–246. [Google Scholar] [CrossRef]
- Mutters, N.T.; Mampel, A.; Kropidlowski, R.; Biehler, K.; Günther, F.; Bălu, I.; Malek, V.; Frank, U. Treating urinary tract infections due to MDR E. coli with Isothiocyanates—A phytotherapeutic alternative to antibiotics? Fitoterapia 2018, 129, 237–240. [Google Scholar] [CrossRef]
- Mishra, S.; Mekap, S.K.; Patra, S.; Dhal, N.K.; Sahooa, S. Antioxidant and anti-infective potential of Oleanolic acid acetate vis-à-vis Vitex negundo Linn. and Oroxylum indicum Vent. against human pathogens causing infections of UT, GIT and skin. Orient. Pharm. Exp. Med. 2014, 15, 73–82. [Google Scholar] [CrossRef]
- McMurdo, M.E.T.; Argo, I.; Phillips, G.; Daly, F.; Davey, P. Cranberry or trimethoprim for the prevention of recurrent urinary tract infections? A randomized controlled trial in older women. J. Antimicrob. Chemother. 2008, 63, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Sandhu, N.S.; Kaur, S.; Chopra, D. Equietum arvense: Pharmacology and phytochemistry—A review. Asian J. Pharm. Clin. Res. 2010, 3, 146–150. [Google Scholar]
- Carneiro, D.M.; Freire, R.C.; Honório, T.C.; Zoghaib, I.; Cardoso, F.F.; Tresvenzol, L.M.; de Paula, J.R.; Sousa, A.L.; Jardim, P.C.; da Cunha, L.C. Randomized, double-blind clinical trial to assess the acute diuretic effect of Equisetum arvense (Field Horsetail) in healthy volunteers. Evid. Based Complement. Altern. Med. 2014, 2014, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dog, T.L. Urinary Tract Infection. In Women’s Health in Complementary and Integrative Medicine; Dog, T.L., Ed.; Churchill Livingstone: Saint Louis, MI, USA, 2005; pp. 293–306. [Google Scholar] [CrossRef]
- Pereira, R.S.; Sumita, T.C.; Furlan, M.R.; Jorge, A.O.C.; Ueno, M. Atividade antibacteriana de óleos essenciais em cepas isoladas de infecção urinária. Rev. Saúde Pública 2004, 38, 326–328. [Google Scholar] [CrossRef]
- Sharma, A.; Chandraker, S.; Patel, V.K.; Ramteke, P. Antibacterial activity of medicinal plants against pathogens causing complicated urinary tract infections. Indian J. Pharm. Sci. 2009, 71, 136–139. [Google Scholar] [CrossRef] [Green Version]
- Rafsanjany, N.; Lechtenberg, M.; Petereit, F.; Hensel, A. Antiadhesion as a functional concept for protection against uropathogenic Escherichia coli: Invitro studies with traditionally used plants with antiadhesive activity against uropathognic Escherichia coli. J. Ethnopharmacol. 2013, 145, 591–597. [Google Scholar] [CrossRef]
- Bag, A.; Bhattacharyya, S.K.; Chattopadhyay, R.R. Medicinal plants and urinary tract infections: An update. Pharm. Rev. 2008, 2, 277–284. [Google Scholar]
- Handeland, M.; Grude, N.; Torp, T.; Slimestad, R. Black chokeberry juice (Aronia melanocarpa) reduces incidences of urinary tract infection among nursing home residents in the long term—A pilot study. Nutr. Res. 2014, 34, 518–525. [Google Scholar] [CrossRef]
- Lagha, R.; Ben Abdallah, F.; Al-Sarhan, B.O.; Al-Sodany, Y.M. Antibacterial and biofilm inhibitory activity of medicinal plant essential oils against Escherichia coli isolated from UTI patients. Molecules 2019, 24, 1161. [Google Scholar] [CrossRef] [Green Version]
- Mishra, M.P.; Rath, S.; Swain, S.S.; Ghosh, G.; Das, D.; Padhy, R.N. In-vitro antibacterial activity of crude extracts of 9 selected medicinal plants against UTI causing MDR bacteria. J. King Saud Univ. Sci. 2017, 29, 84–95. [Google Scholar] [CrossRef] [Green Version]
- Dhanasekaran, S.; Rajesh, A.; Mathimani, T.; Samuel, S.M.; Shanmuganathan, R.; Brindhadevi, K.; Samuel, M.S. Efficacy of crude extracts of Clitoria ternatea for antibacterial activity against gram negative bacterium (Proteus mirabilis). Biocatal. Agric. Biotechnol. 2019, 21, 101328. [Google Scholar] [CrossRef]
- Bouterfas, K.; Mehdadi, Z.; Elaoufi, M.M.; Aouad, L.; Latreche, A.; Benchiha, W. Invitro antibacterial activity of flavonoids extracts from three Algerian horehound (Marrubium vulgare L.) leaves. Orient. Pharm. Exp. Med. 2017, 18, 59–66. [Google Scholar] [CrossRef]
- Alshami, I.; Alharbi, A.E. Antimicrobial activity of Hibiscus sabdariffa extract against uropathogenic strains isolated from recurrent urinary tract infections. Asian Pac. J. Trop. Dis. 2014, 4, 317–322. [Google Scholar] [CrossRef]
- Njobdi, S.; Gambo, M.; Ishaku, G.A. Antibacterial activity of Zingiber officinale on Escherichia coli and Staphylococcus aureus. J. Adv. Biol. Biotechnol. 2018, 19, 1–8. [Google Scholar] [CrossRef]
- Tariq, A.L.; Reyaz, A.L. Terminalia chebula: A treatment against pathogenic proteus vulgaris strains associated with urinary tract infection. Int. J. Res. Ayurveda Pharm. 2013, 4, 560–563. [Google Scholar] [CrossRef]
- Vineeth, T.; Deepak, M.; Shree, A.B.; Vaidya, A. Antibacterial effect of Boerhavia diffusa and Punarnavasavam on urinary tract infection (Uti) causing pathogens. World J. Pharm. Res. 2014, 3, 423–437. [Google Scholar]
- Hankin, M.E. The bactericidal action of the waters of the Jamuna and Ganges rivers on Cholera microbes. Ann. Inst. Pasteur 10:511–523 (1896). Bacteriophage 2011, 1, 117–126. [Google Scholar] [CrossRef]
- Twort, F. An investigation on the nature of ultra-microscopic viruses. Lancet 1915, 186, 1241–1243. [Google Scholar] [CrossRef] [Green Version]
- Ackermann, H.W. On an invisible microbe antagonistic to dysentery bacilli. Note by M. F. d’Herelle, presented by M. Roux. Comptes Rendus Academie des Sciences 1917; 165:373–5. Bacteriophage 2011, 1, 3–5. [Google Scholar] [CrossRef] [Green Version]
- Patey, O.; McCallin, S.; Mazure, H.; Liddle, M.; Smithyman, A.; Dublanchet, A. Clinical indications and compassionate use of phage therapy: Personal experience and literature review with a focus on osteoarticular infections. Viruses 2018, 11, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ujmajuridze, A.; Chanishvili, N.; Goderdzishvili, M.; Leitner, L.; Mehnert, U.; Chkhotua, A.; Kessler, T.M.; Sybesma, W. Adapted bacteriophages for treating urinary tract infections. Front. Microbiol. 2018, 9, 1832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sybesma, W.; Zbinden, R.; Chanishvili, N.; Kutateladze, M.; Chkhotua, A.; Ujmajuridze, A.; Mehnert, U.; Kessler, T.M. Bacteriophages as potential treatment for urinary tract infections. Front. Microbiol. 2016, 7, 465. [Google Scholar] [CrossRef]
- Sulakvelidze, A.; Alavidze, Z.; Morris, J.G. Bacteriophage Therapy. Antimicrob. Agents Chemother. 2001, 45, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Reid, G.; Beuerman, D.; Heinemann, C.; Bruce, A.W. Probiotic Lactobacillus dose required to restore and maintain a normal vaginal flora. FEMS Immunol. Med Microbiol. 2001, 32, 37–41. [Google Scholar] [CrossRef] [Green Version]
- Borchert, D.H.; Sheridan, L.; Papatsoris, A.; Faruquz, Z.; Barua, J.M.; Junaid, I.; Pati, Y.; Chinegwundoh, F.; Buchholz, N. Prevention and treatment of urinary tract infection with probiotics: Review and research perspective. Indian J. Urol. 2008, 24, 139–144. [Google Scholar] [CrossRef]
- Mack, D.R. Probiotics-mixed messages. Can. Fam. Physician 2005, 51, 1455–1457. [Google Scholar] [PubMed]
- Reid, G.; Bruce, A.W. Probiotics to prevent urinary tract infections: The rationale and evidence. World J. Urol. 2006, 24, 28–32. [Google Scholar] [CrossRef]
- Butler, D.S.C.; Silvestroni, A.; Stapleton, A.E. Cytoprotective effect of Lactobacillus crispatus CTV-05 against uropathogenic E. coli. Pathogens 2016, 5, 27. [Google Scholar] [CrossRef] [Green Version]
- Koradia, P.; Kapadia, S.; Trivedi, Y.; Chanchu, G.; Harper, A. Probiotic and cranberry supplementation for preventing recurrent uncomplicated urinary tract infections in premenopausal women: A controlled pilot study. Expert Rev. Anti-Infect. Ther. 2019, 17, 733–740. [Google Scholar] [CrossRef] [Green Version]
- Stapleton, A.E.; Au-Yeung, M.; Hooton, T.M.; Fredricks, D.N.; Roberts, P.L.; Czaja, C.A.; Yarova-Yarovaya, Y.; Fiedler, T.; Cox, M.; Stamm, W.E. Randomized, placebo-controlled phase 2 trial of a Lactobacillus crispatus probiotic given intravaginally for prevention of recurrent urinary tract infection. Clin. Infect. Dis. 2011, 52, 1212–1217. [Google Scholar] [CrossRef] [PubMed]
- Robles-Martínez, M.; Patiño-Herrera, R.; Pérez-Vázquez, F.J.; Montejano-Carrizales, J.M.; González, J.F.C.; Pérez, E. Mentha piperita as a natural support for silver nanoparticles: A new Anti-candida albicans treatment. Colloid Interface Sci. Commun. 2020, 35, 100253. [Google Scholar] [CrossRef]
- Asahara, T.; Nomoto, K.; Watanuki, M.; Yokokura, T. Antimicrobial activity of intraurethrally administered probiotic Lactobacillus casei in a murine model of Escherichia coli urinary tract infection. Antimicrob. Agents Chemother. 2001, 45, 1751–1760. [Google Scholar] [CrossRef] [Green Version]
- Amdekar, S.; Singh, V.; Singh, D.D. Probiotic therapy: Immunomodulating approach toward urinary tract infection. Curr. Microbiol. 2011, 63, 484–490. [Google Scholar] [CrossRef]
- Borriello, S.P.; Hammes, W.P.; Holzapfel, W.; Marteau, P.; Schrezenmeir, J.; Vaara, M.; Valtonen, V. Safety of probiotics that contain Lactobacilli or Bifidobacteria. Clin. Infect. Dis. 2003, 36, 775–780. [Google Scholar] [CrossRef]
- Ng, S.C.; Hart, A.L.; Kamm, M.A.; Stagg, A.J.; Knight, S.C. Mechanisms of action of probiotics: Recent advances. Inflamm. Bowel Dis. 2009, 15, 300–310. [Google Scholar] [CrossRef]
- Inbaneson, S.J.; Sundaram, R.; Manikandan, N. Antibacterial potential of silver nanoparticles against isolated urinary tract infectious bacterial pathogens. Appl. Nanosci. 2011, 1, 231–236. [Google Scholar] [CrossRef] [Green Version]
- Al-Enizi, A.M.; Ahamad, T.; Al-Hajji, A.B.; Ahmed, J.; Chaudhary, A.A.; AlShehri, S.M. Cellulose gum and copper nanoparticles based hydrogel as antimicrobial agents against urinary tract infection (UTI) pathogens. Int. J. Biol. Macromol. 2018, 109, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Al Tameemi, M.B.M.; Stan, R.; Prisacari, V.; Voicu, G.; Popa, M.; Chifiriuc, M.C.; Ott, C.; Marton, G.; Meghea, A. Antimicrobial performance of nanostructured silica–titania sieves loaded with izohidrafural against microbial strains isolated from urinary tract infections. Comptes Rendus Chim. 2017, 20, 475–483. [Google Scholar] [CrossRef]
- Chandra, H.; Patel, D.; Kumari, P.; Jangwan, J.; Yadav, S. Phyto-mediated synthesis of zinc oxide nanoparticles of Berberis aristata: Characterization, antioxidant activity and antibacterial activity with special reference to urinary tract pathogens. Mater. Sci. Eng. C 2019, 102, 212–220. [Google Scholar] [CrossRef]
- Santhoshkumar, J.; Kumar, S.V.; RajeshKumar, S. Synthesis of zinc oxide nanoparticles using plant leaf extract against urinary tract infection pathogen. Resour. Technol. 2017, 3, 459–465. [Google Scholar] [CrossRef]
- Malarkodi, C.; RajeshKumar, S. Invitro bactericidal activity of biosynthesized CuS nanoparticles against UTI-causing pathogens. Inorg. Nano-Metal Chem. 2017, 47, 1290–1297. [Google Scholar] [CrossRef]
- Mishra, M.P.; Padhy, R.N. Antibacterial activity of green silver nanoparticles synthesized from Anogeissus acuminata against multidrug resistant urinary tract infecting bacteria invitro and host-toxicity testing. J. Appl. Biomed. 2018, 16, 120–125. [Google Scholar] [CrossRef]
- Divya, M.; Kiran, G.S.; Hassan, S.; Selvin, J. Biogenic synthesis and effect of silver nanoparticles (AgNPs) to combat catheter-related urinary tract infections. Biocatal. Agric. Biotechnol. 2019, 18, 101037. [Google Scholar] [CrossRef]
- Qais, F.A.; Shafiqab, A.; Ahmada, I.; Husain, F.M.; Khan, R.A.; Hassane, I.; Ahmad, I.; Khan, R.A. Green synthesis of silver nanoparticles using Carum copticum: Assessment of its quorum sensing and biofilm inhibitory potential against gram negative bacterial pathogens. Microb. Pathog. 2020, 144, 104172. [Google Scholar] [CrossRef]
- Tallury, P.; Malhotra, A.; Byrne, L.M.; Santra, S. Nanobioimaging and sensing of infectious diseases. Adv. Drug Deliv. Rev. 2010, 62, 424–437. [Google Scholar] [CrossRef]
- Lin, Y.-S.; Tsai, P.-J.; Weng, M.-F.; Chen, Y.-C. Affinity capture using vancomycin-bound magnetic nanoparticles for the MALDI-MS analysis of bacteria. Anal. Chem. 2005, 77, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Zaha, D.C.; Bungau, S.; Uivarosan, D.; Tit, D.M.; Maghiar, T.A.; Maghiar, O.; Pantis, C.; Fratila, O.; Rus, M.; Vesa, C.M. Antibiotic consumption and microbiological epidemiology in surgery departments: Results from a single study center. Antibiotics 2020, 9, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Culture Media | Colony Characteristic/Color | Probable Bacterium |
|---|---|---|
| CLED | Blue green | E. faecalis |
| Pink colony with pink halo | E. coli | |
| Golden yellow | S. aureus | |
| Orange yellow/Greenish | Pr. mirabilis | |
| MacConkey Agar | Lactose fermenting pink colony | E. coli |
| Lactose fermenting mucoid pink colony | Klebsiella sp. | |
| CHROM Agar orientation (CHROM agar company, France) | Pink | E. coli |
| Turquoise blue | Enterococci | |
| Metallic blue | Klebsiella pneumoniae | |
| Metallic blue | Enterobacter spp. | |
| Gave golden, opaque small white | S. aureus | |
| CPS ID2 medium (bioMe’rieux) | Pink | E. coli |
| Blue Green | Enterococcus | |
| Brown color | Ptoteus mirabilis |
| Antibiotics | Year | Ref. |
|---|---|---|
| Amoxicillin or bacampicillin | 1990 | [31] |
| Nitrofurantoin and trimethoprim-sulfamethoxazole (TMP/SMX) | 1991–1997 | [32] |
| Cefixime and Ofloxacin | 1994 | [33] |
| Levofloxacin | 2008 | [34] |
| Ciprofloxacin | 2015 | [35] |
| Cephalexin and Cefuroxime | 2016 | [12] |
| Cefotaxime/clavulanic acid | 2020 | [36] |
| Plant | Inhibit | Fraction | Ref |
|---|---|---|---|
| Zingiber officinale | E. coli | Ethanol, n-Hexane | [54,63] |
| Punica granatum | E. coli, K. pneumoniae, K. oxytoca, Proteus mirabilis, P. vulgaris, Pseudomonas aeruginosa | Ethanol, methanol | [50,54,55,59] |
| Terminalia chebula | K. pneumoniae, Proteus vulgaris | Ethanol | [54,64] |
| Ocimum sanctum | K. pneumoniae, Enterococcus faecalis | Ethanol | [54] |
| Cinnamomum cassia | Ps. aeruginosa | Ethanol | [54] |
| Azadirachta indica | E. faecalis | Ethanol | [54] |
| Thymus zygis | E. coli | Essential oil | [58] |
| Clitoria ternatea Marrubium vulgare L | Pr. Mirabilis E. coli, B. cereus, Pr. mirabilis | Acetone Methanol | [60,61] |
| Hibiscus sabdariffa | E. coli, K. pneumoniae | Methanol | [62] |
| Boerhavia diffusa | Klebsiella sp., Pseudomonas sp., Enterococcus sp., Escherichia coli and Proteus sp. | Ethanol | [65] |
| Vitex negundo Linn | E. coli, S. flexneri | Methanol:dichloromethane (1:1) | [48] |
| Oroxylum indicum | E. coli, S. flexneri | Methanol:dichloromethane (1:1) | [48] |
| Metal NP | Source | Effective Against | Ref. |
|---|---|---|---|
| ZnO-NP | Beberis aristata | Escherichia coli,Staphylococcus aureus,Klebsiella pneumoniae,Bacillus subtilis,Bacillus cereus,Serratia marcescens | [88] |
| ZnO-NP | Passiflora caerulea | E. coli and Enterococcus | [89] |
| CuS-NPs | Serratia nematodiphila | E. coli, S. aureus, Pr vulgaris, and K. pneumoniae | [90] |
| AgNP | Chemical method | E. coli, Pseudomonas aeruginosa, Klebsiella pneumoniae, Enterobacter sp., Proteus morganii and Staphylococcus aureus | [85] |
| AgNP | Anogeissus acuminate | S. aureus, Enterococcus faecalis, A. baumannii, Citrobacter freundii, Enterobacter aerogenes, Escherichia coli, Klebsiella oxytoca, K. pneumoniae, Proteus mirabilis, P. vulgaris and Pseudomonas aeruginosa | [91] |
| AgNP | Chemical method | E. coli, Staphylococcus | [7] |
| W-NPs | Chemical method | E, coli, Staphylococcus | [6] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandra, H.; Singh, C.; Kumari, P.; Yadav, S.; Mishra, A.P.; Laishevtcev, A.; Brisc, C.; Brisc, M.C.; Munteanu, M.A.; Bungau, S. Promising Roles of Alternative Medicine and Plant-Based Nanotechnology as Remedies for Urinary Tract Infections. Molecules 2020, 25, 5593. https://doi.org/10.3390/molecules25235593
Chandra H, Singh C, Kumari P, Yadav S, Mishra AP, Laishevtcev A, Brisc C, Brisc MC, Munteanu MA, Bungau S. Promising Roles of Alternative Medicine and Plant-Based Nanotechnology as Remedies for Urinary Tract Infections. Molecules. 2020; 25(23):5593. https://doi.org/10.3390/molecules25235593
Chicago/Turabian StyleChandra, Harish, Chanchal Singh, Pragati Kumari, Saurabh Yadav, Abhay P. Mishra, Aleksey Laishevtcev, Ciprian Brisc, Mihaela Cristina Brisc, Mihai Alexandru Munteanu, and Simona Bungau. 2020. "Promising Roles of Alternative Medicine and Plant-Based Nanotechnology as Remedies for Urinary Tract Infections" Molecules 25, no. 23: 5593. https://doi.org/10.3390/molecules25235593
APA StyleChandra, H., Singh, C., Kumari, P., Yadav, S., Mishra, A. P., Laishevtcev, A., Brisc, C., Brisc, M. C., Munteanu, M. A., & Bungau, S. (2020). Promising Roles of Alternative Medicine and Plant-Based Nanotechnology as Remedies for Urinary Tract Infections. Molecules, 25(23), 5593. https://doi.org/10.3390/molecules25235593