1. Introduction
Hip and knee joint arthroplasty represent common treatment options for severe arthritis in both elderly and younger patients [
1]. Different types of bearing materials and combinations are used such as metal-on-polyethylene (MOP), ceramic-on-polyethylene (COP), ceramic-on-ceramic (COC) and metal-on-metal (MOM) [
2,
3]. Since prostheses usually have metallic components, they release degradation products such as particulate wear and corrosion debris, metal-protein complexes, free metallic ions, inorganic metal salts or oxides, and/or metals sequestered in an organic storage form [
2]. Depending on the material composition of the prostheses, a systemic exposure to chromium (Cr), cobalt (Co), nickel (Ni), molybdenum (Mo), vanadium (V), titanium (Ti) and aluminum (Al) alloys occurs and may result in increasing metal concentrations in biological fluids and various organs especially in the case of malfunctions of the joint implants [
2,
3,
4].
High concentrations of Cr, Co, Ni, and Al may result in numerous toxic effects. Implant malfunctions can lead to an increased Ni, Co and/or Cr sensitivity (hypersensitivity), skin rashes such as local or generalized skin eczema, wound healing disorders, recurrent pain, hematoma, limited mobility or even implant loosening [
5,
6]. Carcinogenicity and fetal exposure to metallic ions in pregnancy are further documented effects of prolonged exposure to increased concentrations of metal ions [
7].
The determination of the concentration of metals in body fluids and tissues can be used for predicting failure of hip or knee replacements to prevent subsequent severe intoxications. Hart et al. presented in their study the sensitivity and specificity of Co and Cr values in blood to distinguish between well-working and failed hip replacements [
8]. Several studies reported the determination of the metal concentration in body fluids and tissues using different sample sources, sampling methods and measurement techniques (see
Section 2). The number of samples is still limited and the measurement results are difficult to compare due to the variations of the experiments. Furthermore, the sample preparation procedures are often time consuming and characterized by a high human workload forming a bottleneck in the realization of high-throughput measurements.
The failure of metal-containing orthopedic devices is one way of introducting multiple metals into the body. There are further pathways that can also result in elevated metal levels in tissues such as the ingestion of metals via drinking water and nutrition, envi-ronmental conditions, accidental and occupational exposures, pharmaceuticals as well as personal life style (e.g., smoking) [
9,
10]. A widespread examination of a high number of human samples is required to study the effects of metal debris caused by various kinds of hip and knee implants. Therefore, suitable sample preparation procedures and measurement techniques are required which allow a high sample throughput and provide a similar or even better precision and trueness compared to manual processing.
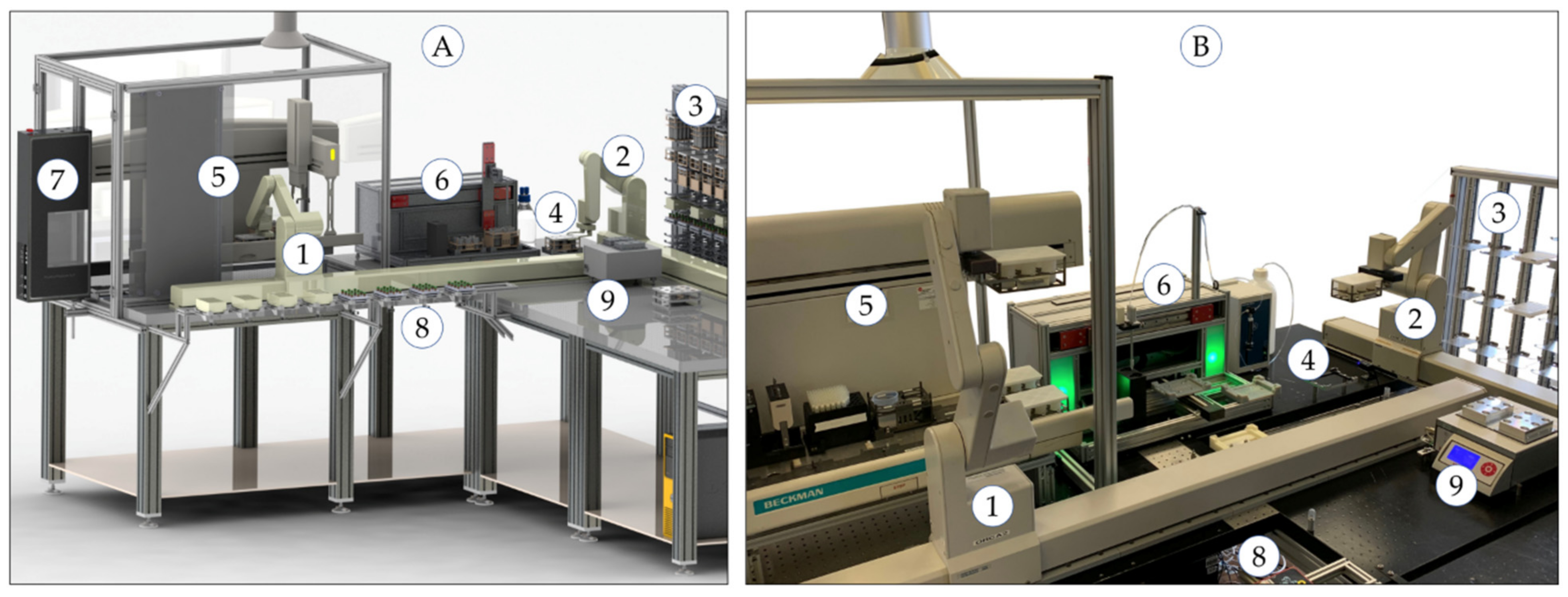
In this study, an semi-automated robot-assisted measurement system is presented for the determination of heavy metals in human tissue samples using inductively coupled plasma mass spectrometry (ICP-MS). In
Section 2, common analytical measurement techniques for the determination of heavy metals in human and animal tissues and body fluids are presented. The advantages of ICP-MS measurements are highlighted for the aim of this study.
Section 3 explains the general measurement process and introduces the system concept and design of the developed robot-assisted automation system. The validation results of the manual and the automated measurement processes are presented in
Section 4 and discussed in
Section 5. Measurement results of the first human samples are given in
Section 6. In the last section, the materials and measurement method details are provided. The paper concludes with a summary and an outlook to further investigations.
2. Determination of Heavy Metals in Human and Animal Tissues
Numerous analytical measurement techniques are available for the determination of metals in biological samples. The most frequently used techniques are flame and graphite furnace atomic absorption spectroscopy (F-AAS, GF-AAS), inductively coupled plasma optical emission spectroscopy (ICP-OES) and, especially, inductively coupled plasma mass spectrometry (ICP-MS) [
11,
12,
13,
14,
15]. Furthermore, measurements using optical microscopy, transmission electron microscopy (TEM), radiochemical neutron activation analysis (RNAA), instrumental neutron activation analysis (INAA), micro X-ray fluorescence (µ-XRF) elemental mapping, and microfocus X-ray absorption spectroscopy (µ-XAS) are documented [
16,
17,
18].
The selection of a suitable analytical measurement technique always depends on the elements to be determined, the sample matrix (e.g., blood, urine, tissue, bone)—which may require a complex sample preparation if necessary—and the aim of investigation. The following examples will give an overview about the recently used measurement procedures in this area.
The determination of essential and toxic trace metals in human autopsy tissues to examine the role of toxic elements such as lead (Pb), cadmium (Cd) and mercury (Hg) was presented by Bush et al. using three different analytical techniques [
19]. Essential elements including calcium (Ca), copper (Cu), iron (Fe), magnesium (Mg), and zinc (Zn) were measured by ICP-OES, heavy metals including cadmium (Cd), manganese (Mn), arsenic (As) and lead (Pb) by GF-AAS, mercury (Hg) by cold vapor AAS and aluminum (Al) by ICP-MS. Prior the measurement, the tissue samples were digested in Teflon vessels at a heating block at 95 °C (203 °F) over 12 h using nitric acid and hydrogen peroxide. The certified reference materials NIST 1577a and NRC Canada DORM-1 were used to determine precision and accuracy. A specialty of this study is the comparison of the measurement of fresh and formalin-fixed tissue samples. No significant influence was reported for the majority of elements measured. Influences were found for calcium (Ca) and magnesium (Mg) from samples in phosphate-buffered formalin solutions. Furthermore, an increasing concentration of aluminum (Al) and a decreasing concentration of manganese (Mn) were observed with an increasing storage time [
19].
The determination of heavy metals in formalin-fixed brain tissue to study neurogenerative disorders was documented by Gellein et al. [
20]. Brain tissue samples with a wet weight of 0.5–1.0 g were freeze-dried until constant weight and digested with 2 mL nitric acid in Teflon vessels using a microwave oven. After appropriate dilution, the analysis was performed using double-focusing magnetic sector field ICP-MS. The results were supported using the certified reference material NIST 1577b (bovine liver). Furthermore, the heavy metal concentrations were determined in fresh unused formalin and in sample storage solutions to study the effects of sample storage. An increasing concentration of the elements measured was documented with increasing storage period over several years. It was concluded that this leaching effect results in too low element concentrations [
20]. Meldrum et al. also describe observed erroneous aluminum (Al) and cobalt (Co) concentrations if the tissue was previously treated using formalin [
21].
The concentrations of cobalt (Co), chromium (Cr), antimony (Sb) and scandium (Sr) were determined in tissues of various organs (heart, kidney, liver and spleen) by Schnabel et al. using radiochemical neutron activation analysis (RNAA) and instrumental neutron activation analysis (INAA) [
17]. Sample weights of 35–75 mg of lyophilized tissues were used. The results are presented in form of concentrations (range of µg/kg) related to the tissue dry weight and show variations between the individual patients and organs [
17]. A study for determining metals in human organ tissue exposed to implant materials was presented by Swiatkowska et al. [
18]. Different measurement techniques and experiments were performed using optical microscopy, laser ablation ICP-MS, synchrotron techniques such as micro X-ray fluorescence (µ-XRF) elemental mapping, and microfocus X-ray absorption spectroscopy (µ-XAS). The results of the different methods were compared to each other [
18].
An experimental setup was developed and presented by Baxmann et al. to examine the susceptibility of hip junctions to fractures, corrosion as well as the release of metal particles and metal ions [
15]. The concentrations of cobalt (Co), chromium (Cr) and titanium (Ti) in the test solutions were determined using ICP-OES and ICP-MS, whereby limits of detection lower than 1 µg/L were reached [
15].
The performance and application forms of ICP-MS in the determination of trace elements in body fluids and tissues, as well as typically appearing interferences, are summarized by Vanhoe et al. [
22,
23]. The ICP-MS is a powerful measurement technique enabling low detection limits, high precision and fast measurement times. Kerger et al. demonstrated the advantages of ICP-MS measurements with interference removal using a dynamic reaction cell and alternatively a collision reaction cell especially for the determination of cobalt (Co) concentrations lower than 5 µg/L [
24,
25]. Furthermore, the authors stated the need for a standardized methodology for metal—especially Co—determination in human tissues using ICP-MS which is up to now not available (blood in particular) [
25].
In conclusion of this literature review, an ICP-MS equipped with a collision reaction cell for interference removal was selected to determine trace metals in human tissue within the scope of this study. The examples from the literature also illustrate the complex sample preparation of tissue samples. In the scope of large studies with a high sample number, manual procedures limit the sample throughput and the accuracy (precision and trueness). Furthermore, human operators work with toxic or harmful chemical reagents. Robot-assisted measurement systems are a promising solution to overcome the limitations of manual sample preparation and to increase the operational safety and health of the laboratory staff. In this study, a measurement procedure was developed for the determination of metal traces in human tissues. The manual process including sample preparation, measurement using ICP-MS, and data evaluation was validated using certified reference material. This process was transferred to a robot-assisted automation system, which was adapted to the special requirements of this application. The automated procedure was also validated using the same reference material, and the results were compared with the manual process. In the last part of this study, metal concentrations were determined in real human tissue samples using the robotic system.
7. Materials and Methods
7.1. Sample Preparation
The tissue samples were dried at 40 °C (104 °F) in a drying chamber UM 400 (Memmert, Schwabach, Germany) until constant weight. The dried tissue was homogenized by milling in ceramic containers using an oscillating ball mill MM 2000 (Retsch, Haan, Germany). The certified reference material NRC-BOVM-1 (Labmix24, Hamminkeln, Germany) was directly used after gentle shaking. Approximately 60 mg of the solid sample were transferred into a microwave vessel Xpress with a total volume of 10 mL (CEM, Kamp-Lintfort, Germany). Nitric acid in suprapure quality (Rotipuran(R)Supra, Carl-Roth, Karlsruhe, Germany) was used as digestion acid. To correct possible vaporization effects during the microwave-assisted acid digestion, an internal standard (ISTD2) Rhenium (Re) (ICP single-element standard, Merck, Darmstadt, Germany) was added to the digestion acid in a concentration of 1 mg/L. After sample processing, the Re concentration is about 80 µg/L in the measurement solution. A volume of 2 mL of the digestion acid with ISTD2 is added to the samples in the microwave digestion vessels. After a rest of 20 min (pre-digestion) with open vessels under the exhaust system, three PTFE agitator balls (diameter 6 mm, Bola, Grünsfeld, Germany) were added to the vessels and the vessels were closed. The microwave digestion was performed using the following parameters: temperature-time ramp to 150 °C (356 °F) in 20 min with a final hold time of 20 min at 150 °C (356 °F) with 100% power of 600W. After cooling down to room temperature, the vessels were opened and the samples dissolved with ultrapure water (1:12.5, v/v).
7.2. Measurement of Aqueous Sample Solutions Using ICP-MS
The calibration was created using the ICP multi-element standard IV and ICP single-element standards of Re, V, Be, As, Mo, Ti and Rb each with an element concentration of 1000 mg/L (Merck, Darmstadt, Germany). The calibration for determining very low concentrations was created using nine calibration standards with element concentrations of 0.01, 0.05, 0.1, 0.5, 1, 5, 10, 50 and 100 µg/L. A typical calibration for the normal ICP-MS working range is created only with five standards of 1, 5, 10, 50 and 100 µg/L. To correct variations in the sample introduction, the internal standard Lu (ISTD 1) with a concentration of 500 µg/L was aspirated by the peristaltic pump, mixed with the sample solution using a T-piece and introduced. The measurements of the diluted sample solutions were performed using an ICP-MS 7700x with the MassHunter 4.4 Workstation Software for 7700 ICP-MS G7201C Version C.01.04 Build 544.3 (Agilent Technologies, Waldbronn, Germany). The following measurement conditions were applied: argon as plasma and nebulizer gas, RF power 1550 W, sample depth 10 mm, nebulizer gas flow 1.05 L/min, nebulizer pump 0.10 rps, spray chamber temperature 13 °C (55.4 °F), collision cell with no helium flow in NoGas tuning mode and 4.3 mL/min helium flow in He tuning mode. Each measurement was performed with three repetitions and the following acquisition parameters: 11B, 27Al and 175Lu (ISTD 1) in NoGas mode with an integration time of 0.1 s (11B, 27Al) and 0.3 s (175Lu) as well as 47Ti, 51V, 52Cr, 55Mn, 58Fe, 60Ni, 63Cu, 66Zn, 75As, 85Rb, 88Sr, 95Mo, 107Ag, 111Cd, 175Lu (ISTD 1), 185Re (ISTD 2), and 206,207,208Pb in He mode with an integration time of 0.3 s. The sample flush time was 10 sec with a pump speed of 0.1 rps. The flushing times between two samples to prevent cross contamination were 55 sec at 0.3 rps with HNO3/HCl (5%/1%, v/v) and 45 sec at 0.4 rps with HNO3 (8%, v/v). The automated sample introduction was performed using the autosampler ASX-500 (Cetac, Omaha, NE, USA).
8. Conclusions
A robot-assisted measurement system is presented for the semi-automated determination of heavy metals in human tissue samples. The manual and the automated measurement processes were similarly validated using certified reference material and the results were compared. The system allows the pre-processing and measurement of a high number of samples with similar precision and trueness compared to manual processing. The total processing time of the automated procedure requires approx. 11% more time than the manual procedure. The system can be further optimized by simultaneous execution of different tasks for several sample batches. During the microwave digestion, the pre-digestion for the next sample batch could take place. This would not reduce the processing time for a sample set, but would allow continuous use of the system. Overall, this would enable a higher sample throughput. In this case, a workflow management system is required that takes over the scheduling of the individual tasks. Another positive effect of automation is, that human operators can take over other tasks in the lab increasing the overall laboratory performance and productivity. Furthermore, the laboratory staff is prevented to work with toxic and harmful chemicals and a high manual workload increasing safety and health.
The manual process was successfully transferred to the automation system and enables the processing of a high sample throughput. Therefore, the semi-automated robot-assisted determination of metals in human tissues may be a powerful driver of the current research into the exploration of negative side effects of implant materials to human health.


 ,
, 










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}