
Diagnostic Accuracy of Serum Hyaluronan for Detecting HCV Infection and Liver Fibrosis in Asymptomatic Blood Donors

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. HCV ELISA, Genotype, and Viral Load in Blood Donors Samples
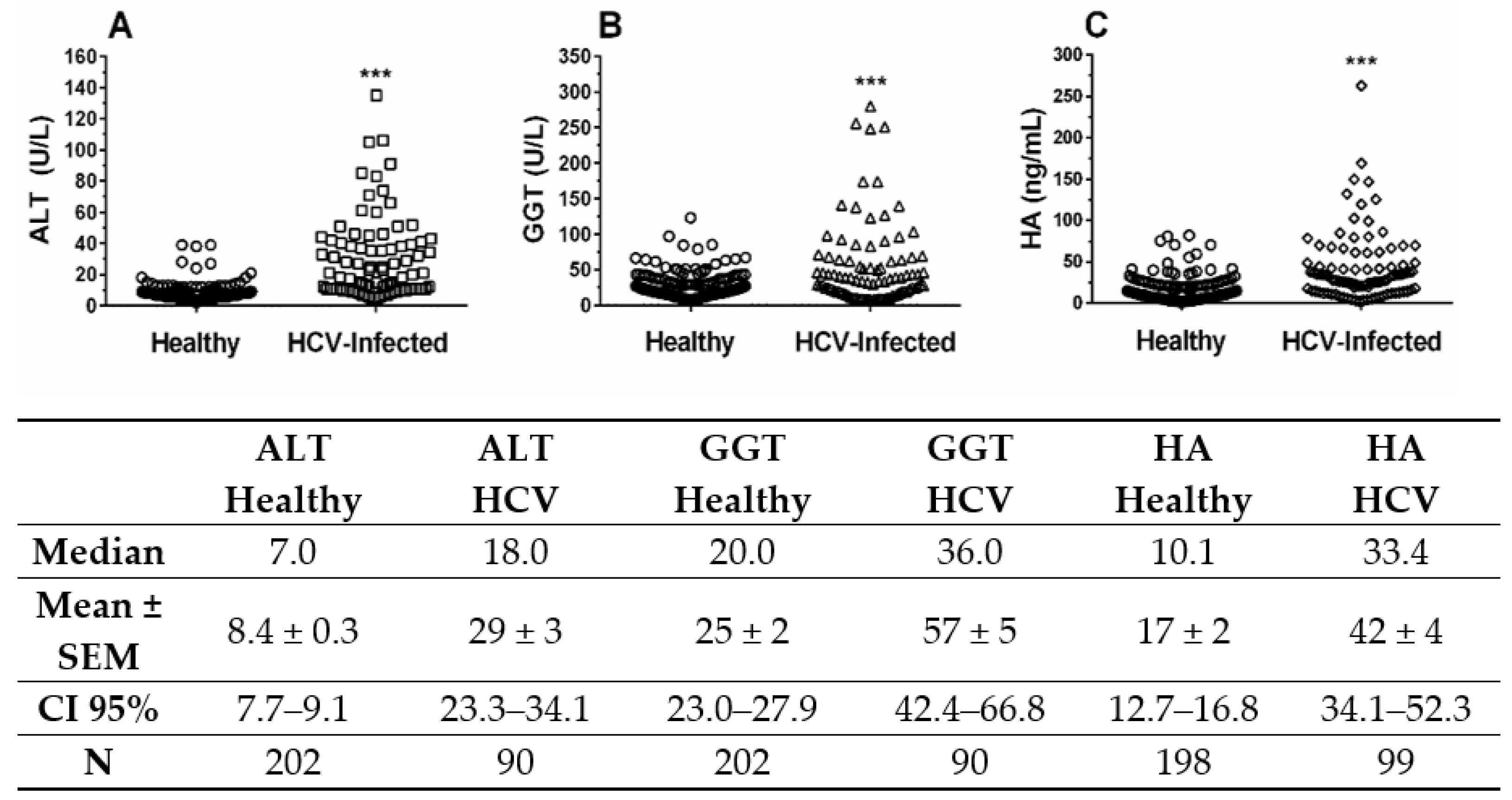
2.2. Liver Biomarkers ALT, GGT, and HA in Blood Donors Infected with HCV
2.3. Hyaluronic Acid Serum Level Is Associated with Antibody Titers Anti-HCV
2.4. Correlation between HA and Liver Enzymes in HCV-Infected Blood Donors
2.5. Analysis of Diagnostic Parameters of HA, ALT and GGT by ROC Curves
3. Discussion
4. Materials and Methods
4.1. Serum Samples
4.2. HCV-ELISA Tests
4.3. HCV-RNA Assays
4.4. Liver Biomarks ALT, GGT and HA Assays
4.5. Determination of Liver Fibrosis
4.6. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Sample Availability
References
- Hajarizadeh, B.; Grebely, J.; Dore, G.J. Epidemiology and natural history of HCV infection. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 553–562. [Google Scholar] [CrossRef]
- Paternostro, C.; David, E.; Novo, E.; Parola, M. Hypoxia, angiogenesis and liver fibrogenesis in the progression of chronic liver diseases. World J. Gastroenterol. 2010, 16, 281–288. [Google Scholar] [CrossRef]
- Andrade, Z.A. Regression of hepatic fibrosis. Rev. Soc. Bras. Med. Trop. 2005, 38, 514–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orlent, H.; Vrolijk, J.M.; Veldt, B.J.; Schalm, S.W. Hepatitis C 2002 guidelines: Summary and annotations. Scand. J. Gastroenterol. Suppl. 2003, 239, 105–110. [Google Scholar]
- Kelleher, T.B.; Mehta, S.H.; Bhaskar, R.; Sulkowski, M.; Astemborski, J.; Thomas, D.L.; Moore, R.E.; Afdhal, N.H. Prediction of hepatic fibrosis in HIV/HCV co-infected patients using serum fibrosis markers: The SHASTA index. J. Hepatol. 2005, 43, 78–84. [Google Scholar] [CrossRef]
- Micheloud, D.; Salcedo, M.; Bañares, R.; Rincón, D.; Lorente, R.; Muñoz-Fernández, M.A.; Resino, S. Serum levels of fibrosis biomarkers measured early after liver transplantation are associated with severe hepatitis C virus recurrence. Transpl. Infect. Dis. 2009, 11, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Pungpapong, S.; Nunes, D.P.; Krishna, M.; Nakhleh, R.; Chambers, K.; Ghabril, M.; Dickson, R.C.; Hughes, C.B.; Steers, J.; Nguyen, J.H.; et al. Serum fibrosis markers can predict rapid fibrosis progression after liver transplantation for hepatitis C. Liver Transpl. 2008, 14, 1294–1302. [Google Scholar] [CrossRef]
- Miyazaki, T.; Honda, A.; Ikegami, T.; Hara, T.; Saitoh, Y.; Hirayama, T.; Doy, M.; Matsuzaki, Y. The associated markers and their limitations for the primary screening of HCV carriers in public health examination. Hepatol. Res. 2009, 39, 664–674. [Google Scholar] [CrossRef]
- Wai, C.T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [Green Version]
- Fujii, H.; Enomoto, M.; Fukushima, W.; Ohfuji, S.; Mori, M.; Kobayashi, S.; Iwai, S.; Morikawa, H.; Tamori, A.; Sakaguchi, H.; et al. Noninvasive laboratory tests proposed for predicting cirrhosis in patients with chronic hepatitis C are also useful in patients with non-alcoholic steatohepatitis. J. Gastroenterol. 2009, 44, 608–614. [Google Scholar] [CrossRef]
- Souza, J.F.; Longui, C.A.; Miorin, L.A.; Sens, Y.A. Gamma-glutamyltransferase activity in chronic dialysis patients and renal transplant recipients with hepatitis C virus infection. Transpl. Proc. 2008, 40, 1319–1323. [Google Scholar] [CrossRef]
- Soresi, M.; Tripi, S.; Franco, V.; Giannitrapani, L.; Alessandri, A.; Rappa, F.; Vuturo, O.; Montalto, G. Impact of liver steatosis on the antiviral response in the hepatitis C virus-associated chronic hepatitis. Liver Int. 2006, 26, 1119–1125. [Google Scholar] [CrossRef]
- Camacho, V.R.; Silveira, T.R.; Oliveira, J.R.; Barros, S.G.; Cerski, C.T. Relationship between serum concentration of type III procollagen, hyaluronan acid and histopathological findings in the liver of HCV-positive blood donors. Arq. Gastroenterol. 2007, 44, 118–122. [Google Scholar] [CrossRef] [Green Version]
- Santos, V.N.; Leite-Mor, M.M.; Kondo, M.; Martins, J.R.; Nader, H.B.; Lanzoni, V.P.; Parise, E.R. Serum laminin, type IV, collagen and hyaluronan as fibrosis markers in non-alcoholic fatty liver disease. Braz. J. Med. Biol. Res. 2005, 38, 747–753. [Google Scholar] [CrossRef] [Green Version]
- Sanvisens, A.; Serra, I.; Tural, C.; Tor, J.; Ojanguren, I.; Barluenga, E.; Rey-Joly, C.; Clotet, B.; Muga, R. Hyaluronic acid, transforming growth factor-beta1 and hepatic fibrosis in patients with chronic hepatitis C virus and human immunodeficiency virus co-infection. J. Viral. Hepat. 2009, 16, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Guéchot, J.; Loria, A.; Serfaty, L.; Giral, P.; Giboudeau, J.; Poupon, R. Serum hyaluronan as a marker of liver fibrosis in chronic viral hepatitis C: Effect of alpha-interferon therapy. J. Hepatol. 1995, 22, 22–26. [Google Scholar] [CrossRef]
- Parise, E.R.; Oliveira, A.C.; Figueiredo-Mendes, C.; Lanzoni, V.; Martins, J.R.M.; Nader, H.B.; Ferraz, M.L. Noninvasive serum markers in the diagnosis of structural liver damage in chronic hepatitis C virus infection. Liver Int. 2006, 26, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- Plevris, J.N.; Haydon, G.H.; Simpson, K.J.; Dawkes, R.; Ludlum, C.A.; Harrison, D.J.; Hayes, P.C. Serum hyaluronan -a non-invasive test for diagnosing liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2000, 12, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.; Liang, J.; Noble, P.W. Hyaluronan in tissue injury and repair. Annu. Rev. Cell Dev. Biol. 2007, 23, 435–461. [Google Scholar] [CrossRef] [Green Version]
- Noble, P.W. Hyaluronan and its catabolic products in tissue injury and repair. Matrix. Biol. 2002, 21, 25–29. [Google Scholar] [CrossRef]
- Ogata, T.; Okuda, K.; Ueno, T.; Saito, N.; Aoyagi, S. Serum hyaluronan as a predictor of hepatic regeneration after hepatectomy in humans. Eur. J. Clin. Investig. 1999, 29, 780–785. [Google Scholar] [CrossRef]
- Yang, Y.M.; Noureddin, M.; Liu, C.; Ohashi, K.; Kim, S.Y.; Ramnath, D.; Powell, E.E.; Sweet, M.J.; Roh, Y.S.; Hsin, I.F.; et al. Hyaluronan synthase 2-mediated hyaluronan production mediates Notch1 activation and liver fibrosis. Sci. Transl. Med. 2019, 11, eaat9284. [Google Scholar] [CrossRef]
- Kim, H.C.; Nam, C.M.; Jee, S.H.; Han, K.H.; Oh, D.K.; Suh, I. Normal serum aminotransferase concentration and risk of mortality from liver diseases: Prospective cohort study. BMJ 2004, 328, 983–988. [Google Scholar] [PubMed] [Green Version]
- Wedemeyer, H.; Hofmann, W.P.; Lueth, S.; Malinski, P.; Thimme, R.; Tacke, F.; Wiegand, J. ALT screening for chronic liver diseases: Scrutinizing the evidence. Z. Gastroenterol. 2010, 48, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Alter, M.J. Epidemiology of hepatitis C virus infection. World J. Gastroenterol. 2007, 13, 2436–2441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irving, W.L.; Brown, R.J.P. Acute hepatitis C virus infection: A dynamic-and challenging concept. J. Infect. Dis. 2010, 202, 1765–1767. [Google Scholar] [CrossRef] [PubMed]
- Contreras, A.M.; Ochoa-Jiménez, R.J.; Celis, A.; Méndez, C.; Olivares, L.; Rebolledo, C.E.; Hernandez-Lugo, I.; Aguirre-Zavala, A.I.; Jiménez-Mendes, R.; Chung, R.T. High antibody level: An accurate serologic marker of viremia in asymptomatic people with hepatitis C infection. Transfusion 2010, 50, 1335–1343. [Google Scholar] [CrossRef]
- Kim, W.R. Global epidemiology and burden of hepatitis C. Microbes Infect. 2002, 4, 1219–1225. [Google Scholar] [CrossRef]
- Husereau, D.; Bassert, K.; Koretz, R. Interferon-based therapies for chronic hepatitis C infection: An assessment of clinical outcomes. Can Agency Drugs Technol. Health 2004. Available online: http://www.cadth.ca/media/pdf/171_hepc_tr_e.pdf (accessed on 12 May 2020).
- Junior, F.L.G.; Stucchi, R.S.; Pavan, M.H.; Papaiordanou, P.M.; Goncalves, N.S.; Pinho, J.R. Elevated alanine aminotransferase in Brazilian blood donors. Transfusion 1988, 38, 416. [Google Scholar] [CrossRef]
- Nascimento, M.C.; Mayaud, P.; Sabino, E.C.; Torres, K.L.; Franceschi, S. Prevalence of hepatitis B and C serological markers among first-time blood donors in Brazil: A multi-center serosurvey. J. Med. Virol. 2008, 80, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, G.L.; Wasley, A.; Simard, E.P.; McQuillan, G.M.; Kuhnert, W.L.; Alter, M.J. The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann. Intern. Med. 2006, 144, 705–714. [Google Scholar] [CrossRef]
- Mutimer, D.J.; Harrison, R.F.; O’Donnell, K.B.; Shaw, J.; Martin, B.A.; Atrah, H.; Ala, F.A.; Skidmore, S.; Hubscher, S.G.; Neuberger, J.M. Hepatitis C virus infection in the asymptomatic British blood donor. J. Viral. Hepatol. 1995, 2, 47–53. [Google Scholar] [CrossRef]
- World Health Organization. Hepatitis C—Revised October 2000; World Health Organization: Geneva, Switzerland, 2000; (Fact Sheet, 164); Available online: http://www.who.int/mediacentre/factsheets/fs164/en/in-dex.html (accessed on 8 May 2020).
- Martins, R.M.; Teles, S.A.; Freitas, N.R.; Motta-Castro, A.R.; Souto, F.J.; Mussi, A.; Amorim, R.M.; Martins, C.R. Distribution of hepatitis C virus genotypes among blood donors from mid-west region of Brazil. Rev. Inst. Med. Trop. São Paulo 2006, 48, 53–55. [Google Scholar] [CrossRef] [Green Version]
- Silva, G.F.; Nishimura, N.F.; Coelho, K.I.; Soares, E.C. Grading and staging chronic hepatitis C and its relation to genotypes and epidemiological factors in Brazilian blood donors. Braz. J. Infect. Dis. 2005, 9, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Imbert-Bismut, F.; Ratziu, V.; Pieroni, L.; Charlotte, F.; Benhamou, Y.; Poynard, T. Biochemical markers of liver fibrosis in patients with hepatitis C virus infection: A prospective study. Lancet 2001, 357, 1069–1075. [Google Scholar] [CrossRef]
- Poynard, T.; Imbert-Bismut, F.; Ratziu, V.; Chevret, S.; Jardel, C.; Moussalli, J.; Messous, D.; Degos, F. GERMED cyt04 group. Biochemical markers of liver fibrosis in patients infected by hepatitis C virus: Longitudinal validation in a randomized trial. J. Viral. Hepat. 2002, 9, 128–133. [Google Scholar] [CrossRef]
- Alberti, A.; Noventa, F.; Benvegnu, L.; Boccato, S.; Gatta, A. Prevalence of liver disease in a population of asymptomatic persons with hepatitis C virus infection. Ann. Intern. Med. 2002, 137, 961–964. [Google Scholar] [CrossRef]
- Pradat, P.; Alberti, A.; Poynard, T.; Esteban, J.I.; Weiland, O.; Marcellin, P.; Badalamenti, S.; Trepo, C. Predictive value of ALT levels for histological findings in chronic hepatitis C: A European collaborative study. Hepatology 2002, 36, 973–977. [Google Scholar]
- Hui, C.K.; Belaye, T.; Montegrande, K.; Wright, T.L. A comparison in the progression of liver fibrosis in chronic hepatitis C between persistently normal and elevated transaminase. J. Hepatol. 2003, 38, 511–517. [Google Scholar] [CrossRef]
- Engelmann, G. Biomarkers in Focus: Alanine Aminotransferase. In Biomarkers in Liver Disease. Biomarkers in Disease: Methods, Discoveries and Applications; Springer: Berlin, Germany, 2017. [Google Scholar]
- Ruhl, C.E.; Everhart, J.E. Upper limits of normal alanine aminotransferase activity in the United States population. Hepatology 2012, 55, 447–454. [Google Scholar] [CrossRef] [Green Version]
- Rockey, D.C.; Bissell, D.M. Noninvasive measures of liver fibrosis. Hepatology 2006, 43, S113–S120. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; Ploutz-Snyder, R.; Nanti, J.; Rawlins, S.R.; Sanderson, S.O.; Levine, R.A. Diagnostic accuracy of serum hyaluronic acid, FIBRO Spect II, and YKL-40 for discriminating fibrosis stages in chronic Hepatitis C. Am. J. Gastroenterol. 2008, 103, 928–936. [Google Scholar] [CrossRef]
- McHutchison, J.G.; Blatt, L.M.; de Medina, M.; Craig, J.R.; Conrad, A.; Schiff, E.R.; Tong, M.J. Measurement of serum hyaluronic acid in patients with chronic hepatitis C and its relationship to liver histology. Consensus Interferon Study Group. J. Gastroenterol. Hepatol. 2000, 15, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Nunes, D.; Fleming, C.; Offner, G.; Craven, D.; Fix, O.; Heeren, T.; Koziel, M.J.; Graham, C.; Tumilty, S.; Skolnik, P.; et al. Noninvasive markers of liver fibrosis are highly predictive of liver-related death in a cohort of HCV-infected individuals with and without HIV infection. Am. J. Gastroenterol. 2010, 105, 1346–1353. [Google Scholar] [CrossRef] [PubMed]
- Peters, L.; Neuhaus, J.; Mocroft, A.; Soriano, V.; Rockstroh, J.; Dore, G.; Puoti, M.; Tedaldi, E.; Clotet, B.; Kupfer, B.; et al. Hyaluronic acid levels predict increased risk of non-AIDS death in hepatitis-coinfected persons interrupting antiretroviral therapy in the SMART Study. Antivir. Ther. 2011, 16, 667–675. [Google Scholar] [PubMed] [Green Version]
- Hansen, J.F.; Christiansen, K.M.; Staugaard, B.; Moessner, B.K.; Lillevang, S.; Krag, A.; Christensen, P.B. Combining liver stiffness with hyaluronic acid provides superior prognostic performance in chronic hepatitis C. PLoS ONE 2019, 14, e0212036. [Google Scholar] [CrossRef]
- Tamaki, S.; Ueno, T.; Torimura, T.; Sata, M.; Tanikawa, K. Evaluation of hyaluronic acid binding ability of hepatic sinusoidal endothelial cells in rats with liver cirrhosis. Gastroenterology 1996, 111, 1049–1057. [Google Scholar] [CrossRef]
- Chan, S.W.; McOmish, F.; Holmes, E.C.; Dow, B.; Peutherer, J.F.; Follett, E.; Yap, P.L.; Simmonds, P. Analysis of a new hepatitis C virus type and its phylogenetic relationship to existing variants. J. Gen. Virol. 1992, 73, 1131–1141. [Google Scholar] [CrossRef] [PubMed]
- Davidson, F.; Simmonds, P.; Ferguson, J.C.; Jarvis, L.M.; Dow, B.C.; Follett, E.A.C.; Seed, C.R.G.; Krusius, T.; Lin, C.; Medgyesi, G.A.; et al. Survey of major genotypes and subtypes of hepatitis C virus using RFLP of sequences amplified from the 5′ non-coding region. J. Gen. Virol. 1995, 76, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- McOmish, F.; Yap, P.L.; Dow, B.C.; Follett, E.A.; Seed, C.; Keller, A.J.; Cobain, T.J.; Krusius, T.; Kolho, E.; Naukkarinen, R. Geographical distribution of hepatitis C virus genotypes in blood donors: An international collaborative survey. J. Clin. Microbiol. 1994, 32, 884–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albertoni, G.; Arnoni, C.P.; Araújo, P.R.; Carvalho, F.O.; Barreto, J.A. Signal to cut-off (S/CO) ratio and detection of HCV genotype 1 by real-time PCR one-step method: Is there any direct relationship? Braz. J. Infect. Dis. 2010, 14, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Martins, J.R.; Passerotti, C.C.; Maciel, J.R.M.; Sampaio, L.O.; Dietrich, C.P.; Nader, H.B. Practical determination of hyaluronan by a new noncompetitive fluorescence-based assay on serum of normal and cirrhotic patients. Anal. Biochem. 2003, 319, 65–72. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody Titers | HCV-RNA Positive | HCV-RNA Negative | |
|---|---|---|---|
| OD >16 | 96 | 29 | PPV = 96/125 (76.8%) |
| OD ≤ 16 | 03 | 180 | NPV = 180/183 (98.4%) |
| Sensitivity = 96/99 (97.0%) | Specificity = 180/209 (86.1%) | Total = 308 |
| HA (ng/mL) | HCV-RNA Positive and ALT ≥ 40 U/L | HCV-RNA Negative and ALT < 40 U/L | |
|---|---|---|---|
| HA ≥ 34.2 | 24 | 20 | PPV = 24/44 (55%) |
| HA < 34.2 | 01 | 184 | NPV = 184/185 (99.5%) |
| Sensitivity = 24/25 (96%) | Specificity = 184/204 (90%) | Total = 229 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodart, I.F.; Pares, M.M.; Mendes, A.; Accardo, C.M.; Martins, J.R.M.; Silva, C.B.; Carvalho, F.O.; Barreto, J.A.; Reis, M.G.; Tersariol, I.L.S.; et al. Diagnostic Accuracy of Serum Hyaluronan for Detecting HCV Infection and Liver Fibrosis in Asymptomatic Blood Donors. Molecules 2021, 26, 3892. https://doi.org/10.3390/molecules26133892
Rodart IF, Pares MM, Mendes A, Accardo CM, Martins JRM, Silva CB, Carvalho FO, Barreto JA, Reis MG, Tersariol ILS, et al. Diagnostic Accuracy of Serum Hyaluronan for Detecting HCV Infection and Liver Fibrosis in Asymptomatic Blood Donors. Molecules. 2021; 26(13):3892. https://doi.org/10.3390/molecules26133892
Chicago/Turabian StyleRodart, Itatiana F., Madalena M. Pares, Aline Mendes, Camila M. Accardo, João R. M. Martins, Cleidenice B. Silva, Fabrício O. Carvalho, José A. Barreto, Mitermayer G. Reis, Ivarne L. S. Tersariol, and et al. 2021. "Diagnostic Accuracy of Serum Hyaluronan for Detecting HCV Infection and Liver Fibrosis in Asymptomatic Blood Donors" Molecules 26, no. 13: 3892. https://doi.org/10.3390/molecules26133892
APA StyleRodart, I. F., Pares, M. M., Mendes, A., Accardo, C. M., Martins, J. R. M., Silva, C. B., Carvalho, F. O., Barreto, J. A., Reis, M. G., Tersariol, I. L. S., & Nader, H. B. (2021). Diagnostic Accuracy of Serum Hyaluronan for Detecting HCV Infection and Liver Fibrosis in Asymptomatic Blood Donors. Molecules, 26(13), 3892. https://doi.org/10.3390/molecules26133892