1. Introduction
Cancer is the world’s second major cause of death among males and females. This reflects ~9.6 million deaths in 2018 (~13% of all deaths). Cancer deaths worldwide are expected to increase significantly, with ~13.1 million deaths in 2030 [
1]. According to many reported studies, cancer is a growing problem [
2,
3,
4] and therefore it continues to spread worldwide, with a tremendous burden on individuals, families, communities and healthcare systems, both mentally and socially [
5]. The majority of health care systems in developed countries are little prepared to deal with this challenge, and many cancer patients globally will not have the privilege of early treatment. In these countries, nearly two-thirds of cancer patients die [
6]. There is evidence that shows that in countries where national health services are well-developed, strategies such as early detection, treatment and survivorship care are improving the survival rates of many types of cancers [
1,
6].
There are a number of treatment options for cancer such as surgery, radiation therapy and/or chemotherapy. For treating localized cancers, radiation therapy and surgery are preferred, while chemotherapy is considered safe for systemic cancers. Although chemotherapeutic agents exert their cytotoxic effect by way of interfering with the synthesis or the function of proteins and other needed cellular biomolecules, they also attack RNA, DNA and other vital proteins. Consequently, one must be careful when administering chemotherapy, as it has major side/toxic effects since it is capable of killing cells. A perfect recorded chemotherapy would be highly selective and specific to sick or cancerous tissues, while leaving healthy ones untouched. Unsurprisingly, the reality always differs from expectations, as most chemotherapies are heavily toxic, particularly for short-lived cells [
7].
Recent developments in life science research in recent years have led to increased understanding of signaling transductions in tumor cells, apoptosis triggering, cellular interactions and other critical processes [
8]. In addition, these chemotherapeutic drugs may be highly selective for DNA and other cellular targets that present in cancer cells as well as normal cells. The use of major intracellular signal transduction enzymes relevant to the differentiation and spread of cancer cells as drug testing objectives has become a hot area for medical research and development of antitumor drugs, and the continued improvement of effective, safe and specific new targeted anticancer drugs [
9].
Tyrosine kinase (TK) is an enzyme that is responsible for transferring phosphate group from adenosine triphosphate (ATP) to the tyrosine residues of certain proteins inside the living cell [
10]. An abnormality in TK could lead to a series of body diseases. Earlier investigations have demonstrated that there are TK activities for more than half of mutated proto-oncogenes and oncogenes, and the irregular expression of these genes can contribute to abnormal cell proliferation and eventually cancer [
11]. Additionally, in conjunction with tumorigenesis, neovascularization and chemotherapy resistance, an abnormal expression of TK has been observed [
12]. For that reason, targeting TK has attracted even more interest for the pharmaceutical industry for developing new chemotherapeutic drugs. Researchers and pharmaceutical organizations have been given high priority to developing tyrosine kinase inhibitors (TKIs) that may affect unique molecular pathways [
13]. In 2001, the Food and Drug Administration (FDA) quickly approved the first targeted TKI drug imatinib and stimulated new energetic thought to cancer treatment [
14,
15,
16]. To date, the FDA has approved over 20 TKI drugs [
17]. These drugs are characterized by high effectiveness and low drawbacks and dominate the management of various types of cancer [
10,
11,
12,
13,
14,
15,
16,
17] compared to traditional cytotoxic antinineoplastics, some of which have become the foremost cancer treatment. The safety and efficacy of TKI medications is principally based on their corresponding pharmaceutical formulation quality, including drug content and uniformity.
For the quality control (QC) of TKIs, it is absolutely necessary to use proper analytical techniques. The analytical methods mentioned in the literature for QC of TKIs in their dosage forms are HPLC and HPTLC [
18,
19,
20,
21,
22,
23,
24,
25,
26,
27], voltammetry [
28], spectrofluorometry [
29,
30,
31,
32] and spectrophotometry [
33,
34,
35,
36,
37,
38,
39,
40,
41,
42,
43,
44]. The most accessible methodology is spectrophotometry, which is quite easy, the least expensive and available in most quality control laboratories. Nevertheless, almost all of these spectrophotometric assays for TKIs are based on measurements of native UV absorption, which are not selective [
33,
34,
35,
36,
37,
38,
39]. Few visible-spectrophotometric methodologies with varying chromogenic reagents have been developed for assaying TKIs [
40,
41,
42,
43,
44]. Even worse, these methods incorporate laborious extraction steps and utilize large volumes of toxic organic solvents [
45,
46,
47,
48]. Furthermore, due to the differences in chemical structures of analyzed TKIs, these assays were individually developed. Besides, these assays have limitations regarding throughput, as they use traditional spectrophotometry.
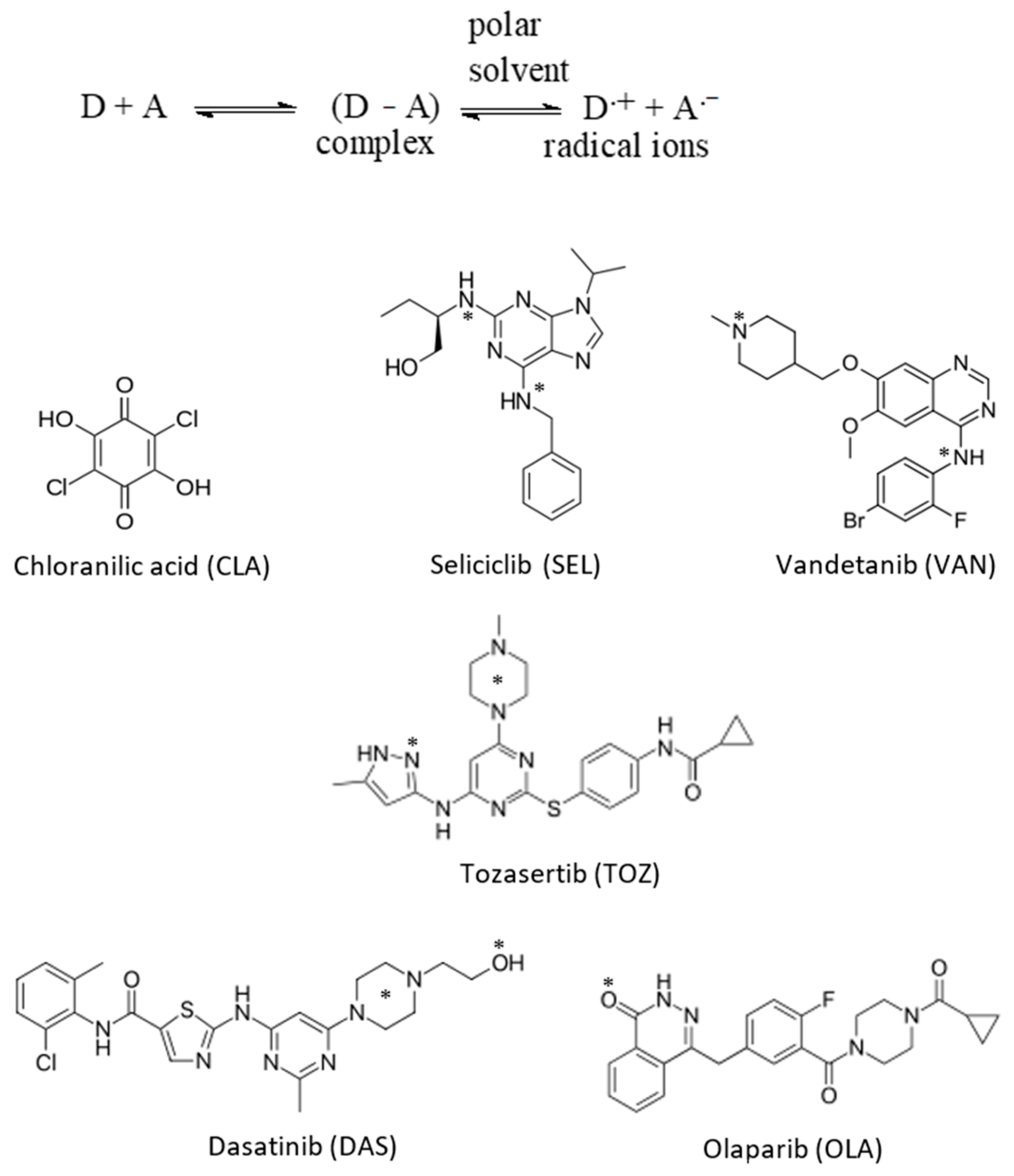
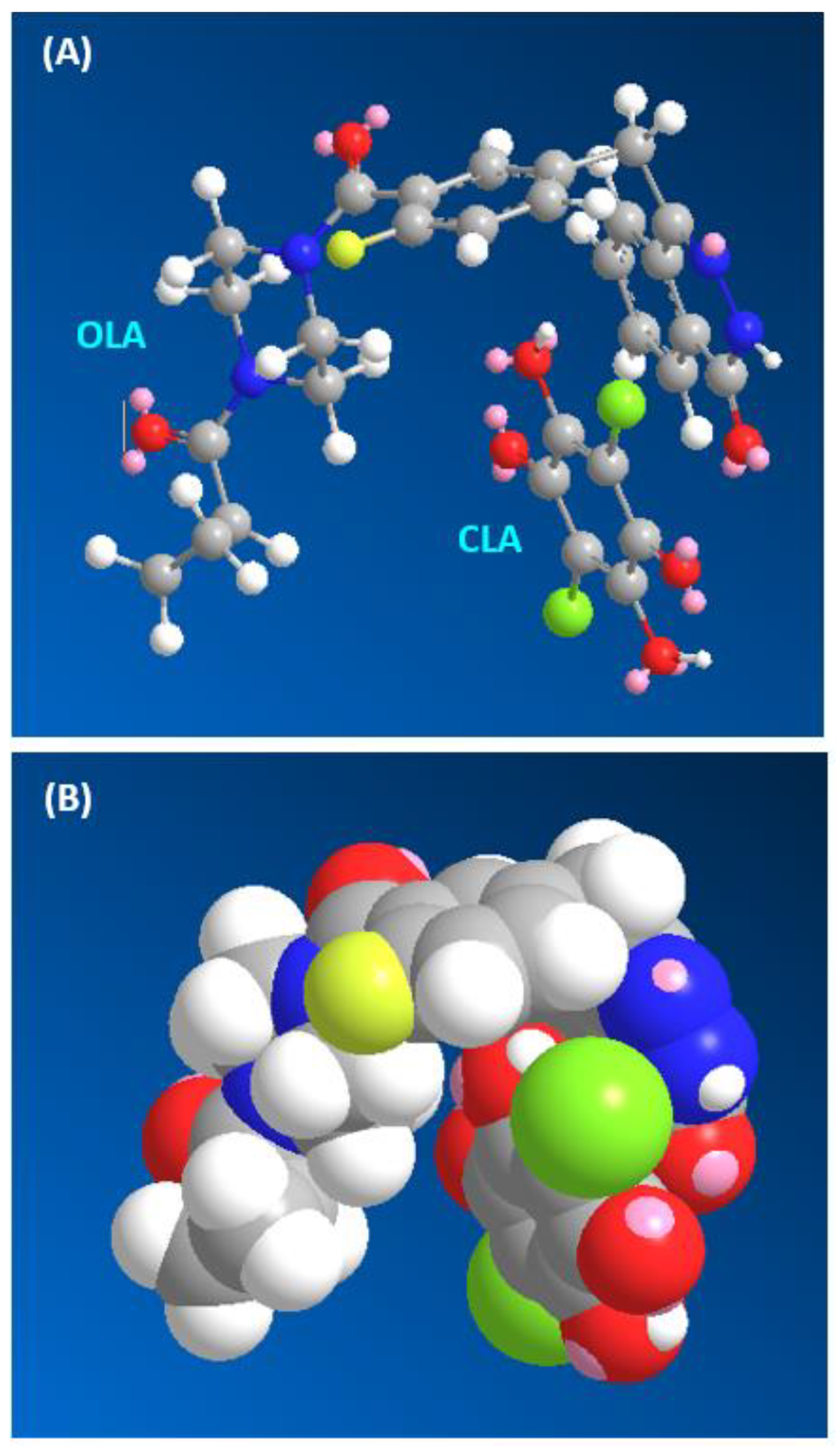
From the presented information, establishing a universal spectrophotometric method for assaying any TKI irrespective of its chemical structure would be of great benefit and convenience. This research is directed to establish a novel 96-microwell-based spectrophotometric assay (MW-SPA) that could be applied in QC laboratories for reliable and accurate determination of any TKI. The proposed approach is based on formation of charge-transfer complexes (CTCs) between TKIs and chloranilic acid (CLA). The proposed procedure was established and validated for five TKIs. These TKIs were seliciclib (SEL), vandetanib (VAN), tozasertib (TOZ), dasatinib (DAS) and olaparib (OLA); their chemical structures are given in
Figure 1. Their chemical names, molecular formulae and molecular weights are given in
Table 1.
3. Experimental
3.1. Apparatus
A double beam ultraviolet–visible spectrophotometer with matched 1-cm quartz cells (UV-1800, Shimadzu Co. Ltd., Kyoto, Japan) was operated for the scanning of all the generated UV–visible spectra. An absorbance microplate reader (ELx808: Bio-Tek Instruments Inc., Winooski, VT, USA) powered by KC Junior software provided with the instrument was used.
3.2. Chemicals and Materials
All the investigated TKIs were procured from LC Laboratories (Woburn, MA, USA) and Weihua Pharma Co. Limited (Hangzhou, Zhejiang, China) and utilized as provided. Their purity was >99% (as claimed by the providing companies), and their solutions remained stable for at least 7 days under refrigeration. CLA was bought from BDH Chemicals Co. (Langenfeld, Germany). Transparent 96-microwell plates were procured from Corning/Costar Inc (Cambridge, USA). Adjus
Table 8-channel pipettes were obtained from Sigma-Aldrich Chemicals Co (St. Louis, Missouri, USA). BRAND
® PP reagent tanks with lids for the pipettes were acquired from Merck KGaA (Darmstadt, Germany). The other reagents and solvents were of analytical grade (Fisher Scientific, California, CA, USA). The pharmaceutical formulations were caprelsa tablets (AstraZeneca, Cambridge, United Kingdom) labelled to contain 300 mg of VAN; sprycel tablets (Bristol Myers Squibb, New York, NY, USA) labelled to contain 50 mg DAS per tablet; and lynparza tablets (AstraZeneca, Cambridge, United Kingdom) labelled to contain 150 mg OLA per tablet. Laboratory-made tablets were prepared in the lab by combining individually accurate amounts (100 mg) of TOZ and SEL with 25 mg of each of starch, lactose monohydrate, microcrystalline cellulose and hydroxypropyl cellulose.
3.3. Preparation of TKIs Standard Solutions
Stock solutions of 5 mg/mL of SEL, VAN and OLA were obtained by dissolving 50 mg of the standard material in 10 mL of methanol, while 0.5 mg/mL of DAS and TOZ solutions were made by dissolving 5 mg of the standard material in 10 mL of methanol. These above-mentioned stock solutions were found to be stable over a period of 14 days when stored in the refrigerator.
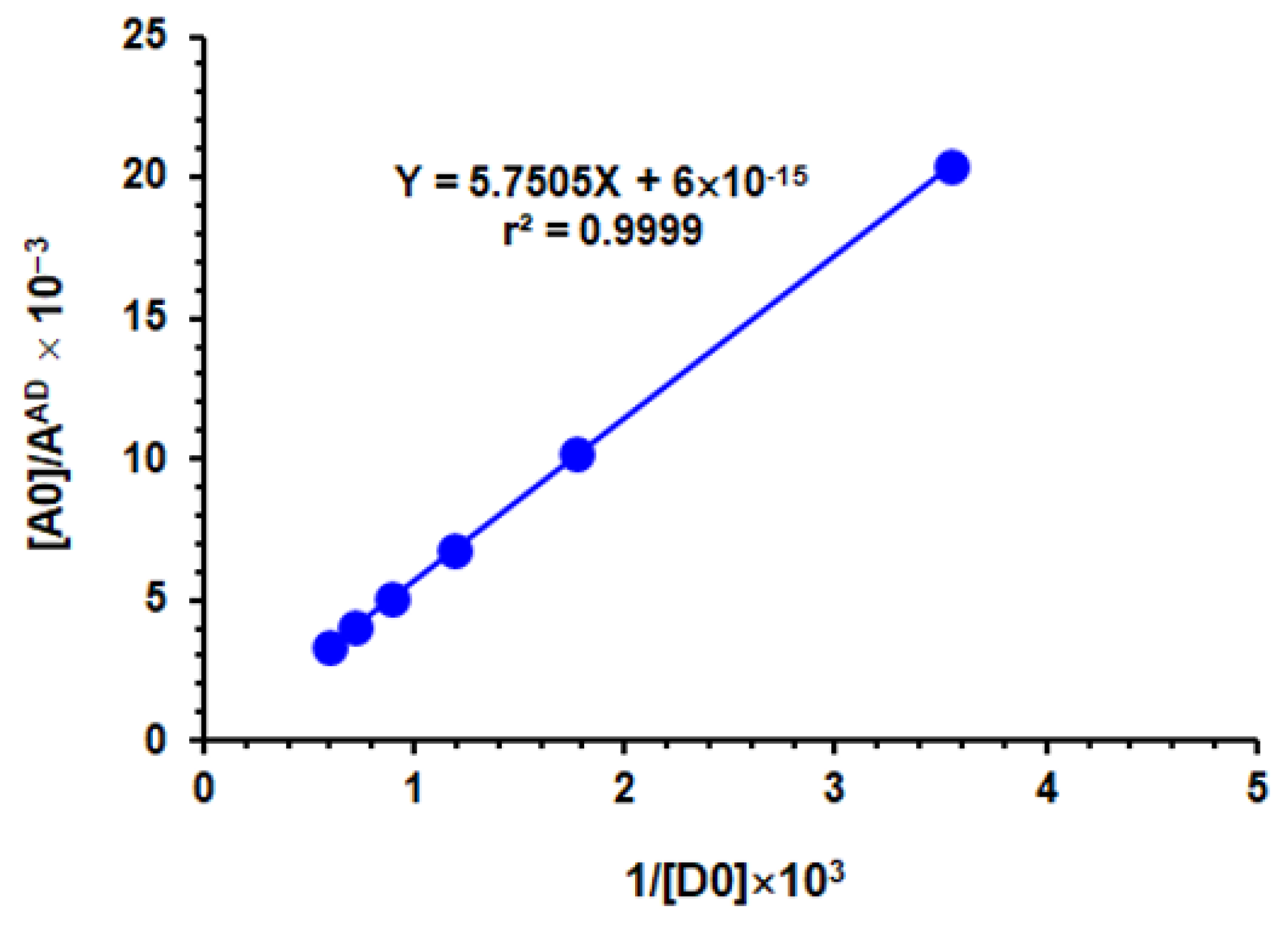
3.4. Determination of Association Constants
A set of TKI solutions ranging from 1.79 × 10
−4 to 1.85 × 10
−3 M were swirled with a constant CLA concentration (4.8 × 10
−3 M). The reaction was instant at room temperature (25 ± 2 °C). The absorbances of the colored solutions were recorded at their absorption peaks against exactly prepared reagent blanks. The measured absorbances were utilized to produce the plot of Benesi–Hildebrand [
58] by plotting the values [A
0]/A
AD versus l/[D
0]. Linear regression analysis was shown for the data using the following Benesi–Hildebrand equation [
60]:
where [A
0] represents the CLA molar concentration (the acceptor); [D
0] represents TKI molar concentration (the donor); A
AD represents the absorbance of the CTC reaction mixture formed; ε
AD represents the molar absorptivity of the CTC; and
KcAD represents the formation constant of the complex (L mol
−1). The intercept of the linear fitting equation was equivalent to 1/ε
AD, and the formation constant was calculated from the derived value of ε
AD in addition to the slope of the equation.
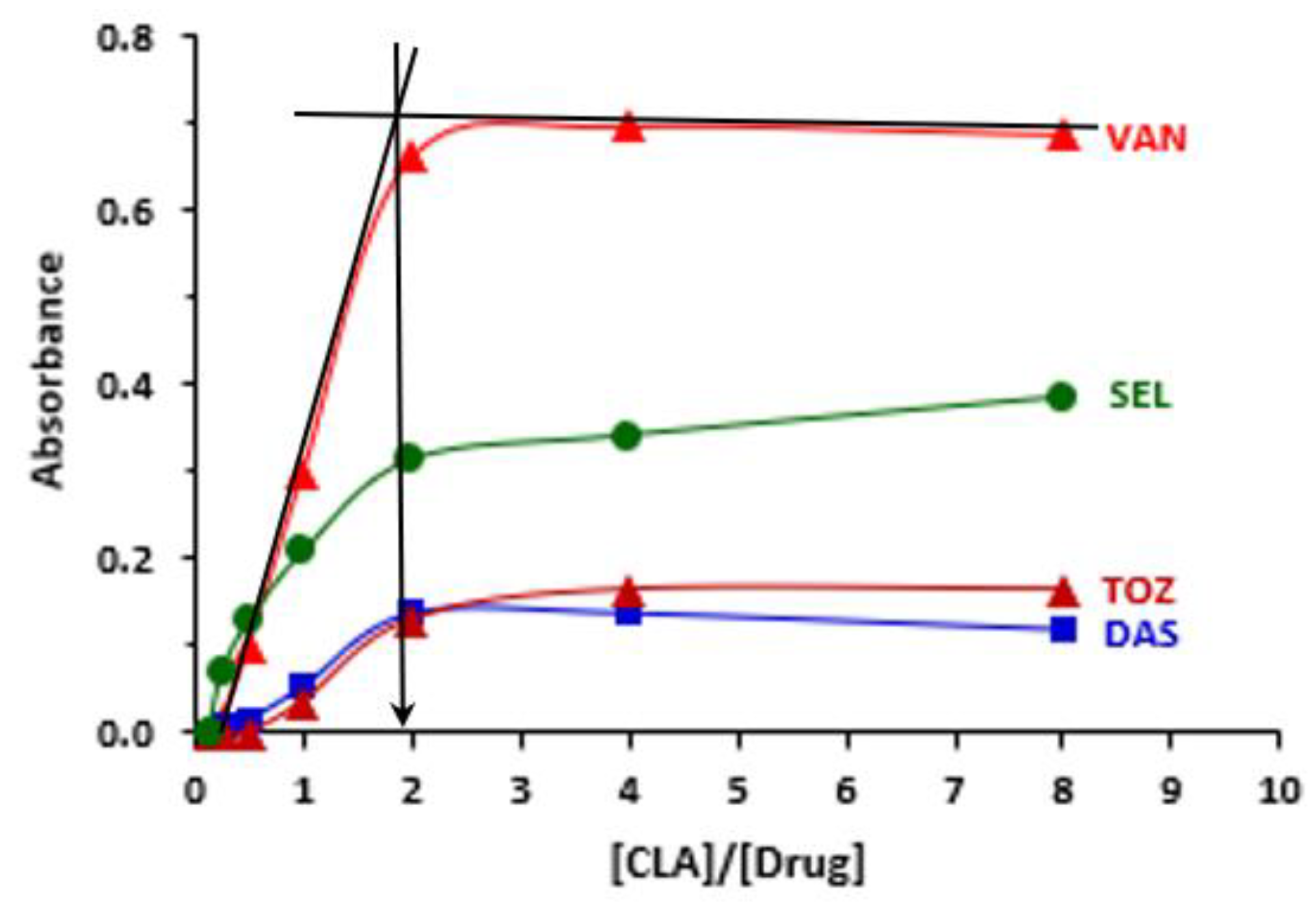
3.5. Determination of CLA:TKI Molar Ratio
The spectrophotometric titration methods were applied in the current work [
61]. Principal solutions of the investigated TKIs (2.5 × 10
−3 M) and CLA (2 × 10
−2 M) were readily prepared (i.e., molar concentration of CLA was 8 times bigger than that of TKI). Exceptionally, PEL concentration was (1 × 10
−3 M) and that of CLA was 8 × 10
−3 M. A set of master solutions of both the investigated TKIs and CLA were made to give molar ratios of TKI:CLA of 0.25:8. These solutions were always composed of constant TKI concentrations. The temperature was 25 ± 2 °C, and the corrected absorbances of the products were measured at 490 nm (after subtracting the readings of blanks that were treated similarly but using methanol instead of the sample) A graph was drawn by plotting the corrected measured absorbances versus the TKI:CLA molar ratio. From this graph, the molar ratio of the reaction was computed. The mole ratio corresponds to the point of intersection of the tangents of straight-line portions of the plots.
3.6. Preparation of TKI Tablets Solutions
The total amount of commercialized or synthetic tablets accounting for 50 mg of TKI (5 mg was used in case of DAS and TOZ) was placed in a 10-mL measuring flask, dissolved in a volume of 5 mL methanol, mixed thoroughly and sonicated for 5 min, completed to the mark with methanol, well shaken for 10 min and then filtered. The first portion of the filtrate was thrown away, and the exact volume of the filtrate was diluted with methanol. The final concentrations of TKIs ranged from 50 to 5000 μg mL−1.
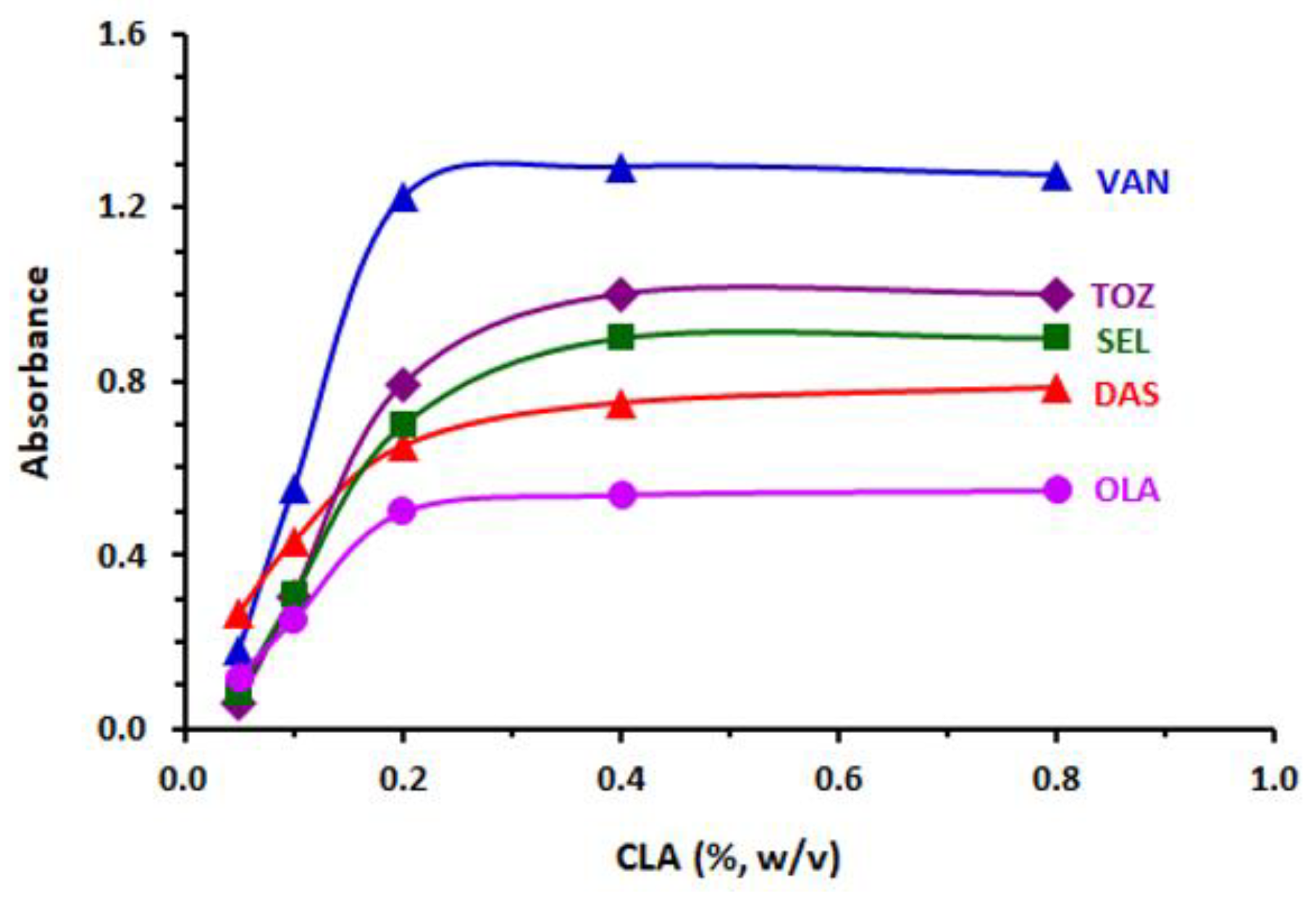
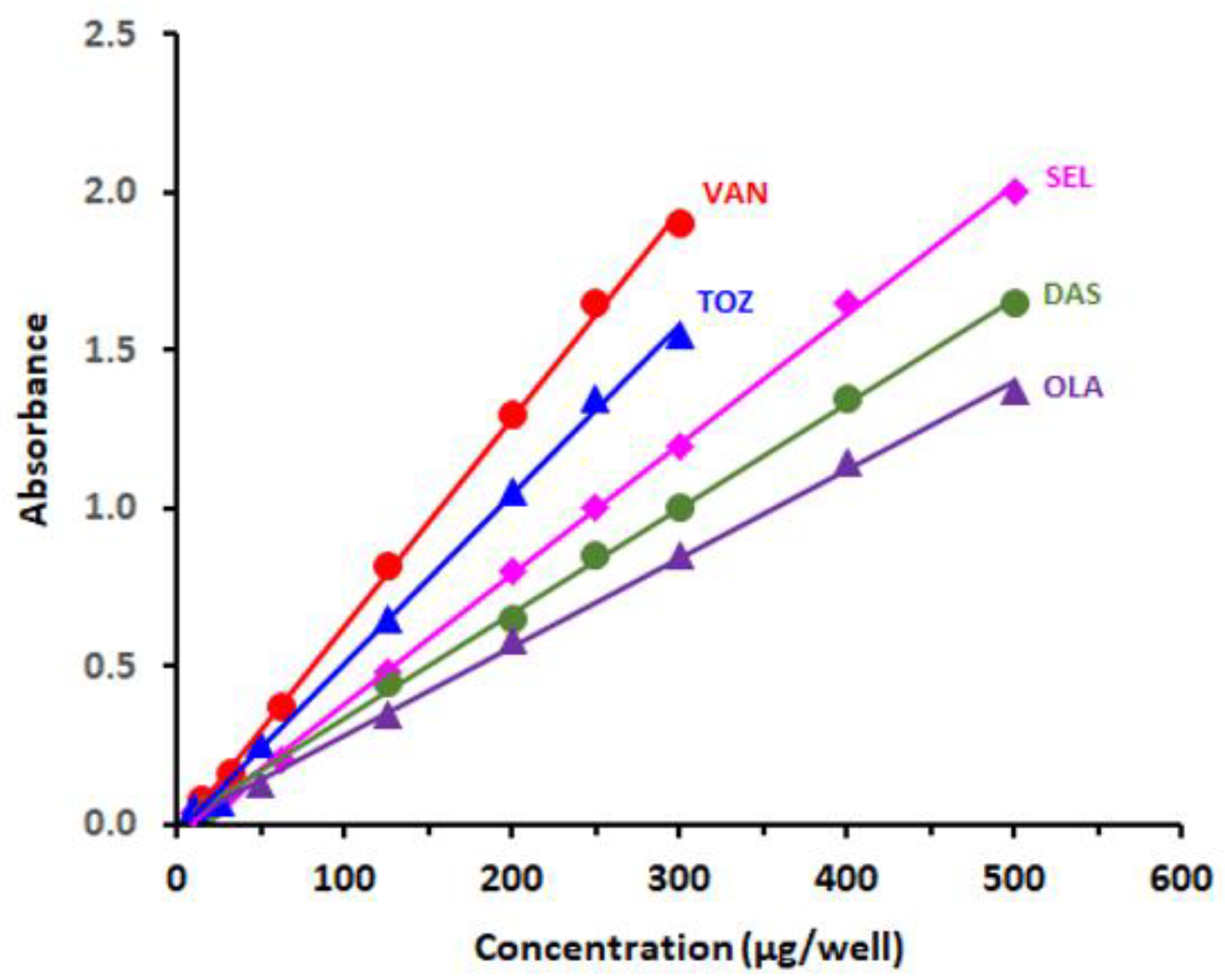
3.7. Procedure of MW-SPA
Aliquots (100 microliters) of the standard or tablet sample solutions were composed of varying concentrations of TKI, ranging from 5 to 500 µg, and were placed to 96-well plates in addition to 100 microliters of 0.4% w/v of CLA solution. The reaction was carried out at 25 ± 2 °C for 5 min. Absorbances of the product were measured by the plate reader at a selected wavelength (490 nm). The blank wells were treated exactly the same as the other wells, except for the addition of 100 µL of methanol to each of them instead of the TKI solutions. Then, the absorbances of the samples were corrected by subtracting those of the blanks.













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}