
Impact of Matrix Metalloproteinase-9 during Periodontitis and Cardiovascular Diseases

 ,
,  , ,
, , 
Abstract
:1. Introduction
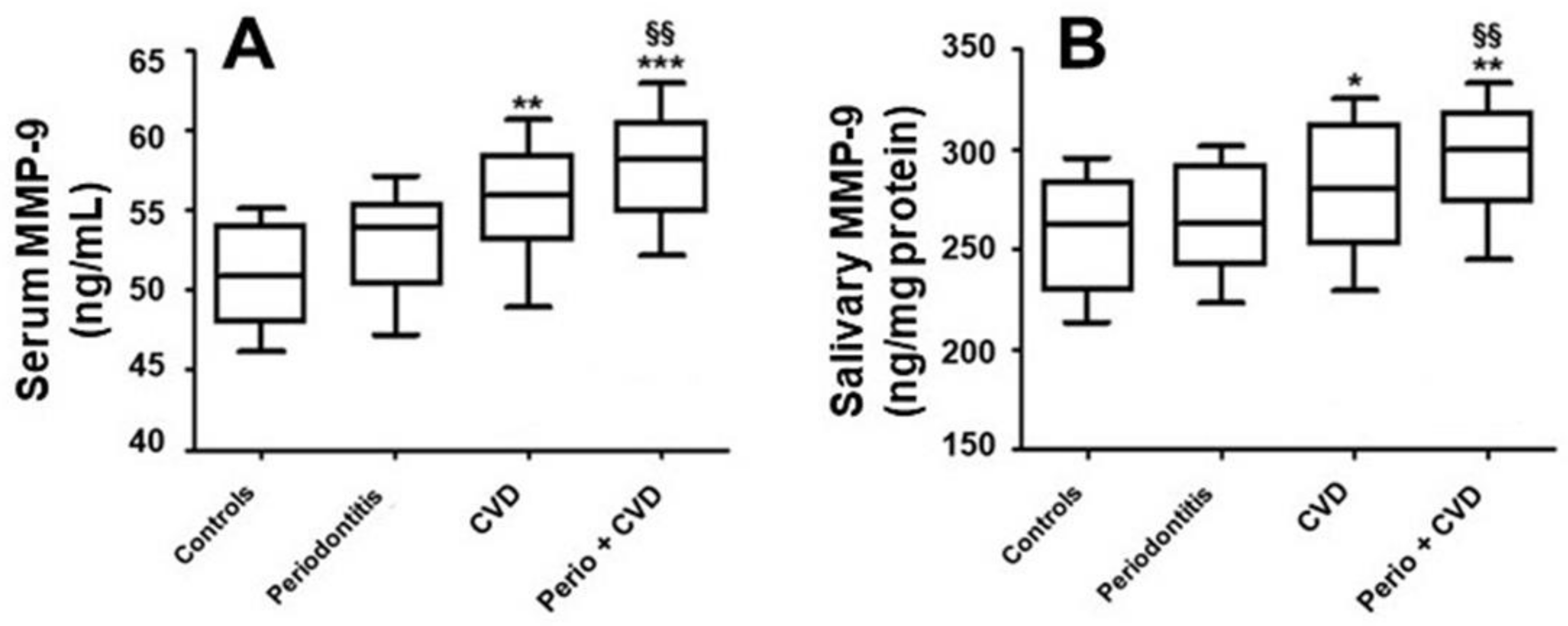
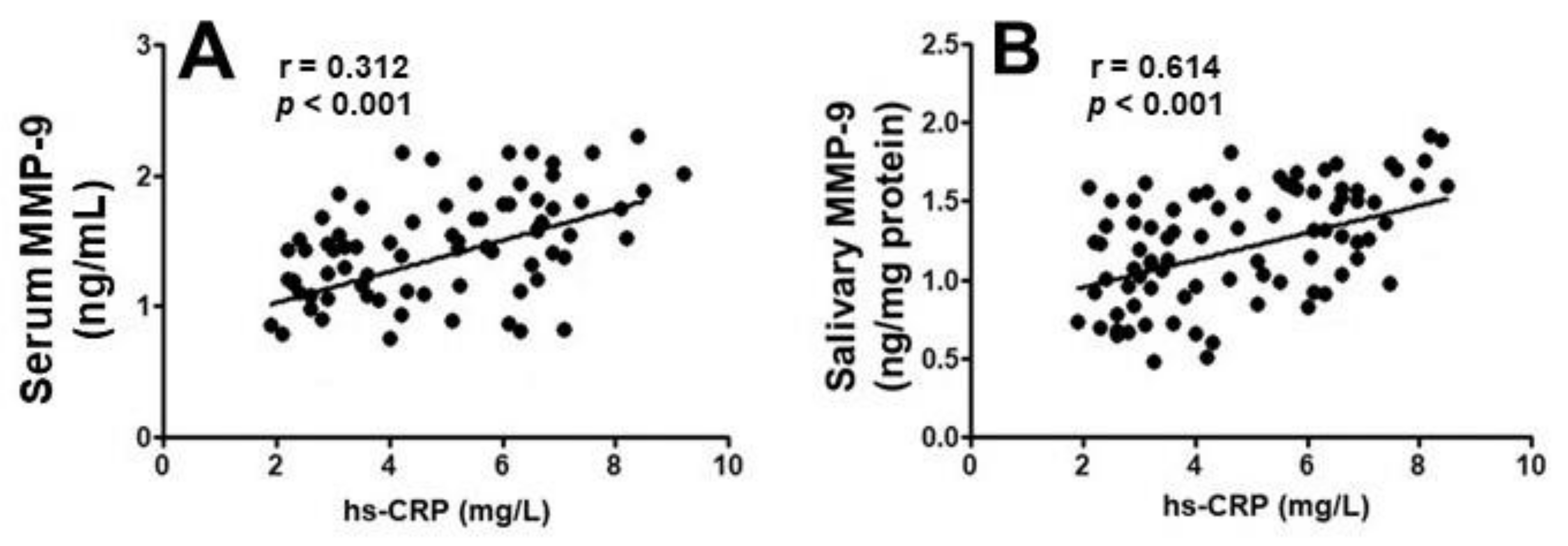
2. Results
3. Discussion
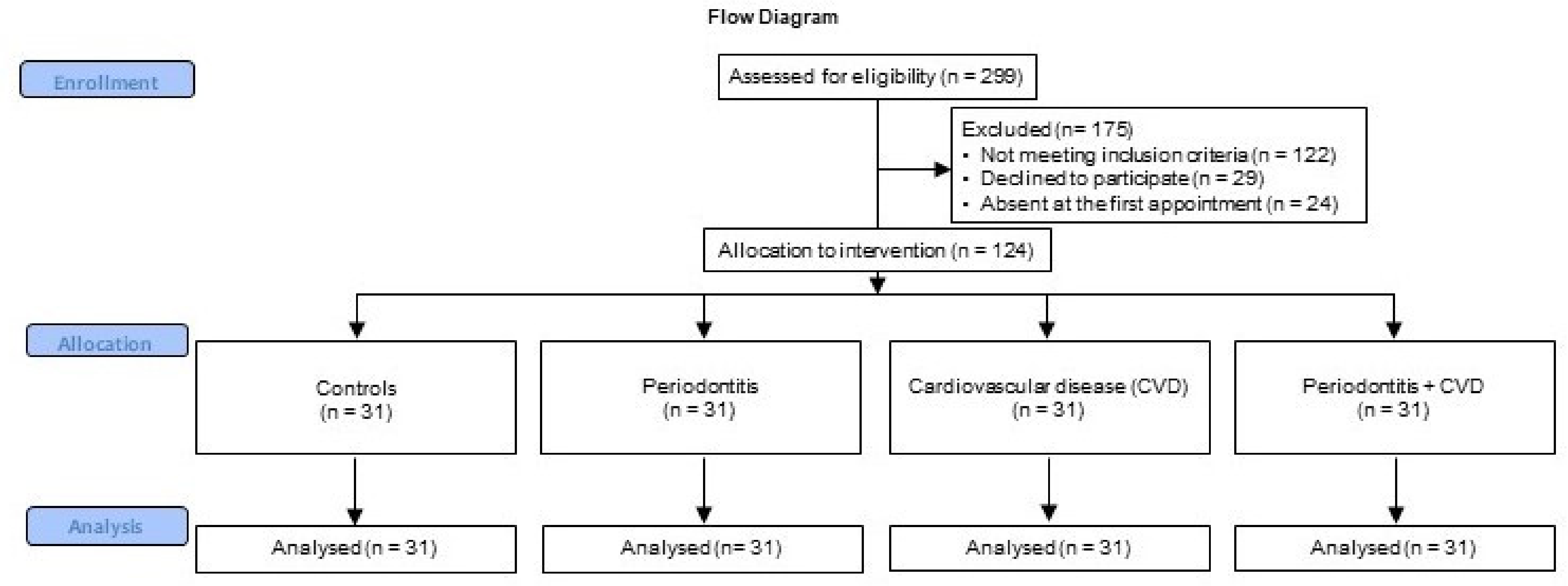
4. Materials and Methods
4.1. Serological Analysis and MMP-9 Evaluation
4.2. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Sample Availability
References
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef] [Green Version]
- Widén, C.; Holmer, H.; Sättlin, S.; Renvert, S.; Lernmark, Å.; Persson, G.R. Periodontal conditions, retinopathy, and serum markers in individuals with type 1 diabetes. J. Periodontol. 2020, 91, 1436–1443. [Google Scholar] [CrossRef] [PubMed]
- Polizzi, A.; Santonocito, S.; Vaccaro, M.; Fichera, G.; Torrisi, S.; Ronsivalle, V.; Palazzo, G.; Sicari, F.; Indelicato, F. Relationship between periodontitis and psychosocial impact in patients with systemic sclerosis: A clinical study. Mediterr. J. Clin. Psychol. 2020, 8, 2. [Google Scholar]
- Bilgin Çetin, M.; Önder, C.; Orhan, K.; Kumbasar, D.; Serdar, M.A.; Ünsal, E. Relationship of periodontitis and edentulism to angiographically diagnosed coronary artery disease: A cross-sectional study. J. Periodontal Res. 2020, 55, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.; Strecker, P.; Kreuz, M.; Löffler, M.; Kiess, W.; Hirsch, C.; Thiery, J.; Baber, R.; Bae, Y.J.; Kratzsch, J.; et al. Stress-related hormones in association with periodontal condition in adolescents—results of the epidemiologic LIFE Child study. Clin. Oral Investig. 2018, 23, 1793–1802. [Google Scholar] [CrossRef] [PubMed]
- Holmlund, A.; Holm, G.; Lind, L. Number of Teeth as a Predictor of Cardiovascular Mortality in a Cohort of 7,674 Subjects Followed for 12 Years. J. Periodontol. 2010, 81, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Polizzi, A.; Alibrandi, A.; Williams, R.C.; Leonardi, R. Independent impact of periodontitis and cardiovascular disease on elevated soluble urokinase-type plasminogen activator receptor (suPAR) levels. J. Periodontol. 2020. [Google Scholar] [CrossRef]
- Li, C.; Lv, Z.; Shi, Z.; Zhu, Y.; Wu, Y.; Li, L.; Iheozor-Ejiofor, Z. Periodontal therapy for the management of cardiovascular disease in patients with chronic periodontitis. Cochrane Database Syst. Rev. 2014, 8, CD009197. [Google Scholar] [CrossRef]
- Senini, V.; Amara, U.; Paul, M.; Kim, H. Porphyromonas gingivalis lipopolysaccharide activates platelet Cdc42 and promotes platelet spreading and thrombosis. J. Periodontol. 2019, 90, 1336–1345. [Google Scholar] [CrossRef]
- Ninomiya, M.; Hashimoto, M.; Yamanouchi, K.; Fukumura, Y.; Nagata, T.; Naruishi, K. Relationship of oral conditions to the incidence of infective endocarditis in periodontitis patients with valvular heart disease: A cross-sectional study. Clin. Oral Investig. 2020, 24, 833–840. [Google Scholar] [CrossRef]
- Sharma, P.; Dietrich, T.; Ferro, C.J.; Cockwell, P.; Chapple, I.L. Association between periodontitis and mortality in stages 3–5 chronic kidney disease: NHANES III and linked mortality study. J. Clin. Periodontol. 2016, 43, 104–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Boer, S.P.; Cheng, J.M.; Range, H.; Garcia-Garcia, H.M.; Heo, J.H.; Akkerhuis, K.M.; Meilhac, O.; Cosler, G.; Pussinen, P.J.; van Geuns, R.J.; et al. Antibodies to periodontal pathogens are associated with coronary plaque remodeling but not with vulnerability or burden. Atherosclerosis 2014, 237, 84–91. [Google Scholar] [CrossRef]
- Sanz, M.; Del Castillo, A.M.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and Cardiovascular Diseases. Consensus Report. Glob. Hear 2020, 15, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schenkein, H.A.; Loos, B.G. Inflammatory mechanisms linking periodontal diseases to cardiovascular diseases. J. Clin. Periodontol. 2013, 40, S51–S69. [Google Scholar] [CrossRef] [PubMed]
- Lahdentausta, L.; Paju, S.; Mäntylä, P.; Buhlin, K.; Pietiäinen, M.; Tervahartiala, T.; Nieminen, M.S.; Sinisalo, J.; Sorsa, T.; Pussinen, P.J. Smoking confounds the periodontal diagnostics using saliva biomarkers. J. Periodontol. 2019, 90, 475–483. [Google Scholar] [CrossRef] [Green Version]
- Bastos, M.F.; Tucci, M.A.; Siqueira, A.; Faveri, M.; Figueiredo, L.C.; Vallim, P.C.; Duarte, P.M. Diabetes may affect the expression of matrix metalloproteinases and their inhibitors more than smoking in chronic periodontitis. J. Periodontal Res. 2016, 52, 292–299. [Google Scholar] [CrossRef]
- Nagase, H. Activation mechanisms of matrix metalloproteinases. Biol. Chem. 1997, 378, 151–160. [Google Scholar]
- Yabluchanskiy, A.; Ma, Y.; Iyer, R.P.; Hall, M.E.; Lindsey, M.L. Matrix Metalloproteinase-9: Many Shades of Function in Cardiovascular Disease. Physiology 2013, 28, 391–403. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, S.; Ramadori, G.; Moriconi, F. Modulation of Chemokine- and Adhesion-Molecule Gene Expression and Recruitment of Neutrophil Granulocytes in Rat and Mouse Liver after a Single Gadolinium Chloride or Zymosan Treatment. Int. J. Mol. Sci. 2018, 19, 3891. [Google Scholar] [CrossRef] [Green Version]
- de Souza, R.G.M.; Gomes, A.C.; Navarro, A.M.; Cunha, L.C.D.; Silva, M.A.C.; Junior, F.B.; Mota, J.F. Baru Almonds Increase the Activity of Glutathione Peroxidase in Overweight and Obese Women: A Randomized, Placebo-Controlled Trial. Nutrients 2019, 11, 1750. [Google Scholar] [CrossRef] [Green Version]
- Boelen, G.-J.; Boute, L.; D’Hoop, J.; Ezeldeen, M.; Lambrichts, I.; Opdenakker, G. Matrix metalloproteinases and inhibitors in dentistry. Clin. Oral Investig. 2019, 23, 2823–2835. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.D.; Kim, S.; Jeon, S.; Kim, S.J.; Cho, H.J.; Choi, Y.N. Diagnostic and Prognostic ability of salivary MMP-9 and S100A8 for per-iodontitis. J. Clin. Periodontol. 2020, 47, 1191–1200. [Google Scholar] [CrossRef] [PubMed]
- Dds, L.S.B.; Franco, G.C.N.; Castro, M.L.; Vieira, M.S.; Galvão-Moreira, L.V.; Dds, S.C.C.; Anbinder, A.L.; Kawai, T.; Rosalen, P.L. Protective effects of desipramine on alveolar bone in experimental periodontitis. J. Periodontol. 2020, 91, 1694–1703. [Google Scholar] [CrossRef]
- Yang, M.; Li, L.; Soh, Y.; Heo, S. Effects of omega-3 fatty acids and aspirin on Porphyromonas gingivalis -induced periodontitis in rats. J. Periodontol. 2019, 90, 1307–1319. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-C.; Chu, S.-C.; Yang, S.-F.; Hsieh, Y.-S.; Yang, L.-C.; Huang, F.-M. Examination of the signal transduction pathways leading to activation of gelatinolytic activity by interleukin-1alpha and Porphyromonas gingivalis in human osteosarcoma cells. J. Periodontal Res. 2004, 39, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Holtfreter, B.; Empen, K.; Gläser, S.; Lorbeer, R.; Völzke, H.; Ewert, R.; Kocher, T.; Dörr, M. Periodontitis Is Associated with Endothelial Dysfunction in a General Population: A Cross-Sectional Study. PLoS ONE 2013, 8, e84603. [Google Scholar] [CrossRef] [PubMed]
- Díaz, C.M.; Bullon, B.; Ruiz-Salmerón, R.J.; Fernández-Riejos, P.; Fernández-Palacín, A.; Battino, M.; Cordero, M.D.; Quiles, J.L.; Varela-López, A.; Bullón, P. Molecular inflammation and oxidative stress are shared mechanisms involved in both myocardial infarction and periodontitis. J. Periodontal Res. 2020, 55, 519–528. [Google Scholar] [CrossRef]
- Andrukhov, O.; Haririan, H.; Bertl, K.; Rausch, W.-D.; Bantleon, H.-P.; Moritz, A.; Rausch-Fan, X. Nitric oxide production, systemic inflammation and lipid metabolism in periodontitis patients: Possible gender aspect. J. Clin. Periodontol. 2013, 40, 916–923. [Google Scholar] [CrossRef]
- Gurav, A.N. The implication of periodontitis in vascular endothelial dysfunction. Eur. J. Clin. Investig. 2014, 44, 1000–1009. [Google Scholar] [CrossRef] [Green Version]
- Rathnayake, N.; Gustafsson, A.; Norhammar, A.; Kjellström, B.; Klinge, B.; Rydén, L.; Tervahartiala, T.; Sorsa, T. PAROKRANK Steering Group Salivary Matrix Metalloproteinase-8 and -9 and Myeloperoxidase in Relation to Coronary Heart and Periodontal Diseases: A Subgroup Report from the PAROKRANK Study (Periodontitis and Its Relation to Coronary Artery Disease). PLoS ONE 2015, 10, e0126370. [Google Scholar] [CrossRef] [Green Version]
- Tabeta, K.; Hosojima, M.; Nakajima, M.; Miyauchi, S.; Miyazawa, H.; Takahashi, N.; Matsuda, Y.; Sugita, N.; Komatsu, Y.; Sato, K.; et al. Increased serum PCSK9, a potential biomarker to screen for periodontitis, and decreased total bilirubin associated with probing depth in a Japanese community survey. J. Periodontal Res. 2018, 53, 446–456. [Google Scholar] [CrossRef]
- Yoshimura, S.; Nishimura, Y.; Nishiuma, T.; Yamashita, T.; Kobayashi, K.; Yokoyama, M. Overexpression of nitric oxide synthase by the endothelium attenuates bleomycin-induced lung fibrosis and impairs MMP-9/TIMP-1 balance. Respirology 2006, 11, 546–556. [Google Scholar] [CrossRef]
- Kendall, H.K.; Marshall, R.I.; Bartold, P.M. Nitric oxide, and tissue destruction. Oral Dis. 2001, 7, 2–10. [Google Scholar] [CrossRef]
- Aurer, A.; Aleksić, J.; Ivić-Kardum, M.; Aurer, J.; Čulo, F. Nitric oxide synthesis is decreased in periodontitis. J. Clin. Periodontol. 2001, 28, 565–568. [Google Scholar] [CrossRef] [PubMed]
- Ruest, L.B.; Ranjbaran, H.; Tong, E.J.; Svoboda, K.K.; Feng, J.Q. Activation of Receptor Activator of Nuclear Factor-κB Ligand and Matrix Metalloproteinase Production in Periodontal Fibroblasts by Endothelin Signaling. J. Periodontol. 2016, 87, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Marcaccini, A.M.; Novaes, A.B.; Meschiari, C.A.; Souza, S.L.; Palioto, D.B.; Sorgi, C.A.; Faccioli, L.H.; Tanus-Santos, J.E.; Gerlach, R.F. Circulating matrix metalloproteinase-8 (MMP-8) and MMP-9 are increased in chronic periodontal disease and decrease after non-surgical periodontal therapy. Clin. Chim. Acta 2009, 409, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Filho, I.S.; Coelho, J.M.F.; Miranda, S.S.; Cruz, S.S.; Trindade, S.C.; Cerqueira, E.M.; Passos-Soares, J.S.; Costa, M.D.C.N.; Vianna, M.I.P.; Figueiredo, A.C.M.; et al. Severe and moderate periodontitis are associated with acute myocardial infarction. J. Periodontol. 2020, 91, 1444–1452. [Google Scholar] [CrossRef]
- Santonocito, S.; Ronsivalle, V.; Fichera, G.; Indelicato, F. Psychological impact and patient perception of occlusion and orthodontic treatment in periodontitis patients. Mediterr. J. Clin. Psychol. 2020, 8. [Google Scholar] [CrossRef]
- Köse, O.; Kurt Bayrakdar, S.; Akyıldız, K.; Altın, A.; Arabacı, T.; Yemenoglu, H.; Zihni Korkmaz, M.; Köse, T.E.; Türker Sener, L.; Mercantepe, T.; et al. Melatonin ameliorates periodontitis-related inflammatory stress at cardiac left ventricular tissues in rats. J. Periodontol. 2020, 91, 1486–1494. [Google Scholar] [CrossRef]
- Wu, Y.-C.; Ning, L.; Tu, Y.-K.; Huang, C.-P.; Huang, N.-T.; Chen-Pang, H.; Chang, P.-C. Salivary biomarker combination prediction model for the diagnosis of periodontitis in a Taiwanese population. J. Formos. Med Assoc. 2018, 117, 841–848. [Google Scholar] [CrossRef]
- Maneesai, P.; Bunbupha, S.; Potue, P.; Berkban, T.; Kukongviriyapan, U.; Kukongviriyapan, V.; Prachaney, P.; Pakdeechote, P. Hes-peridin Prevents Nitric Oxide Deficiency-Induced Cardiovascular Remodeling in Rats via Suppressing TGF-β1 and MMPs Protein Expression. Nutrients 2018, 10, 1549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangel, T.P.; Reis, A.A.; Caponi, L.; Pena, L.C.S.; Ruiz, K.G.S.; Santamaria, M.P.; Mathias-Santamaria, I.F.; Casati, M.Z.; Casarin, R.C.V. Subgingival endotoxin and lipoteichoic acid modulate cytokine production in diabetic subjects: A Case–control Study. Oral Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Vicente, A.; Bravo-González, L.-A.; Navarro, J.A.; Buendía, A.J.; Camacho-Alonso, F. Effects of diabetes on oxidative stress, periodontal ligament fiber orientation, and matrix metalloproteinase 8 and 9 expressions during orthodontic tooth movement. Clin. Oral Investig. 2021, 25, 1383–1394. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, A.; Realini, O.; Hernández, M.; Albers, D.; Weber, L.; Ramírez, V.; Param, F.; Kusanovic, J.P.; Sorsa, T.; Rice, G.E.; et al. Early pregnancy levels of gingival crevicular fluid matrix metalloproteinases-8 and -9 are associated with the severity of periodontitis and the development of gestational diabetes mellitus. J. Periodontol. 2021, 92, 205–215. [Google Scholar] [CrossRef]
- Rabe, A.; Salazar, M.G.; Fuchs, S.; Kocher, T.; Völker, U. Comparative analysis of Salivette® and paraffin gum preparations for establishment of a metaproteomics analysis pipeline for stimulated human saliva. J. Oral Microbiol. 2018, 10, 1428006. [Google Scholar] [CrossRef] [PubMed]
- Silva, N.L.C.; Motta, N.A.V.; Soares, M.A.; Araujo, O.M.O.; Espíndola, L.C.P.; Colombo, A.P.V.; Lopes, R.T.; Brito, F.C.F.; Miranda, A.L.P.; Tributino, J.L.M. Periodontal status, vascular reactivity, and platelet aggregation changes in rats submitted to hypercholesterolemic diet and periodontitis. J. Periodontal Res. 2020, 55, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Bodis, S.; Haregewoin, A. Significantly reduced salivary nitric oxide levels in smokers. Ann. Oncol. 1994, 5, 371–372. [Google Scholar] [CrossRef] [PubMed]
- De Araújo, A.A.; Pereira, A.D.S.B.F.; De Medeiros, C.A.C.X.; Brito, G.A.D.C.; Leitao, R.F.D.C.; Araújo, L.D.S.; Guedes, P.M.M.; Hiyari, S.; Pirih, F.Q.; Júnior, R.F.D.A. Effects of metformin on inflammation, oxidative stress, and bone loss in a rat model of periodontitis. PLoS ONE 2017, 12, e0183506. [Google Scholar] [CrossRef] [Green Version]
- Yucel, Z.P.K.; Afacan, B.; Emingil, G.; Tervahartiala, T.; Kose, T.; Sorsa, T. Local and systemic levels of aMMP-8 in gingivitis and stage 3 grade C periodontitis. J. Periodontal Res. 2020, 55, 887–894. [Google Scholar] [CrossRef]
- Karatas, O.; Yuce, H.B.; Tulu, F.; Taskan, M.M.; Gevrek, F.; Toker, H. Evaluation of apoptosis and hypoxia-related factors in gingival tissues of smoker and non-smoker periodontitis patients. J. Periodontal Res. 2019, 55, 392–399. [Google Scholar] [CrossRef]
- Kuula, H.; Salo, T.; Pirilä, E.; Hagström, J.; Luomanen, M.; Gutierrez-Fernandez, A.; Romanos, G.E.; Sorsa, T. Human beta-defensin-1 and -2 and matrix metalloproteinase-25 and -26 expression in chronic and aggressive periodontitis and in peri-implantitis. Arch. Oral Biol. 2008, 53, 175–186. [Google Scholar] [CrossRef]
- Schmidt, J.; Weigert, M.; Leuschner, C.; Hartmann, H.; Raddatz, D.; Haak, R.; Mausberg, R.; Kottmann, T.; Schmalz, G.; Ziebolz, D. Active matrix metalloproteinase-8 and periodontal bacteria-interlink between periodontitis and inflammatory bowel disease? J. Periodontol. 2018, 89, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Preethi, S.; Jose, J.I.; Sivapathasundharam, B.; Sabarinath, B. Evaluation of Salivary Nitric Oxide Levels in Smokers, Tobacco Chewers and Patients with Oral Lichenoid Reactions. J. Clin. Diagn. Res. 2016, 10, ZC63–ZC66. [Google Scholar] [CrossRef]
- Polizzi, A.; Santonocito, S.; Di Stefano, M.; Ferlito, S.; Indelicato, F.; Palazzo, G. The effects on oral related quality of life induced by periodontitis in patients with juvenile idiopathic arthritis. Mediterr. J. Clin. Psychol. 2020, 8, 1. [Google Scholar]
- Tayman, M.A.; Kurgan, Ş.; Önder, C.; Güney, Z.; Serdar, M.A.; Kantarcı, A.; Günhan, M.; Tayman, A. A disintegrin-like and metalloproteinase with thrombospondin-1 (ADAMTS-1) levels in gingival crevicular fluid correlate with vascular endothelial growth factor-A, hypoxia-inducible factor-1α, and clinical parameters in patients with advanced periodontitis. J. Periodontol. 2019, 90, 1182–1189. [Google Scholar] [CrossRef] [PubMed]
- Lekic, A.; Brekalo, Z.; Kvesic, A.; Kovacevic, M.; Baricev-Novakovic, Z.; Sutic, I.; Bulog, A.; Pavisic, V.; Mrakovcic-Sutic, I. Crosstalk Between Enzyme Matrix Metalloproteinases 2 and 9 and Regulatory T Cell Immunity in the Global Burden of Atherosclerosis. Scand. J. Immunol. 2017, 86, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Sczepanik, F.S.C.; Grossi, M.L.; Casati, M.; Goldberg, M.; Glogauer, M.; Fine, N.; Tenenbaum, H.C. Periodontitis is an inflammatory disease of oxidative stress: We should treat it that way. Periodontology 2000 2020, 84, 45–68. [Google Scholar] [CrossRef]
- Higashi, Y.; Goto, C.; Jitsuiki, D.; Umemura, T.; Nishioka, K.; Hidaka, T.; Takemoto, H.; Nakamura, S.; Soga, J.; Chayama, K.; et al. Periodontal Infection Is Associated With Endothelial Dysfunction in Healthy Subjects and Hypertensive Patients. Hypertension 2008, 51, 446–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, D.-H.; Moon, I.-S.; Choi, B.-K.; Paik, J.-W.; Kim, Y.-S.; Choi, S.-H.; Kim, C.-K. Effects of sub-antimicrobial dose doxycycline therapy on crevicular fluid MMP-8, and gingival tissue MMP-9, TIMP-1 and IL-6 levels in chronic periodontitis. J. Periodontal Res. 2003, 39, 20–26. [Google Scholar] [CrossRef]
- Kornman, K.S.; Papapanou, P.N. Clinical application of the new classification of periodontal diseases: Ground rules, clarifications and “gray zones”. J. Periodontol. 2020, 91, 352–360. [Google Scholar] [CrossRef]
- Isola, G.; Polizzi, A.; Patini, R.; Ferlito, S.; Alibrandi, A.; Palazzo, G. Association among serum and salivary A. actinomycetemcomitans specific immunoglobulin antibodies and periodontitis. BMC Oral Health 2020, 20, 283. [Google Scholar] [CrossRef] [PubMed]
- Bassand, J.P.; Hamm, C.W.; Ardissino, D.; Boersma, E.; Budaj, A.; Fernández-Avilés, F.; Fox, K.A.A.; Hasdai, D.; Magnus Ohman, E.; Wallentin, L.; et al. Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes: The Task Force for the Diagnosis and Treatment of Non-ST-Segment Elevation Acute Coronary Syn-dromes of the European Society of Cardiology. Eur. Heart J. 2007, 28, 1598–1660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The Plaque Control Record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Hollander, M.; Wolfe, D.A.; Chicken, E. Nonparametric Statistical Methods, 3rd ed.; John Wiley & Sons: New York, NY, USA, 2013. [Google Scholar]
- Skurska, A.; Dolinska, E.; Pietruska, M.; Pietruski, J.K.; Dymicka, V.; Kemona, H.; Arweiler, N.B.; Milewski, R.; Sculean, A. Effect of nonsurgical periodontal treatment in conjunction with either systemic administration of amoxicillin and metronidazole or additional photodynamic therapy on the concentration of matrix metalloproteinases 8 and 9 in gingival crevicular fluid in patients with aggressive periodontitis. BMC Oral Health 2015, 15, 63. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Controls | Periodontitis | CVD | Periodontitis + CVD | |
|---|---|---|---|---|
| Age (years) | 52 (47; 57) | 53 (48; 58) | 52 (47; 57) | 53 (46; 57) |
| Gender (male/female) | 16/15 | 15/16 | 14/17 | 15/16 |
| Education level | ||||
| Primary school, n (%) | 12 (35.4) | 13 (41.9) | 15 (48.4) | 14 (45.2) |
| High school, n (%) | 13 (45.2) | 12 (38.7) | 11 (35.5) | 12 (38.7) |
| College/university, n (%) | 6 (19.4) | 6 (19.4) | 5 (16.1) | 5 (16.1) |
| Body mass index (kg/m2) | 25.4 (21.8; 27.8) | 24.9 (22.4; 26.4) | 25.8 (21.6; 27.1) | 26.5 (22.5; 26.1) |
| Fasting glucose (mg/dl) | 88.9 (82.1; 93.2) | 89.7 (82.3; 105.3) | 87.1 (80.6; 114.6) | 90.1 (85.1; 109.2) |
| Smoking | ||||
| Never smokers, n (%) | 25 (80.7) | 27 (87.1) | 28 (90.4) | 26 (83.9) |
| Past smokers, n (%) | 4 (12.9) | 1 (3.2) | 1 (3.2) | 3 (9.7) |
| Current smokers, n (%) | 2 (6.4) | 3 (9.7) | 2 (6.4) | 2 (6.4) |
| Current smokers—number cigarettes per day, n | 5 (3; 5) | 6 (4; 7) | 6 (3; 6) | 5 (4; 6) |
| Comorbidities | ||||
| Diabetes, n (%) | - | 3 (9.6) ** | 2 (6.4) ** | 2 (9.6) ** |
| Previous CVD | ||||
| Atrial fibrillation, n (%) | - | - | 6 (19.3) **,§§ | 5 (16.1) **,§§ |
| Angina pectoris, n (%) | - | - | 12 (38.7) **,§§ | 13 (41.9) **,§§ |
| Stroke, n (%) | - | - | 5 (16.1) **, §§ | 7 (22.6) **,§§ |
| Heart failure, n (%) | - | - | 6 (19.3) **,§§ | 5 (16.1) **,§§ |
| Medications | ||||
| Antihypertensive, n (%) | - | - | 10 (32.2) **,§§ | 10 (32.2) **,§§ |
| Statins, n (%) | - | - | 10 (32.2) **,§§ | 9 (29) **,§§ |
| Low-dose aspirin, n (%) | - | - | 7 (22.6) **,§§ | 7 (22.6) **,§§ |
| Beta blockers, n (%) | - | - | 7 (22.6) **,§§ | 8 (25.8) **,§§ |
| hs-CRP (mg/L) | 2.5 (2.1; 2.9) | 3.1 (2.5; 3.9) * | 5.6 (4.8; 6.2) ** | 6.7 (5.8; 7.1) **,§§, # |
| Total cholesterol (mg/dl) | 166 (139; 181) | 165 (133; 181) | 172 (139; 197) | 175 (178; 201) |
| Triglycerids (mg/dl) | 121 (91; 145) | 102 (66; 128) | 141 (122; 166) | 139 (103; 158) |
| Controls | Periodontitis | CVD | Periodontitis + CVD | |
|---|---|---|---|---|
| Number of teeth | 25 (21; 26) | 19 (17; 22) ** | 22 (20; 25) **,§§ | 19 (18; 21) **,## |
| CAL (mm) | 1.1 (0.8; 1.4) | 3.3 (3; 3.9) ** | 2.2 (1.9; 2.3) **,§§ | 3.6 (3.1; 3.9) **,## |
| % CAL 4–5 mm | - | 36.6 (35.4; 43.7) ** | - | 39.9 (34.8; 45.1) **,## |
| % CAL ≥ 6 mm | - | 19.1 (17.7; 23.1) ** | - | 18.1 (16.1; 23.1) **,## |
| PD (mm) | 1.4 (1.4; 1.8) | 4.3 (3.6; 4.8) ** | 1.9 (1.7; 2.5) **,§§ | 3.8 (3.6; 4.45 **,## |
| % PD 4–5 mm | - | 41.2 (37.9; 44.6) ** | - | 43.3 (41.9; 49.2) **,## |
| % PD ≥ 6 mm | - | 22.9 (18.6; 24.4) ** | - | 23.2 (21.1; 25.9) **,§§,## |
| % BOP | 7.7 (5.9; 9.1) | 39.9 (35.8; 47.1) ** | 7.9 (5.9; 9.2) **,§§ | 41.6 (39.9; 47.1) **,§§,## |
| PI (%) | 5.9 (4.8; 8.8) | 33.2 (32.4; 35.8) ** | 12.3 (8.9; 11.4) **,§§ | 35.5 (29.9; 35.7) **,## |
| Rx alveolar bone loss (mm) | 0.1 (0; 0.6) | 2.7 (2.1; 3.2) ** | 0.2 (0.1; 0.4) **,§§ | 3.1 (1.9; 4.4) **,## |
| Serum MMP-9 Levels | Univariate | Multivariate | |||||
| Variable | Beta | 95% CI | p | Beta | 95% CI | p | |
| CVD | 0.439 | 0.221; 0.443 | <0.001 | 0.124 | −0.356; 0.442 | 0.312 | |
| Periodontitis | 0.274 | 0.179; 0.331 | 0.028 | 0.236 | −0.114; 0.212 | 0.208 | |
| hs-CRP | 0.225 | 0.111;0.145 | <0.001 | 0.288 | 0.054; 0.213 | <0.001 | |
| Age | −0.074 | −0.287; 0.056 | 0.078 | −0.039 | −0.111; 0.315 | 0.287 | |
| Female sex | 0.118 | −0.78; 0.549 | 0.331 | 0.219 | −0.88; 0.428 | 0.112 | |
| Education | −0.124 | −0.151; 0.144 | 0.281 | −0.117 | −0.279; 0.412 | 0.247 | |
| Salivary MMP-9 levels | |||||||
| CVD | 0.379 | 0.133; 0.441 | <0.001 | 0.014 | 0.09; 0.115 | 0.366 | |
| Periodontitis | 0.076 | −0.124; 0.248 | 0.428 | 0.012 | −0.155; 0.315 | 0.574 | |
| hs-CRP | 0.084 | 0.112; 0.366 | <0.001 | 0.125 | 0.015; 0.228 | <0.001 | |
| Age | −0.055 | −0.110; 0.036 | 0.347 | 0.055 | −0.028; 0.087 | 0.741 | |
| Female sex | 0.079 | −0.112; 0.211 | 0.311 | 0.07 | −0.065; 0.412 | 0.321 | |
| Total Cholesterol | −0.058 | −0.151; −0.062 | 0.032 | −0.66 | −0.041; 0.314 | 0.029 | |
| Serum MMP-9 | 0.124 | −0.021; 0.557 | 0.059 | −0.038 | −0.369; 0.166 | 0.331 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isola, G.; Polizzi, A.; Ronsivalle, V.; Alibrandi, A.; Palazzo, G.; Lo Giudice, A. Impact of Matrix Metalloproteinase-9 during Periodontitis and Cardiovascular Diseases. Molecules 2021, 26, 1777. https://doi.org/10.3390/molecules26061777
Isola G, Polizzi A, Ronsivalle V, Alibrandi A, Palazzo G, Lo Giudice A. Impact of Matrix Metalloproteinase-9 during Periodontitis and Cardiovascular Diseases. Molecules. 2021; 26(6):1777. https://doi.org/10.3390/molecules26061777
Chicago/Turabian StyleIsola, Gaetano, Alessandro Polizzi, Vincenzo Ronsivalle, Angela Alibrandi, Giuseppe Palazzo, and Antonino Lo Giudice. 2021. "Impact of Matrix Metalloproteinase-9 during Periodontitis and Cardiovascular Diseases" Molecules 26, no. 6: 1777. https://doi.org/10.3390/molecules26061777
APA StyleIsola, G., Polizzi, A., Ronsivalle, V., Alibrandi, A., Palazzo, G., & Lo Giudice, A. (2021). Impact of Matrix Metalloproteinase-9 during Periodontitis and Cardiovascular Diseases. Molecules, 26(6), 1777. https://doi.org/10.3390/molecules26061777