
Cannabis Bioactive Compound-Based Formulations: New Perspectives for the Management of Orofacial Pain





Abstract
:1. Introduction
2. Mechanisms of Orofacial Pain
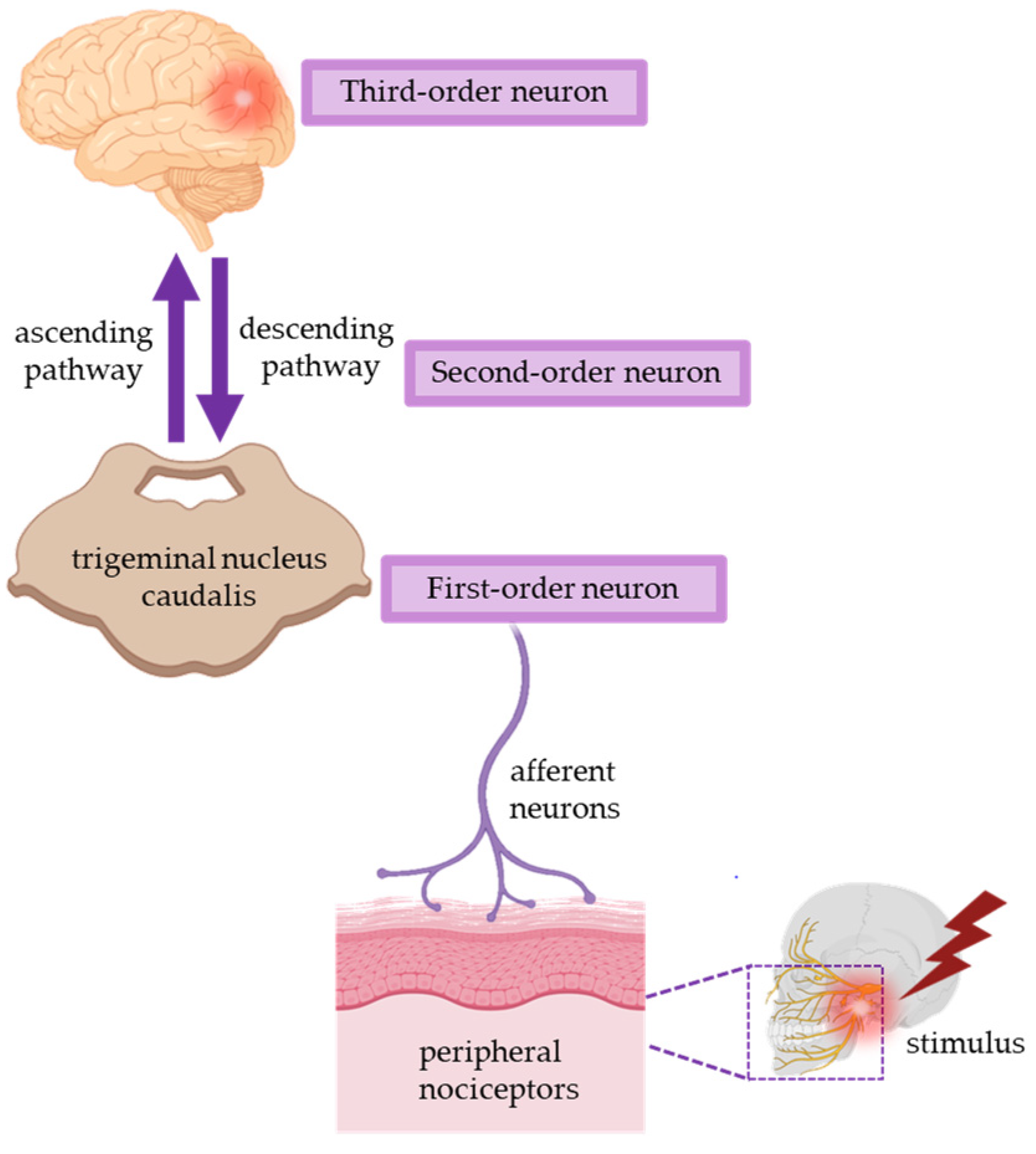
2.1. Physiological Mechanisms of Peripheral Nociceptive Pain
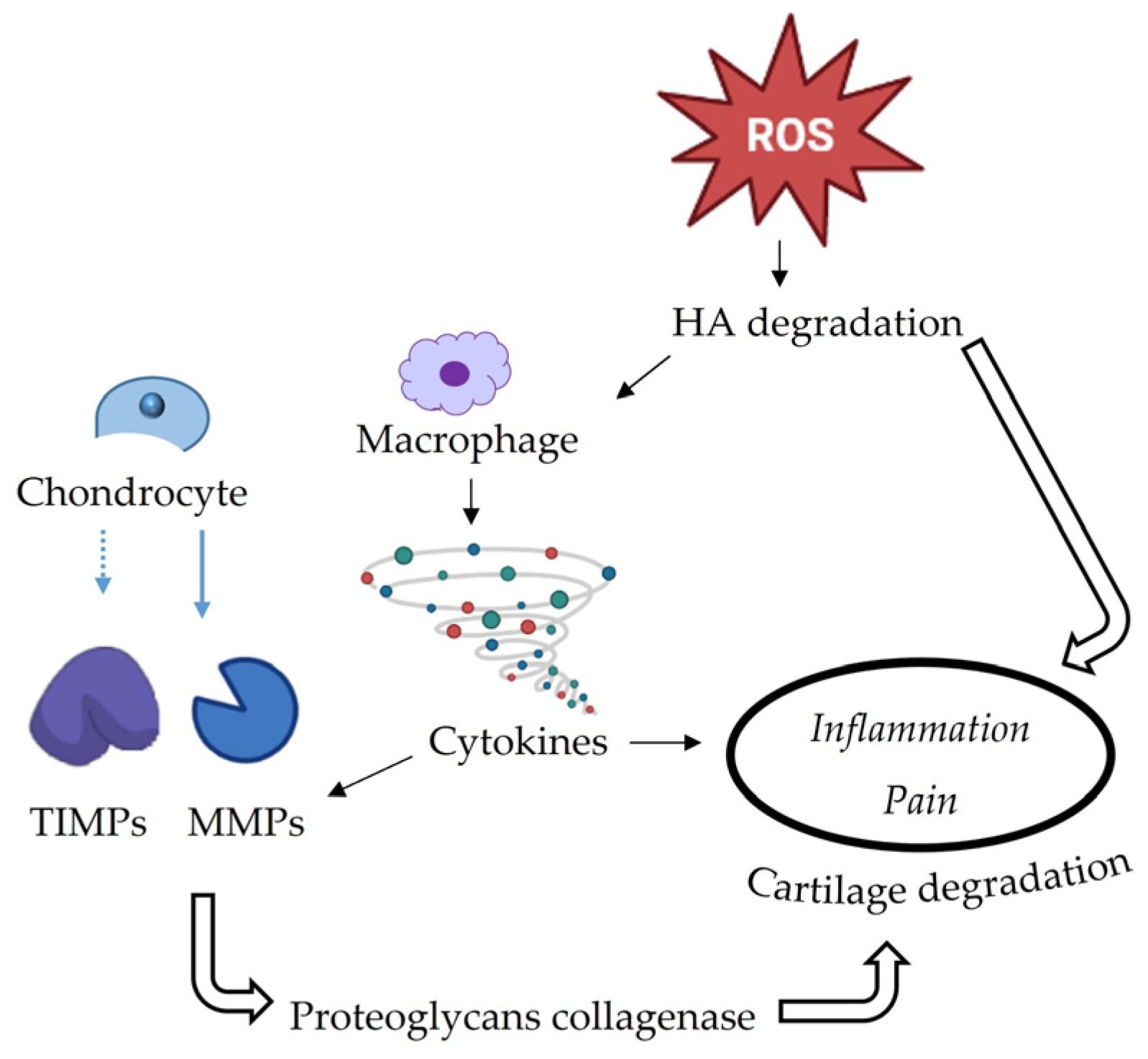
2.2. TMJ-Related Inflammatory Pain
2.3. Pathophysiology of Neuropathic Pain
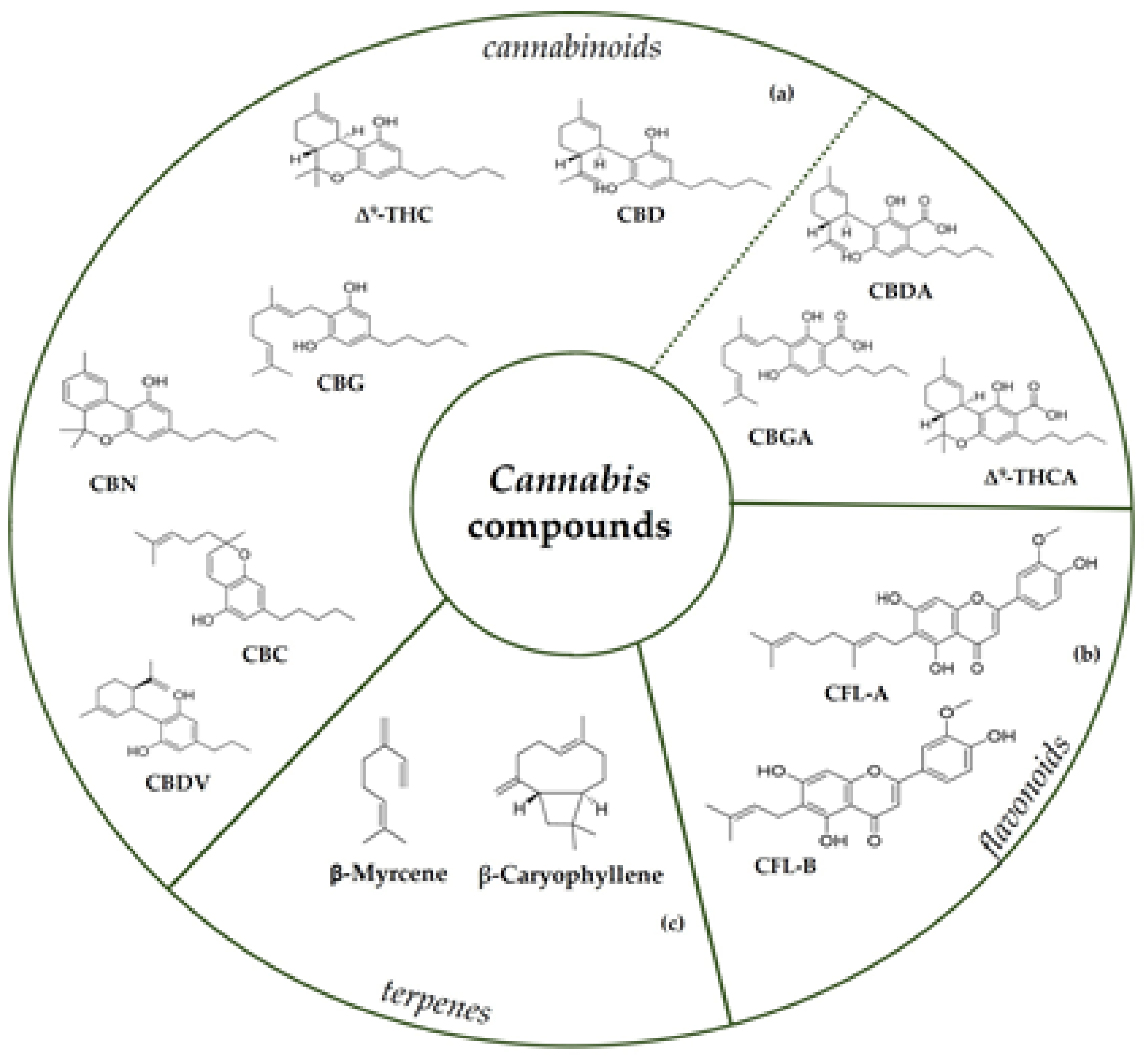
3. Cannabis Bioactive Compounds
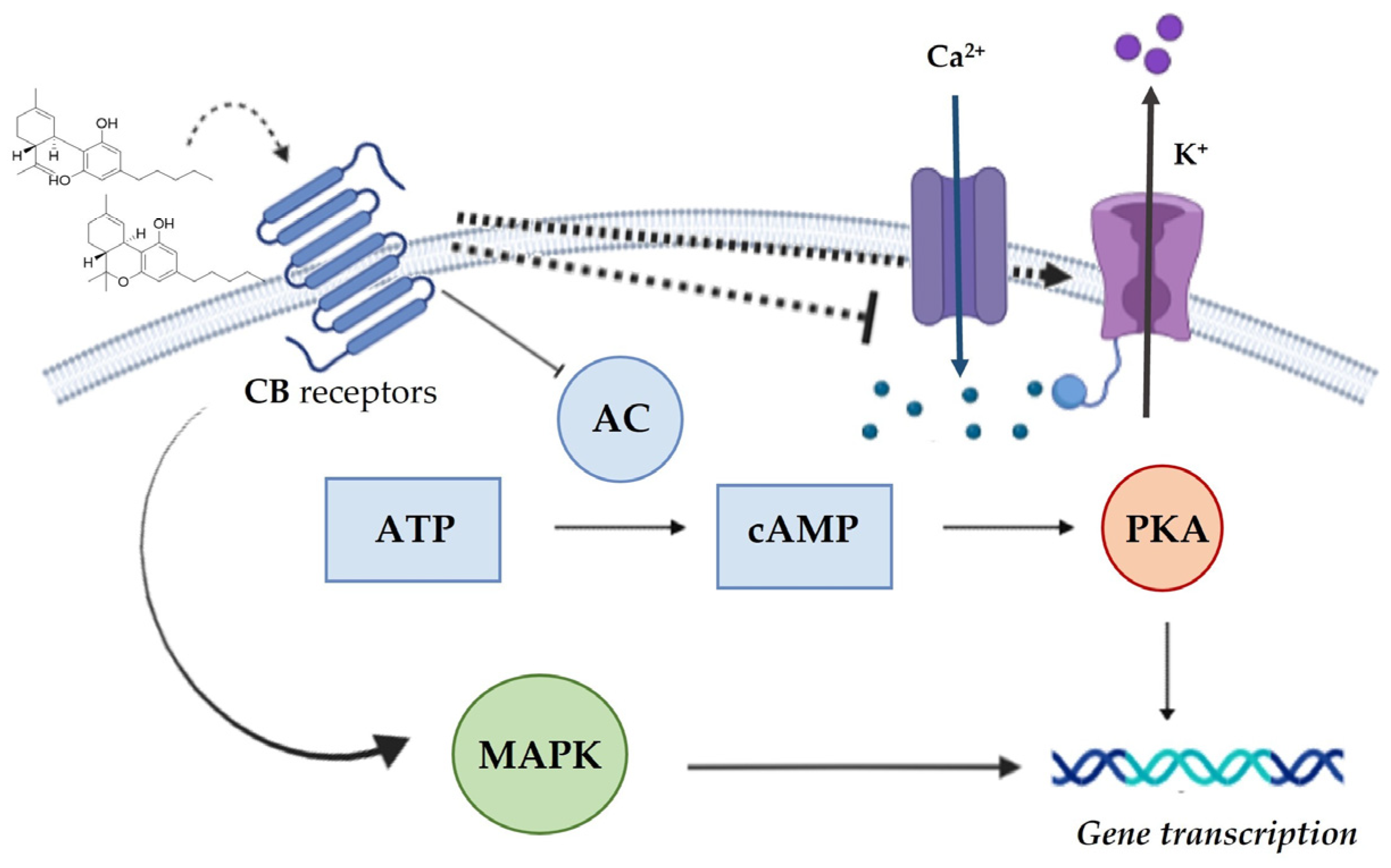
3.1. Cannabinoids and the Endocannabinoid System
3.2. Cannabis-Based Formulations as Orofacial Pain Relievers
3.3. Synthetic Cannabinoids Agonist Receptor-Based Formulations as Orofacial Pain Relievers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| TMJ | temporomandibular joint |
| TMD | temporomandibular disorders |
| TRPV1 | transient receptor potential vanilloid 1 |
| ATP | adenosine triphosphate |
| PGE | prostaglandin |
| CGRP | gene-related peptide calcitonin |
| CCK | cholecystokinin |
| IL | interleukin |
| TNF-α | tumor necrosis factor-alpha |
| HA | hyaluronic acid |
| MMPs | matrix metalloproteinases |
| TIMPs | tissue inhibitor of metalloproteinases |
| THC | Δ9-tetrahydrocannabinol |
| Δ9-THCA | Δ9-tetrahydrocannabinolic acid |
| CBD | cannabidiol |
| CBDA | cannabidiolic acid |
| CBG | cannabigerol |
| CBGA | cannabigerolic acid |
| CBDV | cannabidivarin |
| CBN | cannabinol |
| CBC | cannabichromene |
| CFL-A | cannflavin A |
| CFL-B | cannflavin B |
| CBR | cannabinoid receptors |
| AEA | N-arachidonoylethanolamide |
| 2-AG | 2-arachidonoylglycerol |
| 2-AGE | 2-arachidonyl glyceryl ether |
| NADA | N-arachidonoyl-dopamine |
| CB1 | cannabinoid receptor 1 |
| CB2 | cannabinoid receptor 2 |
| AC | adenylyl cyclase |
| PKA | protein kinase A |
| K+ channel | potassium channel |
| Ca2+ channel | calcium channel |
| cAMP | 3’,5’-cyclic adenosine monophosphate |
| MAPK | mitogen-activated protein kinases |
| GABA | γ-aminobutyric acid |
| GPR55 | G protein-coupled receptor 55 |
| PGE | prostaglandin |
| TRPM8 | transient receptor potential melastatin 8 |
| NF-KB | nuclear factor kappaB |
| NO | nitric oxide |
| OA | osteoarthritis |
| mGlu2 | metabotropic glutamate receptor 2 |
| NMDA | N-methyl-d-aspartate |
| AAE | anandamide and derivatives |
References
- Chichorro, J.G.; Porreca, F.; Sessle, B. Mechanisms of craniofacial pain. Cephalalgia 2017, 37, 613–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ananthan, S.; Benoliel, R. Chronic orofacial pain. J. Neural Transm. 2020, 127, 575–588. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, L.J.; Seminowicz, D.A.; Moayedi, M. A meta-analytic study of experimental and chronic orofacial pain excluding headache disorders. NeuroImage Clin. 2018, 20, 901–912. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Kramer, P.; Tao, F. Editorial: Mechanisms of Orofacial Pain and Sex Differences. Front. Integr. Neurosci. 2021, 15, 599580. [Google Scholar] [CrossRef] [PubMed]
- Bitiniene, D.; Zamaliauskienė, R.; Kubilius, R.; Leketas, M.; Gailius, T.; Smirnovaite, K. Quality of life in patients with temporomandibular disorders. A systematic review. Stomatologija 2018, 20, 3–9. [Google Scholar]
- Sessle, B. Chronic Orofacial Pain: Models, Mechanisms, and Genetic and Related Environmental Influences. Int. J. Mol. Sci. 2021, 22, 7112. [Google Scholar] [CrossRef]
- Minervini, G.; Fiorillo, L.; Russo, D.; Lanza, A.; D’Amico, C.; Cervino, G.; Meto, A.; Di Francesco, F. Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature. Prosthesis 2022, 4, 253–262. [Google Scholar] [CrossRef]
- Minervini, G.; Romano, A.; Petruzzi, M.; Maio, C.; Serpico, R.; Lucchese, A.; Candotto, V.; Di Stasio, D. Telescopic overdenture on natural teeth: Prosthetic rehabilitation on (OFD) syndromic patient and a review on available literature. J. Biol. Regul. Homeost. Agents 2018, 32, 131–134. [Google Scholar]
- Aviram, J.; Samuelly-Leichtag, G. Efficacy of Cannabis-Based Medicines for Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pain Physician 2017, 20, E755–E796. [Google Scholar] [CrossRef]
- Oliveira, J.P.; Souza, M.T.; Cercato, L.M.; Souza, A.W.; Nampo, F.K.; Camargo, E.A. Natural products for orofacial nociception in pre-clinical studies: A systematic review. Arch. Oral Biol. 2020, 117, 104748. [Google Scholar] [CrossRef]
- Moccia, S.; Nucci, L.; Spagnuolo, C.; D’Apuzzo, F.; Piancino, M.G.; Minervini, G. Polyphenols as Potential Agents in the Management of Temporomandibular Disorders. Appl. Sci. 2020, 10, 5305. [Google Scholar] [CrossRef]
- Minervini, G.; Russo, D.; Herford, A.S.; Gorassini, F.; Meto, A.; D’Amico, C.; Cervino, G.; Cicciù, M.; Fiorillo, L. Teledentistry in the Management of Patients with Dental and Temporomandibular Disorders. BioMed. Res. Int. 2022, 2022, 7091153. [Google Scholar] [CrossRef] [PubMed]
- Bai, R.; Yao, C.; Zhong, Z.; Ge, J.; Bai, Z.; Ye, X.; Xie, T.; Xie, Y. Discovery of natural anti-inflammatory alkaloids: Potential leads for the drug discovery for the treatment of inflammation. Eur. J. Med. Chem. 2021, 213, 113165. [Google Scholar] [CrossRef] [PubMed]
- Moccia, S.; Siano, F.; Russo, G.L.; Volpe, M.G.; La Cara, F.; Pacifico, S.; Piccolella, S.; Picariello, G. Antiproliferative and antioxidant effect of polar hemp extracts (Cannabis sativa L., Fedora cv.) in human colorectal cell lines. Int. J. Food Sci. Nutr. 2020, 71, 410–423. [Google Scholar] [CrossRef]
- Tedesco, I.; Spagnuolo, C.; Russo, G.; Russo, M.; Cervellera, C.; Moccia, S. The Pro-Oxidant Activity of Red Wine Polyphenols Induces an Adaptive Antioxidant Response in Human Erythrocytes. Antioxidants 2021, 10, 800. [Google Scholar] [CrossRef] [PubMed]
- Takeda, M.; Shimazu, Y. Modulatory mechanism underlying how dietary constituents attenuate orofacial pain. J. Oral Sci. 2020, 62, 140–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, C.E.B.; Ouyang, L.; Kandasamy, R. Antinociceptive effects of minor cannabinoids, terpenes and flavonoids in Cannabis. Behav. Pharmacol. 2022, 33, 130–157. [Google Scholar] [CrossRef]
- Corder, G.; Castro, D.C.; Bruchas, M.R.; Scherrer, G. Endogenous and Exogenous Opioids in Pain. Annu. Rev. Neurosci. 2018, 41, 453–473. [Google Scholar] [CrossRef]
- Gouveia, D.N.; Pina, L.T.S.; Rabelo, T.K.; da Rocha Santos, W.B.; Quintans, J.S.S.; Guimaraes, A.G. Monoterpenes as Perspective to Chronic Pain Management: A Systematic Review. Curr. Drug Targets 2018, 19, 960–972. [Google Scholar] [CrossRef]
- Pergolizzi, J.V., Jr.; Taylor, R., Jr.; LeQuang, J.-A.; Raffa, R.B.; The NEMA Research Group. The role and mechanism of action of menthol in topical analgesic products. J. Clin. Pharm. Ther. 2018, 43, 313–319. [Google Scholar] [CrossRef] [Green Version]
- Baron, E.P. Medicinal Properties of Cannabinoids, Terpenes, and Flavonoids in Cannabis, and Benefits in Migraine, Headache, and Pain: An Update on Current Evidence and Cannabis Science. Headache 2018, 58, 1139–1186. [Google Scholar] [CrossRef] [PubMed]
- Lim, X.Y.; Tan, T.Y.C.; Rosli, S.H.M.; Sa’At, M.N.F.; Ali, S.S.; Mohamed, A.F.S. Cannabis sativa subsp. sativa’s pharmacological properties and health effects: A scoping review of current evidence. PLoS ONE 2021, 16, e0245471. [Google Scholar] [CrossRef] [PubMed]
- Tamba, B.I.; Stanciu, G.D.; Urîtu, C.M.; Rezus, E.; Stefanescu, R.; Mihai, C.T.; Luca, A.; Rusu-Zota, G.; Leon-Constantin, M.-M.; Cojocaru, E.; et al. Challenges and Opportunities in Preclinical Research of Synthetic Cannabinoids for Pain Therapy. Medicina 2020, 56, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossman, S.; Tan, H.; Gadiwalla, Y. Cannabis and orofacial pain: A systematic review. Br. J. Oral Maxillofac. Surg. 2022, 60, e677–e690. [Google Scholar] [CrossRef]
- Kopustinskiene, D.M.; Masteikova, R.; Lazauskas, R.; Bernatoniene, J. Cannabis sativa L. Bioactive Compounds and Their Protective Role in Oxidative Stress and Inflammation. Antioxidants 2022, 11, 660. [Google Scholar] [CrossRef]
- Henshaw, F.R.; Dewsbury, L.S.; Lim, C.K.; Steiner, G.Z. The Effects of Cannabinoids on Pro- and Anti-Inflammatory Cytokines: A Systematic Review of In Vivo Studies. Cannabis Cannabinoid Res. 2021, 6, 177–195. [Google Scholar] [CrossRef]
- Martínez, V.; Iriondo De-Hond, A.; Borrelli, F.; Capasso, R.; Del Castillo, M.D.; Abalo, R. Cannabidiol and Other Non-Psychoactive Cannabinoids for Prevention and Treatment of Gastrointestinal Disorders: Useful Nutraceuticals? Int. J. Mol. Sci. 2020, 21, 3067. [Google Scholar] [CrossRef]
- Atalay, S.; Jarocka-Karpowicz, I.; Skrzydlewska, E. Antioxidative and Anti-Inflammatory Properties of Cannabidiol. Antioxidants 2019, 9, 21. [Google Scholar] [CrossRef] [Green Version]
- Burgos, E.; Pascual, D.; Martín, M.I.; Goicoechea, C. Antinociceptive effect of the cannabinoid agonist, WIN 55,212-2, in the orofacial and temporomandibular formalin tests. Eur. J. Pain 2010, 14, 40–48. [Google Scholar] [CrossRef]
- Rotpenpian, N.; Yakkaphan, P. Review of Literatures: Physiology of Orofacial Pain in Dentistry. Eneuro 2021, 8, 1–7. [Google Scholar] [CrossRef]
- Shinoda, M.; Hitomi, S.; Iwata, K.; Hayashi, Y. Plastic changes in nociceptive pathways contributing to persistent orofacial pain. J. Oral Biosci. 2022, 64, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Shinoda, M.; Hayashi, Y.; Kubo, A.; Iwata, K. Pathophysiological mechanisms of persistent orofacial pain. J. Oral Sci. 2020, 62, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Crandall, J.A. An Introduction to Orofacial Pain. Dent. Clin. N. Am. 2018, 62, 511–523. [Google Scholar] [CrossRef]
- Luo, Y.; Suttle, A.; Zhang, Q.; Wang, P.; Chen, Y. Transient Receptor Potential (TRP) Ion Channels in Orofacial Pain. Mol. Neurobiol. 2021, 58, 2836–2850. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Gan, Y.-H. Prostaglandin E2 Upregulated Trigeminal Ganglionic Sodium Channel 1.7 Involving Temporomandibular Joint Inflammatory Pain in Rats. Inflammation 2017, 40, 1102–1109. [Google Scholar] [CrossRef]
- Shinoda, M.; Kubo, A.; Hayashi, Y.; Iwata, K. Peripheral and Central Mechanisms of Persistent Orofacial Pain. Front. Neurosci. 2019, 13, 1227. [Google Scholar] [CrossRef]
- Racich, M.J. Occlusion, temporomandibular disorders, and orofacial pain: An evidence-based overview and update with recommendations. J. Prosthet. Dent. 2018, 120, 678–685. [Google Scholar] [CrossRef]
- Ibi, M. Inflammation and Temporomandibular Joint Derangement. Biol. Pharm. Bull. 2019, 42, 538–542. [Google Scholar] [CrossRef] [Green Version]
- Bai, Q.; Liu, S.; Shu, H.; Tang, Y.; George, S.; Dong, T.; Schmidt, B.L.; Tao, F. TNFα in the Trigeminal Nociceptive System Is Critical for Temporomandibular Joint Pain. Mol. Neurobiol. 2019, 56, 278–291. [Google Scholar] [CrossRef]
- Ernberg, M. The role of molecular pain biomarkers in temporomandibular joint internal derangement. J. Oral Rehabil. 2017, 44, 481–491. [Google Scholar] [CrossRef]
- Harper, D.; Schrepf, A.; Clauw, D. Pain Mechanisms and Centralized Pain in Temporomandibular Disorders. J. Dent. Res. 2016, 95, 1102–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villa, G.; Ceruti, S.; Zanardelli, M.; Magni, G.; Jasmin, L.; Ohara, P.T.; Abbracchio, M.P. Temporomandibular Joint Inflammation Activates Glial and Immune Cells in Both the Trigeminal Ganglia and in the Spinal Trigeminal Nucleus. Mol. Pain 2010, 6, 89. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Bao, M.; Hou, C.; Wang, Y.; Zheng, L.; Peng, Y. The Role of TNF-α in the Pathogenesis of Temporomandibular Disorders. Biol. Pharm. Bull. 2021, 44, 1801–1809. [Google Scholar] [CrossRef]
- Güven, O.; Tekin, U.; Salmanoğlu, B.; Kaymak, E. Tumor necrosis factor-alpha levels in the synovial fluid of patients with temporomandibular joint internal derangement. J. Cranio-Maxillofac. Surg. 2015, 43, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Scrivani, S.J.; Khawaja, S.N.; Bavia, P.F. Nonsurgical Management of Pediatric Temporomandibular Joint Dysfunction. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Wieckiewicz, M.; Boening, K.; Wiland, P.; Shiau, Y.-Y.; Paradowska-Stolarz, A. Reported concepts for the treatment modalities and pain management of temporomandibular disorders. J. Headache Pain 2015, 16, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sommer, C.; Leinders, M.; Üçeyler, N. Inflammation in the pathophysiology of neuropathic pain. Pain 2018, 159, 595–602. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Kuner, R.; Jensen, T.S. Neuropathic pain: From mechanisms to treatment. Physiol. Rev. 2021, 101, 259–301. [Google Scholar] [CrossRef]
- Iwata, K.; Imamura, Y.; Honda, K.; Shinoda, M. Physiological Mechanisms of Neuropathic Pain: The Orofacial Region. Int. Rev. Neurobiol. 2011, 97, 227–250. [Google Scholar] [CrossRef]
- Pellati, F.; Borgonetti, V.; Brighenti, V.; Biagi, M.; Benvenuti, S.; Corsi, L. Cannabis sativa L. and Nonpsychoactive Cannabinoids: Their Chemistry and Role against Oxidative Stress, Inflammation, and Cancer. BioMed. Res. Int. 2018, 2018, 1691428. [Google Scholar] [CrossRef] [Green Version]
- Pollastro, F.; Minassi, A.; Fresu, L.G. Cannabis Phenolics and their Bioactivities. Curr. Med. Chem. 2018, 25, 1160–1185. [Google Scholar] [CrossRef] [PubMed]
- Radwan, M.; Chandra, S.; Gul, S.; ElSohly, M. Cannabinoids, Phenolics, Terpenes and Alkaloids of Cannabis. Molecules 2021, 26, 2774. [Google Scholar] [CrossRef] [PubMed]
- Mastinu, A.; Ribaudo, G.; Ongaro, A.; Bonini, S.A.; Memo, M.; Gianoncelli, A. Critical Review on the Chemical Aspects of Cannabidiol (CBD) and Harmonization of Computational Bioactivity Data. Curr. Med. Chem. 2021, 28, 213–237. [Google Scholar] [CrossRef] [PubMed]
- Nigro, E.; Formato, M.; Crescente, G.; Daniele, A. Cancer Initiation, Progression and Resistance: Are Phytocannabinoids from Cannabis sativa L. Promising Compounds? Molecules 2021, 26, 2668. [Google Scholar] [CrossRef]
- Landucci, E.; Pellegrini-Giampietro, D.; Gianoncelli, A.; Ribaudo, G. Cannabidiol preferentially binds TRPV2: A novel mechanism of action. Neural Regen. Res. 2022, 17, 2693–2694. [Google Scholar] [CrossRef]
- Brighenti, V.; Pellati, F.; Steinbach, M.; Maran, D.; Benvenuti, S. Development of a new extraction technique and HPLC method for the analysis of non-psychoactive cannabinoids in fibre-type Cannabis sativa L. (hemp). J. Pharm. Biomed. Anal. 2017, 143, 228–236. [Google Scholar] [CrossRef]
- Pellati, F.; Brighenti, V.; Sperlea, J.; Marchetti, L.; Bertelli, D.; Benvenuti, S. New Methods for the Comprehensive Analysis of Bioactive Compounds in Cannabis sativa L. (hemp). Molecules 2018, 23, 2639. [Google Scholar] [CrossRef] [Green Version]
- Kim, A.L.; Yun, Y.J.; Choi, H.W.; Hong, C.-H.; Shim, H.J.; Lee, J.H.; Kim, Y.-C. Profiling Cannabinoid Contents and Expression Levels of Corresponding Biosynthetic Genes in Commercial Cannabis (Cannabis sativa L.) Cultivars. Plants 2022, 11, 3088. [Google Scholar] [CrossRef]
- Finn, D.P.; Haroutounian, S.; Hohmann, A.G.; Krane, E.; Soliman, N.; Rice, A.S. Cannabinoids, the endocannabinoid system, and pain: A review of preclinical studies. Pain 2021, 162, S5–S25. [Google Scholar] [CrossRef]
- Woodhams, S.G.; Chapman, V.; Finn, D.P.; Hohmann, A.G.; Neugebauer, V. The cannabinoid system and pain. Neuropharmacology 2017, 124, 105–120. [Google Scholar] [CrossRef] [Green Version]
- Howlett, A.C.; Abood, M.E. CB1 and CB2 Receptor Pharmacology. Adv. Pharmacol. 2017, 80, 169–206. [Google Scholar] [CrossRef]
- Konermann, A.; Jäger, A.; Held, S.A.E.; Brossart, P.; Schmöle, A. In vivo and In vitro Identification of Endocannabinoid Signaling in Periodontal Tissues and Their Potential Role in Local Pathophysiology. Cell. Mol. Neurobiol. 2017, 37, 1511–1520. [Google Scholar] [CrossRef] [PubMed]
- McDonough, P.; McKenna, J.P.; McCreary, C.; Downer, E.J. Neuropathic orofacial pain: Cannabinoids as a therapeutic avenue. Int. J. Biochem. Cell Biol. 2014, 55, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Zubrzycki, M.; Stasiolek, M.; Zubrzycka, M. Opioid and Endocannabinoid System in Orofacial Pain. Physiol. Res. 2019, 68, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Greco, R.; Demartini, C.; Zanaboni, A.M.; Francavilla, M.; De Icco, R.; Ahmad, L.; Tassorelli, C. The endocannabinoid system and related lipids as potential targets for the treatment of migraine-related pain. Headache 2022, 62, 227–240. [Google Scholar] [CrossRef]
- Khan, H.; Ghori, F.K.; Ghani, U.; Javed, A.; Zahid, S. Cannabinoid and endocannabinoid system: A promising therapeutic intervention for multiple sclerosis. Mol. Biol. Rep. 2022, 49, 5117–5131. [Google Scholar] [CrossRef]
- Zou, S.; Kumar, U. Cannabinoid Receptors and the Endocannabinoid System: Signaling and Function in the Central Nervous System. Int. J. Mol. Sci. 2018, 19, 833. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Zhou, J.; Lehmann, C. GPR55–A putative “type 3” cannabinoid receptor in inflammation. J. Basic Clin. Physiol. Pharmacol. 2016, 27, 297–302. [Google Scholar] [CrossRef] [Green Version]
- Muller, C.; Morales, P.; Reggio, P.H. Cannabinoid Ligands Targeting TRP Channels. Front. Mol. Neurosci. 2019, 11, 487. [Google Scholar] [CrossRef] [Green Version]
- Bruni, N.; Della Pepa, C.; Oliaro-Bosso, S.; Pessione, E.; Gastaldi, D.; Dosio, F. Cannabinoid Delivery Systems for Pain and Inflammation Treatment. Molecules 2018, 23, 2478. [Google Scholar] [CrossRef] [Green Version]
- Lucas, C.J.; Galettis, P.; Schneider, J. The pharmacokinetics and the pharmacodynamics of cannabinoids. Br. J. Clin. Pharmacol. 2018, 84, 2477–2482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitecka-Buchta, A.; Nowak-Wachol, A.; Wachol, K.; Walczyńska-Dragon, K.; Olczyk, P.; Batoryna, O.; Kempa, W.; Baron, S. Myorelaxant Effect of Transdermal Cannabidiol Application in Patients with TMD: A Randomized, Double-Blind Trial. J. Clin. Med. 2019, 8, 1886. [Google Scholar] [CrossRef] [PubMed]
- Hammell, D.; Zhang, L.; Ma, F.; Abshire, S.; McIlwrath, S.; Stinchcomb, A.; Westlund, K. Transdermal cannabidiol reduces inflammation and pain-related behaviours in a rat model of arthritis. Eur. J. Pain 2016, 20, 936–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phan, N.Q.; Siepmann, D.; Gralow, I.; Ständer, S. Adjuvant topical therapy with a cannabinoid receptor agonist in facial postherpetic neuralgia. J. Dtsch. Dermatol. Ges. 2010, 8, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Kress, M.; Kuner, R. Mode of action of cannabinoids on nociceptive nerve endings. Exp. Brain Res. 2009, 196, 79–88. [Google Scholar] [CrossRef]
- Ibrahim, M.M.; Porreca, F.; Lai, J.; Albrecht, P.J.; Rice, F.L.; Khodorova, A.; Davar, G.; Makriyannis, A.; Vanderah, T.W.; Mata, H.P.; et al. CB2 cannabinoid receptor activation produces antinociception by stimulating peripheral release of endogenous opioids. Proc. Natl. Acad. Sci. USA 2005, 102, 3093–3098. [Google Scholar] [CrossRef] [Green Version]
- Júnior, J.M.; Damasceno, M.B.; Santos, S.A.; Barbosa, T.M.; Araújo, J.R.; Vieira-Neto, A.E.; Wong, D.V.; Lima-Júnior, R.C.; Campos, A.R. Acute and neuropathic orofacial antinociceptive effect of eucalyptol. Inflammopharmacology 2017, 25, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Votrubec, C.; Tran, P.; Lei, A.; Brunet, Z.; Bean, L.; Olsen, B.; Sharma, D. Cannabinoid therapeutics in orofacial pain management: A systematic review. Aust. Dent. J. 2022, 67, 314–327. [Google Scholar] [CrossRef]
- Liang, Y.C.; Huang, C.C.; Hsu, K.-S. The synthetic cannabinoids attenuate allodynia and hyperalgesia in a rat model of trigeminal neuropathic pain. Neuropharmacology 2007, 53, 169–177. [Google Scholar] [CrossRef]
- Kalliomäki, J.; Segerdahl, M.; Webster, L.; Reimfelt, A.; Huizar, K.; Annas, P.; Karlsten, R.; Quiding, H. Evaluation of the analgesic efficacy of AZD1940, a novel cannabinoid agonist, on post-operative pain after lower third molar surgical removal. Scand. J. Pain 2013, 4, 17–22. [Google Scholar] [CrossRef]
- Ostenfeld, T.; Price, J.; Albanese, M.; Bullman, J.; Guillard, F.; Meyer, I.; Leeson, R.; Costantin, C.; Ziviani, L.; Nocini, P.F.; et al. A Randomized, Controlled Study to Investigate the Analgesic Efficacy of Single Doses of the Cannabinoid Receptor-2 Agonist GW842166, Ibuprofen or Placebo in Patients with Acute Pain Following Third Molar Tooth Extraction. Clin. J. Pain 2011, 27, 668–676. [Google Scholar] [CrossRef] [PubMed]
- Sainsbury, B.; Bloxham, J.; Pour, M.H.; Padilla, M.; Enciso, R. Efficacy of cannabis-based medications compared to placebo for the treatment of chronic neuropathic pain: A systematic review with meta-analysis. J. Dent. Anesth. Pain Med. 2021, 21, 479–506. [Google Scholar] [CrossRef] [PubMed]
- Russo, E.B. Taming THC: Potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br. J. Pharmacol. 2011, 163, 1344–1364. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, A.G.; Quintans, J.S.S.; Quintans-Júnior, L.J. Monoterpenes with Analgesic Activity—A Systematic Review. Phytother. Res. 2013, 27, 1–15. [Google Scholar] [CrossRef]
- Burkhart, C.G.; Burkhart, H.R. Contact irritant dermatitis and anti-pruritic agents: The need to address the itch. J. Drugs Dermatol. 2003, 2, 143–146. [Google Scholar]
- Andre, C.M.; Hausman, J.-F.; Guerriero, G. Cannabis sativa: The Plant of the Thousand and One Molecules. Front. Plant Sci. 2016, 7, 19. [Google Scholar] [CrossRef] [Green Version]
- Iqubal, A.; Ahmed, M.; Iqubal, M.K.; Pottoo, F.H.; Haque, S.E. Polyphenols as Potential Therapeutics for Pain and Inflammation in Spinal Cord Injury. Curr. Mol. Pharmacol. 2021, 14, 714–730. [Google Scholar] [CrossRef]
- Hashempur, M.H.; Sadrneshin, S.; Mosavat, S.H.; Ashraf, A. Green tea (Camellia sinensis) for patients with knee osteoarthritis: A randomized open-label active-controlled clinical trial. Clin. Nutr. 2018, 37, 85–90. [Google Scholar] [CrossRef]
- Schell, J.; Scofield, R.H.; Barrett, J.R.; Kurien, B.T.; Betts, N.; Lyons, T.J.; Zhao, Y.D.; Basu, A. Strawberries Improve Pain and Inflammation in Obese Adults with Radiographic Evidence of Knee Osteoarthritis. Nutrients 2017, 9, 949. [Google Scholar] [CrossRef] [Green Version]
- Uddin, S.J.; Hasan, F.; Afroz, M.; Sarker, D.K.; Rouf, R.; Islam, M.T.; Shilpi, J.A.; Mubarak, M.S. Curcumin and its Multi-target Function Against Pain and Inflammation: An Update of Pre-clinical Data. Curr. Drug Targets 2021, 22, 656–671. [Google Scholar] [CrossRef]
- Ma, Y.; Liu, S.; Shu, H.; Crawford, J.; Xing, Y.; Tao, F. Resveratrol alleviates temporomandibular joint inflammatory pain by recovering disturbed gut microbiota. Brain Behav. Immun. 2020, 87, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Di Marzo, V. The endocannabinoidome as a substrate for noneuphoric phytocannabinoid action and gut microbiome dysfunction in neuropsychiatric disorders. Dialogues Clin. Neurosci. 2020, 22, 259–269. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) | ||||
| Formulation | Dose and Route/Time of Administration | Study Participants | Results | Reference |
| CBD formulation | Topical/twice a day for 14 days | 60 patients (Female/male) | Reduction in masseter activity; decrease of pain intensity according to VAS scale; improvement of muscle function in patients with myofascial pain | [72] |
| (b) | ||||
| Formulation | Dose and route/time of administration | Animal models | Results | Reference |
| Eucalyptol | 100, 200, and 400 mg/kg; Single dose 1 h before the induction | Male Swiss, C57BL/6 J or BALB/c mice; 20–25 g; | Reduction of face rubbing time on capsaicin and glutamate tests | [77] |
| (a) | ||||
| Formulation | Dose and Route/Time of Administration | Study Participants | Results | Reference |
| Agonist of CBR-2 (GW842166) | 100 mg; Single dose 1 h before the surgical third molar removal | 34 patients (Female/male) | Similar effect to the placebo | [81] |
| Agonist of CBR-2 (GW842166) | 800 mg; Single dose 1 h before the surgical third molar removal | 27 patients (Female/male) | Improvement in analgesia over placebo with both VAS and VRS pain ratings | [81] |
| Cannabinoid agonist (AZD1940) | 800 μg; Single dose 1.5 h before the surgical third molar removal | 61 patients (Female/male) | No statistically significant difference in pain compared with the placebo | [80] |
| (b) | ||||
| Formulation | Dose and route/time of administration | Animal models | Results | Reference |
| Cannabinoid agonist (WIN 55,212-2) | Intraperitoneal; 0.5, 1 mg/kg; Single dose 30 min before the nociceptive stimulus | Adult male Wistar rats; weight: 200–250 g | Antinociceptive effect | [29] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crescente, G.; Minervini, G.; Spagnuolo, C.; Moccia, S. Cannabis Bioactive Compound-Based Formulations: New Perspectives for the Management of Orofacial Pain. Molecules 2023, 28, 106. https://doi.org/10.3390/molecules28010106
Crescente G, Minervini G, Spagnuolo C, Moccia S. Cannabis Bioactive Compound-Based Formulations: New Perspectives for the Management of Orofacial Pain. Molecules. 2023; 28(1):106. https://doi.org/10.3390/molecules28010106
Chicago/Turabian StyleCrescente, Giuseppina, Giuseppe Minervini, Carmela Spagnuolo, and Stefania Moccia. 2023. "Cannabis Bioactive Compound-Based Formulations: New Perspectives for the Management of Orofacial Pain" Molecules 28, no. 1: 106. https://doi.org/10.3390/molecules28010106
APA StyleCrescente, G., Minervini, G., Spagnuolo, C., & Moccia, S. (2023). Cannabis Bioactive Compound-Based Formulations: New Perspectives for the Management of Orofacial Pain. Molecules, 28(1), 106. https://doi.org/10.3390/molecules28010106